Family Food Providers’ Perceptions of the Causes of Obesity and Effectiveness of Weight Control Strategies in Five Countries in the Asia Pacific Region: A Cross-Sectional Survey


Abstract
:1. Introduction
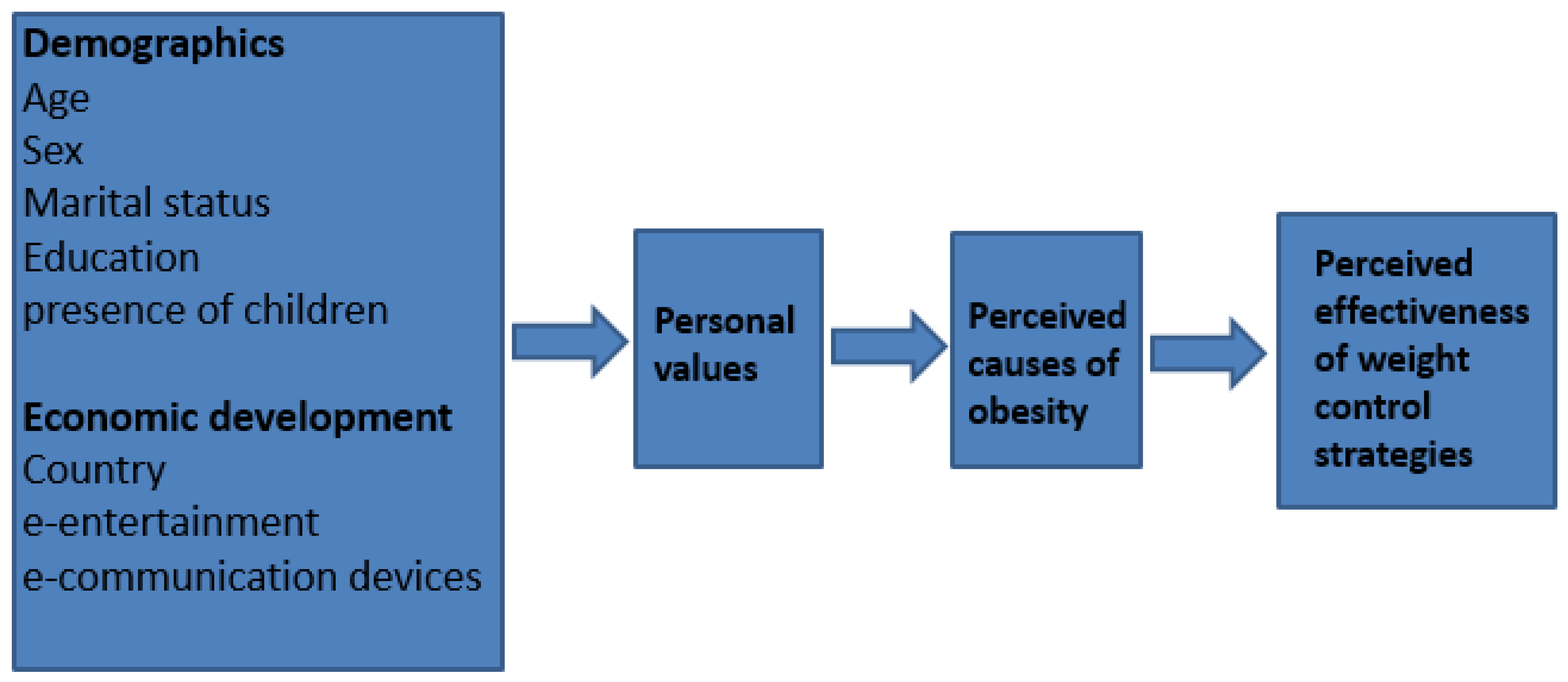
- Demographic characteristics: Older people tend to be more concerned about food and health issues than younger people [9,10,11,12], as are most women [13]. Therefore, women and older people may view the causes of obesity differently to men and younger people. Highly educated people also tend to be more health conscious [14] and more able to afford exercise and dietary innovations [15], so they may emphasize individual responsibility for obesity. Similarly, being married may positively influence health and food consumption [16], and the presence of young children in the household may expose food providers to food marketing and obesogenic influences [17,18].
