A Pilot Study to Validate a Standardized One-Week Salt Estimation Method Evaluating Salt Intake and Its Sources for Family Members in China

Abstract
:1. Introduction
2. Methods
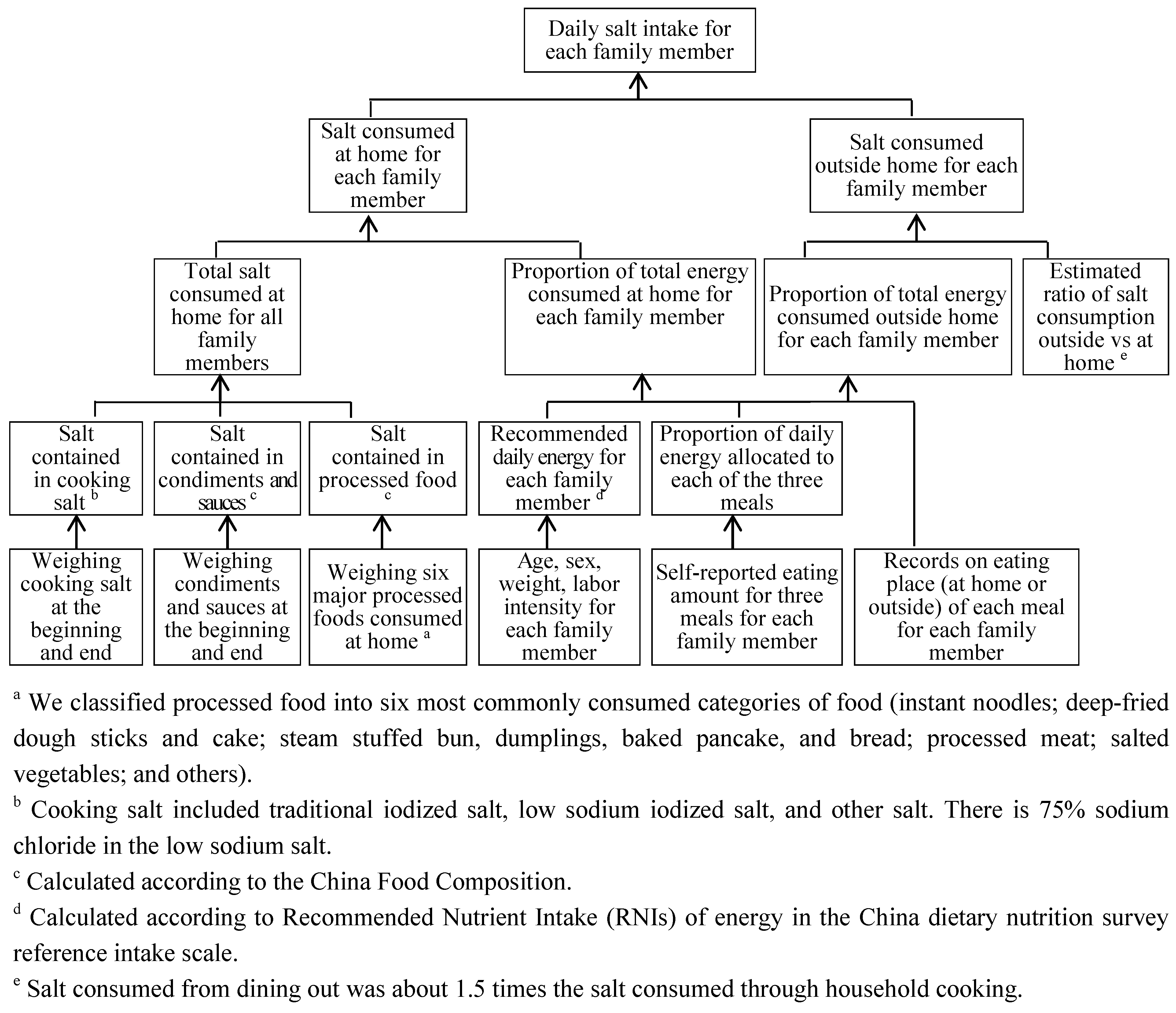
2.1. Principles of the One-Week Salt Estimation Method

2.2. Comparison between the “One-Week Salt Estimation Method” and 24-h Urine Collection
2.3. Participants
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Basic Characteristics

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Children | Adults |
|---|---|---|
| Age range | 2–11 | 34–74 |
| Participants who completed the dietary record (n = 37) | ||
| Number | 12 | 25 |
| Male (%) | 6 (50.0) | 11 (44.0) |
| Age (mean ± SD) | 10.0 ± 3.2 | 42.3 ± 9.4 |
| Weight (Kg) (mean ± SD) | 36.7 ± 11.3 | 69.0 ± 14.1 |
| Participants who completed the 7-day 24-h urine collection (n = 26) | ||
| Number (%) | 10 | 16 |
| Male (%) | 5 (50.0) | 8 (50.0) |
| Age (mean ± SD) | 10.1 ± 0.3 | 39.4 ± 3.0 |
| Weight (Kg) (mean ± SD) | 37.1 ± 5.8 | 70.1 ± 11.8 |
3.2. 24-h Urine Collection
| Age Group | N | Urine Volume | Creatinine Excretion | Sodium Excretion | Potassium Excretion | Sodium-Potassium Ratio |
|---|---|---|---|---|---|---|
| (mL/24 h) | (mmol/24 h) | (mmol/24 h) | (mmol/24 h) | (mmol:mmol) | ||
| Total | 26 | 1678.1 ± 678.5 | 10.8 ± 4.5 | 268.5 ± 94.4 | 55.8 ± 23.3 | 5.2 ± 1.5 |
| Adults | 10 | 2078.7 ± 529.0 | 13.8 ± 2.9 | 330.4 ± 54.6 | 68.9 ± 18.9 | 5.1 ± 1.3 |
