Impact of Flavonols on Cardiometabolic Biomarkers: A Meta‐Analysis of Randomized Controlled Human Trials to Explore the Role of Inter‐Individual Variability


 ,
,  ,
,  , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction
2.3. Assessment of Bias
2.4. Data Analysis
3. Results
3.1. Description of the Included Studies
3.2. Characteristics of Participants
3.3. Effect of Flavonol Supplementation on Biomarkers of Cardiometabolic Risk
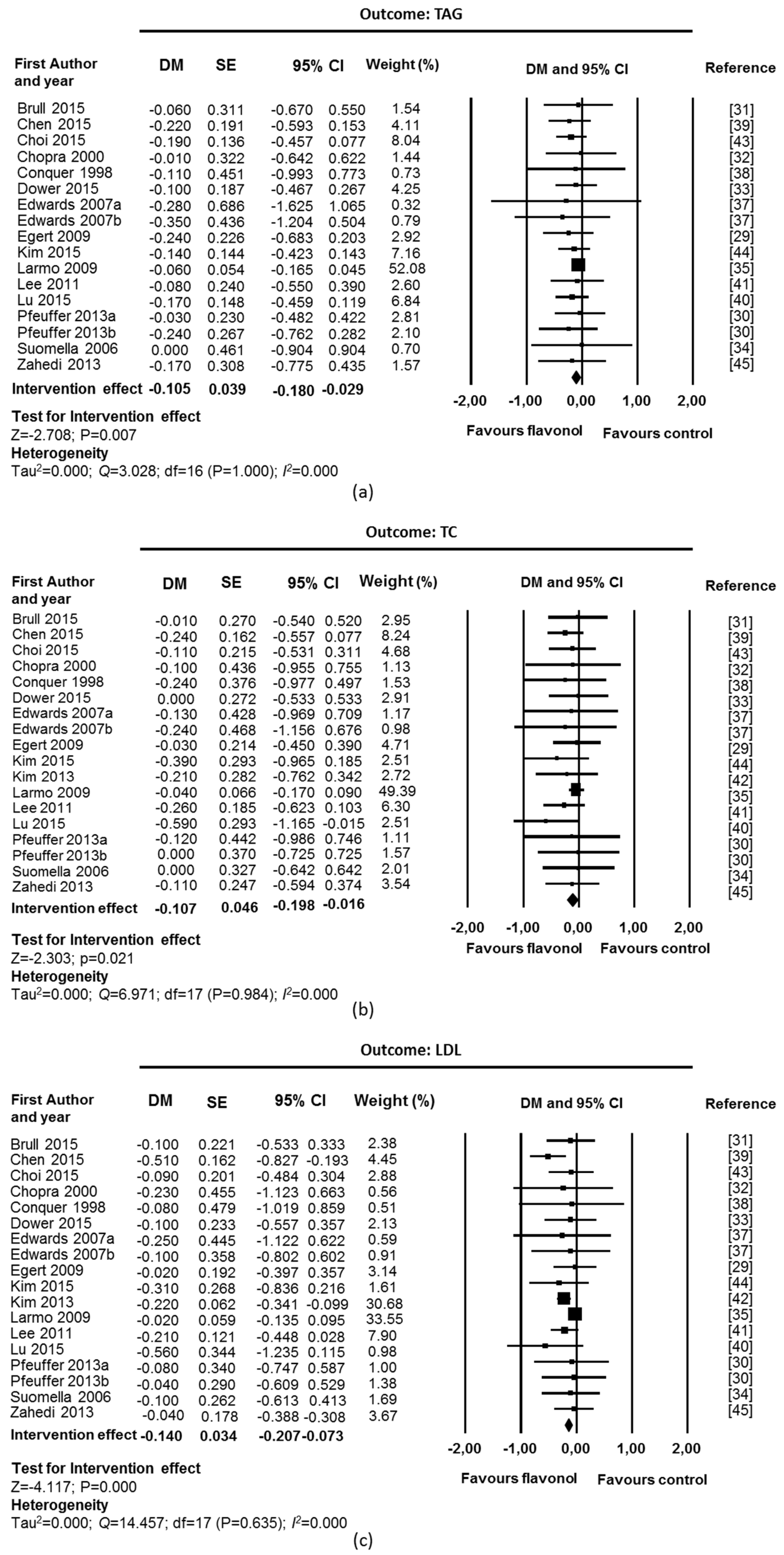
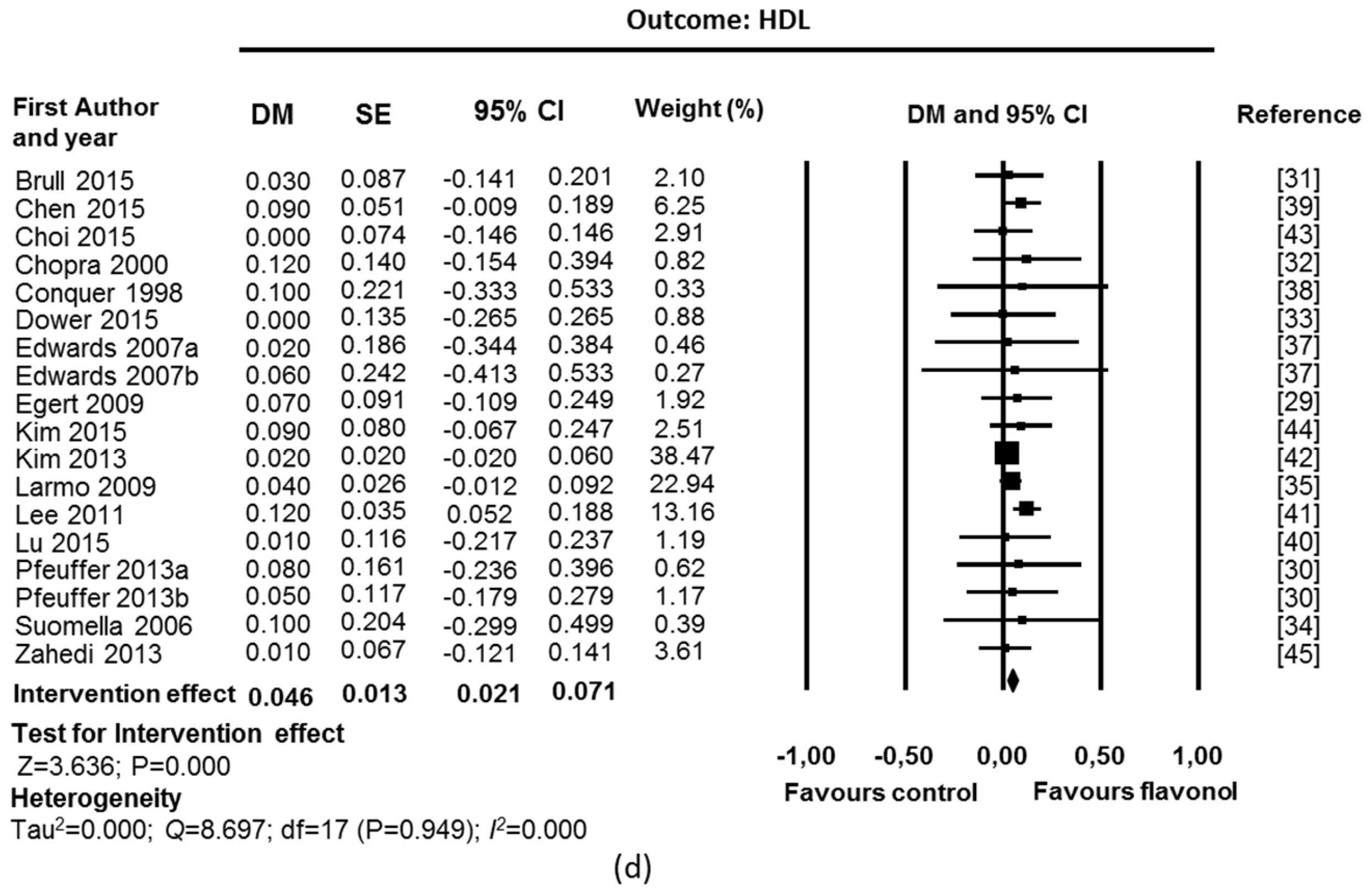
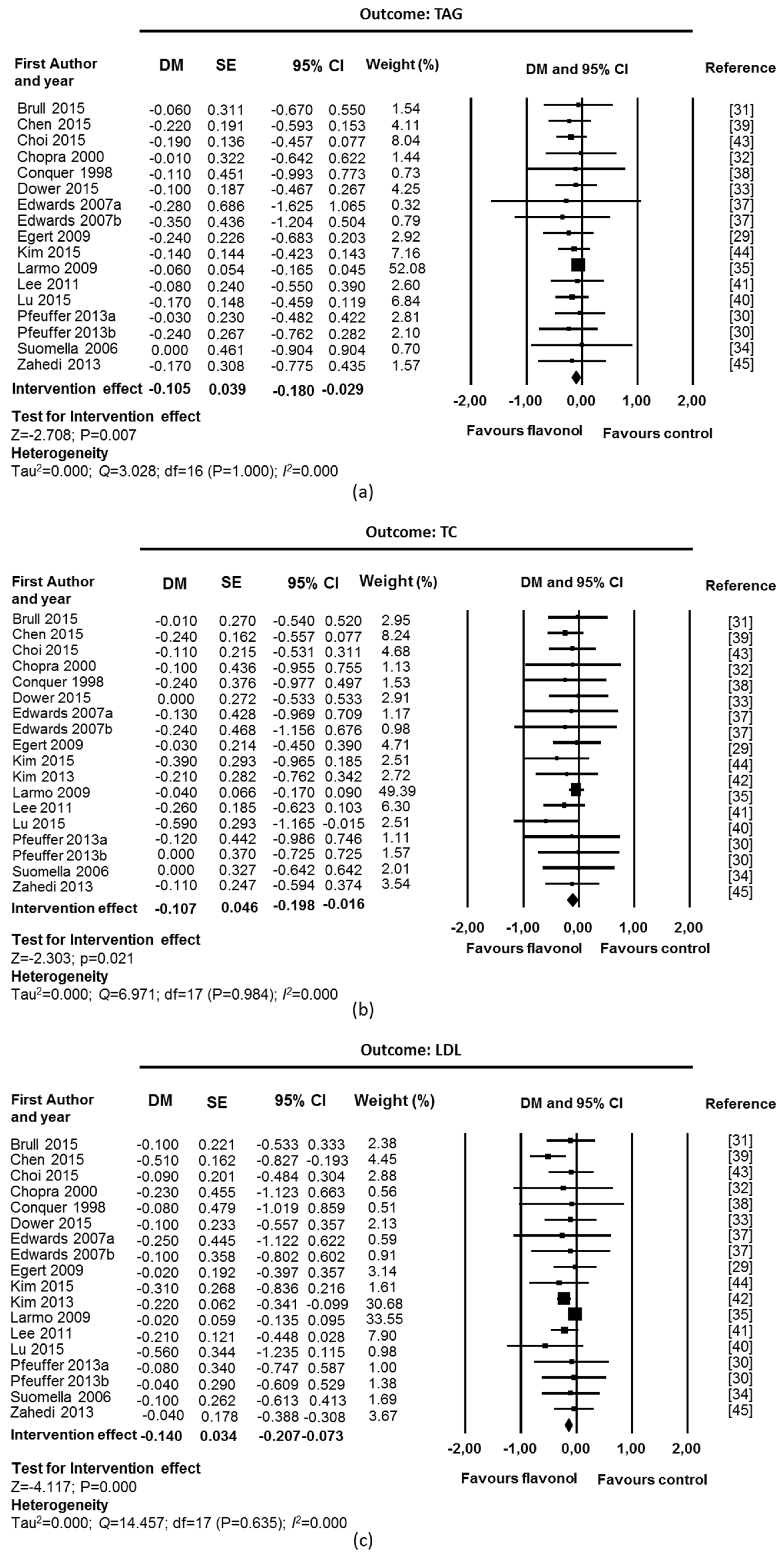
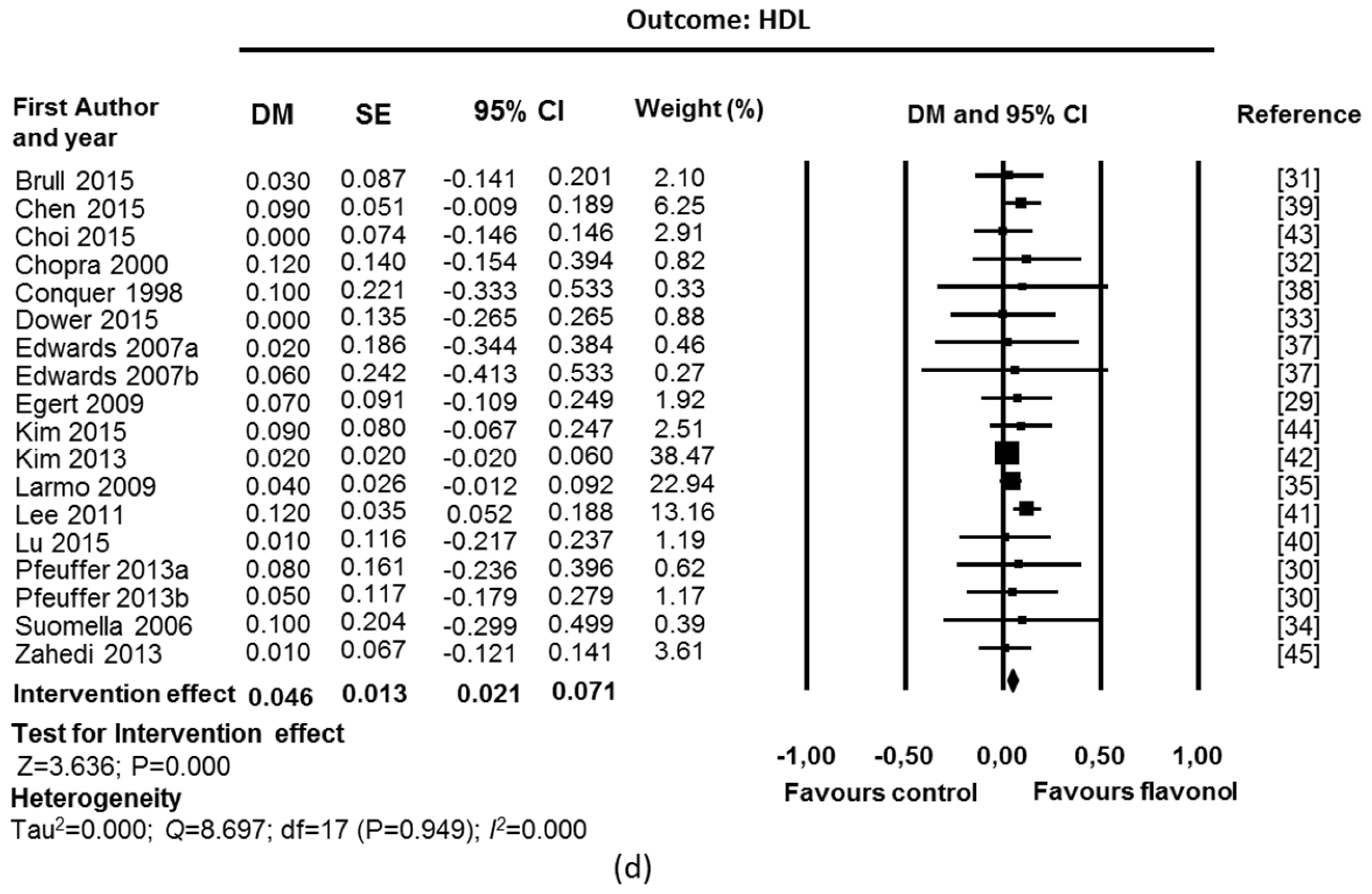
3.3.1. Blood Lipids
3.3.2. Blood Pressure
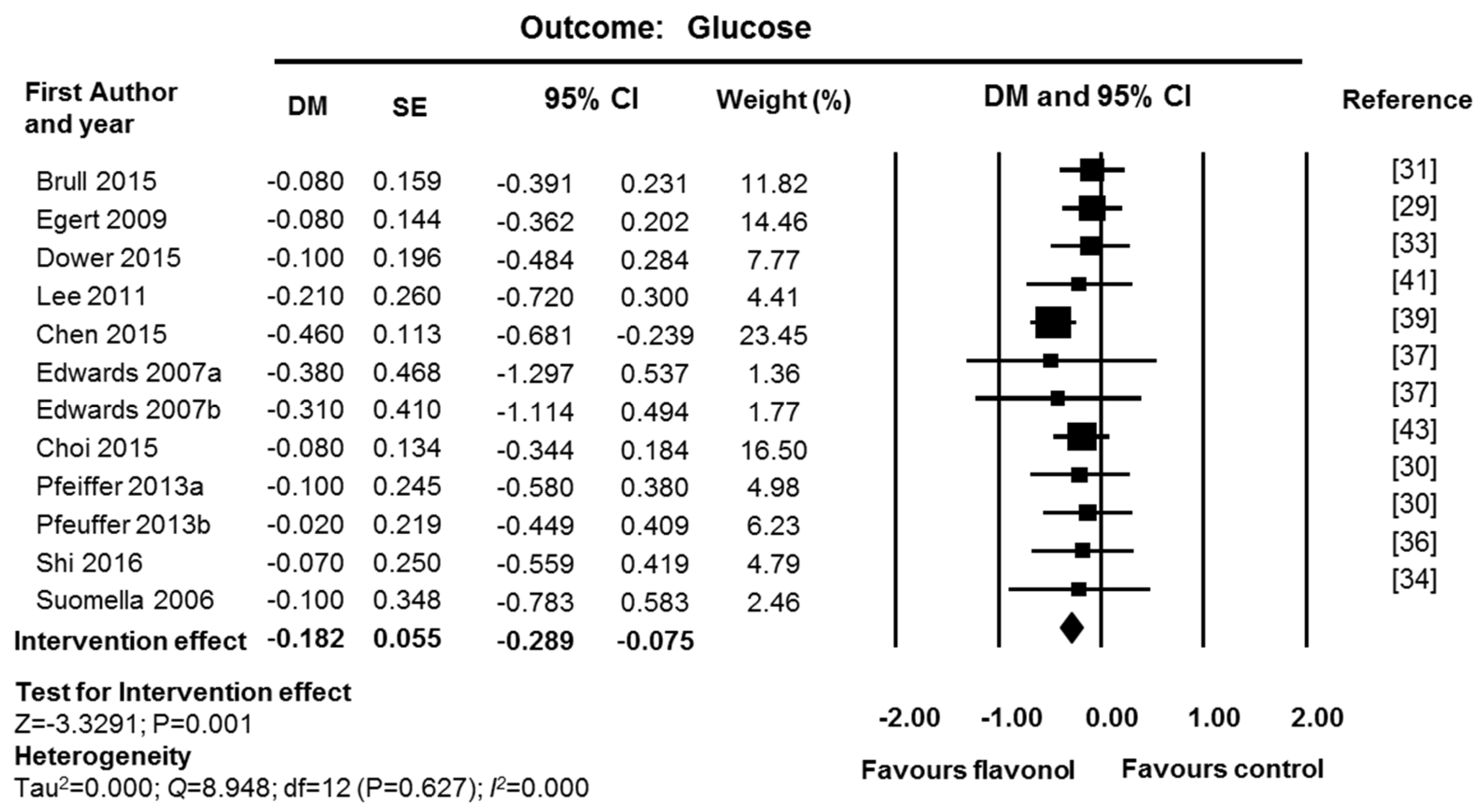
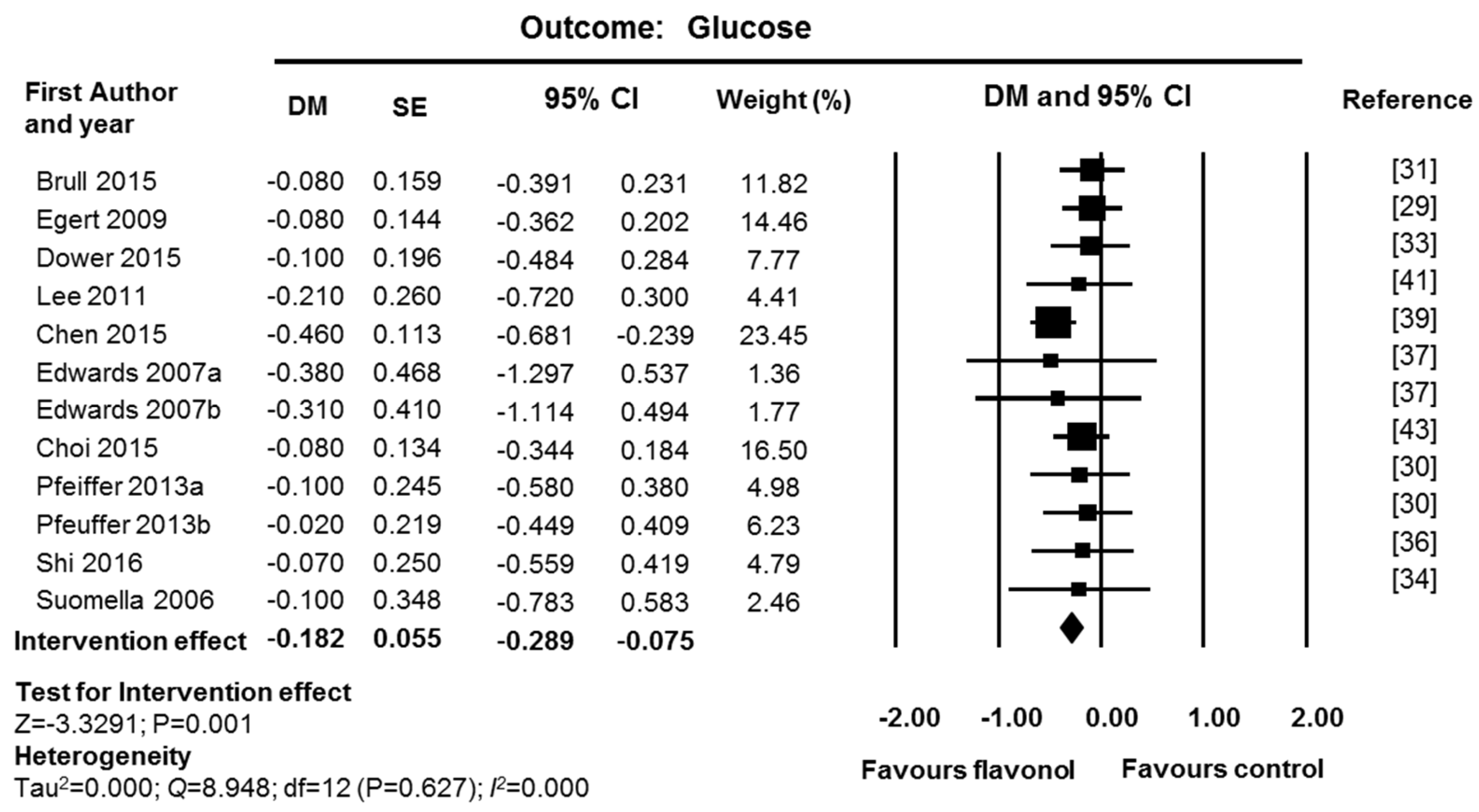
3.3.3. Fasting Glucose
3.4. Subgroup Analyses for Identification of Factors Affecting Inter-Individual Variability
3.4.1. Stratification by Age, Sex, and Country
3.4.2. Stratification by Health Status
3.5. Influence of the Type and Dose of Flavonol
4. Discussion
4.1. Quality of Evidence and Clinical Importance of the Observed Effects
4.2. Inter-Individual Variability
5. Conclusions
Supplementary Materials
Acknowledgments
Conflicts of Interest
References
