The Use of Fish Oil with Warfarin Does Not Significantly Affect either the International Normalised Ratio or Incidence of Adverse Events in Patients with Atrial Fibrillation and Deep Vein Thrombosis: A Retrospective Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Study Variables
2.4. Statistical Methods
2.5. Ethical Approval
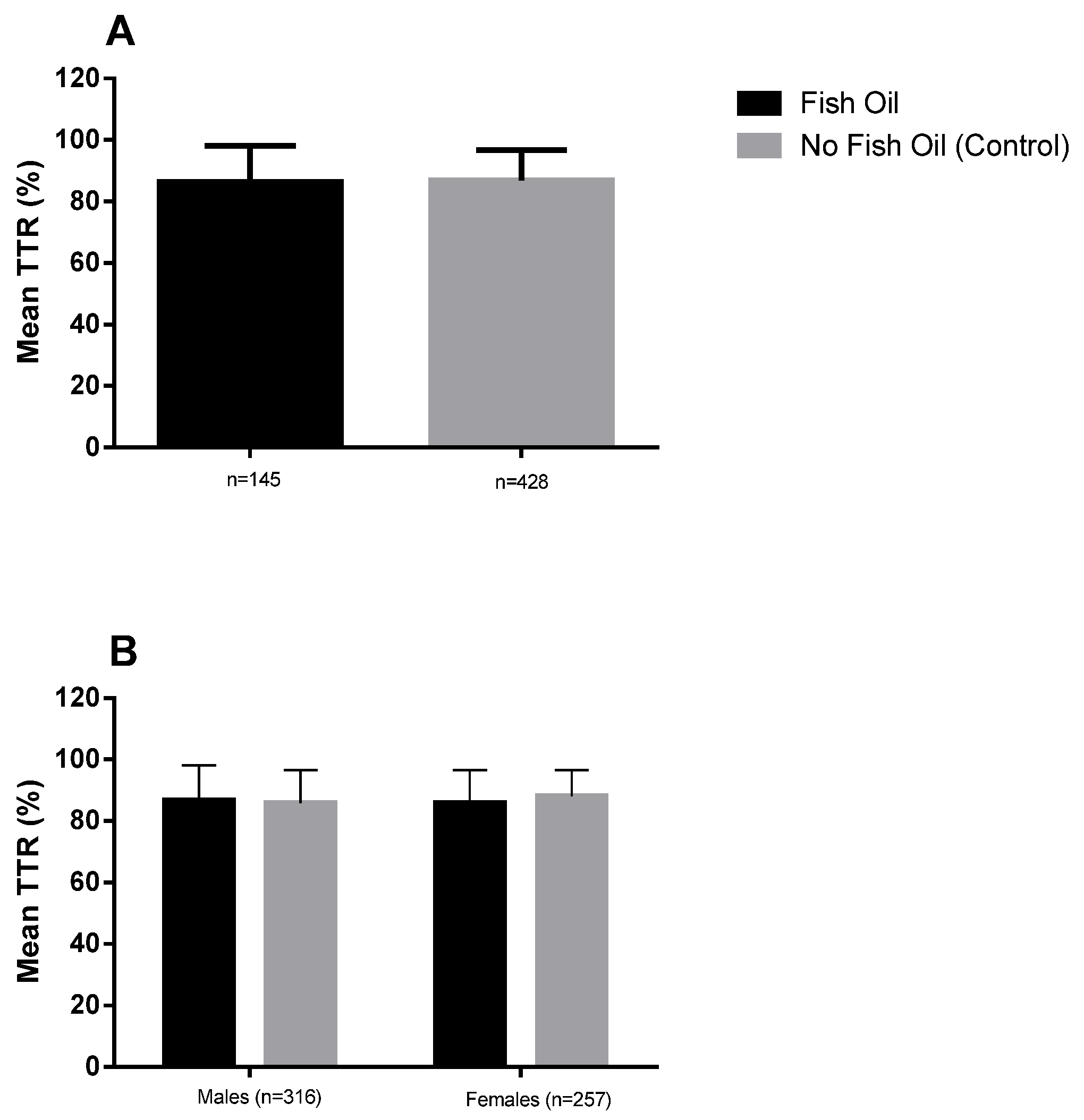
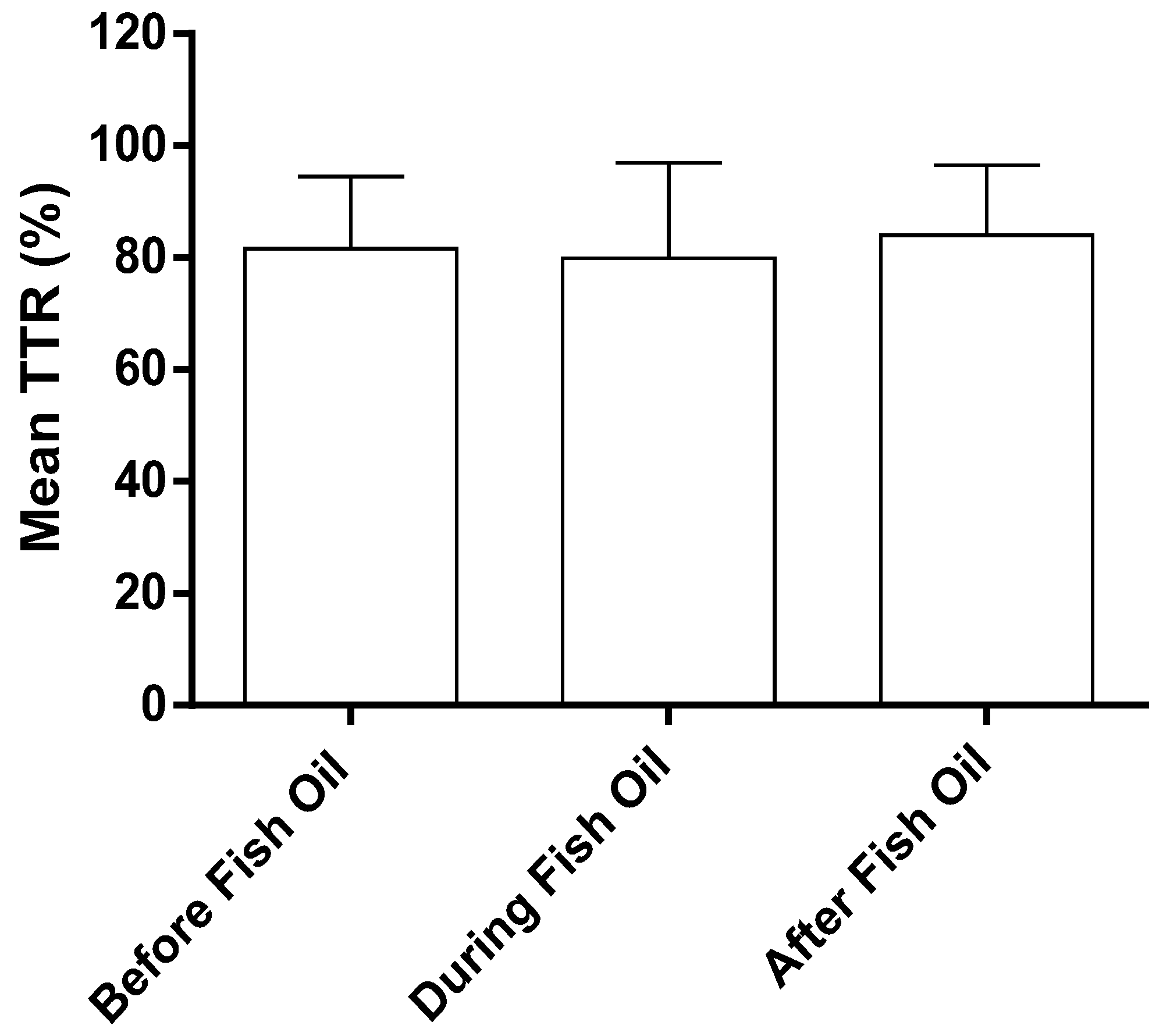
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Tran, H.A.; Chunilal, S.D.; Harper, P.L.; Tran, H.; Wood, E.M.; Gallus, A.S. An update of consensus guidelines for warfarin reversal. Med. J. Aust. 2013, 198, 198–199. [Google Scholar] [CrossRef] [PubMed]
- Campbell, P.; Roberts, G.; Eaton, V.; Coghlan, D.; Gallus, A. Managing warfarin therapy in the community. Aust. Prescr. 2001, 24, 86–89. [Google Scholar] [CrossRef]
- Kearon, C.; Kahn, S.R.; Agnelli, G.; Goldhaber, S.; Raskob, G.E.; Comerota, A.J. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians evidence-based clinical practice guidelines. CHEST 2008, 133, 454S–545S. [Google Scholar] [CrossRef] [PubMed]
- Rosendaal, F.; Cannegieter, S.; Van der Meer, F.; Briet, E. A method to determine the optimal intensity of oral anticoagulant therapy. Thrombosis Haemost. 1993, 69, 236–239. [Google Scholar]
- Connolly, S.J.; Pogue, J.; Eikelboom, J.; Flaker, G.; Commerford, P.; Franzosi, M.G.; Healey, J.S.; Yusuf, S.; Active, W. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation 2008, 118, 2029–2037. [Google Scholar] [CrossRef] [PubMed]
- White, H.D.; Gruber, M.; Feyzi, J.; Kaatz, S.; Tse, H.F.; Husted, S.; Albers, G.W. Comparison of outcomes among patients randomized to warfarin therapy according to anticoagulant control: Results from SPORTIF III and V. Arch. Intern. Med. 2007, 167, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Lip, G.Y.; De Caterina, R.; Savelieva, I.; Atar, D.; Hohnloser, S.H.; Hindricks, G.; Kirchhof, P. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation. Eur. Heart J. 2012, 33, 2719–2747. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Warfarin Management in the Community. Available online: https://www.health.qld.gov.au/publications/clinical-practice/guidelines-procedures/medicines/warfarin-gguideline.pdf (accessed on 18 September 2016).