| Children | 16 | 1037.1 ± 265.7 | 6.0 ± 1.0 | 169.4 ± 45.3 | 34.8 ± 10.6 | 5.2 ± 1.8 |
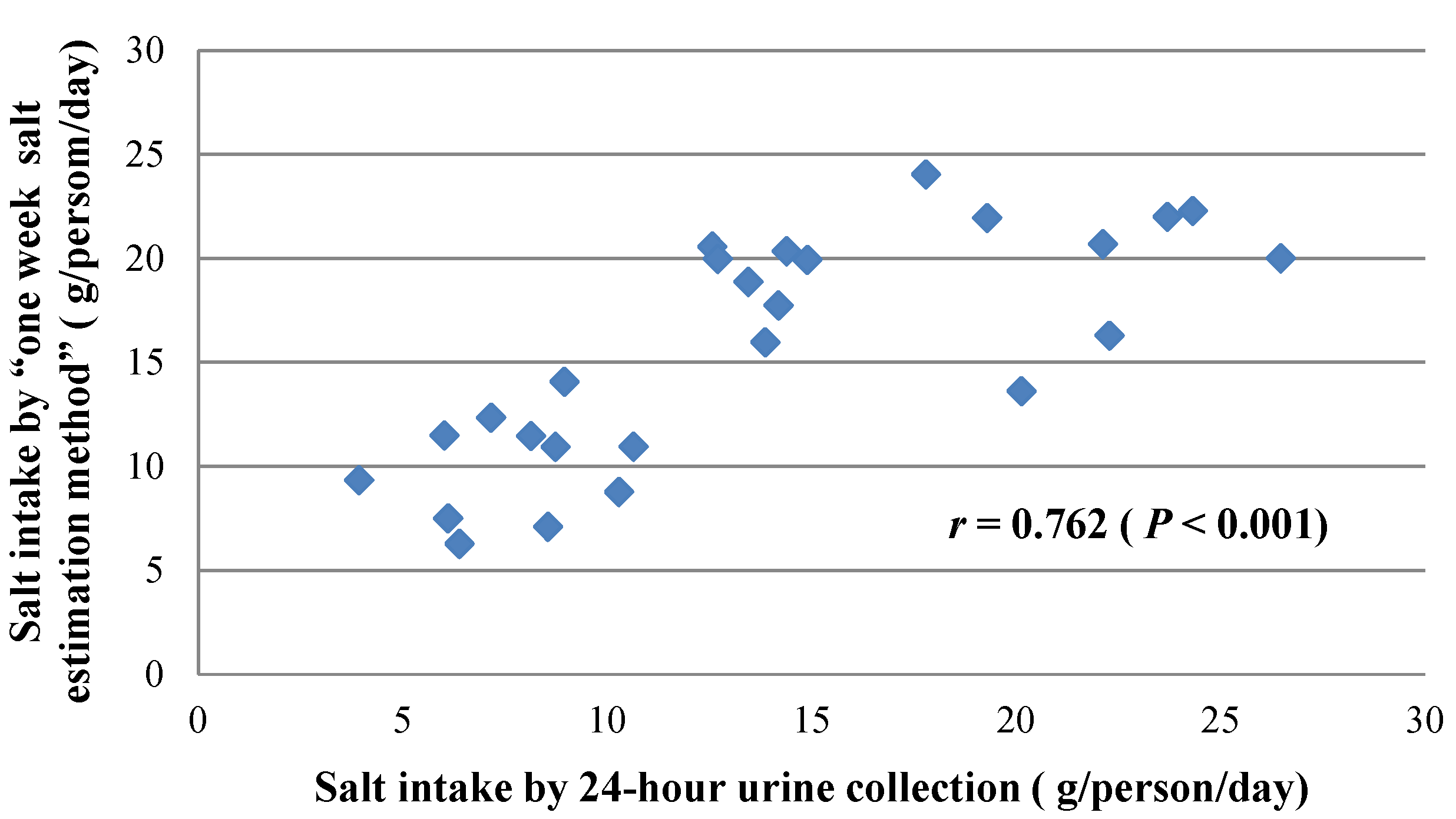
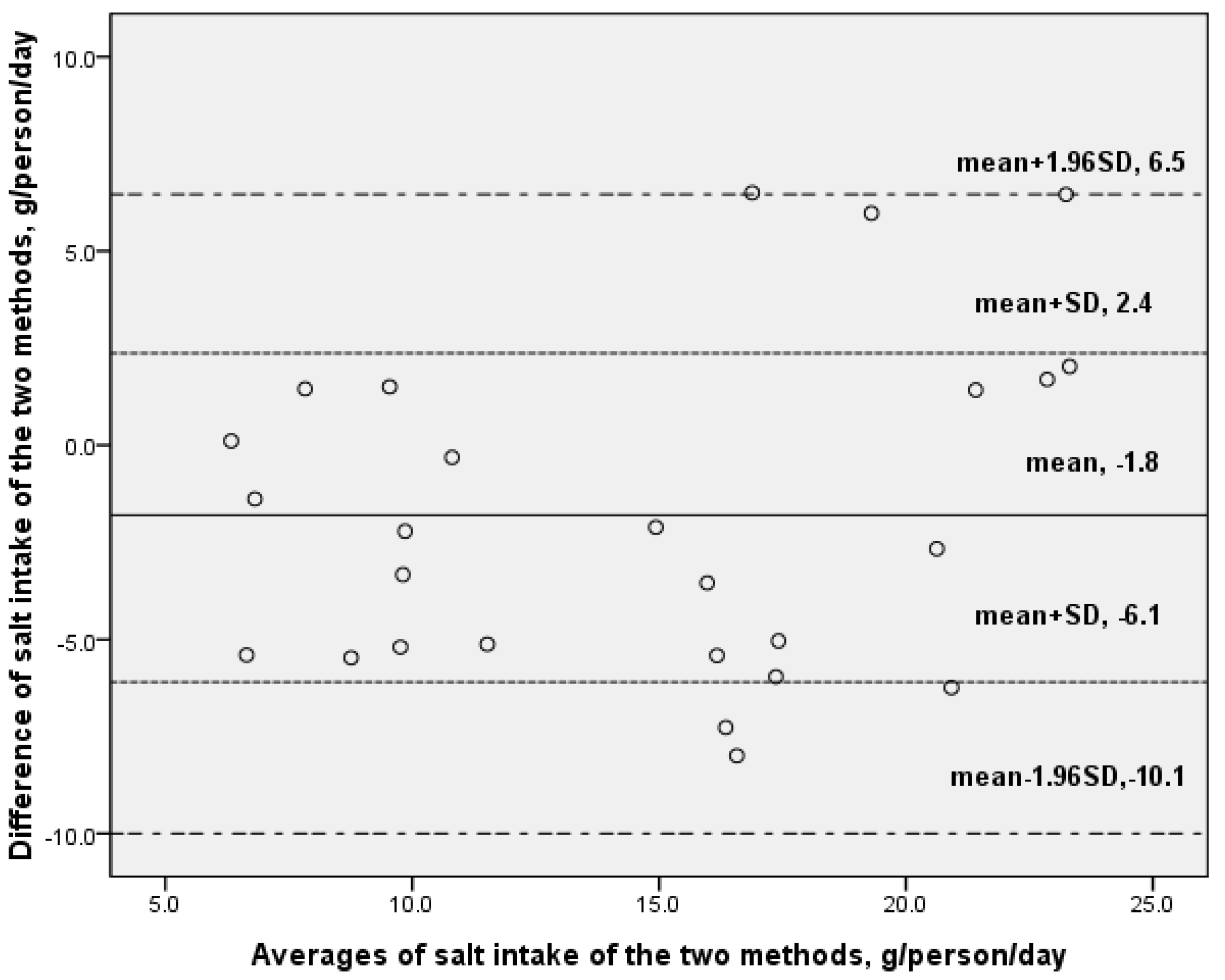
3.3. Comparison between One-Week Salt Estimation Method and 24-h Urine Collection

| Method | Estimated Salt Intake (g/Day, Mean ± SD) | ||
|---|---|---|---|
| Children | Adults | Total | |
| 7 days 24-h urine collection (standard method) | 9.8 ± 2.4 | 19.2 ± 3.2 | 15.6 ± 5.5 |
| One-week salt estimation (new method) | 7.8 ± 2.1 | 17.5 ± 5.4 | 13.7. ± 6.5 |
| Difference | 2.0 ± 2.7 | 1.7 ± 5.0 | 1.8 ± 4.2 |
| p = 0.044 | p = 0.193 | p = 0.037 | |
3.4. Results of the “One-Week Salt Estimation Method”

| Family Members | Daily Salt Intake (g/person, Mean ± SD) | Proportion of the Different Sources (%) | |||
|---|---|---|---|---|---|
| Cooking Salt Added | Condiments and Sauces | Restaurants or Canteen | Processed Food | ||
| Total (n = 37) | 13.6 ± 6.7 | 33.5 | 10.2 | 43.4 | 12.9 |
| Male (n = 17) | 15.7 ± 7.1 | 28.4 | 9.1 | 51.2 | 11.3 |
| Female (n = 20) | 11.9 ± 6.0 | 37.9 | 11.2 | 36.7 | 14.2 |
| Children (n = 12) | 7.6 ± 2.9 | 35.1 | 11.0 | 40.3 | 13.5 |
| Boy (n = 6) | 8.6 ± 2.4 | 30.7 | 10.3 | 44.8 | 14.2 |
| Girl (n = 6) | 6.6 ± 3.1 | 39.6 | 11.7 | 35.9 | 12.9 |
| Adults (n = 25) | 16.5 ± 6.1 | 32.8 | 9.8 | 44.8 | 12.6 |
| Male (n = 11) | 19.6 ± 5.6 | 27.2 | 8.4 | 54.7 | 9.7 |
| Female (n = 14) | 14.1 ± 5.5 | 37.2 | 11.0 | 37.1 | 14.8 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar]
