Iron-Folic Acid Supplementation During Pregnancy Reduces the Risk of Stunting in Children Less Than 2 Years of Age: A Retrospective Cohort Study from Nepal

Abstract
:1. Introduction
2. Methods
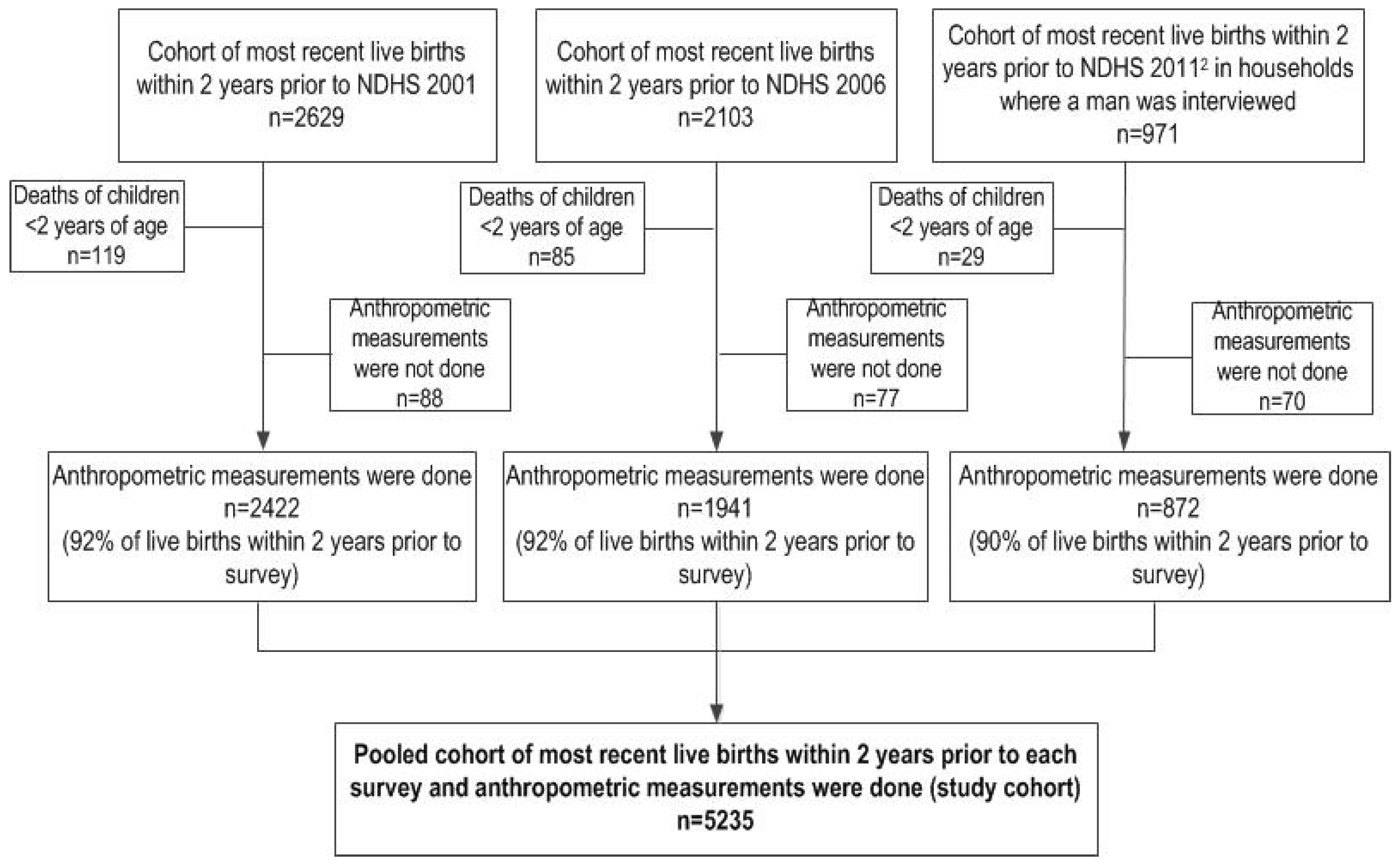
2.1. Study Design
2.2. Data Sources

2.3. Ethics
2.4. Study Outcomes
2.5. Exposure Variables and Potential Confounding Factors

{kind=link}
{kind=link}
| Variables | Definition and Categorization |
|---|---|
| Community-Level and Socioeconomic Status Factors | |
| Ecological region and place of residence | Ecological regions and place of residence of the respondent (1 = Terai region, urban; 2 = Terai region, rural; 3 = Hill region, urban; 4 = Hill region, rural; 5 = Mountain region, urban; and 6 = Mountain, rural). |
| Maternal marital status | Marital status of the mother (1 = currently married; and 2 = formerly married). |
| Maternal religion | Religion of the mother (1 = Hindu; 2 = Buddhist and others). |
| Maternal educational status | Maternal level of attained education (1 = secondary and above; 2 = completed primary; and 3 = no education). |
| Maternal occupation | Maternal employment status in the past 12 months prior to interview (1 = not working; 2 = working in agriculture; and 3 = working in non-agriculture). |
| Paternal educational status | Paternal level of attained education (1 = secondary and above; 2 = completed primary; and 3 = no education). |
| Paternal occupation | Paternal employment status in the past 12 months prior to interview (1 = working in non-agriculture; and 2 = working in agriculture). |
| Fuel used for cooking | Fuel used for cooking at home (1 = natural gas; and 2 = biomass energy) |
| Source of drinking water | Source of water used for drinking at home was classified based on WHO/UNICEF guidelines [17] (1 = improved; and 2 = unimproved). |
| Sanitation facilities | Sanitation refers to toilet facility at home was classified based on WHO/UNICEF guidelines [17] (1 = improved; and 2 = unimproved). |
| Pooled household wealth index | Composite index of household amenities using pooled NDHS data and a principal component analysis [18] of household assets. The wealth index was used to rank households across the 3 surveys into quintiles. |
| Maternal and child characteristics | |
| Maternal age at childbirth | Maternal age at childbirth (1 ≤ 20 years; 2 = 20–24 years; and 3 ≥ 25 years). |
| Maternal desire for pregnancy | Maternal intention to become pregnant (1 = wanted then; 2 = wanted later; and 3 = wanted no more). |
| Maternal smoking status | Current smoking status of mothers (1 = non-smokers; and 2 = smokers). |
