Systematic Review of Anthocyanins and Markers of Cardiovascular Disease

Abstract
:1. Introduction
2. Materials and Methods
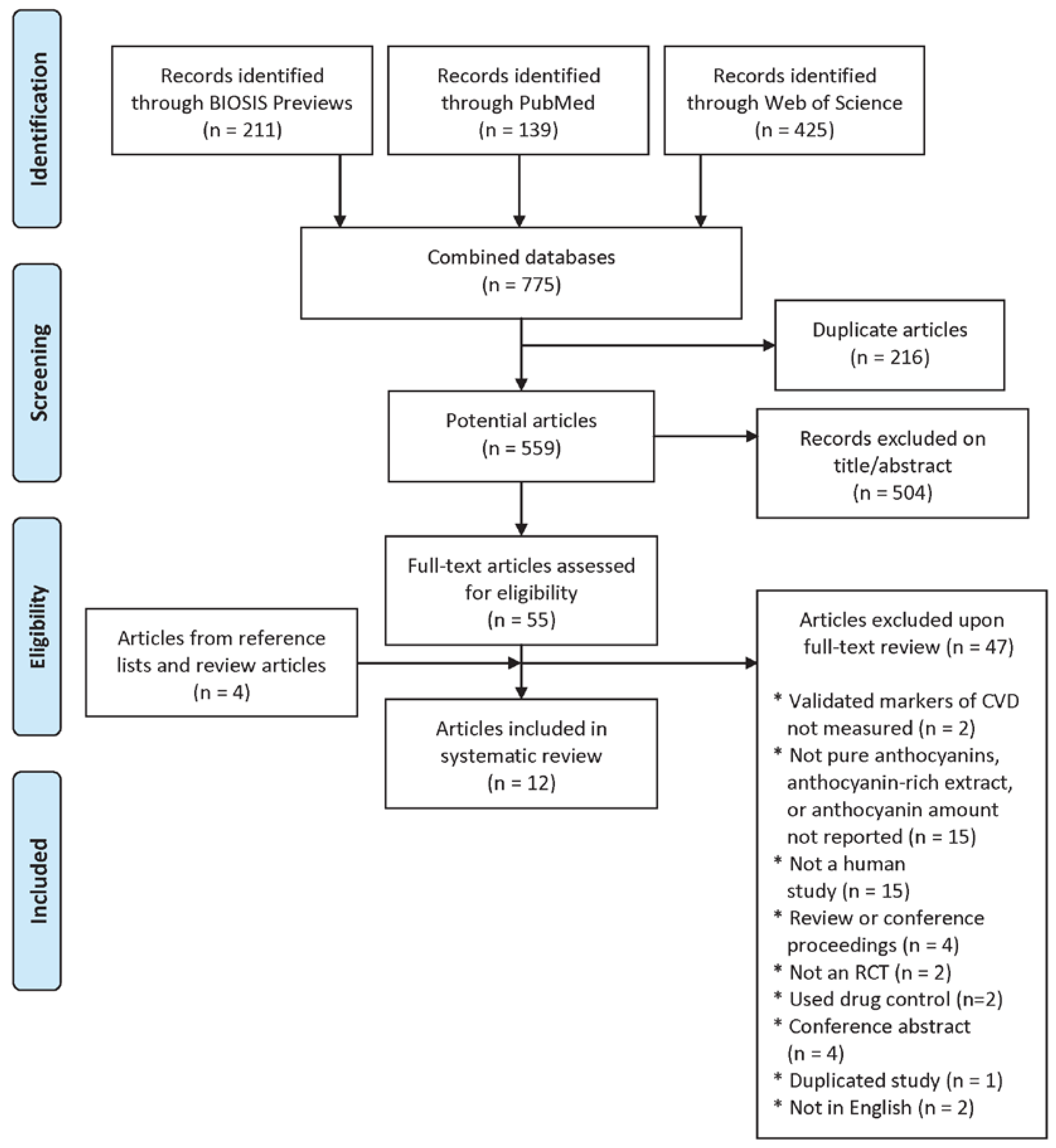
2.1. Literature Search
2.2. Study Selection

2.3. Data Synthesis

{kind=link}
| Reference | Country | Design | No. Randomized | No. Completed | Gender | Age (Year) | BMI or Weight Status | CVD-Related Disease Status | Intervention | Extract Dose | Anthocyanin Dose | Control | Intervention Length | End Point(s) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Curtis et al., 2009 [14] | United Kingdom | Parallel | 57 | 52 | Postmenopausal women | <70 | 20–32 | Healthy | Elderberry extract capsule | NR | 500 mg/day | Placebo capsule | 12 weeks | Triglycerides, TC, LDL, HDL, SBP, and DBP |
| Gurrola-Díaz et al., 2010 [15] | Mexico | Parallel | 152 | 124 | Women and men | 30–71 | NR | Healthy and MetS | Hibiscus sabdariffa extract powder + preventative diet | 100 mg/day | 19.24 mg/day | Preventive diet | 1 month | Triglycerides, TC, LDL, HDL, SBP, and DBP |
| Hansen et al., 2005 [16] | Denmark | Parallel | 70 | 69 | Women and men | 38–75 | Mean 25 | Healthy | Red grape extract | Full or half dose (unclear) | 71 mg/day for men; 48 mg/day for women; 36 mg/day for men; 24 mg/day for women | Placebo capsule (microcrystalline cellulose) | 4 weeks | TC, LDL, HDL, SBP, and DBP |
| Hassellund et al., 2012 [17] | Norway | Crossover | 31 | 27 | Men | 35–51 | Mean 27 | Prehypertensive | Purified anthocyanins from bilberry and black currant | NA | 640 mg/day | Placebo capsule (maltodextrin) | 4 weeks | SBP and DBP |
| Hassellund et al., 2013 [18] | Norway | Crossover | 31 | 27 | Men | 35–51 | NR | Prehypertensive | Purified anthocyanins from bilberry and black currant | NA | 640 mg/day | Placebo capsule (maltodextrin + blue color) | 4 weeks | Triglycerides, TC, LDL, and HDL |
| Karlsen et al., 2007 [19] | Norway | Parallel | 120 | 118 | Women and men | 40–74 | Mean 25 | Healthy | Purified anthocyanins from bilberry and black currant | NA | 300 mg/day | Placebo capsule (maltodextrin + blue color) | 3 weeks | TC and HDL |
| Kianbakht et al., 2014 [20] | Iran | Parallel | 105 | 80 | Women and men | 20–60 | Mean 30 | Primary hyperlipidemia | Whortleberry extract | 1050 mg/day | 7.35 mg/day | Placebo capsule (toast powder) | 2 months | Triglycerides, TC, LDL, and HDL |