- World Health Organization. Reducing Salt Intake in Populations: Report of a WHO Forum and Technical Meeting; World Health Organization: Paris, France, 2006; pp. 6–11. [Google Scholar]
- Li, L.M.; Rao, K.Q.; Kong, L.Z.; Yao, C.H.; Xiang, H.D.; Zhai, F.Y.; Ma, G.S.; Yang, X.G. A description on the Chinese national nutrition and health survey in 2002. Chin. J. Epidemiol. 2005, 26, 478–484. [Google Scholar]
- Dong, W. The Beijing government started to promote the use of low sodium salt (in Chinese); China Food Safety News: Beijing, China, 2011. [Google Scholar]
- Wang, L. Chinese Residents Nutrition and Health Survey in 2002; People’s Medical Publishing House: Beijing, China, 2005; p. 21. [Google Scholar]
- Pietinen, P.; Uusitalo, U.; Nissinen, A. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 h urinary sodium and potassium excretion. BMJ 1988, 297, 319–328. [Google Scholar]
- Anderson, C.A.; Appel, L.J.; Okuda, N.; Brown, I.J.; Chan, Q.; Zhao, L.; Ueshima, H.; Kesteloot, H.; Miura, K.; Curb, J.D.; et al. Dietary sources of sodium in China, Japan, the United Kingdom, and the United States, women and men aged 40 to 59 years: The INTERMAP study. J. Am. Diet. Assoc. 2010, 110, 736–745. [Google Scholar]
- He, J.; Klag, M.J.; Whelton, P.K.; Chen, J.Y.; Mo, J.P.; Qian, M.C.; Coresh, J.; Mo, P.S.; He, G.Q. Agreement between overnight and 24-h urinary cation excretions in southern Chinese men. Am. J. Epidemiol. 1993, 137, 1212–1220. [Google Scholar]