- Body Mass Index status: People who are overweight or obese might be expected to have greater reason than others to consider the causes of obesity as well as methods to control body weight. In terms of attribution theory, their greater involvement suggests that as “actors” they may be more likely than slimmer people to attribute obesity to external causes beyond their personal control [19].
- Personal value orientations: These are generally associated with attitudes and opinions [20]. For example, people with communitarian, “other-oriented” values [21] tend to look to external factors when explaining phenomena such as the role of government in the provision of school lunches [22], whereas those who hold more individualist values tend to place a greater emphasis on individual responsibility. We expected respondents with strong communitarian values [23] would emphasize the importance of external causes of obesity e.g., food marketing and environmental influences, and conversely, those with stronger self-oriented values would favour causes related to individual control, e.g., over-eating.
- Levels of economic development: In regions undergoing rapid economic and epidemiologic transitions [24], the expanding middle class might be most exposed to consumerist (individualist) trends and fashions such as beauty culture, international film and media, and, food marketing. We hypothesized that people in economically developed regions (such as Melbourne and Singapore) would hold more individualistic views of obesity causation than those in recently developing regions (i.e., Indonesia, Vietnam and Shanghai). We expected household ownership of electronic communication and entertainment devices, indices of consumerist (individualist) culture, would parallel these regional differences.
- Perceptions of effective weight control strategies: The perceived causes of obesity may influence perceptions of effective ways to control body weight. For example, those who believe environmental influences are mainly responsible for obesity might see environmental changes as the most effective ways to maintain a healthy body weight. Identification of food providers’ support for valid effective weight control activities could be used to develop supporting obesity prevention policies.
2. Materials and Methods
2.1. Design and Sampling
2.2. Procedure
2.3. The Questionnaire
3. Results
3.1. The Demographic Characteristics of the Samples
3.2. Concern about Body Weight
3.3. Perceived Causes of Obesity
3.4. Perceived Effectiveness of Personal Weight Control Options
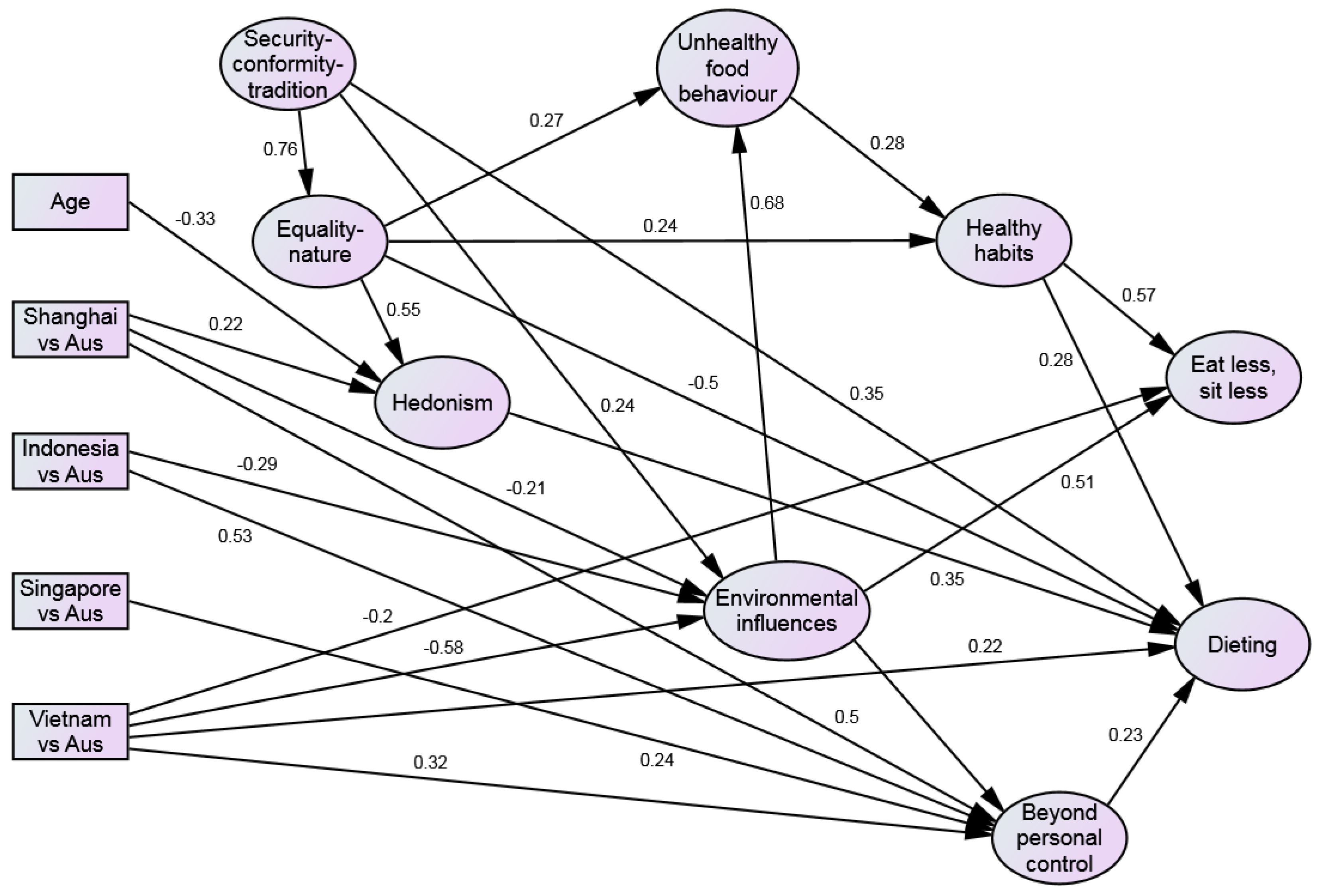
3.5. SEM Pathways
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dobbs, R.; Sawers, C.; Thompson, F.; Manyika, J.; Woetzel, J.; Child, P.; McKenna, S.; Spatharou, A. Overcoming Obesity: An Initial Economic Analysis; McKinsey Global Institute: London, UK, 2014. [Google Scholar]