| Naruszewicz et al., 2007 [14] | Poland | Parallel | NR | 44 | Postmenopausal women, and men | Mean 66 | Mean 26 | Post-MI | Chokeberry extract | 255 mg/day | 63.75 mg/day | Placebo capsule (maltodextrin) | 6 weeks | Triglycerides, TC, LDL, HDL, SBP, and DBP |
| Qin et al., 2009 [21] | China | Parallel | NR | 120 | Women and men | 40–65 | Mean 27 | Dyslipidemic | Purified anthocyanins from bilberry and black currant | NA | 320 mg/day | Placebo capsule (maltodextrin and pullalan) | 12 weeks | Triglycerides, TC, LDL, HDL, SBP, and DBP |
| Soltani et al., 2014 [22] | Iran | Parallel | 54 | 50 | Women and men | ≥18 | Mean 25 | Hyperlipidemic | Vaccinium arctostaphylos extract | 1000 mg/day | 90 mg/day | Placebo capsule (calcium phosphate) | 4 weeks | Triglycerides, TC, LDL, and HDL |
| Zhu et al., 2011 [23] | China | Crossover | 150 | 146 | Women and men | 40–65 | Mean 26 | Hypercholesterolemic | Purified anthocyanins from bilberry and black currant | NA | 320 mg/day | Placebo capsule | 12 weeks | SBP and DBP |
| Zhu et al., 2013 [24] | China | Parallel | 150 | 146 | Women and men | 40–65 | Mean 26 | Hypercholesterolemic | Purified anthocyanins from bilberry and black currant | NA | 320 mg/day | Placebo capsule | 24 weeks | Triglycerides, TC, LDL, and HDL |
2.4. Study Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Lipoproteins
| Reference | SIGN Quality | Anthocyanin Dose (mg/Day) | CVD-Related Disease Status | LDL (mg/dL) | HDL (mg/dL) | Total Cholesterol (mg/dL) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Percent Change in Intervention | Percent Change in Control | Percent Difference Compared with Control | P | Percent Change in Intervention | Percent Change in Control | Percent Difference Compared with Control | P | Percent Change in Intervention | Percent Change in Control | Percent Difference Compared with Control | P | ||||
| Curtis et al., 2009 [26] | H | 500 | Healthy | 0.00 | −5.71 | 5.71 | NS | 0.00 | 0.00 | 0.00 | NS | 1.85 | −3.64 | 5.49 | NS |
| Gurrola-Díaz et al., 2010 [15] | A | 19.24 | Healthy | −4.12 | #### | 10.73 | NR | 3.88 | 0.86 | 3.03 | NR | −4.58 | −10.45 | 5.87 | NR |