- Liu, K.; Dyer, A.R.; Cooper, R.S.; Stamler, R.; Stamler, J. Can overnight urine replace 24-h urine collection to assess salt intake? Hypertension 1979, 1, 529–536. [Google Scholar]
- Micheli, E.T.; Rosa, A.A. Estimation of sodium intake by urinary excretion and dietary records in children and adolescents from Porto Alegre, Brazil: A comparision of two methods. Nutr. Res. 2003, 23, 1477–1487. [Google Scholar]
- Anmin, N.; Yonglu, W.; Tianlu, Y. The comparison of Na and K between four period urine and 24 h urine in 42 adults. J. Lanzhou Univ. (Med. Sci.) 1983, 4, 63–64. [Google Scholar]
- Sasaki, S.; Yanagibori, R.; Amano, K. Validity of a self-administered diet history questionnaire for assessment of sodium and potassium: Comparison with single 24-h urinary excretion. Jpn. Circ. J. 1998, 62, 431–435. [Google Scholar]
- Tuomilehto, J.; Tanskanen, A.; Pietinen, P. Value of overnight urines in the follow-up of people with borderline hypertensive trying to reduce their salt intake. Acta Cardiol. 1985, 40, 325–328. [Google Scholar]
- Leiba, A.; Vald, A.; Peleg, E.; Shamiss, A.; Grossman, E. Does dietary recall adequately assess sodium, potassium, and calcium intake in hypertensive patients. Nutrition 2005, 21, 462–466. [Google Scholar]
- Luft, F.C.; Fineberg, N.S.; Sloan, R.S. Overnight urine collections to estimate sodium intake. Hypertension 1982, 4, 494–498. [Google Scholar]