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics—2013 update: A report from the american heart association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Roger, V.L.; Dunlay, S.M.; Go, A.S.; Rosamond, W.D. Challenges of ascertaining national trends in the incidence of coronary heart disease in the united states. J. Am. Heart Assoc. 2014, 3, e001097. [Google Scholar] [CrossRef] [PubMed]
- Perk, J.; De Backer, G.; Gohlke, H.; Graham, I.; Reiner, Ž.; Verschuren, M.; Albus, C.; Benlian, P.; Boysen, G.; Cifkova, R.; et al. European guidelines on cardiovascular disease prevention in clinical practice (version 2012). Eur. Heart J. 2012, 33, 1635–1701. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.J.; Robinson, J.; Lichtenstein, A.H.; Merz, C.N.B.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation 2013. [Google Scholar] [CrossRef] [PubMed]
- Woodside, J.V.; Young, I.S.; McKinley, M.C. Fruit and vegetable intake and risk of cardiovascular disease. Proc. Nutr. Soc. 2013, 72, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, M.F.; Macdonald, R.; Lovegrove, J.A. Fruit polyphenols and CVD risk: A review of human intervention studies. Br. J. Nutr. 2010, 104 (Suppl. S3), S28–S39. [Google Scholar] [CrossRef] [PubMed]
- Lecour, S.; Lamont, K.T. Natural polyphenols and cardioprotection. Mini Rev. Med. Chem. 2011, 11, 1191–1199. [Google Scholar] [CrossRef] [PubMed]
