Association between Low Dietary Protein Intake and Geriatric Nutrition Risk Index in Patients with Chronic Kidney Disease: A Retrospective Single-Center Cohort Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Assessment of Body Composition
2.3. Endpoints
2.4. Statistical Analyses
3. Results
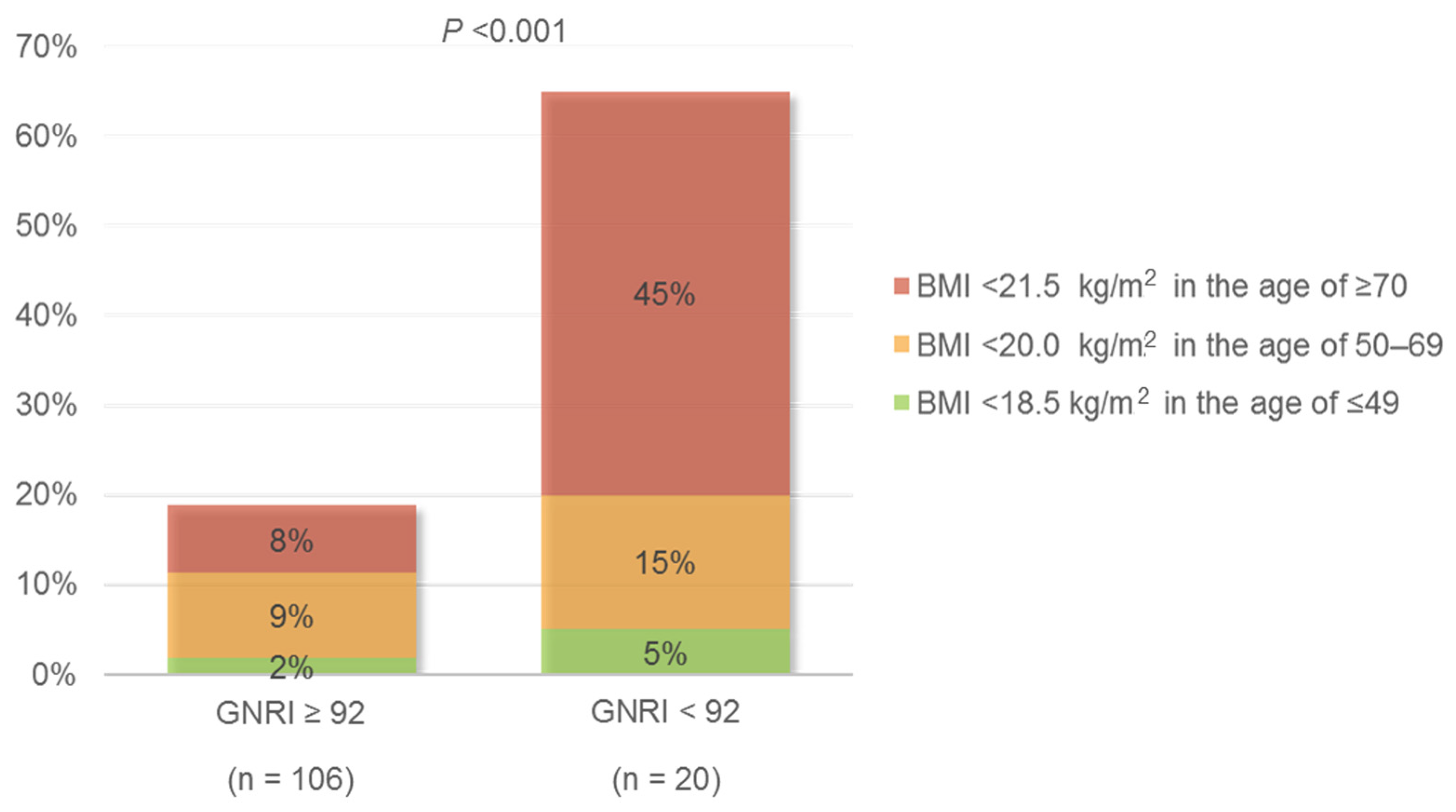
3.1. Patient Characteristics at the Time of Dietary Nutrient Assessment
3.2. Dietary Intake of Sodium, Protein, and Energy at the Time of Dietary Nutrient Assessment
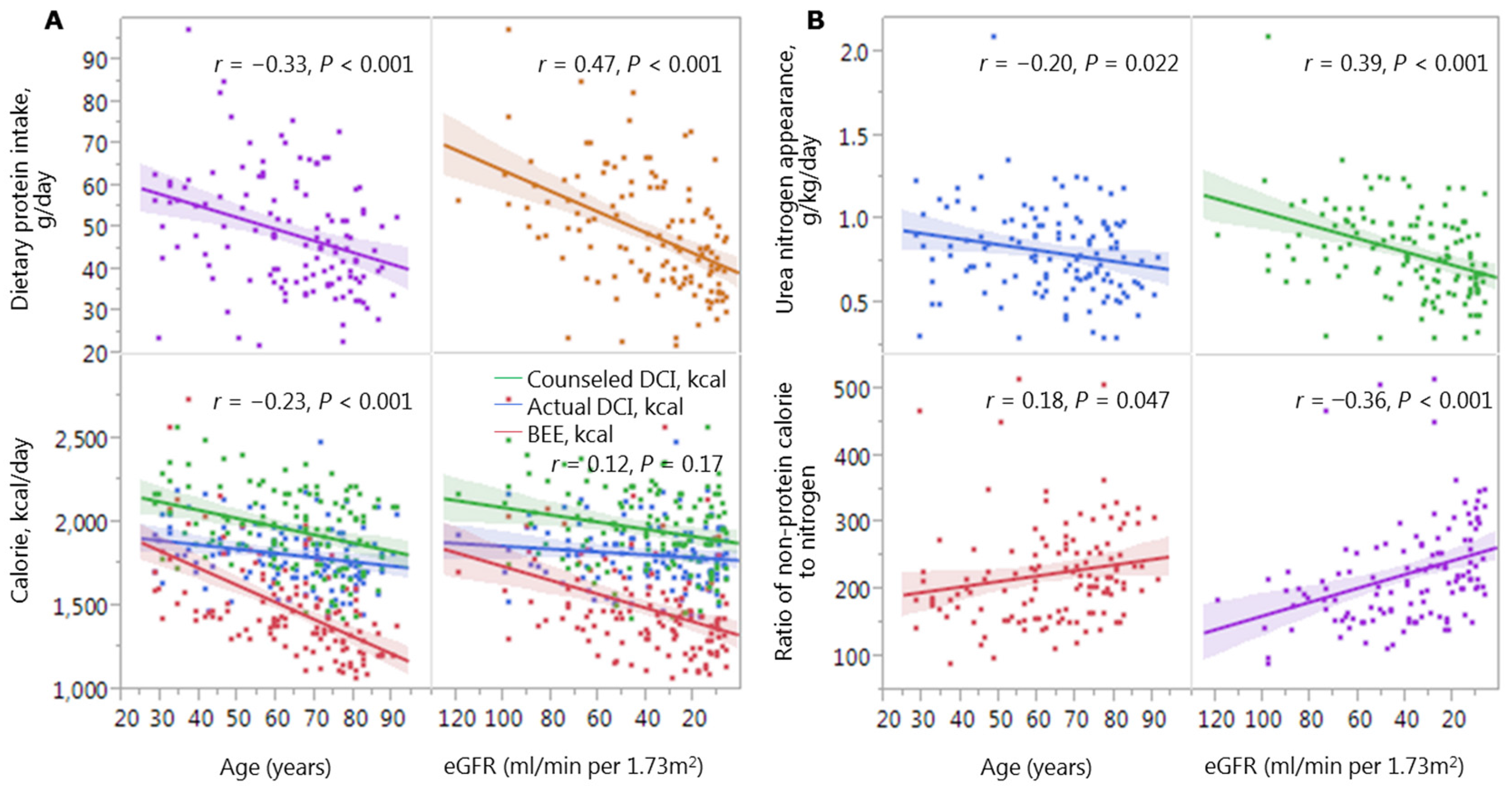
3.3. Associations of Protein and Calorie Intake with Age and Kidney Function
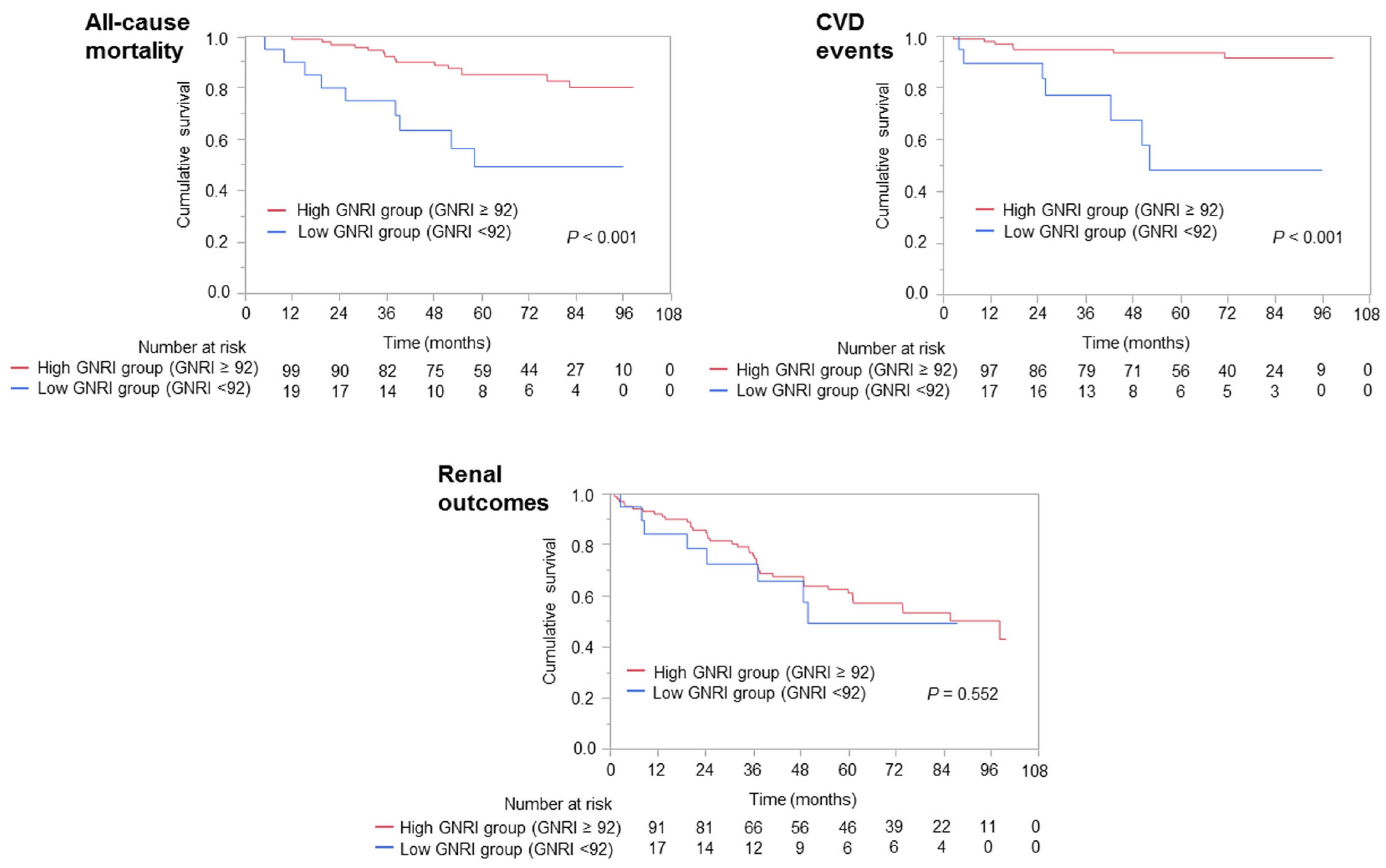
3.4. Associations of GNRI with All-Cause Mortality, Cardiovascular Events, and Adverse Renal Outcomes
3.5. Independent Factors Associated with GNRI < 92
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BEE | basal energy expenditure |
| BIA | bioimpedance analysis |
| BMI | body mass index |
| CKD | chronic kidney disease |
| CI | confidence interval |
| Cr | serum creatinine |
| ECW | extracellular water |
| eGFR | estimated glomerular filtration rate |
| GNRI | geriatric nutritional risk index |
| HR | hazard ratio |
| ICW | intracellular water |