| Hansen et al., 2005, full [16] | A | 71 or 48 | Healthy | 0.93 | −1.26 | 2.19 | 0.643 | −6.11 | −9.70 | 3.59 | <0.001 | −1.48 | −5.59 | 4.10 | 0.405 |
| Hansen et al., 2005, half [16] | A | 36 or 24 | Healthy | 3.42 | −1.26 | 4.68 | 0.643 | −6.11 | −9.70 | 3.59 | <0.001 | −1.36 | −5.59 | 4.22 | 0.405 |
| Karlsen et al., 2007 [19] | A | 300 | Healthy | — | — | — | — | −1.67 | −2.63 | 0.96 | NS | −0.16 | −2.38 | 2.22 | NS |
| Gurrola-Díaz et al., 2010 [15] | A | 19.24 | MetS | −1.81 | 2.17 | −3.98 | NS | 30.06 | 23.47 | 6.59 | 0.002 | 1.10 | 6.96 | −5.86 | 0.019 |
| Hassellund et al., 2013 [18] | A | 640 | Prehypertensive | ND | ND | ND | 0.341 | ND | ND | ND | 0.043 | ND | ND | ND | 0.432 |
| Kianbakht et al., 2014 [20] | A | 7.35 | Hyperlipidemic | −32.04 | −9.12 | −22.92 | 0.002 | 36.63 | 2.52 | 34.11 | <0.001 | −28.29 | −2.76 | −25.53 | <0.001 |
| Naruszewicz et al., 2007 [14] | A | ~64 | Post-MI | −0.34 | −5.82 | 5.48 | NS | 2.84 | 1.75 | 1.09 | NS | 0.91 | −3.07 | 3.98 | NS |
| Qin et al., 2009 [21] | H | 320 | Dyslipidemic | −12.12 | −0.76 | −11.37 | <0.001 | 11.55 | 1.74 | 9.81 | <0.001 | −2.52 | −0.85 | −1.67 | 0.435 |
| Soltani et al., 2014 [22] | H | 90 | Hyperlipidemic | −8.61 | 2.71 | −11.32 | 0.004 | −0.35 | −1.89 | 1.54 | 0.631 | −15.21 | 1.51 | −16.71 | <0.001 |
| Zhu et al., 2013 [24] | A | 320 | Hyperlipidemic | −10.42 | 0.30 | −10.72 | 0.030 | 12.30 | −0.81 | 13.10 | 0.036 | −4.19 | −3.55 | −0.64 | 0.556 |
3.3. Triglycerides
| Reference | SIGN Quality | CVD-Related Disease Status | Anthocyanin Dose (mg/Day) | Triglycerides (mg/dL) | |||
|---|---|---|---|---|---|---|---|
| Percent Change in Intervention | Percent Change in Control | Percent Difference Compared with Control | P | ||||
| Curtis et al., 2009 [26] | H | Healthy | 500 | 11.11 | 11.11 | 0.00 | NS |
| Gurrola-Díaz et al., 2010 [15] | A | Healthy | 19.24 | −8.24 | −19.73 | 11.50 | NR |
| Gurrola-Díaz et al., 2010 [15] | A | MetS | 19.24 | −37.94 | −17.04 | −20.91 | NS |
| Hassellund et al., 2013 [18] | A | Prehypertension | 640 | ND | ND | ND | 0.127 |
| Kianbakht et al., 2014 [20] | A | Hyperlipidemic | 7.35 | −18.67 | −9.68 | −8.99 | 0.002 |
| Naruszewicz et al., 2007 [14] | A | Post-MI | 64 | −6.15 | −3.49 | −2.66 | NS |