- Apostolakis, S.; Sullivan, R.M.; Olshansky, B.; Lip, G.Y. Factors affecting quality of anticoagulation control among patients with atrial fibrillation on warfarin: The SAMe-TT2R2 score. CHEST 2013, 144, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Garcia, D.; Crowther, M.A.; Ageno, W. Practical management of coagulopathy associated with warfarin. BMJ 2010, 340, 1813. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S. Australian Medicines Handbook; Australian Medicines: Adelaide, Australia, 2006; pp. 2–3. [Google Scholar]
- Williamson, E.M.; Driver, S.; Baxter, K. Stockley’s Herbal Medicines Interactions; Pharmaceutical Press: London, UK, 2009. [Google Scholar]
- NPS Annual Consumer Surveys: Findings about Complementary Medicines Use 2006. Available online: http://www.nps.org.au/about-us/what-we-do/our-research/complementary-medicines/nps-consumer-sursur-cms-use-findings (accessed on 11 July 2016).
- Wood, M.J.; Stewart, R.L.; Merry, H.; Johnstone, D.E.; Cox, J.L. Use of complementary and alternative medical therapies in patients with cardiovascular disease. Am. Heart J. 2003, 145, 806–812. [Google Scholar] [CrossRef]
- Valli, G.; Giardina, E.-G.V. Benefits, adverse effects and drug interactionsof herbal therapies with cardiovascular effects. J. Am. Coll. Cardiol. 2002, 39, 1083–1095. [Google Scholar] [CrossRef]
- Ramsay, N.A.; Kenny, M.W.; Davies, G.; Patel, J.P. Complimentary and alternative medicine use among patients starting warfarin. Br. J. Haematol. 2005, 130, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Mechanisms of action of (n-3) fatty acids. J. Nutr. 2012, 142, 592S–599S. [Google Scholar] [CrossRef] [PubMed]
- Bunea, R.; El Farrah, K.; Deutsch, L. Evaluation of the effects of Neptune Krill Oil on the clinical course of hyperlipidemia. Altern. Med. Rev. 2004, 9, 420–428. [Google Scholar] [PubMed]
- Monograph, F.O. Natural Medicines Comprehensive Database; Therapeutic Research Faculty: Stockton, CA, USA, 2000; p. 919. [Google Scholar]
- Calder, P. Long-chain n-3 fatty acids and inflammation: Potential application in surgical and trauma patients. Br. J. Med. Biol. Res. 2003, 36, 433–446. [Google Scholar] [CrossRef]
- Fetterman, J.W., Jr.; Zdanowicz, M.M. Therapeutic potential of n-3 polyunsaturated fatty acids in disease. Am. J. Health Syst. Pharm. 2009, 66, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Marine omega-3 fatty acids and inflammatory processes: Effects, mechanisms and clinical relevance. Biochim. Biophys. Acta 2015, 1851, 469–484. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, A.C.; Harris, W.S.; Amin, A.P.; Reid, K.J.; O’Keefe, J.H.; Spertus, J.A. Relation between red blood cell omega-3 fatty acid index and bleeding during acute myocardial infarction. Am. J. Cardiol. 2012, 109, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.E.; Van Elswyk, M.; Alexander, D.D. Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and blood pressure: A meta-analysis of randomized controlled trials. Am. J. Hypertens. 2014, 27, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Nestel, P.; Clifton, P.; Colquhoun, D.; Noakes, M.; Mori, T.A.; Sullivan, D.; Thomas, B. Indications for omega-3 long chain polyunsaturated fatty acid in the prevention and treatment of cardiovascular disease. Heart Lung Circ. 2015, 24, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Information Use and Needs of Complementary Medicines Users. Available online: https://www.nps.org.au/__data/assets/pdf_file/0010/66619/Complementary_Medicines_Report_-_ConsuCCon.pdf (accessed on 18 September 2016).