- Rangel-Huerta, O.D.; Pastor-Villaescusa, B.; Aguilera, C.M.; Gil, A. A systematic review of the efficacy of bioactive compounds in cardiovascular disease: Phenolic compounds. Nutrients 2015, 7, 5177–5216. [Google Scholar] [CrossRef] [PubMed]
- Alissa, E.M.; Ferns, G.A. Dietary fruits and vegetables and cardiovascular diseases risk. Crit. Rev. Food Sci. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Bruno, R.S. Endogenous and exogenous mediators of quercetin bioavailability. J. Nutr. Biochem. 2015, 26, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Pinto, P.; Santos, C.N. Worldwide (poly)phenol intake: Assessment methods and identified gaps. Eur. J. Nutr. 2017. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Knaze, V.; Rothwell, J.A.; Hemon, B.; Moskal, A.; Overvad, K.; Tjonneland, A.; Kyro, C.; Fagherazzi, G.; Boutron-Ruault, M.C.; et al. Dietary polyphenol intake in Europe: The european prospective investigation into cancer and nutrition (EPIC) study. Eur. J. Nutr. 2016, 55, 1359–1375. [Google Scholar] [CrossRef] [PubMed]
- Ibarra, M.; Moreno, L.; Vera, R.; Cogolludo, A.; Duarte, J.; Tamargo, J.; Perez-Vizcaino, F. Effects of the flavonoid quercetin and its methylated metabolite isorhamnetin in isolated arteries from spontaneously hypertensive rats. Planta Med. 2003, 69, 995–1000. [Google Scholar] [PubMed]