| Qin et al., 2009 [21] | H | Dyslipidemic | 320 | −4.24 | −2.62 | −1.62 | 0.576 |
| Soltani et al., 2014 [22] | H | Hyperlipidemic | 90 | −30.79 | 3.76 | −34.55 | <0.001 |
| Zhu et al., 2013 [24] | A | Hyperlipidemic | 320 | −4.08 | −2.90 | −1.18 | 0.462 |
3.4. Blood Pressure
| Reference | SIGN Quality | CVD-Related Disease Status | Anthocyanin Dose (mg/Day) | Systolic Blood Pressure (mmHg) | Diastolic Blood Pressure (mmHg) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Percent Change in Intervention | Percent Change in Control | Percent Difference Compared with Control | P | Percent Change in Intervention | Percent Change in Control | Percent Difference Compared with Control | P | ||||
| Curtis et al., 2009 [26] | H | Healthy | 500 | 0.81 | −4.62 | 5.43 | NR | −1.28 | −2.44 | 1.16 | NR |
| Gurrola-Díaz et al., 2010 [15] | A | Healthy | 19.2 | ND | −2.09 | ND | NS | ND | −2.62 | ND | NS |
| Hansen et al., 2005, full [16] | A | Healthy | 71 or 48 | −4.48 | −3.13 | −1.35 | 0.605 | −3.66 | −5.00 | 1.34 | 0.261 |
| Hansen et al., 2005, half [16] | A | Healthy | 36 or 24 | −1.61 | −3.13 | 1.51 | 0.605 | −1.27 | −5.00 | 3.73 | 0.261 |
| Gurrola-Díaz et al., 2010 [15] | A | MetS | 19.2 | −5.57 | −9.04 | 3.47 | NS | −11.25 | −2.96 | −8.29 | NS |
| Hassellund et al., 2012 [17] | A | Prehypertension | 640 | −5.59 | −6.99 | 1.40 | 0.254 | −13.54 | −14.58 | 1.04 | 0.324 |
| Naruszewicz et al., 2007 [14] | A | Post-MI | 64 | −8.32 | 4.36 | −12.68 | <0.001 | −8.34 | 1.70 | −10.04 | <0.001 |
| Qin et al., 2009 [21] | H | Dyslipidemic | 320 | −0.95 | −3.33 | 2.38 | 0.888 | 0.00 | −0.97 | 0.97 | 0.343 |
| Zhu et al., 2011 [23] | A | Hyperlipidemic | 320 | −5.31 | −0.40 | −4.91 | 0.245 | −2.24 | −1.93 | −0.31 | 0.290 |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs). Fact Sheet No. 317. 2011. Available online: http://www.who.int/cardiovascular_diseases/en/ (accessed on 23 December 2014).
- US Department of Health and Human Services, US Department of Agriculture. Dietary Guidelines for Americans, 2010, 7th ed.US Government Printing Office: Washington, DC, USA, 2010.
- US Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. ODPHP Publication No. U0036; US Department of Health and Human Services: Washington, DC, USA, 2008.