- Dennis, B.; Stamler, J.; Buzzard, M.; Conway, R.; Elliott, P.; Moag-Stahlberg, A.; Okayama, A.; Okuda, N.; Robertson, C.; Robinson, F.; et al. INTERMAP: The dietary data—Process and quality control. J. Hum. Hypertens. 2003, 17, 609–622. [Google Scholar]
- Li, Y.; He, Y.; Zhai, F.; Yang, X.; Hu, X.; Zhao, W.; Ma, G. Comparison of assessment of food intakes by using three dietary survey methods. Chin. J. Prev. Med. 2006, 40, 273–280. [Google Scholar]
- Yang, Y. China Food Composition; Peking University Medical Press: Beijing, China, 2002; pp. 201–212. [Google Scholar]
- Bu, S.Y.; Kang, M.H.; Kim, E.J.; Choi, M.K. Dietary intake ratios of calcium-to-phosphorus and sodium-to-potassium are associated with serum lipid levels in healthy Korean adults. Prev. Nutr. Food Sci. 2012, 17, 93–100. [Google Scholar]
- Chinese Nutrition Association. Chinese DRIs; China Light Industry Press: Beijing, China, 2006; pp. 92–94. [Google Scholar]
- Bi, Z.; Liang, X.; Xu, A.; Wang, L.; Shi, X.; Zhao, W.; Ma, J.; Guo, X.; Zhang, X.; Zhang, J.; et al. Hypertension prevalence, awareness, treatment, and control and sodium intake in Shandong Province, China: Baseline results from Shandong-Ministry of Health Action on Salt Reduction and Hypertension (SMASH), 2011. Prev. Chronic. Dis. 2014, 11. [Google Scholar] [CrossRef]
- Xu, J.; Zhao, J.; Ma, J. Investigation of the main condiments used in restaurants and cafeterias in Shandong Pronvince. Chin. J. Prev. Med. 2014, 1, 72–73. [Google Scholar]
- Chinese Nutrition Society. Dietary Guidelines for Chinese Residents 2007; The Peoples Press of Tibet: Lhasa, China, 2008; pp. 14–25. [Google Scholar]