| Maternal height | Height of mothers at the time of survey (1 = normal height, i.e., ≥145 cm; and 2 = short stature i.e., <145 cm). |
| Maternal perception of birth size | Subjective assessment of the respondent on the birth size (1 = average; 2 = very small; 3 = smaller than average; 4 = larger than average; and 5 = large). |
| Birth status | Birth status of the child (1 = singleton; 2 = multiple). |
| Birth rank and birth interval | Birth rank and birth interval of child (1 = 2nd or 3rd birth rank, birth interval >2 years; 2 = 1st birth rank; 3 = 2nd or 3rd birth rank, birth interval ≤2 years; 4 = ≥4th birth rank, birth interval >2 years; and 5 = ≥4th birth rank, birth interval ≤2 years). |
| Sex of child | Sex of the child (1 = male; and 2 = female). |
| Timing of initiation of breastfeeding | Timing of initiation of breastfeeding (1 = <1 h; 2= 1 to 24 h; 3 = >24 h; and 4 =never breastfed). |
| Duration of breastfeeding | Median duration of breastfeeding in months (as continous variable) |
| Age of child | Age of children in months (as continuous variable) |
| Child had diarrhoea during the last 2 weeks prior to interview | Child had diarrhoea within 2 weeks prior to the interview date (1 = no; and 2 = yes). |
| Perinatal health services variable | |
| Number of antenatal care (ANC) visits | Number of antenatal care visits (1 = no antenatal care visit; 2 = <4 antenatal care visits; and 3 = ≥4 antenatal care visits). |
2.6. Statistical Analysis
3. Results
| Study Cohort (NDHS 2001–2011) | |||
|---|---|---|---|
| Variables | n 1 | n 2 | % 2 |
| Year of Survey | |||
| 2001 | 2422 | 2452 | 47.1 |
| 2006 | 1941 | 1839 | 35.3 |
| 2011 | 872 | 916 | 17.6 |
| Community-level and socioeconomic factors | |||
| Ecological region and area of residence | |||
| Terai region, urban | 443 | 231 | 4.4 |
| Terai region, rural | 1973 | 2461 | 47.3 |
| Hill region, urban | 315 | 209 | 4.0 |
| Hill region, rural | 1683 | 1897 | 36.4 |
| Mountain region, urban | 46 | 5 | 0.2 |
| Mountain region, rural | 775 | 405 | 7.7 |
| Maternal marital status | |||
| Currently married | 5206 | 5175 | 99.4 |
| Formerly married | 29 | 32 | 0.6 |
| Maternal religion | |||
| Hindu | 4470 | 4377 | 84.0 |
| Buddhist and others | 765 | 830 | 16.0 |
| Maternal educational status | |||
| Secondary and above | 1175 | 1159 | 22.2 |
| Completed primary | 891 | 900 | 17.3 |
| No education | 3169 | 3148 | 60.5 |
| Maternal occupation | |||
| Not working | 1052 | 1200 | 23.0 |
| Working in agriculture | 3829 | 3673 | 70.5 |
| Working in non-agriculture | 353 | 333 | 6.4 |
| Missing | 1 | 1 | 0.1 |
| Paternal educational status | |||
| Secondary and above | 973 | 950 | 48.2 |