- Basu, A.; Rhone, M.; Lyons, T.J. Berries: Emerging impact on cardiovascular health. Nutr. Rev. 2010, 66, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Jennings, A.; Welch, A.A.; Fairweather-Tait, S.J.; Kay, C.; Minihane, A.M.; Chowienczyk, P.; Jiang, B.; Cecelja, M.; Spector, T.; Macgregor, A.; et al. Higher anthocyanin intake is associated with lower arterial stiffness and central blood pressure in women. Am. J. Clin. Nutr. 2012, 96, 781–788. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Peterson, J.J.; Patel, R.; Jacques, P.F.; Shah, R.; Dwyer, J.T. Flavonoid intake and cardiovascular disease mortality in a prospective cohort of US adults. Am. J. Clin. Nutr. 2012, 95, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Mink, P.J.; Scrafford, C.G.; Barraj, L.M.; Harnack, L.; Hong, C.P.; Nettleton, J.A.; Jacobs, D.R., Jr. Flavonoid intake and cardiovascular disease mortality: A prospective study in postmenopausal women. Am. J. Clin. Nutr. 2007, 85, 895–909. [Google Scholar] [PubMed]
- Cassidy, A.; O’Reilly, É.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.P.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C. Anthocyanins in cardiovascular disease. Adv. Nutr. 2011, 2, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0. Available online: http://www.cochrane-handbook.org (accessed on 24 November 2014).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, A.H.; Yetley, E.A.; Lau, J. Application of systematic review methodology to the field of nutrition. J. Nutr. 2008, 138, 2297–2306. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Tricco, A.C. Issues related to the conduct of systematic reviews: a focus on the nutrition field. Am. J. Clin. Nutr. 2008, 88, 1191–1199. [Google Scholar] [PubMed]
- Naruszewicz, M.; Łaniewska, I.; Millo, B.; Dłużniewski, M. Combination therapy of statin with flavonoids rich extract from chokeberry fruits enhanced reduction in cardiovascular risk markers in patients after myocardial infarction (MI). Atherosclerosis 2007, 194, e179–e184. [Google Scholar] [CrossRef] [PubMed]
- Gurrola-Díaz, C.M.; García-López, P.M.; Sánchez-Enríquez, S.; Troyo-Sanromán, R.; Andrade-González, I.; Gómez-Leyva, J.F. Effects of Hibiscus sabdariffa extract powder and preventive treatment (diet) on the lipid profiles of patients with metabolic syndrome (MeSy). Phytomedicine 2010, 17, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.S.; Marckmann, P.; Dragsted, L.O.; Finné Nielsen, I.L.; Neilsen, S.E.; Grønbæk, M. Effect of red wine and red grape extract on blood lipids, haemostatic factors, and other risk factors for cardiovascular disease. Eur. J. Clin. Nutr. 2005, 59, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Hassellund, S.S.; Flaa, A.; Sandvik, L.; Kjeldsen, S.E.; Rostrup, M. Effects of anthocyanins on blood pressure and stress reactivity: A double-blind randomized placebo-controlled crossover study. J. Hum. Hypertens 2012, 26, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Hassellund, S.S.; Flaa, A.; Kjeldsen, S.E.; Seljeflot, I.; Karlsen, A.; Erlund, I.; Rostrup, M. Effects of anthocyanins on cardiovascular risk factors and inflammation in pre-hypertensive men: A double-blind randomized placebo-controlled crossover study. J. Hum. Hypertens 2013, 27, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, A.; Retterstøl, L.; Lakke, P.; Paur, I.; Kjølsrud-Bøhn, S.; Sandvik, L.; Blomhoff, R. Anthocyanins inhibit nuclear factor-κB activation in monocytes and reduce plasma concentrations of pro-inflammatory mediators in healthy adults. J. Nutr. 2007, 137, 1951–1954. [Google Scholar] [PubMed]
- Kianbakht, S.; Abasi, B.; Dabaghian, F.H. Improved lipid profile in hyperlipidemic patients taking Vaccinium arctostaphylos fruit hydroalcoholic extract: A randomized double-blind placebo-controlled clinical trial. Phytother. Res. 2014, 28, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Xia, M.; Ma, J.; Hao, Y.T.; Liu, J.; Mou, H.Y.; Cao, L.; Ling, W. Anthocyanin supplementation improves serum LDL- and HDL-cholesterol concentrations associated with the inhibition of cholesteryl ester transfer protein in dyslipidemic subjects. Am. J. Clin. Nutr. 2009, 90, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Soltani, R.; Hakimi, M.; Asgary, S.; Ghanadian, S.M.; Keshvari, M.; Sarrafzadegan, N. Evaluation of the effects of Vaccinium arctostaphylos L. fruit extract on serum lipids and hs-CRP levels and oxidative stress in adult patients with hyperlipidemia: A randomized, double-blind, placebo-controlled clinical trial. Evid. Based Complement. Altern. Med. 2014, 2014, 217451. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xia, M.; Yang, Y.; Liu, F.; Li, Z.; Hao, Y.; Mi, M.; Jin, T.; Ling, W. Purified anthocyanin supplementation improves endothelial function via NO-cGMP activation in hypercholesterolemic individuals. Clin. Chem. 2011, 57, 1524–1533. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Ling, W.; Guo, H.; Song, F.; Ye, Q.; Zou, T.; Li, D.; Zhang, Y.; Li, G.; Xiao, Y.; et al. Anti-inflammatory effect of purified dietary anthocyanin in adults with hypercholesterolemia: A randomized controlled trial. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Scottish Intercollegiate Guidelines Network (SIGN). Methodology Checklist 2: Randomized Controlled Trials. Available online: http://www.sign.ac.uk/methodology/checklists.html (accessed on 6 March 2015).