- Yao, Z.; Sha, Y.; Yu, Y.; Li, H.; Teng, R.; Ma, X.; Li, C.; Xin, X.; Huang, L. A preliminary study on nutritional status of Beijing residents in 2009 and its changing trend. Chin. J. Public Health 2010, 26, 1595–1596. [Google Scholar]
- Mattes, R.D.; Donnelly, D. Relative contributions of dietary sodium sources. J. Am. Coll. Nutr. 1991, 10, 383–393. [Google Scholar]
- Bland, J.M.; Altman, D.G. Agreement between methods of measurement with multiple observations per individual. J. Biopharm. Stat. 2007, 17, 571–582. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Zhao, F.; Zhang, P.; Gao, J.; Liu, C.; He, F.J.; Lin, C.-P. A Pilot Study to Validate a Standardized One-Week Salt Estimation Method Evaluating Salt Intake and Its Sources for Family Members in China. Nutrients 2015, 7, 751-763. https://doi.org/10.3390/nu7020751
Zhang L, Zhao F, Zhang P, Gao J, Liu C, He FJ, Lin C-P. A Pilot Study to Validate a Standardized One-Week Salt Estimation Method Evaluating Salt Intake and Its Sources for Family Members in China. Nutrients. 2015; 7(2):751-763. https://doi.org/10.3390/nu7020751
Chicago/Turabian StyleZhang, Lu, Fang Zhao, Puhong Zhang, Jianmei Gao, Caixia Liu, Feng J. He, and Ching-Ping Lin. 2015. "A Pilot Study to Validate a Standardized One-Week Salt Estimation Method Evaluating Salt Intake and Its Sources for Family Members in China" Nutrients 7, no. 2: 751-763. https://doi.org/10.3390/nu7020751