- Ajay, M.; Achike, F.I.; Mustafa, A.M.; Mustafa, M.R. Effect of quercetin on altered vascular reactivity in aortas isolated from streptozotocin-induced diabetic rats. Diabetes Res. Clin. Pract. 2006, 73, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hollman, P.C.H.; Geelen, A.; Kromhout, D. Dietary flavonol intake may lower stroke risk in men and women. J. Nutr. 2010, 140, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.-M.; Zhao, D.; Nie, Z.-L.; Zhao, H.; Zhou, B.; Gao, W.; Wang, L.-S.; Yang, Z.-J. Flavonol intake and stroke risk: A meta-analysis of cohort studies. Nutrition 2014, 30, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.M.; Nie, Z.L.; Zhou, B.; Lian, X.Q.; Zhao, H.; Gao, W.; Wang, Y.S.; Jia, E.Z.; Wang, L.S.; Yang, Z.J. Flavonols intake and the risk of coronary heart disease: A meta-analysis of cohort studies. Atherosclerosis 2012, 222, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Serban, M.C.; Sahebkar, A.; Zanchetti, A.; Mikhailidis, D.P.; Howard, G.; Antal, D.; Andrica, F.; Ahmed, A.; Aronow, W.S.; Muntner, P.; et al. Effects of quercetin on blood pressure: A systematic review and meta-analysis of randomized controlled trials. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2016, 5, e002713. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A. Effects of quercetin supplementation on lipid profile: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- MEDLINE. Available online: http://www.ncbi.nlm.nih.gov/pubmed (accessed on 21 December 2015).
- COPUS. Available online: http://www.scopus.com (accessed on 4 February 2016).
- Web of Knowledge. Available online: http://apps.webofknowledge.com (accessed on 18 December 2015).
- Clinical Trials.gov. Available online: (https ://www.clinicaltrials.gov/) (accessed on 4 February 2016).
- International Clinical Trials Registry Platform. Available online: www.who.int/trialsearch/ (accessed on 4 February 2016).
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. (Eds.) Assessing risk of bias in included studies. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (Updated March 2011). The Cochrane Collaboration, 2011. Available online: www.handbook.cochrane.org (accessed on 20 September 2016).
- Haidich, A.B. Meta-analysis in medical research. Hippokratia 2010, 14, 29–37. [Google Scholar] [PubMed]
- Higgins, J.; Green, S. (Eds.) Assessing the quality of a body of evidence. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration, 2011. Available online: www.handbook.cochrane.org (accessed on 20 September 2016).