| MDRD | Modification of Diet in Renal Disease |
| NPC/N | non-protein calorie to nitrogen |
| PEW | protein-energy wasting |
| TBW | total body water |
| UNA | urea nitrogen appearance |
| UPCR | urinary protein-to-creatinine ratio |
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. Chapter 3: Management of Progression and Complications of CKD. Kidney Int. Suppl. 2013, 3, 73–90. [Google Scholar]
- Cano, N.; Fiaccadori, E.; Tesinsky, P.; Toigo, G.; Druml, W.; German Society for Nutritional Medicine (DGEM); Kuhlmann, M.; Mann, H.; Horl, W.H.; European Society for Parenteral and Enteral Nutrition (ESPEN). ESPEN guidelines on enteral nutrition: Adult renal failure. Clin. Nutr. 2006, 25, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, M.; Bellizzi, V.; Chauveau, P.; Cupisti, A.; Ecder, T.; Fouque, D.; Garneata, L.; Lin, S.; Mitch, W.E.; Teplan, V.; et al. KETO acid therapy in predialysis chronic kidney disease patients: Final consensus. J. Ren. Nutr. 2012, 22, S22–S24. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, M.; Bellizzi, V.; Chauveau, P.; Cupisti, A.; Ecder, T.; Fouque, D.; Garneata, L.; Lin, S.; Mitch, W.E.; Teplan, V.; et al. Protein-restricted diets plus KETO/AMINO acids—A valid therapeutic approach for chronic kidney disease patients. J. Ren. Nutr. 2012, 22, S1–S21. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, V.; Cupisti, A.; Locatelli, F.; Bolasco, P.; Brunori, G.; Cancarini, G.; Caria, S.; de Nicola, L.; di Iorio, B.R.; di Micco, L.; et al. Low-protein diets for chronic kidney disease patients: The Italian experience. BMC Nephrol. 2016, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Tamakoshi, A.; Yatsuya, H.; Lin, Y.; Tamakoshi, K.; Kondo, T.; Suzuki, S.; Yagyu, K.; Kikuchi, S.; JACC Study Group. Bmi and all-cause mortality among japanese older adults: Findings from the Japan collaborative cohort study. Obesity 2010, 18, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Kuriyama, S.; Kakizaki, M.; Ohmori-Matsuda, K.; Sugawara, Y.; Sone, T.; Hozawa, A.; Tsuji, I. Effect of age on the association between body mass index and all-cause mortality: The Ohsaki cohort study. J. Epidemiol. 2010, 20, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, T.; Sairenchi, T.; Iso, H.; Irie, F.; Tanaka, K.; Fukasawa, N.; Ota, H.; Muto, T. Age- and gender-specific bmi in terms of the lowest mortality in Japanese general population. Obesity 2008, 16, 2348–2355. [Google Scholar] [CrossRef] [PubMed]
- Kuriyama, S.; Ohmori, K.; Miura, C.; Suzuki, Y.; Nakaya, N.; Fujita, K.; Sato, Y.; Tsubono, Y.; Tsuji, I.; Fukao, A.; et al. Body mass index and mortality in Japan: The MIYAGI cohort study. J. Epidemiol. 2004, 14, S33–S38. [Google Scholar] [CrossRef] [PubMed]
- Tsugane, S.; Sasaki, S.; Tsubono, Y. Under- and overweight impact on mortality among middle-aged Japanese men and women: A 10-year follow-up of JPHC study cohort. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M.; Babazono, A.; Ishii, T.; Sugie, T.; Momose, Y.; Iwahashi, M.; Une, H. Effects of low body mass index and smoking on all-cause mortality among middle-aged and elderly Japanese. J. Epidemiol./Jpn. Epidemiol. Assoc. 2002, 12, 40–44. [Google Scholar] [CrossRef]
- Sasazuki, S.; Inoue, M.; Tsuji, I.; Sugawara, Y.; Tamakoshi, A.; Matsuo, K.; Wakai, K.; Nagata, C.; Tanaka, K.; Mizoue, T.; et al. Body mass index and mortality from all causes and major causes in Japanese: Results of a pooled analysis of 7 large-scale cohort studies. J Epidemiol. 2011, 21, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Overview of Dietary Reference Intakes for Japanese (2015). Available online: http://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/Overview.pdf (accessed on 18 October 2016).