- Curtis, P.J.; Kroon, P.A.; Hollands, W.J.; Walls, R.; Jenkins, G.; Kay, C.D.; Cassidy, A. Cardiovascular disease risk biomarkers and liver and kidney function are not altered in postmenopausal women after ingesting an elderberry extract rich in anthocyanins for 12 weeks. J. Nutr. 2009, 139, 2266–2271. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, I.; Kobayashi, M.; Hamada, T.; Tsuda, K.; Goto, H.; Imaizumi, K.; Nozawa, A.; Sugimoto, A.; Kakuda, T. Heat-epimerized tea catechins rich in gallocatechin gallate and catechin gallate are more effective to inhibit cholesterol absorption than tea catechins rich in epigallocatechin gallate and epicatechin gallate. J. Agric. Food Chem. 2003, 51, 7303–7307. [Google Scholar] [CrossRef] [PubMed]
- Takikawa, M.; Inoue, S.; Horio, F.; Tsuda, T. Dietary anthocyanin-rich bilberry extract ameliorates hyperglycemia and insulin sensitivity via activation of AMP-activated protein kinase in diabetic mice. J. Nutr. 2010, 140, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Liu, G.; Zhong, R.; Wang, Y.; Wang, D.; Xia, M. Cyanidin-3-O-β-glucoside regulates fatty acid metabolism via an AMP-activated protein kinase-dependent signaling pathway in human HepG2 cells. Lipids Health Dis. 2012, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Towler, M.C.; Hardie, D.G. AMP-activated protein kinase in metabolic control and insulin signaling. Circ. Res. 2007, 100, 328–341. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, J.H.; Gheewala, N.M.; O’Keefe, J.O. Dietary strategies for improving post-prandial and lipid profile in patients suffering from coronary artery disease. Expert. Opin. Ther. Targets 2008, 51, 249–255. [Google Scholar]
- Basu, A.; Wilkinson, M.; Penugonda, K.; Simmons, B.; Betts, N.M.; Lyons, T.J. Freeze-dried strawberry powder improves lipid profile and lipid peroxidation in women with metabolic syndrome: Baseline and post intervention effects. Nutr. J. 2009, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Erlund, I.; Koli, R.; Alfthan, G. Favorable effects of berry consumption on platelet function, blood pressure, and HDL cholestrol. Am. J. Clin. Nutr. 2008, 87, 323–331. [Google Scholar] [PubMed]
- McAnulty, S.R.; McAnulty, L.S.; Morrow, J.D. Effect of daily fruit ingestion on angiotensin converting enzyme activity, blood pressure, and oxidative stress in chronic smokers. Free Radic. Res. 2005, 39, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.T.; Chan, Y.C.; Lin, C.W.; Lee, W.J.; Sheu, W.H. Effect of cranberry extracts on lipid profiles in subjects with type-2 diabetes. Diabet. Med. 2008, 25, 1473–1477. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wallace, T.C.; Slavin, M.; Frankenfeld, C.L. Systematic Review of Anthocyanins and Markers of Cardiovascular Disease. Nutrients 2016, 8, 32. https://doi.org/10.3390/nu8010032
Wallace TC, Slavin M, Frankenfeld CL. Systematic Review of Anthocyanins and Markers of Cardiovascular Disease. Nutrients. 2016; 8(1):32. https://doi.org/10.3390/nu8010032
Chicago/Turabian StyleWallace, Taylor C., Margaret Slavin, and Cara L. Frankenfeld. 2016. "Systematic Review of Anthocyanins and Markers of Cardiovascular Disease" Nutrients 8, no. 1: 32. https://doi.org/10.3390/nu8010032