| Completed primary | 1962 | 1927 | 37.0 |
| No education | 2300 | 2330 | 44.8 |
| Paternal occupation | |||
| Working in non-agriculture | 2814 | 2820 | 54.2 |
| Working in agriculture | 2266 | 2229 | 42.8 |
| Missing | 155 | 158 | 3.0 |
| Fuel used for cooking | |||
| Natural gas | 468 | 465 | 8.9 |
| Biomass energy | 4375 | 4309 | 82.8 |
| Missing | 392 | 433 | 8.3 |
| Source of drinking water | |||
| Improved | 3777 | 3847 | 73.9 |
| Unimproved | 1065 | 926 | 17.8 |
| Missing | 393 | 434 | 8.3 |
| Sanitary facilities | |||
| Improved | 1689 | 1584 | 30.4 |
| Unimproved | 3154 | 3190 | 61.3 |
| Missing | 392 | 433 | 8.3 |
| Pooled household wealth index | |||
| Quintile 1 (Wealthiest) | 727 | 711 | 13.6 |
| Quintile 2 | 874 | 934 | 17.9 |
| Quintile 3 (Middle) | 957 | 966 | 18.6 |
| Quintile 4 | 989 | 957 | 18.4 |
| Quintile 5 (Poorest) | 1290 | 1199 | 23.0 |
| Missing | 398 | 440 | 8.5 |
| Maternal and child characteristics | |||
| Maternal age at child birth | |||
| <20 years | 3030 | 3050 | 58.6 |
| 20 to 24 years | 1878 | 1839 | 35.3 |
| ≥25 years | 327 | 318 | 6.1 |
| Maternal desire for pregnancy | |||
| Wanted then | 3403 | 3390 | 65.1 |
| Wanted later | 812 | 817 | 15.7 |
| Wanted no more | 1020 | 1000 | 19.2 |
| Maternal smoking status | |||
| Non-smokers | 4221 | 4252 | 81.7 |
| Smokers | 1014 | 955 | 18.3 |
| Maternal height | |||
| Normal height (≥145 cm) | 4523 | 4477 | 86.0 |
| Short stature (<145 cm) | 712 | 730 | 14.0 |
| Birth status | |||
| Singleton | 5200 | 5174 | 99.4 |
| Multiple | 35 | 33 | 0.6 |
| Birth rank and birth interval | |||
| 2nd/3rd birth rank, >2 years interval | 1650 | 1623 | 31.2 |
| 1st birth rank | 1469 | 1494 | 28.7 |
| 2nd/3rd birth rank, ≤2 years interval | 557 | 558 | 10.7 |
| ≥4th birth rank, >2 years interval | 1196 | 1179 | 22.6 |
| ≥4th birth rank, ≤2 years interval | 363 | 353 | 6.8 |
| Sex of child | |||
| Male | 2595 | 2583 | 49.6 |
| Female | 2640 | 2624 | 50.4 |
| Timing of initiation of breastfeeding | |||
| Never breastfed | 11 | 11 | 0.2 |
| <1 hours | 3013 | 2863 | 55.0 |
| 1 to 24 hours | 1169 | 1098 | 21.1 |
| >24 hours | 1041 | 1234 | 23.7 |
| Missing | 1 | 1 | 0.0 |
| Duration of breastfeeding (months) 4 | 21.0 (12.0, 23.0) | ||
| Age of children (months) 4 | 11.6 (±0.1) | ||
| Child had diarrhoea during the last 2 weeks prior to interview | |||
| No | 3978 | 3960 | 76.1 |
| Yes | 1257 | 1247 | 23.9 |
| Perinatal health services | |||
| Number of antenatal care visits | |||
| No antenatal care visit | 1805 | 1775 | 34.1 |
| <4 antenatal care visits | 1973 | 2023 | 38.8 |
| ≥4 antenatal care visits | 1457 | 1410 | 27.1 |