- Ikizler, T.A.; Cano, N.J.; Franch, H.; Fouque, D.; Himmelfarb, J.; Kalantar-Zadeh, K.; Kuhlmann, M.K.; Stenvinkel, P.; TerWee, P.; Teta, D.; et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: A consensus statement by the international society of renal nutrition and metabolism. Kidney Int. 2013, 84, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric nutritional risk index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [PubMed]
- Cereda, E.; Limonta, D.; Pusani, C.; Vanotti, A. Assessing elderly at risk of malnutrition: The new geriatric nutritional risk index versus nutritional risk index. Nutrition 2006, 22, 680–682. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [PubMed]
- Calhoun, D.A.; Jones, D.; Textor, S.; Goff, D.C.; Murphy, T.P.; Toto, R.D.; White, A.; Cushman, W.C.; White, W.; Sica, D.; et al. Resistant hypertension: Diagnosis, evaluation, and treatment. A scientific statement from the American heart association professional education committee of the council for high blood pressure research. Hypertension 2008, 51, 1403–1419. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 Report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Prevalence of gout and hyperuricemia in the US general population: The national health and nutrition examination survey 2007–2008. Arthritis Rheum. 2011, 63, 3136–3141. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, J.A.; Benedict, F.G. A biometric study of human basal metabolism. Proc. Natl. Acad. Sci. USA 1918, 4, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Klersy, C.; Pedrolli, C.; Cameletti, B.; Bonardi, C.; Quarleri, L.; Cappello, S.; Bonoldi, A.; Bonadeo, E.; Caccialanza, R. The geriatric nutritional risk index predicts hospital length of stay and in-hospital weight loss in elderly patients. Clin. Nutr. 2015, 34, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C. The geriatric nutritional risk index. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Izawa, K.P.; Watanabe, S.; Oka, K.; Mogamiya, T.; Tada, M.; Nakata, S.; Nitobe, S.; Yoshizawa, K.; Hirano, Y.; Osada, N.; et al. Differences in physical performance based on the geriatric nutritional risk index in elderly female cardiac patients. Aging Clin. Exp. Res. 2015, 27, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Cha, K.; Brown, E.F.; Wilmore, D.W. A new bioelectrical impedance method for measurement of the erythrocyte sedimentation rate. Physiol. Meas. 1994, 15, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Lammersfeld, C.A.; Vashi, P.G.; King, J.; Dahlk, S.L.; Grutsch, J.F.; Lis, C.G. Bioelectrical impedance phase angle as a prognostic indicator in breast cancer. BMC Cancer 2008, 8, 249. [Google Scholar] [CrossRef] [PubMed]