- Barnes, P.M.; Bloom, B.; Nahin, R.L. Complementary and alternative medicine use among adults and children: United States, 2007. Natl. Health Stat. Report. 2008, 10, 1–23. [Google Scholar]
- Wachira, J.K.; Larson, M.K.; Harris, W.S. N-3 fatty acids affect haemostasis but do not increase the risk of bleeding: Clinical observations and mechanistic insights. Br. J. Nutr. 2014, 111, 1652–1662. [Google Scholar] [CrossRef] [PubMed]
- Eritsland, J.; Arnesen, H.; Seljeflot, I.; Kierulf, P. Long-term effects of n-3 polyunsaturated fatty acids on haemostatic variables and bleeding episodes in patients with coronary artery disease. Blood Coagul. Fibrinolysis 1995, 6, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Jalili, M.; Dehpour, A.R. Extremely prolonged INR associated with warfarin in combination with both trazodone and omega-3 fatty acids. Arch. Med. Res. 2007, 38, 901–904. [Google Scholar] [CrossRef] [PubMed]
- McClaskey, E.M.; Michalets, E.L. Subdural hematoma after a fall in an elderly patient taking high-dose omega-3 fatty acids with warfarin and aspirin: Case report and review of the literature. Pharmacotherapy 2007, 27, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Buckley, M.S.; Goff, A.D.; Knapp, W.E. Fish oil interaction with warfarin. Ann. Pharmacother. 2004, 38, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials a consensus report from the bleeding academic research consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed]
- Bender, N.K.; Kraynak, M.A.; Chiquette, E.; Linn, W.D.; Clark, G.M.; Bussey, H.I. Effects of marine fish oils on the anticoagulation status of patients receiving chronic warfarin therapy. J. Thromb. Thrombolysis 1998, 5, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Small, N.L.; Giamonna, K.A. Interaction between warfarin and trazodone. Ann. Pharmacother. 2000, 34, 734–736. [Google Scholar] [CrossRef] [PubMed]
- Hardy, J.-L.; Sirois, A. Reduction of prothrombin and partial thromboplastin times with trazodone. CMAJ 1986, 135, 1372. [Google Scholar] [PubMed]
- Holub, B.J. Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. CMAJ 2002, 166, 608–615. [Google Scholar] [PubMed]
- Flaten, H.; Høstmark, A.; Kierulf, P.; Lystad, E.; Trygg, K.; Bjerkedal, T.; Osland, A. Fish-oil concentrate: Effects on variables related to cardiovascular disease. Am. J. Clin. Nutr. 1990, 52, 300–306. [Google Scholar] [PubMed]
- Oosthuizen, W.; Vorster, H.; Jerling, J.; Barnard, H.; Smuts, C.; Silvis, N.; Kruger, A.; Venter, C.S. Both fish oil and olive oil lowered plasma fibrinogen in women with high baseline fibrinogen levels. Thromb. Haemost. 1994, 72, 557–562. [Google Scholar] [PubMed]
- Vanschoonbeek, K.; Feijge, M.A.; Paquay, M.; Rosing, J.; Saris, W.; Kluft, C.; Giesen, P.L.; de Maat, M.P.; Heemskerk, J.W. Variable hypocoagulant effect of fish oil intake in humans modulation of fibrinogen level and thrombin generation. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1734–1740. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuys, C.M.; Feijge, M.A.; Vermeer, C.; Hennissen, A.H.; Béguin, S.; Heemskerk, J.W. Vitamin K-dependent and vitamin K-independent hypocoagulant effects of dietary fish oil in rats. Thromb. Res. 2001, 104, 137–147. [Google Scholar] [CrossRef]