| Study Cohort | 2001 | 2006 | 2011 | |||
|---|---|---|---|---|---|---|
| Variables | n 1 | n 2 | % 2 | % 2 | % 2 | % 2 |
| Study exposure variables | ||||||
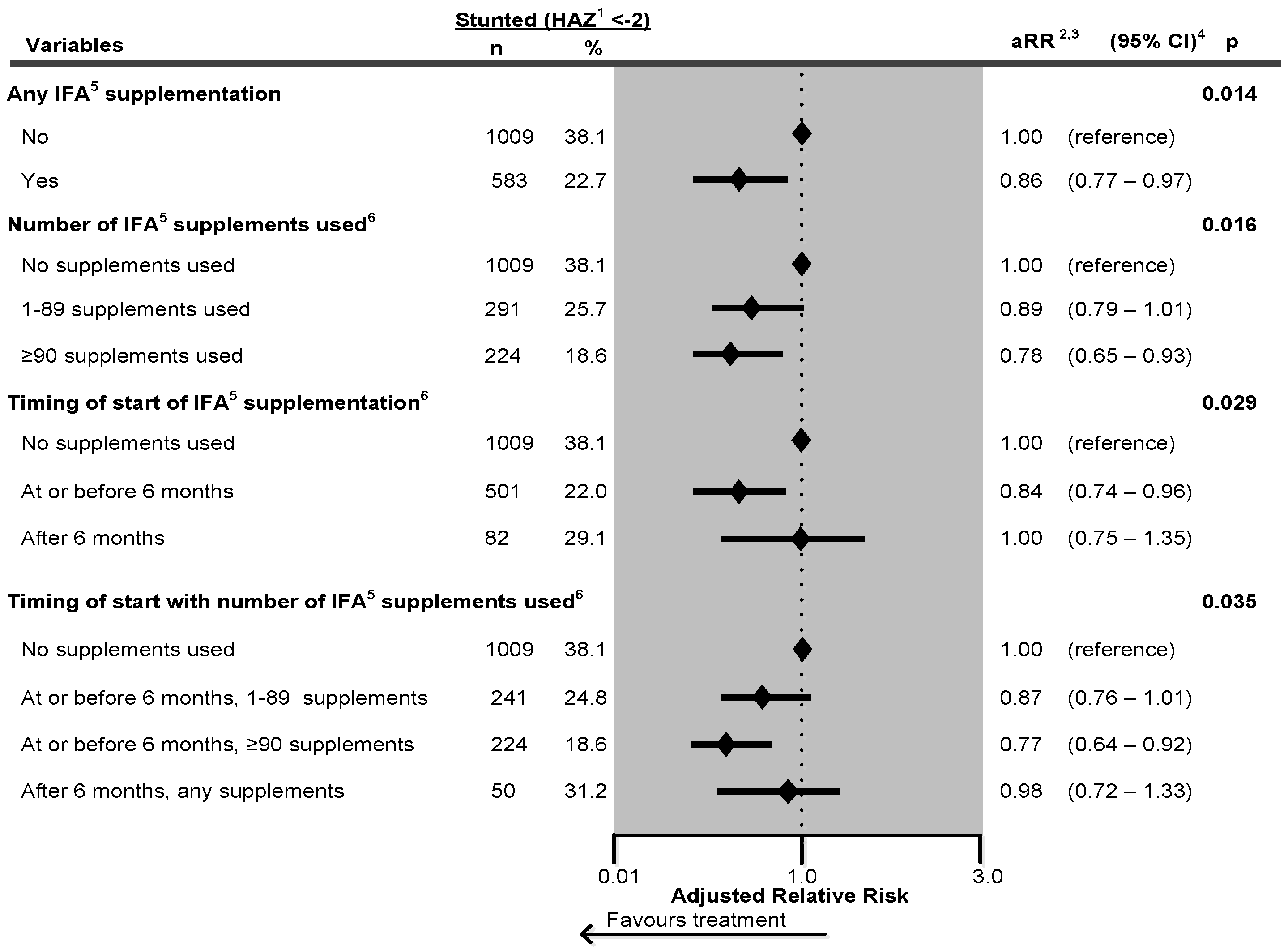
| Iron-folic acid (IFA) supplementation | ||||||
| No | 2675 | 2645 | 50.8 | 75.8 | 34.5 | 16.5 |
| Yes | 2560 | 2562 | 49.2 | 24.2 | 65.5 | 83.5 |
| Number of iron-folic acid (IFA) supplements used | ||||||
| No IFA supplementation | 2675 | 2645 | 50.8 | 75.8 | 34.5 | 16.5 |
| 1–89 supplements used | 1142 | 1133 | 21.8 | 16.3 | 30.3 | 19.3 |
| ≥90 supplements used | 1212 | 1206 | 23.1 | 5.6 | 30.0 | 56.4 |
| Missing | 206 | 223 | 4.3 | 2.3 | 5.2 | 7.7 |
| Timing of start of iron-folic acid (IFA) supplements during pregnancy | ||||||
| No IFA supplementation | 2675 | 2645 | 50.8 | 75.8 | 34.5 | 16.5 |
| At or before 6 months | 2289 | 2280 | 43.8 | 19.9 | 58.9 | 77.4 |
| After 6 months | 271 | 282 | 5.4 | 4.3 | 6.6 | 6.1 |
| Timing of start with number of iron-folic acid (IFA) supplements used during pregnancy | ||||||
| No IFA supplementation | 2675 | 2645 | 50.8 | 75.8 | 34.5 | 16.5 |
| At or before 6 months, 1–89 supplements used | 980 | 971 | 18.6 | 13.8 | 25.8 | 17.4 |
| At or before 6 months, ≥90 supplements used | 1212 | 1206 | 23.2 | 5.6 | 30.0 | 56.5 |
| After 6 months, any IFA supplements used | 162 | 162 | 3.1 | 2.5 | 4.4 | 1.9 |
| Missing | 206 | 223 | 4.3 | 2.3 | 5.2 | 7.7 |
| Study outcome variables | ||||||
| Stunting status of child | ||||||
| Not stunted | 3603 | 3616 | 69.4 | 64.7 | 71.6 | 77.8 |
| Stunted (HAZ 3 < −2) | 1632 | 1591 | 30.6 | 35.3 | 28.4 | 22.2 |
| Stunting status of child | ||||||
| Not severely stunted | 4706 | 4691 | 90.1 | 87.6 | 91.6 | 93.5 |
| Severely stunted (HAZ 3 <-3) | 529 | 516 | 9.9 | 12.4 | 8.4 | 6.5 |
| Maternal perception of birth size | ||||||
| Average or larger than average | 4080 | 4157 | 79.8 | 77.3 | 81.7 | 82.7 |
| Smaller than average | 1154 | 1047 | 20.1 | 22.7 | 18.3 | 17.0 |
| Missing | 1 | 3 | 0.1 | 0.0 | 0.0 | 0.3 |
| Stunted (HAZ 1 < −2) | Unadjusted | Adjusted 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Variables | n | % | RR 3 | 95% CI 4 | p | RR 3 | 95% CI 4 | p |
| Community-level and socioeconomic factors | ||||||||
| Ecological region and place of residence | <0.0001 | 0.001 | ||||||
| Terai region, urban | 43 | 18.7 | 1.00 | (reference) | 1.00 | (reference) | ||
| Terai region, rural | 681 | 27.7 | 1.48 | (1.18–1.85) | 1.22 | (0.96–1.54) | ||
| Hill region, urban | 30 | 14.3 | 0.76 | (0.53–1.09) | 0.91 | (0.66–1.26) | ||
| Hill region, rural | 661 | 34.8 | 1.86 | (1.49–2.32) | 1.34 | (1.05–1.70) | ||