- Amraoui, F.; Bos, S.; Vogt, L.; van den Born, B.J. Long-term renal outcome in patients with malignant hypertension: A retrospective cohort study. BMC Nephrol. 2012, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Parsa, A.; Kao, W.H.; Xie, D.; Astor, B.C.; Li, M.; Hsu, C.Y.; Feldman, H.I.; Parekh, R.S.; Kusek, J.W.; Greene, T.H.; et al. Apol1 risk variants, race, and progression of chronic kidney disease. N. Engl. J. Med. 2013, 369, 2183–2196. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Laville, M. Low protein diets for chronic kidney disease in non diabetic adults. Cochrane Database Syst. Rev. 2006. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Greene, J.H.; Wingard, R.L.; Parker, R.A.; Hakim, R.M. Spontaneous dietary protein intake during progression of chronic renal failure. J. Am. Soc. Nephrol. 1995, 6, 1386–1391. [Google Scholar] [PubMed]
- Wallace, J.I.; Schwartz, R.S.; LaCroix, A.Z.; Uhlmann, R.F.; Pearlman, R.A. Involuntary weight loss in older outpatients: Incidence and clinical significance. J. Am. Geriatr. Soc. 1995, 43, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, F.R.; Safran, C.; Levkoff, S.E.; Minaker, K.L. Serum albumin level on admission as a predictor of death, length of stay, and readmission. Arch. Intern. Med. 1992, 152, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Owen, W.F., Jr.; Lew, N.L.; Liu, Y.; Lowrie, E.G.; Lazarus, J.M. The urea reduction ratio and serum albumin concentration as predictors of mortality in patients undergoing hemodialysis. N. Engl. J. Med. 1993, 329, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Bills, J.E.; Light, R.P. Diagnosing obesity by body mass index in chronic kidney disease: An explanation for the “obesity paradox?”. Hypertension 2010, 56, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Cooper, B.A.; Penne, E.L.; Bartlett, L.H.; Pollock, C.A. Protein malnutrition and hypoalbuminemia as predictors of vascular events and mortality in ESRD. Am. J. Kidney Dis. 2004, 43, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Steinman, T.I. Serum albumin: Its significance in patients with ESRD. Semin. Dial. 2000, 13, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Torino, C.; Tripepi, G.; Mallamaci, F. Assessment of obesity in chronic kidney disease: What is the best measure? Curr. Opin. Nephrol. Hypertens. 2012, 21, 641–646. [Google Scholar] [CrossRef] [PubMed]
- White, J.V.; Guenter, P.; Jensen, G.; Malone, A.; Schofield, M.; Academy of Nutrition and Dietetics Malnutrition Work Group; A.S.P.E.N. Malnutrition Task Force; A.S.P.E.N. Board of Directors. Consensus Statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: Characteristics Recommended for the Identification and Documentation of Adult Malnutrition (Undernutrition). J. Parenter. Enteral. Nutr. 2012, 36, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, Y.; Saito, A.; Yamazaki, K.; Tai, R.; Matsukiyo, T.; Aikawa, A.; Sakai, K. Brain natriuretic peptide and body fluid composition in patients with chronic kidney disease: A cross-sectional study to evaluate the relationship between volume overload and malnutrition. Cardiorenal. Med. 2016, 6, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, Y.; Tai, R.; Aoki, T.; Mizuiri, S.; Ogura, T.; Tanaka, Y.; Okada, T.; Aikawa, A.; Sakai, K. The associations of malnutrition and aging with fluid volume imbalance between intra- and extracellular water in patients with chronic kidney disease. J. Nutr. Health Aging 2015, 19, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C. Biological indexes considered in the derivation of the bioelectrical impedance analysis. Am. J. Clin. Nutr. 1996, 64, 397S–404S. [Google Scholar] [PubMed]
- Beberashvili, I.; Azar, A.; Sinuani, I.; Shapiro, G.; Feldman, L.; Stav, K.; Sandbank, J.; Averbukh, Z. Bioimpedance phase angle predicts muscle function, quality of life and clinical outcome in maintenance hemodialysis patients. Eur. J. Clin. Nutr. 2014, 68, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Da, J.; Xie, X.; Wolf, M.; Disthabanchong, S.; Wang, J.; Zha, Y.; Lv, J.; Zhang, L.; Wang, H. Serum phosphorus and progression of CKD and mortality: A meta-analysis of cohort studies. Am. J. Kidney Dis. 2015, 66, 258–265. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Low or No Nutrition-Related Risk (GNRI ≥ 92) n = 106 (84.1%) | Moderate or Severe Nutrition-Related Risk (GNRI < 92) n = 20 (15.9%) | p-Value |
|---|---|---|---|
| Age, years | 62.1 ± 16.3 | 69.7 ± 14.3 | 0.043 |
| Sex, male, n (%) | 55 (51.9) | 10 (50.0) | 0.88 |
| Time from first visit to the dietary clinic to the day of dietary recording, days | 1829 ± 1691 | 1981 ± 1706 | 0.72 |
| Height, cm | 160 ± 10 | 156 ± 10 | 0.09 |
| Weight, kg | 60 ± 13 | 48 ± 7 | <0.001 |
| Body mass index, kg/m2 | 23.3 ± 3.8 | 19.6 ± 2.1 | <0.001 |
| Underling kidney disease | |||
| Glomerulonephritis, n (%) | 45 (42.5) | 7 (35.0) | 0.94 |
| Diabetes mellitus, n (%) | 14 (13.2) | 4 (20.0) | |
| Nephrosclerosis, n (%) | 22 (20.8) | 4 (20.0) | |
| Others/Unknown, n (%) | 25 (23.5) | 5 (25.0) | |
| Systolic BP, mmHg | 124 ± 16 | 123 ± 14 | 0.85 |
| Diastolic BP, mmHg | 72 ± 9 | 67 ± 11 | 0.10 |
| Resistant high blood pressure, n (%) | 23 (21.7) | 5 (25.0) | 0.74 |
| Pulse pressure, mmHg | 52 ± 12 | 56 ± 13 | 0.21 |
| Blood urea nitrogen, mg/dL | 29 ± 17 | 29 ± 17 | 0.87 |
| Serum creatinine, mg/dL | 1.97 ± 1.44 | 1.98 ± 1.34 | 0.99 |
| eGFRMDRD, mL/min per 1.73 m2 | 40 ± 27 | 36 ± 24 | 0.48 |
| GFR categories in KDIGO 2012 | |||
| G1 or 2, n (%) | 26 (24.5) | 3 (15.0) | 0.56 |
| G3a or G3b, n (%) | 34 (32.1) | 7 (35.0) | |
| G4, n (%) | 23 (21.7) | 7 (35.0) | |
| G5, n (%) | 23 (21.7) | 3 (15.0) | |
| Serum albumin, mg/dL | 4.0 ± 0.4 | 3.3 ± 0.4 | <0.001 |
| Total cholesterol, mg/dL | 193 ± 31 | 189 ± 56 | 0.76 |
| Triglyceride, mg/dL | 140 ± 84 | 120 ± 61 | 0.21 |
| Fasting blood glucose, mg/dL | 118 ± 36 | 148 ± 48 | 0.09 |
| Uric acid > 7.0 mg/dL in males or >6.0 mg/dL in females, n (%) | 60 (57.1) | 16 (80.0) | 0.06 |
| Calcium, mg/dL | 8.7 ± 0.6 | 8.7 ± 0.6 | 0.65 |
| Phosphorus, mg/dL | 3.4 ± 0.7 | 3.4 ± 0.6 | 0.65 |