- Egert, S.; Bosy-Westphal, A.; Seiberl, J.; Kürbitz, C.; Settler, U.; Plachta-Danielzik, S.; Wagner, A.E.; Frank, J.; Schrezenmeir, J.; Rimbach, G.; et al. Quercetin reduces systolic blood pressure and plasma oxidised low-density lipoprotein concentrations in overweight subjects with a high-cardiovascular disease risk phenotype: A double-blinded, placebo-controlled cross-over study. Br. J. Nutr. 2009, 102, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Pfeuffer, M.; Auinger, A.; Bley, U.; Kraus-Stojanowic, I.; Laue, C.; Winkler, P.; Rüfer, C.E.; Frank, J.; Bösch-Saadatmandi, C.; Rimbach, G.; et al. Effect of quercetin on traits of the metabolic syndrome, endothelial function and inflammation in men with different apoe isoforms. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Brüll, V.; Burak, C.; Stoffel-Wagner, B.; Wolffram, S.; Nickenig, G.; Müller, C.; Langguth, P.; Alteheld, B.; Fimmers, R.; Naaf, S.; et al. Effects of a quercetin-rich onion skin extract on 24 h ambulatory blood pressure and endothelial function in overweight-to-obese patients with (pre-)hypertension: A randomised double-blinded placebo-controlled cross-over trial. Br. J. Nutr. 2015, 114, 1263–1277. [Google Scholar] [CrossRef] [PubMed]
- Chopra, M.; Fitzsimons, P.E.E.; Strain, J.J.; Thurnham, D.I.; Howard, A.N. Nonalcoholic red wine extract and quercetin inhibit ldl oxidation without affecting plasma antioxidant vitamin and carotenoid concentrations. Clin. Chem. 2000, 46, 1162–1170. [Google Scholar] [PubMed]
- Dower, J.I.; Geleijnse, J.M.; Gijsbers, L.; Zock, P.L.; Kromhout, D.; Hollman, P.C.H. Effects of the pure flavonoids epicatechin and quercetin on vascular function and cardiometabolic health: A randomized, double-blind, placebo-controlled, crossover trial. Am. J. Clin. Nutr. 2015, 101, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Suomela, J.-P.; Ahotupa, M.; Yang, B.; Vasankari, T.; Kallio, H. Absorption of flavonols derived from sea buckthorn (Hippophaë rhamnoides L.) and their effect on emerging risk factors for cardiovascular disease in humans. J. Agric. Food Chem. 2006, 54, 7364–7369. [Google Scholar] [CrossRef] [PubMed]
- Larmo, P.S.; Yang, B.; Hurme, S.A.M.; Alin, J.A.; Kallio, H.P.; Salminen, E.K.; Tahvonen, R.L. Effect of a low dose of sea buckthorn berries on circulating concentrations of cholesterol, triacylglycerols, and flavonols in healthy adults. Eur. J. Nutr. 2009, 48, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Williamson, G. Quercetin lowers plasma uric acid in pre-hyperuricaemic males: A randomised, double-blinded, placebo-controlled, cross-over trial. Br. J. Nutr. 2016, 115, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.L.; Lyon, T.; Litwin, S.E.; Rabovsky, A.; Symons, J.D.; Jalili, T. Quercetin reduces blood pressure in hypertensive subjects. J. Nutr. 2007, 137, 2405–2411. [Google Scholar] [PubMed]
- Conquer, J.A.; Maiani, G.; Azzini, E.; Raguzzini, A.; Holub, B.J. Supplementation with quercetin markedly increases plasma quercetin concentration without effect on selected risk factors for heart disease in healthy subjects. J. Nutr. 1998, 128, 593–597. [Google Scholar] [PubMed]
- Chen, S.; Zhao, X.; Wan, J.; Ran, L.; Qin, Y.; Wang, X.; Gao, Y.; Shu, F.; Zhang, Y.; Liu, P.; et al. Dihydromyricetin improves glucose and lipid metabolism and exerts anti-inflammatory effects in nonalcoholic fatty liver disease: A randomized controlled trial. Pharmacol. Res. 2015, 99, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.M.; Chiu, H.F.; Shen, Y.C.; Chung, C.C.; Venkatakrishnan, K.; Wang, C.K. Hypocholesterolemic efficacy of quercetin rich onion juice in healthy mild hypercholesterolemic adults: A pilot study. Plant Foods Hum. Nutr. 2015, 70, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Park, E.; Lee, H.J.; Kim, M.O.; Cha, Y.J.; Kim, J.M.; Lee, H.; Shin, M.J. Effects of daily quercetin-rich supplementation on cardiometabolic risks in male smokers. Nutr. Res. Pract. 2011, 5, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Cha, Y.J.; Lee, K.H.; Park, E. Effect of onion peel extract supplementation on the lipid profile and antioxidative status of healthy young women: A randomized, placebo-controlled, double-blind, crossover trial. Nutr. Res. Pract. 2013, 7, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.Y.; Lee, H.; Woo, J.S.; Jang, H.H.; Hwang, S.J.; Kim, H.S.; Kim, W.S.; Kim, Y.S.; Choue, R.; Cha, Y.J.; et al. Effect of onion peel extract on endothelial function and endothelial progenitor cells in overweight and obese individuals. Nutrition 2015, 31, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.A.; Yim, J.E. Antioxidative activity of onion peel extract in obese women: A randomized, double-blind, placebo controlled study. J. Cancer Prev. 2015, 20, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Zahedi, M.; Ghiasvand, R.; Feizi, A.; Asgari, G.; Darvish, L. Does quercetin improve cardiovascular risk factors and inflammatory biomarkers in women with type 2 diabetes: A double-blind randomized controlled clinical trial. Int. J. Prev. Med. 2013, 4, 777–785. [Google Scholar] [PubMed]
- Javadi, F.; Eghtesadi, S.; Ahmadzadeh, A.; Aryaeian, N.; Zabihiyeganeh, M.; Foroushani, A.R.; Jazayeri, S. The effect of quercetin on plasma oxidative status, C-reactive protein and blood pressure in women with rheumatoid arthritis. Int. J. Prev. Med. 2014, 5, 293–301. [Google Scholar] [PubMed]