| Mountain region, urban | 1 | 4.6 | 0.24 | (0.04–1.52) | 0.32 | (0.06–1.77) | ||
| Mountain region, rural | 176 | 43.5 | 2.32 | (1.82–2.96) | 1.58 | (1.22–2.03) | ||
| Maternal religion | 0.251 | 0.011 | ||||||
| Hindu | 1359 | 30.1 | 1.00 | (reference) | 1.00 | (reference) | ||
| Buddhist and others | 232 | 27.9 | 0.90 | (0.75–1.08) | 0.83 | (0.72–0.96) | ||
| Maternal educational status | <0.0001 | 0.001 | ||||||
| Secondary and above | 183 | 15.8 | 1.00 | (reference) | 1.00 | (reference) | ||
| Completed primary | 230 | 25.6 | 1.62 | (1.30–2.00) | 1.26 | (0.99–1.61) | ||
| No education | 1177 | 37.4 | 2.36 | (1.98–2.81) | 1.47 | (1.18–1.83) | ||
| Pooled household wealth index | <0.0001 | 0.015 | ||||||
| Quintile 1 (Wealthiest) | 98 | 13.8 | 1.00 | (reference) | 1.00 | (reference) | ||
| Quintile 2 | 219 | 23.4 | 1.70 | (1.31–2.21) | 1.22 | (0.92–1.62) | ||
| Quintile 3 (Middle) | 302 | 31.3 | 2.27 | (1.76–2.92) | 1.44 | (1.08–1.93) | ||
| Quintile 4 | 358 | 37.4 | 2.72 | (2.15–3.43) | 1.52 | (1.14–2.05) | ||
| Quintile 5 (Poorest) | 521 | 43.5 | 3.15 | (2.50–3.98) | 1.60 | (1.18–2.17) | ||
| Maternal and child characteristics | ||||||||
| Maternal smoking status | <0.0001 | 0.006 | ||||||
| Non-smokers | 1163 | 27.4 | 1.00 | (reference) | 1.00 | (reference) | ||
| Smokers | 428 | 44.8 | 1.64 | (1.49–1.80) | 1.14 | (1.04–1.25) | ||
| Maternal height | <0.0001 | <0.0001 | ||||||
| Normal stature (≥145 cm) | 1274 | 28.5 | 1.00 | (reference) | 1.00 | (reference) | ||
| Short stature (<145 cm) | 317 | 43.5 | 1.52 | (1.37–1.70) | 1.37 | (1.23–1.52) | ||
| Maternal perception of birth size | <0.0001 | <0.0001 | ||||||
| Average | 892 | 28.9 | 1.00 | (reference) | 1.00 | (reference) | ||
| Very small | 123 | 44.0 | 1.52 | (1.30–1.78) | 1.29 | (1.10–1.52) | ||
| Smaller than average | 328 | 42.8 | 1.48 | (1.31–1.67) | 1.22 | (1.09–1.37) | ||
| Larger than average | 208 | 23.5 | 0.81 | (0.69–0.96) | 0.80 | (0.70–0.92) | ||
| Large | 39 | 20.8 | 0.72 | (0.52–0.99) | 0.61 | (0.43–0.85) | ||
| Birth status | <0.0001 | 0.038 | ||||||
| Singleton | 1570 | 30.3 | 1.00 | (reference) | 1.00 | (reference) | ||
| Multiple | 21 | 63.6 | 2.09 | (1.61–2.72) | 1.49 | (1.02–2.18) | ||
| Birth rank and birth interval | <0.0001 | 0.005 | ||||||
| 2nd/3rd birth rank, >2 years interval | 446 | 27.5 | 1.00 | (reference) | 1.00 | (reference) | ||
| 1st birth rank | 377 | 25.2 | 0.92 | (0.80–1.06) | 1.05 | (0.91–1.22) | ||
| 2nd/3rd birth rank, ≤2 years interval | 165 | 29.5 | 1.07 | (0.91–1.27) | 1.07 | (0.90–1.26) | ||
| ≥4th birth rank, >2 years interval | 421 | 35.7 | 1.30 | (1.14–1.48) | 1.06 | (0.95–1.20) | ||