- Field, P.A. Advocacy for Using Evidence in Public Health Nutrition Policy Making. Ph.D. Thesis, University of Otago, Dunedin, New Zealand, 2014. [Google Scholar]
- Goody, J. Cooking, Cuisine and Class: A Study in Comparative Sociology; Cambridge University Press: Cambridge, UK, 1982. [Google Scholar]
- Reid, M.; Worsley, A.; Mavondo, F. The obesogenic household: Factors influencing dietary gatekeeper satisfaction with family diet. Psychol. Market. 2015, 32, 544–557. [Google Scholar] [CrossRef]
- Hardus, P.M.; van Vuuren, C.L.; Crawford, D.; Worsley, A. Public perceptions of the causes and prevention of obesity among primary school children. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Easterly, W. The Middle Class Consensus and Economic Development. J. Econ. Growth. 2001, 6, 317–335. [Google Scholar] [CrossRef]
- Murphy, K.M.; Shleifer, A.; Vishny, R.W. Industrialization and the Big Push. J. Polit. Econ. 1989, 97, 1003–1026. [Google Scholar] [CrossRef]
- Banerjee, A.V.; Duflo, E. What is Middle Class about the Middle Classes around the World? J. Econ. Perspect. 2008, 22, 3–28. [Google Scholar] [CrossRef] [PubMed]
- Koivisto Hursti, U.; Magnusson, M.K.; Algers, A. Swedish consumers’ opinions about gene technology. Brit. Food. J. 2002, 104, 860–872. [Google Scholar] [CrossRef]
- Miles, S.; Brennan, M.; Kuznesof, S.; Ness, M.; Ritson, C.; Frewer, L.J. Public worry about specific food safety issues. Brit. Food. J. 2004, 106, 9–22. [Google Scholar] [CrossRef]
- Verbeke, W.A.J.; Viaene, J. Ethical Challenges for Livestock Production: Meeting Consumer Concerns about Meat Safety and Animal Welfare. J. Agric. Environ. Ethic. 1999, 12, 141–151. [Google Scholar] [CrossRef]
- Worsley, A.; Scott, V. Consumers’ concerns about food and health in Australia and New Zealand. Asia Pac. J. Clin. Nutr. 2000, 9, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, R.O.; Warland, R.H.; Sterngold, A. Nutrition concerns and food-safety concerns occur independently among adults. J. Am. Diet. Assoc. 2000, 100, 947–949. [Google Scholar] [CrossRef]
- Pill, R.; Peters, T.J.; Robling, M.R. Social class and preventive health behaviour: A British example. J. Epidemiol. Community Health 1995, 49, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Quesnel-Vallée, A.; Jenkins, T. Social policies and health inequalities. In The New Blackwell Companion to Medical Sociology; Cockerham, W.C., Ed.; Wiley-Blackwell: Oxford, UK, 2010; pp. 455–483. [Google Scholar]
- Wood, R.G.; Goesling, B.; Avellar, S. The Effects of Marriage on Health: A synthesis of Recent Research Evidence. Available online: https://cire.mathematica-mpr.com/~/media/publications/pdfs/marriagehealth.pdf (accessed on 14 January 2017).