- Weber, M.A.; Schiffrin, E.L.; White, W.B.; Mann, S.; Lindholm, L.H.; Kenerson, J.G.; Flack, J.M.; Carter, B.L.; Materson, B.J.; Ram, C.V.; et al. Clinical practice guidelines for the management of hypertension in the community: A statement by the American society of hypertension and the international society of hypertension. J. Clin. Hypertens. 2014, 16, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, P.S.; Smith, D.A.; Mehta, A.E.; Ganda, O.; Handelsman, Y.; Rodbard, H.W.; Shepherd, M.D.; Seibel, J.A. American association of clinical endocrinologists’ guidelines for management of dyslipidemia and prevention of atherosclerosis. Endocr. Pract. 2012, 18 (Suppl. S1), 1–78. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association (ADA). Standards of medical care in diabetes: Classification and diagnosis of diabetes. Diabetes Care 2015, 38, S8–S16. [Google Scholar]
- Larson, A.J.; Symons, J.D.; Jalili, T. Therapeutic potential of quercetin to decrease blood pressure: Review of efficacy and mechanisms. Adv. Nutr. 2012, 3, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Parichatikanond, W.; Pinthong, D.; Mangmool, S. Blockade of the renin-angiotensin system with delphinidin, cyanin, and quercetin. Planta Med. 2012, 78, 1626–1632. [Google Scholar] [CrossRef] [PubMed]
- Perez-Vizcaino, F.; Duarte, J.; Jimenez, R.; Santos-Buelga, C.; Osuna, A. Antihypertensive effects of the flavonoid quercetin. Pharmacol. Rep. 2009, 61, 67–75. [Google Scholar] [CrossRef]
- Sahebkar, A.; Ferri, C.; Giorgini, P.; Bo, S.; Nachtigal, P.; Grassi, D. Effects of pomegranate juice on blood pressure: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2016, 115, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Feringa, H.H.; Laskey, D.A.; Dickson, J.E.; Coleman, C.I. The effect of grape seed extract on cardiovascular risk markers: A meta-analysis of randomized controlled trials. J. Am. Diet. Assoc. 2011, 111, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Zhou, R.; Wang, B.; Yu, X.; Yang, X.; Liu, K.; Mi, M. Effect of green tea consumption on blood pressure: A meta-analysis of 13 randomized controlled trials. Sci. Rep. 2014, 4, 6251. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Kay, C.; Abdelhamid, A.; Kroon, P.A.; Cohn, J.S.; Rimm, E.B.; Cassidy, A. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: A systematic review and meta-analysis of randomized trials. Am. J. Clin. Nutr. 2012, 95, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Bo, Y.; Wang, X.; Lu, W.; Wang, X.; Han, Z.; Qiu, C. The effect of anthocyanins on blood pressure: A prisma-compliant meta-analysis of randomized clinical trials. Medicine 2016, 95, e3380. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Simental-Mendia, L.E.; Giorgini, P.; Ferri, C.; Grassi, D. Lipid profile changes after pomegranate consumption: A systematic review and meta-analysis of randomized controlled trials. Phytomedicine 2016, 23, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Tokede, O.A.; Onabanjo, T.A.; Yansane, A.; Gaziano, J.M.; Djousse, L. Soya products and serum lipids: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2015, 114, 831–843. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Chen, C.; Wang, Y.; Liu, J.; Lin, R. Effect of black tea consumption on blood cholesterol: A meta-analysis of 15 randomized controlled trials. PLoS ONE 2014, 9, e107711. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; He, J.; Appel, L.J.; Cutler, J.A.; Havas, S.; Kotchen, T.A.; Roccella, E.J.; Stout, R.; Vallbona, C.; Winston, M.C.; et al. Primary prevention of hypertension: Clinical and public health advisory from the national high blood pressure education program. J. Am. Med. Assoc. 2002, 288, 1882–1888. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Morris, P.B.; Ballantyne, C.M.; Birtcher, K.K.; Daly, D.D., Jr.; DePalma, S.M.; Minissian, M.B.; Orringer, C.E.; Smith, S.C., Jr. 2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: A report of the American college of cardiology task force on clinical expert consensus documents. J. Am. Coll. Cardiol. 2016, 68, 92–125. [Google Scholar] [PubMed]
- Jia, L.; Liu, X.; Bai, Y.Y.; Li, S.H.; Sun, K.; He, C.; Hui, R. Short-term effect of cocoa product consumption on lipid profile: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2010, 92, 218–225. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year Country (Reference) | Type of RCT NT/NC Duration | Dose of Flavonol/Day 1 | Cardiometabolic Markers 2 | Risk of Bias 3 |
|---|---|---|---|---|
| Brull, 2015 Germany [31] | Crossover 68/68 42 days | 162 mg quercetin (OPE) | BP, TC, HDL, LDL, TAG, Glucose, Insulin, HOMA-IR, HbA1c | Low |
| Chen, 2015 China [39] | Parallel 30/30 84 days | 600 mg dihydromyricetin (commercial) | BMI, BP, TC, HDL, LDL, TAG, Glucose, Insulin, HOMA-IR | Low |
| Choi, 2015 Korea [43] | Parallel 34/38 84 days | 100 mg quercetin (OPE) | FMD, BMI, BP, TC, HDL, LDL, TAG, Glucose | Moderate |
| Chopra, 2000 Ireland [32] | Crossover 20/20 14 days | 30 mg quercetin aglycone (commercial) | TC, HDL, LDL, TAG | High |
| Conquer, 1998 Canada [38] | Parallel 13/14 28 days | 1000 mg quercetin + 200 mg rutin (commercial) | BP, TC, HDL, LDL, TAG | Moderate |