| ≥4th birth rank, ≤2 years interval | 183 | 51.9 | 1.89 | (1.65–2.17) | 1.30 | (1.13–1.49) | ||
| Timing of initiation of breastfeeding | 0.200 | 0.016 | ||||||
| Never breastfed | 6 | 50.3 | 1.00 | (reference) | 1.00 | (reference) | ||
| <1 hours | 845 | 29.5 | 0.59 | (0.31–1.11) | 0.42 | (0.22–0.80) | ||
| 1 to 24 hours | 343 | 31.3 | 0.62 | (0.33–1.17) | 0.44 | (0.23–0.84) | ||
| >24 hours | 397 | 32.2 | 0.64 | (0.34–1.21) | 0.49 | (0.25–0.93) | ||
| Perinatal health services | ||||||||
| Number of antenatal care visits | <0.0001 | 0.024 | ||||||
| No antenatal care visit | 699 | 39.4 | 1.00 | (reference) | 1.00 | (reference) | ||
| <4 antenatal care visits | 631 | 31.2 | 0.79 | (0.71–0.88) | 1.01 | (0.92–1.12) | ||
| ≥4 antenatal care visits | 260 | 18.5 | 0.47 | (0.40–0.55) | 0.81 | (0.68–0.97) | ||
4. Discussion
4.1. Main Findings and Their Significance
4.2. Strengths and Limitations
4.3. Comparison with Other Studies
4.4. Impact on Reduction in Stunting
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- UNICEF; WHO. Low Birthweight: Country, Regional and Global Estimates; UNICEF: New York, NY, USA, 2004. [Google Scholar]
- Kramer, M.S. Determinants of low birth weight: Methodological assessment and meta-analysis. Bull. World Health Organ. 1987, 65, 663–737. [Google Scholar] [PubMed]
- Grantham-McGregor, S.; Cheung, Y.B.; Cueto, S.; Glewwe, P.; Richter, L.; Strupp, B. Developmental potential in the first 5 years for children in developing countries. Lancet 2007, 369, 60–70. [Google Scholar] [CrossRef]
- Ministry of Health and Population (MOHP) [Nepal]; New ERA; ICF International Inc. NepalDemographic and Health Survey 2011; MOHP, New ERA, and ICF International: Kathmandu, Nepal; Calverton, MA, USA, 2012. [Google Scholar]
- Haider, B.A.; Olofin, I.; Wang, M.; Spiegelman, D.; Ezzati, M. Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 2013, 346. [Google Scholar] [CrossRef] [PubMed]
- Imdad, A.; Bhutta, Z.A. Routine iron/folate supplementation during pregnancy: Effect on maternal anaemia and birth outcomes. Paediatr. Perinat. Epidemiol. 2012, 26, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Pena-Rosas, J.P.; de-Regil, L.M.; Dowswell, T.; Viteri, F.E. Daily oral iron supplementation during pregnancy. Cochrane Database Syst. Rev. 2012, 12, CD004736. [Google Scholar] [PubMed]
- World Health Organization. Guideline: Daily Iron and Folic Acid Supplementation in Pregnant Women; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Ministry of Health [Nepal]; New ERA. ORC Macro Nepal Demographic and Health Survey 2001; Family Health Division, Ministry of Health; New ERA; and ORC Macro: Calverton, MA, USA, 2002.