- Sharma, A.; Sonwaney, V. Theoretical Modeling of Influence of Children on Family Purchase Decision Making. Procedia Soc. Behav. Sci. 2014, 133, 38–46. [Google Scholar] [CrossRef]
- Harris, J.L.; Sarda, V.; Schwartz, M.B.; Brownell, K.D. Redefining “child-directed advertising” to reduce unhealthy television food advertising. Am. J. Prev. Med. 2013, 44, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.E.; Nisbett, R.E. The Actor and the Observer: Divergent Perceptions of the Causes of Behavior; General Learning Press: New York, NY, USA, 1971. [Google Scholar]
- Ajzen, I. Theories of Cognitive Self-RegulationThe theory of planned behavior. Organ. Behav. Hum. Dec. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Grunert, K.G.; Brunso, K.; Bisp, S. Food-related lifestyle: Development of a cross-culturally valid instrument for market surveillance. In Values, Lifestyles and Psychographics; Kahle, L.R., Chiagouris, L., Eds.; Lawrence Erlbaum Associates: Mahway, NJ, USA, 1997. [Google Scholar]
- Worsley, A. Lay People’s views of school food policy options: Associations with confidence, personal values and demographics. Health Educ. Res. 2006, 21, 848–861. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.H. Universals in the content and structure of values: Theoretical advances and empirical tests in 20 countries. Adv. Exp. Soc. Psychol. 1992, 25, 1–65. [Google Scholar]
- Popkin, B.; Monteiro, C.; Swinburn, B. Overview: Bellagio Conference on Program and Policy Options for Preventing Obesity in the Low-and Middle-Income Countries. Obes. Rev. 2013, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight: WHO Global Strategy on Diet, Physical Activity and Health; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Venn, A.J.; Thomson, R.J.; Schmidt, M.D.; Cleland, V.J.; Curry, B.A.; Gennat, H.C.; Dwyer, T. Overweight and obesity from childhood to adulthood: A follow-up of participants in the 1985 Australian Schools Health and Fitness Survey. Med. J. Aust. 2007, 186, 458–460. [Google Scholar] [PubMed]
- Schwartz, S.H. Basic Human Values: An Overview 2006. Available online: http://segr-did2.fmag.unict.it/allegati/convegno 7-8-10-05/schwartzpaper.pdf (accessed on 14 January 2017).
- SPSS. SPSS for Windows, 20th ed.; SPSS Inc.: Chicago, IL, USA, 2014. [Google Scholar]
- Muthén, L.K. Mplus User’s Guide, 6th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2013. [Google Scholar]
- International Food Information Council. 2014 Food and Nutrition Survey. Available online: http://www.foodinsight.org/sites/default/files/2014 Food and Health Survey Full Report.pdf (accessed on 3 March 2015).