- Bernaitis, N.; Badrick, T.; Davey, A.K.; Anoopkumar-Dukie, S. Quality of warfarin control in atrial fibrillation patients in South East Queensland, Australia. Intern. Med. J. 2016, 46, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Chiquette, E.; Amato, M.G.; Bussey, H.I. Comparison of an anticoagulation clinic with usual medical care: Anticoagulation control, patient outcomes, and health care costs. Arch. Intern. Med. 1998, 158, 1641–1647. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable—n (%) | All Patients | Fish Oil | No Fish Oil |
|---|---|---|---|
| (n = 573) | (n = 145) | (n = 428) | |
| Age (years) | |||
| Mean (Standard Deviation) | 75.0 (14.1) | 76.8 (11.9) | 74.4 (14.7) |
| ≤25 | 2 (0.3) | 0 | 2 (0.5) |
| 26 to ≤50 | 38 (6.6) | 6 (4.1) | 32 (7.5) |
| 51 to ≤75 | 198 (34.6) | 50 (34.5) | 148 (34.6) |
| 75 to ≤100 | 335 (585) | 89 (61.4) | 246 (57.5) |
| Gender | |||
| Male | 316 (55.1) | 75 (51.7) | 241 (56.3) |
| Female | 257 (44.9) | 70 (48.3) | 187 (43.7) |
| Comorbidities | |||
| AF | 416 (72.6) | 113 (77.9) | 303 (70.8) |
| DVT | 157 (27.4) | 32 (22.1) | 125 (29.2) |
| HTN | 165 (30.6) | 37 (29.4) | 128 (31.0) |
| Diabetes | 56 (10.4) | 13 (10.3) | 43 (10.4) |
| Hypercholesterolemia | 28 (5.2) | 6 (4.8) | 22 (5.3) |
| Angina | 9 (1.5) | 3 (2.4) | 5 (1.2) |
| HF | 8 (1.5) | - | 8 (1.9) |
| IHD | 29 (5.4) | 9 (7.1) | 20 (4.7) |
| COPD | 16 (3.0) | 1 (0.8) | 15 (3.6) |
| Asthma | 16 (3.0) | 4 (3.2) | 12 (2.9) |
| Dyslipidaemia | 20 (3.7) | 4 (3.2) | 16 (3.9) |
| Gout | 18 (3.3) | 3 (2.4) | 15 (3.6) |
| Cancer | 28 (3.3) | 4 (3.2) | 14 (3.4) |
| GORD | 27 (5.0) | 8 (6.3) | 19 (4.6) |
| Arthritis | 49 (9.1) | 13 (10.3) | 36 (8.7) |
| Renal Failure | 9 (1.7) | 3 (2.4) | 6 (1.5) |
| OP | 23 (4.3) | 4 (3.2) | 19 (4.6) |
| Bleeding Event | Supplement Group | Control Group | ||
|---|---|---|---|---|
| A | ||||
| Minor | 0.07 | 0.09 | ||
| Major | 0 | 0 | ||
| B | ||||
| Males | Females | Males | Females | |
| Minor | 0.04 | 0.05 | 0.10 | 0.08 |
| Major | 0.00 | 0.01 | 0.01 | 0.00 |
| Bleeding Event | Before Fish Oil | During Fish Oil | After Fish Oil |
|---|---|---|---|
| Minor | 0.16 | 0.16 | 0.22 |
| Major | 0.01 | 0.00 | 0.00 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pryce, R.; Bernaitis, N.; Davey, A.K.; Badrick, T.; Anoopkumar-Dukie, S. The Use of Fish Oil with Warfarin Does Not Significantly Affect either the International Normalised Ratio or Incidence of Adverse Events in Patients with Atrial Fibrillation and Deep Vein Thrombosis: A Retrospective Study. Nutrients 2016, 8, 578. https://doi.org/10.3390/nu8090578
Pryce R, Bernaitis N, Davey AK, Badrick T, Anoopkumar-Dukie S. The Use of Fish Oil with Warfarin Does Not Significantly Affect either the International Normalised Ratio or Incidence of Adverse Events in Patients with Atrial Fibrillation and Deep Vein Thrombosis: A Retrospective Study. Nutrients. 2016; 8(9):578. https://doi.org/10.3390/nu8090578
Chicago/Turabian StylePryce, Rebecca, Nijole Bernaitis, Andrew K. Davey, Tony Badrick, and Shailendra Anoopkumar-Dukie. 2016. "The Use of Fish Oil with Warfarin Does Not Significantly Affect either the International Normalised Ratio or Incidence of Adverse Events in Patients with Atrial Fibrillation and Deep Vein Thrombosis: A Retrospective Study" Nutrients 8, no. 9: 578. https://doi.org/10.3390/nu8090578