- Wang, W.; Yan, H.; Zeng, L.; Cheng, Y.; Wang, D.; Li, Q. No effect of maternal micronutrient supplementation on early childhood growth in rural western China: 30 month follow-up evaluation of a double blind, cluster randomized controlled trial. Eur. J. Clin. Nutr. 2012, 66, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.P.; Christian, P.; LeClerq, S.C.; West, K.P., Jr.; Khatry, S.K. Antenatal supplementation with folic acid + iron + zinc improves linear growth and reduces peripheral adiposity in school-age children in rural Nepal. Am. J. Clin. Nutr. 2009, 90, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Islam Khan, A. Effects of pre- and postnatal nutrition interventions on child growth and body composition: The MINIMat trial in rural Bangladesh. Glob. Health Action 2013, 6, 22476. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Population (MOHP) [Nepal]; New ERA; Macro International Inc. Nepal Demographic and Health Survey 2006; MOHP, New ERA, and Macro International Inc.: Kathmandu, Nepal, 2007.
- Macro International. Sampling Manual; DHS-III Basic Documentation No 6; Macro International Inc.: Calverton, MD, USA, 1996. [Google Scholar]
- Channon, A.A. Can mothers judge the size of their newborn? Assessing the determinants of a mother’s perception of a baby’s size at birth. J. Biosoc. Sci. 2011, 43, 555–573. [Google Scholar] [CrossRef] [PubMed]
- UNICEF; WHO. Progress on Drinking Water and Sanitation Joint Monitoring Programme Update 2012; UNICEF: New York, NY, USA, 2012. [Google Scholar]
- Filmer, D.; Pritchett, L.H. Estimating wealth effects without expenditure data—or tears: An application to educational enrollments in states of India. Demography 2001, 38, 115–132. [Google Scholar] [PubMed]
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M.T. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, S.; Lipsitz, S.R.; Rimm, E. A simple method of determining confidence intervals for population attributable risk from complex surveys. Stat. Med. 2007, 26, 3229–3239. [Google Scholar] [CrossRef] [PubMed]
- Rockhill, B.; Newman, B.; Weinberg, C. Use and misuse of population attributable fractions. Am. J. Public Health 1998, 88, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Lash, T.L.; Greenland, S. Modern Epidemiology, 3rd ed.; Lippincott, Williams, & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- National Planning Commission Secretariat, Central Bureau of Statistics. National Population and Housing Census 2011; (National Report); Government of Nepal: Kathmandu, Nepal, November 2012.