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S. Profits and pandemics: Prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Brownell, K.D. Thinking forward: The quicksand of appeasing the food industry. PLoS Med. 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Foedermayr, E.K.; Diamantopoulos, A. Market Segmentation in Practice: Review of Empirical Studies, Methodological Assessment, and Agenda for Future Research. J. Strat. Market. 2008, 16, 223–265. [Google Scholar] [CrossRef]
- Drewnowski, A.; Specter, S.E. Poverty and obesity: The role of energy density and energy costs. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| Melbourne n = 769 | Shanghai n= 807 | Indonesia n = 788 | Singapore n = 771 | Vietnam n = 810 | Total n = 3945 | |
|---|---|---|---|---|---|---|
| Gender: Female (%) | 58.4 | 57.2 | 59.5 | 49.3 | 60.5 | 57.3 |
| * Age: Mean (Std Dev) | 41.43 (12.70) | 37.81 (10.53) | 32.97 (9.07) | 37.45 (11.68) | 29.25 (7.35) | 35.72 (11.23) |
| Marital status: Married/de facto (%) | 61.0 | 77.4 | 57.2 | 55.3 | 51.4 | 60.4 |
| Education: Bachelor degree or higher (%) | 58.9 | 89.5 | 80.8 | 74.2 | 90.7 | 78.8 |
| Families with children between 0 and 5 years (%) | 20.4 | 34.9 | 39.3 | 25.9 | 54.2 | 35.2 |
| Families with children between 6 and 12 (%) | 18.1 | 16.5 | 30.9 | 21.4 | 27.8 | 23 |
| Families with children between 13 and 18 (%) | 15.6 | 14.7 | 25.1 | 19.2 | 21.4 | 19.2 |
| BMI: Mean (Std Dev) | 26.89 (7.03) | 23.60 (6.92) | 23.11 (5.17) | 23.08 (4.53) | 20.81 (3.32) | 23.47 (5.91) |
| Own or buying household accommodation (%) | 65.8 | 89.2 | 67.1 | 85.1 | 73.8 | 76.3 |
| E-communication devices: Mean (Std Dev) | 3.7 (2.1) | 4.2 (1.6) | 3.9 (2.4) | 5.0 (2.4) | 3.8 (2.0) | 4.1 (2.2) |
| E-entertainment devices: Mean (Std Dev) | 5.7 (3.3) | 4.9 (2.0) | 4.7 (2.8) | 5.1 (2.8) | 4.3 (2.8) | 4.9 (2.8) |
| Melbourne (n = 769) | Shanghai (n = 807) | Indonesia (n = 788) | Singapore (n = 771) | Vietnam (n = 810) | Total (n = 3945) | Chi-square | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Are you concerned about your weight at the moment? | Not at all | 20.6 | 22.8 | 26.6 | 14.7 | 14.4 | 19.8 | 170.70 | <0.01 |
| A little concerned | 29.5 | 28.0 | 28.8 | 19.3 | 21.7 | 25.5 | |||
| Somewhat concerned | 33.0 | 38.7 | 32.5 | 38.8 | 43.2 | 37.3 | |||
| Very concerned | 16.9 | 10.5 | 12.1 | 27.2 | 20.6 | 17.4 | |||
| Are you trying to do anything about your weight? | Yes | 61.7 | 67.3 | 72.5 | 61.6 | 70.7 | 66.8 | 36.29 | <0.01 |
| * Are you trying to lose weight? | Yes | 53.9 | 42.5 | 53.8 | 49.0 | 37.9 | 47.3 | 182.63 | <0.01 |
| * Are you trying to gain weight? | Yes | 3.2 | 4.5 | 13.5 | 6.1 | 26.0 | 10.8 | 197.82 | <0.01 |
| * Are you trying to maintain weight? | Yes | 3.5 | 17.5 | 4.5 | 4.7 | 5.2 | 7.1 | 7.84 | >0.05 |
| Have you heard of the Body Mass Index (BMI)? | Yes | 83.9 | 55.0 | 60.7 | 91.4 | 69.4 | 71.8 | 379.08 | <0.01 |