| C-reactive protein, mg/dL | 0.2 ± 0.8 | 0.4 ± 0.6 | 0.43 |
| Hemoglobin, g/dL | 12.3 ± 2.0 | 11.1 ± 1.5 | 0.006 |
| UPCR, g/g Cr | 0.8 ± 1.3 | 1.8 ± 2.1 | 0.045 |
| Urea nitrogen appearance, g/kg per day | 0.84 ± 0.20 | 0.89 ± 0.31 | 0.53 |
| Patients Characteristics | No Nutrition-Related Risk (GNRI ≥ 92) n = 106 (84.1%) | Nutrition-Related Risk (GNRI < 92) n = 20 (15.9%) | p-Value |
|---|---|---|---|
| Sodium intake, mg/day | 3077 ± 1,210 | 2942 ± 1,139 | 0.65 |
| Sodium intake per BW, mg/kg/day | 52 ± 19 | 64 ± 26 | 0.07 |
| Protein intake, g/day | 47 ± 15 | 41 ± 15 | 0.09 |
| Protein intake per BW, g/kg/day | 0.80 ± 0.24 | 0.87 ± 0.35 | 0.37 |
| Protein intake per ideal BW g/standard weight/day | 0.83 ± 0.26 | 0.77 ± 0.29 | 0.36 |
| Calorie intake, kcal/day | 1819 ± 189 | 1763 ± 129 | 0.11 |
| Calorie intake per BW, kcal/kg/day | 31 ± 5 | 38 ± 4 | <0.001 |
| Calorie intake per ideal BW, kcal/standard weight/day | 32 ± 3 | 33 ± 3 | 0.19 |
| Ratio of non-protein calories to nitrogen | 218 ± 71 | 261 ± 86 | 0.043 |
| Basal energy expenditure, kcal | 1530 ± 285 | 1270 ± 140 | <0.001 |
| Variables | HR (95% CI) | p-Value |
|---|---|---|
| All-cause death | ||
| Unadjusted | 3.87 (1.62–8.72) | 0.003 |
| Age-adjusted | 3.91 (1.62–8.94) | 0.003 |
| Multivariable-adjusted a | 5.95 (1.94–18.04) | 0.002 |
| Cardiovascular disease event | ||
| Unadjusted | 8.26 (2.73–25.84) | <0.001 |
| Age-adjusted | 13.44 (3.99–50.51) | 0.001 |
| Multivariable-adjusted b | 9.48 (2.47–44.31) | <0.001 |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age, per 10 years of age | 0.77 (0.54–1.05) | 0.12 | 0.85 (0.57–1.20) | 0.36 |
| UPCR, g/g Cr | 0.69 (0.51–0.92) | 0.01 | 0.71 (0.52–0.96) | 0.03 |
| Uric acid > 7.0 mg/dL in males or >6.0 mg/dL in females | 2.89 (0.98–10.60) | 0.05 | 2.10 (0.66–8.12) | 0.21 |
| Ratio of non-protein calorie to nitrogen, per 10 units | 0.94 (0.88–0.99) | 0.02 | 0.93 (0.87–0.99) | 0.04 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiuchi, A.; Ohashi, Y.; Tai, R.; Aoki, T.; Mizuiri, S.; Ogura, T.; Aikawa, A.; Sakai, K. Association between Low Dietary Protein Intake and Geriatric Nutrition Risk Index in Patients with Chronic Kidney Disease: A Retrospective Single-Center Cohort Study. Nutrients 2016, 8, 662. https://doi.org/10.3390/nu8100662
Kiuchi A, Ohashi Y, Tai R, Aoki T, Mizuiri S, Ogura T, Aikawa A, Sakai K. Association between Low Dietary Protein Intake and Geriatric Nutrition Risk Index in Patients with Chronic Kidney Disease: A Retrospective Single-Center Cohort Study. Nutrients. 2016; 8(10):662. https://doi.org/10.3390/nu8100662
Chicago/Turabian StyleKiuchi, Aki, Yasushi Ohashi, Reibin Tai, Toshiyuki Aoki, Sonoo Mizuiri, Toyoko Ogura, Atsushi Aikawa, and Ken Sakai. 2016. "Association between Low Dietary Protein Intake and Geriatric Nutrition Risk Index in Patients with Chronic Kidney Disease: A Retrospective Single-Center Cohort Study" Nutrients 8, no. 10: 662. https://doi.org/10.3390/nu8100662