- Nisar, Y.B.; Dibley, M.J. Earlier initiation and use of a greater number of iron-folic acid supplements during pregnancy prevents early neonatal deaths in Nepal and Pakistan. PLoS ONE 2014, 14, e112446. [Google Scholar] [CrossRef] [PubMed]
- Mahy, M. Childhood Mortality in the Developing World: A Review of Evidence from the Demographic and Health Surveys; DHS Comparative Reports No. 4; ORC Macro: Calverton, MA, USA, 2003. [Google Scholar]
- Hill, K.; Choi, Y. Neonatal mortality in the developing world. Demogr. Res. 2006, 14, 429–452. [Google Scholar] [CrossRef]
- Hall, S. Neonatal Mortality in Developing Countries: What Can We Learn from DHS Data; University of Southampton, Statistical Sciences Research Institute: Southampton, UK, 2005. [Google Scholar]
- Dang, S.; Yan, H.; Yamamoto, S. High altitude and early childhood growth retardation: New evidence from Tibet. Eur. J. Clin. Nutr. 2008, 62, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Haider, B.A.; Bhutta, Z.A. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2012, 11, CD004905. [Google Scholar] [PubMed]
- Sandstrom, B. Micronutrient interactions: Effects on absorption and bioavailability. Br. J. Nutr. 2001, 85, S181–S185. [Google Scholar] [CrossRef] [PubMed]
- Siega-Riz, A.M.; Hartzema, A.G.; Turnbull, C.; Thorp, J.; McDonald, T.; Cogswell, M.E. The effects of prophylactic iron given in prenatal supplements on iron status and birth outcomes: A randomized controlled trial. Am. J. Obstet. Gynecol. 2006, 194, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, M.E.; Parvanta, I.; Ickes, L.; Yip, R.; Brittenham, G.M. Iron supplementation during pregnancy, anemia, and birth weight: A randomized controlled trial. Am. J. Clin. Nutr. 2003, 78, 773–781. [Google Scholar] [PubMed]
- Makrides, M.; Crowther, C.A.; Gibson, R.A.; Gibson, R.S.; Skeaff, C.M. Efficacy and tolerability of low-dose iron supplements during pregnancy: A randomized controlled trial. Am. J. Clin. Nutr. 2003, 78, 145–153. [Google Scholar] [PubMed]
- Espo, M.; Kulmala, T.; Maleta, K.; Cullinan, T.; Salin, M.L.; Ashorn, P. Determinants of linear growth and predictors of severe stunting during infancy in rural Malawi. Acta Paediatr. 2002, 91, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Christian, P.; Lee, S.E.; Donahue Angel, M.; Adair, L.S.; Arifeen, S.E.; Ashorn, P.; Barros, F.C.; Fall, C.H.; Fawzi, W.W.; Hao, W.; et al. Risk of childhood undernutrition related to small-for-gestational age and preterm birth in low- and middle-income countries. Int. J. Epidemiol. 2013, 42, 1340–1355. [Google Scholar] [CrossRef] [PubMed]
- Pokharel, R.K.; Maharjan, M.R.; Mathema, P.; Harvey, P.W.J. Success in Delivering Interventions to Reduce Maternal Anemia in Nepal: A Case Study of the Intensification of Maternal and Neonatal Micronutrient Program; United States Agency for International Development (USAID): Washington, DC, USA, 2009. [Google Scholar]
- Nisar, Y.B.; Alam, A.; Aurangzeb, B.; Dibley, M.J. Perceptions of antenatal iron-folic acid supplements in urban and rural Pakistan: A qualitative study. BMC Pregnancy Childbirth 2014, 14, 344. [Google Scholar] [CrossRef] [PubMed]
- Nisar, Y.B.; Dibley, M.J.; Mir, M.A. Factors associated with non-use of antenatal iron and folic acid supplements among Pakistani women: A cross sectional household survey. BMC Pregnancy Childbirth 2014, 14, 305. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nisar, Y.B.; Dibley, M.J.; Aguayo, V.M. Iron-Folic Acid Supplementation During Pregnancy Reduces the Risk of Stunting in Children Less Than 2 Years of Age: A Retrospective Cohort Study from Nepal. Nutrients 2016, 8, 67. https://doi.org/10.3390/nu8020067
Nisar YB, Dibley MJ, Aguayo VM. Iron-Folic Acid Supplementation During Pregnancy Reduces the Risk of Stunting in Children Less Than 2 Years of Age: A Retrospective Cohort Study from Nepal. Nutrients. 2016; 8(2):67. https://doi.org/10.3390/nu8020067
Chicago/Turabian StyleNisar, Yasir Bin, Michael J. Dibley, and Victor M. Aguayo. 2016. "Iron-Folic Acid Supplementation During Pregnancy Reduces the Risk of Stunting in Children Less Than 2 Years of Age: A Retrospective Cohort Study from Nepal" Nutrients 8, no. 2: 67. https://doi.org/10.3390/nu8020067
APA StyleNisar, Y. B., Dibley, M. J., & Aguayo, V. M. (2016). Iron-Folic Acid Supplementation During Pregnancy Reduces the Risk of Stunting in Children Less Than 2 Years of Age: A Retrospective Cohort Study from Nepal. Nutrients, 8(2), 67. https://doi.org/10.3390/nu8020067