| Melbourne (n = 769) | Shanghai (n = 807) | Indonesia (n = 788) | Singapore (n = 771) | Vietnam (n = 810) | Total (n = 3945) | Chi-square | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Unhealthy food behaviour (α = 0.68) | ||||||||
| Eating oversized servings of foods | 87.8 | 88.7 | 89.3 | 84.0 | 69.4 | 83.8 | 300.48 | <0.01 |
| Regular consumption of fast foods | 89.6 | 79.7 | 79.6 | 87.0 | 70.9 | 81.2 | 270.07 | <0.01 |
| Overconsumption of sugar sweetened drinks | 88.9 | 86.1 | 89.1 | 86.6 | 74.2 | 84.9 | 257.85 | <0.01 |
| Beyond personal control (α = 0.55) | ||||||||
| People aren’t aware of the dangers of obesity | 56.8 | 67.9 | 81.7 | 65.5 | 65.6 | 67.6 | 223.38 | <0.01 |
| Lack of availability of healthy foods | 41.0 | 65.4 | 53.8 | 50.3 | 32.7 | 48.7 | 273.02 | <0.01 |
| Lack of physical activity opportunities | 66.6 | 87.0 | 81.6 | 76.9 | 70.5 | 76.6 | 238.76 | <0.01 |
| Genes cause obesity | 44.5 | 61.8 | 58.4 | 62.4 | 36.5 | 52.7 | 387.60 | <0.01 |
| Environmental influences (α = 0.59) | ||||||||
| Modern technology (e.g., cars, computers, video games) | 68.8 | 62.3 | 43.3 | 64.9 | 45.9 | 56.9 | 343.08 | <0.01 |
| The promotion of unhealthy foods (in stores, the mass media and online) | 72.8 | 64.9 | 55.3 | 73.4 | 35.7 | 60.2 | 438.28 | <0.01 |
| The low cost of unhealthy food | 71.4 | 41.3 | 57.1 | 62.1 | 30.1 | 52.1 | 400.97 | <0.01 |
| Melbourne (n = 769) | Shanghai (n = 807) | Indonesia (n = 788) | Singapore (n = 771) | Vietnam (n = 810) | Total (n = 3945) | Chi-square (df = 8) | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Healthy habits (α = 0.65) | ||||||||
| Establish an exercise routine | 87.7 | 87.5 | 91.9 | 84.8 | 84.7 | 87.4 | 42.29 | <0.01 |
| Make a regular shopping list | 65.1 | 57.9 | 55.0 | 50.6 | 61.4 | 58.0 | 68.69 | <0.01 |
| Try not to eat sweetened foods like cakes or confectionery | 75.7 | 67.9 | 68.6 | 69.9 | 64.4 | 69.2 | 38.78 | <0.01 |
| Avoid alcoholic drinks | 58.1 | 49.4 | 77.6 | 59.9 | 56.4 | 60.2 | 167.38 | <0.01 |
| Eat less, sit less (α = 0.70) | ||||||||
| Don’t sit down for longer than 15–20 min at a time | 43.8 | 68.9 | 40.0 | 42.0 | 47.7 | 48.6 | 223.41 | <0.01 |
| Use smaller plates and dishes | 68.8 | 55.8 | 36.8 | 54.6 | 30.1 | 49.0 | 470.46 | <0.01 |
| Don’t have second helpings | 72.5 | 58.9 | 66.2 | 59.1 | 31.2 | 57.4 | 517.43 | <0.01 |
| Try to eat less | 70.4 | 51.1 | 54.4 | 58.2 | 32.5 | 53.1 | 428.91 | <0.01 |
| Dieting (α = 0.68) | ||||||||
| Go on a slimming diet | 30.4 | 41.0 | 50.4 | 30.9 | 57.3 | 42.2 | 202.22 | <0.01 |
| Weigh yourself regularly | 39.0 | 47.5 | 56.6 | 52.0 | 53.8 | 49.8 | 87.37 | <0.01 |
| Substitute diet soft drinks for regular soft drinks | 23.5 | 31.7 | 46.9 | 29.3 | 62.6 | 39.0 | 425.78 | <0.01 |
| Use commercial meal replacements | 19.0 | 31.2 | 29.5 | 21.9 | 30.5 | 26.5 | 138.06 | <0.01 |
| Melbourne (n = 769) | Shanghai (n = 807) | Indonesia (n = 788) | Singapore (n = 771) | Vietnam (n = 810) | Total (n = 3945) | Chi-square (df = 8) | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Security-Conformity-Tradition (α = 0.68) | ||||||||
| 1. I prefer to live in secure surroundings and avoid doing things that might endanger my safety. | 61.7 | 63.3 | 69.5 | 59.1 | 71.5 | 65.1 | 48.41 | <0.01 |
| 2. I always try to follow the rules of society and do what is expected of me, even when no one is watching. | 54.7 | 54.4 | 62.0 | 48.6 | 56.2 | 55.2 | 37.10 | <0.01 |
| 3. I always try to behave properly and to avoid doing anything people would say is wrong. | 57.1 | 44.1 | 61.9 | 52.0 | 68.9 | 56.8 | 135.73 | <0.01 |
| 4. I adhere to traditions and try to follow the customs handed down to me by religion or family. | 43.5 | 58.5 | 64.6 | 44.0 | 53.1 | 52.8 | 164.33 | <0.01 |
| Self-oriented Hedonism (α = 0.73) | ||||||||
| 1. I like to be constantly surprised, to do many different things in my life, and always look for new things to do. | 39.1 | 48.2 | 55.1 | 44.0 | 52.3 | 47.8 | 73.54 | <0.01 |
| 2. I like being seen as very successful and recognised by others for my achievements. | 27.4 | 59.2 | 37.1 | 43.1 | 48.4 | 43.2 | 310.13 | <0.01 |
| 3. I always seek adventure and take risks to lead an exciting life. | 25.1 | 30.2 | 41.7 | 36.3 | 39.0 | 34.5 | 152.56 | <0.01 |
| 4. I take every chance I have to seek out fun and to always do the things that give me pleasure. | 35.1 | 63.9 | 47.5 | 42.0 | 70.4 | 52.1 | 334.35 | <0.01 |
| Equality-nature (α = 0.74) | ||||||||
| 1. I believe it’s important that every person in the world should be treated equally no matter who, where, or what they are. | 73.5 | 70.8 | 81.0 | 66.1 | 73.1 | 72.9 | 58.83 | <0.01 |
| 2. I believe everyone should have equal opportunities in life no matter who, where, or what they are. | 76.6 | 74.1 | 81.7 | 68.7 | 76.2 | 75.5 | 38.89 | <0.01 |
| 3. I am always willing to listen to people who are different and even when I disagree with them I still want to understand them. | 62.7 | 59.9 | 71.6 | 55.0 | 71.4 | 64.2 | 76.48 | <0.01 |
| 4. I care for nature and always look after the Environmental influences. | 59.9 | 71.6 | 71.6 | 54.6 | 58.1 | 63.2 | 105.99 | <0.01 |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Worsley, A.; Wang, W.; Sarmugam, R.; Pham, Q.; Februhartanty, J.; Ridley, S. Family Food Providers’ Perceptions of the Causes of Obesity and Effectiveness of Weight Control Strategies in Five Countries in the Asia Pacific Region: A Cross-Sectional Survey. Nutrients 2017, 9, 78. https://doi.org/10.3390/nu9010078
Worsley A, Wang W, Sarmugam R, Pham Q, Februhartanty J, Ridley S. Family Food Providers’ Perceptions of the Causes of Obesity and Effectiveness of Weight Control Strategies in Five Countries in the Asia Pacific Region: A Cross-Sectional Survey. Nutrients. 2017; 9(1):78. https://doi.org/10.3390/nu9010078
Chicago/Turabian StyleWorsley, Anthony, Wei Wang, Rani Sarmugam, Quynh Pham, Judhiastuty Februhartanty, and Stacey Ridley. 2017. "Family Food Providers’ Perceptions of the Causes of Obesity and Effectiveness of Weight Control Strategies in Five Countries in the Asia Pacific Region: A Cross-Sectional Survey" Nutrients 9, no. 1: 78. https://doi.org/10.3390/nu9010078