| Dower, 2015 Netherland [33] | Crossover 35/35 28 days | 160 mg quercetin-3-glucoside | FMD, BP, TC, HDL, LDL, TAG, Glucose, Insulin, HOMA-IR | Low |
| Edwards, 2007 USA [37] | Crossover 41/41 28 days | 728 mg quercetin aglycone (commercial) | BMI, BP, TC, HDL, LDL, TAG, Glucose | Moderate |
| Egert, 2009 Germany [29] | Crossover 93/93 42 days | 150 mg quercetin dehydrate (commercial) | BP, TC, HDL, LDL, TAG, Glucose | Low |
| Javadi, 2014 Iran [46] | Parallel 20/20 56 days | 500 mg quercetin (commercial) | BP | Moderate |
| Kim, 2013 Korea [42] | Crossover 12/12 14 days | 100 mg quercetin (OPE) | BP, TC, HDL, LDL | Moderate |
| Kim, 2015 Korea [44] | Parallel 18/19 84 days | 100 mg quercetin (OPE) | BMI, WC, BP, TC, HDL, LDL, TAG | Moderate |
| Larmo, 2009 Finland [35] | Parallel 115/114 90 days | 13 mg isorhamnetin + 3 mg quercetin (SBP) | TC, HDL, LDL, TAG | Low |
| Lee, 2011 Korea [41] | Parallel 49/43 70 days | 400 mg quercetin (OPE) | BMI, WC, BP, TC, HDL, LDL, TAG, Glucose | High |
| Lu, 2015 China [40] | Parallel 12/12 56 days | 6 mg quercetin (onion juice) | BMI, WC, TC, HDL, LDL, TAG | Moderate |
| Pfeuffer, 2013 Germany [30] | Crossover 49/49 56 days | 150 mg quercetin dehydrate (commercial) | BMI, WC, BP, TC, HDL, LDL, TAG, Glucose, Insulin, HOMA-IR, HbA1c | Moderate |
| Shi, 2016 UK [36] | Crossover 22/22 28 days | 500 mg quercetin aglycone (commercial) | BP, Glucose | Low |
| Suomela, 2006 Finland [34] | Crossover 14/14 28 days | 54 mg isorhamnetin + 20 mg quercetin (SBE) | TC, HDL, LDL, TAG, Glucose | Moderate |
| Zahedi, 2013 Iran [45] | Parallel 34/28 70 days | 500 mg quercetin (commercial) | TC, HDL, LDL, TAG | Moderate |
| First Author, Year (Reference) | Age (Mean, SD or Range) Sex (nM/nF) | Health Status 1 BMI (Mean, SD) Healthy/Disease Med/Smoking | Fasting Baseline Values 2 |
|---|---|---|---|
| Brull, 2015 [31] | 47.4 (10.5) 34 M/34 F | 31.1 (3.4) MS Med/non smokers | BP: Pre-HT/HT TC, HDL, LDL, TAG: borderline Glucose: normal |
| Chen, 2015 [39] | 45.1 (10.0) 40 M/20 F | 25.6 (2.6) NAFLD Not Med/smoking NR | BP: normal/pre-HT TC: normal/borderline, HDL: borderline LDL: normal, TAG: high Glucose: normal/IFG |
| Choi, 2015 [43] | 43.1 (6.7) 11 M/51 F | 26.6 (2.9) Healthy Med NR/5% smokers | BP: normal/pre-HT TC: normal,HDL: borderline LDL: normal/borderline, TAG: normal, Glucose: NR |
| Chopra, 2000 [32] | 46 (SD NR) 20 M | BMI NR Healthy Med NR/non smokers | BP: NR, TC, HDL, LDL: borderline, TAG: normal; Glucose: NR |
| Conquer, 1998 [38] | 42.0 (13.5) M/F (n NR) | 26.1 (4.4) Healthy Med NR/smoking NR | BP: normal TC, HDL, LDL,TAG: normal; Glucose: NR |
| Dower, 2015 [33] | 66.4 (7.9) 25 M/12 F | 26.7 (3.3) Healthy Not Med/non smokers | BP: normal/pre-HT TC, LDL: borderline, HDL: normal/borderline, TAG: normal Glucose: normal/IFG |
| Edwards, 2007 [37] Pre-HT group | 47.8 (15.2) 13 M/6 F | 29.8 (5.7) Healthy Not Med/non smokers | BP: pre-HT/HT1 TC, LDL: normal/borderline HDL: borderline, TAG—borderline/high Glucose: normal/IFG |
| HT1 group | 49.2 (13.6) 13 M/9 F | 29.5 (6.6) HT Not Med/non smokers | |
| Egert, 2009 [29] | 45.1 (10.5) 42 M/51 F | 30.6 (3.2) MS Med/non smokers | BP: normal/pre-HT TC, HDL, LDL, TAG: borderline/high Glucose: normal/IFG |
| Javadi, 2014 [46] | 47.3 (9.1) 40 F | 29.3 (4.5) RA Med/non smokers | BP: normal TC, HDL, LDL, TAG: NR Glucose: NR |
| Kim, 2013 [42] | 20–25 12 F | 20.2 (1.7) Healthy Not Med/smoking NR | BP: normal TC: NR HDL, LDL,TAG: normal Glucose: NR |
| Kim, 2015 [44] | 45.0 (8.5) 37 F | 26.6 (3.2) Healthy Not Med/smoking NR | BP: normal TC, LDL, TAG: normal HDL: borderline Glucose: NR |
| Larmo, 2009 [35] | 30.8 (8.7) 51 M/178 F | 23.1 (2.9) Healthy Not Med/7% smokers | BP: NR TC, HDL, LDL, TAG: normal Glucose: NR |
| Lee, 2011 [41] | 44.2 (7.8) 92 M | 24.8 (2.9) Healthy Not Med/smokers | BP: normal/pre-HT TC, LDL: normal HDL,TAG: borderline Glucose: normal/IFG |
| Lu, 2015 [40] | 35–55 10 M/13 F | 25.5 (2.6) Healthy Not Med/non smokers | BP: NR TC, HDL, LDL: borderline TAG: normal Glucose: NR |
| Pfeuffer, 2013 [30] | 59.4 (6.3) 49 M | 26.3 (2.1) Healthy Not Med/non smokers | BP: pre-HT TC, HDL, LDL: borderline TAG: normal Glucose: normal/IFG |
| Shi, 2016 [36] | 29.9 (12.9) 22 M | 24.8 (3.0) Healthy Med NR/non smokers | BP: normal/pre-HT TC, HDL, LDL, TAG: NR Glucose: normal/IFG |
| Suomela, 2006 [34] | 46.6 (5.6) 14 M | 25.8 (SD NR) Healthy Not Med/non smokers | BP: NR TC, HDL, LDL: borderline TAG: normal Glucose: normal |
| Zahedi, 2013 [45] | 35–55 62 F | BMI NR DM 2 Med/non smokers | BP: normal TC, LDL: normal HDL, TAG: borderline Glucose: NR |
| Factor Subgroups | TAG (mmol/L) DM (95% CI) 1 | TC (mmol/L) DM (95% CI) 1 | LDL (mmol/L) DM (95% CI) 1 | HDL (mmol/L) DM (95% CI) 1 |
|---|---|---|---|---|
| Age | ||||
| ≥40 | −0.11 (−0.35, 0.13) | −0.03 (−0.41, 0.36) | −0.08 (−0.38, 0.22) | 0.05 (−0.10, 0.19) |
| Mixed | −0.11 (−0.19, −0.02) * | −0.10 (−0.19, −0.00) | −0.09 (−0.18, −0.00) * | 0.04 (0.01, 0.08) * |
| Sex | ||||
| F | −0.14 (−0.40, 0.11) | −0.22 (−0.53, 0.09) | −0.12 (−0.41, −0.17) | 0.04 (−0.06, 0.14) |
| M | −0.10 (−0.42, 0.22) | −0.03 (−0.45, 0.39) | −0.07 (−0.41, 0.26) | 0.07 (−0.10, 0.23) |
| Mixed | −0.10 (−0.19, −0.02) * | −0.08 (−0.19, 0.02) | −0.09 (−0.18, 0.01) | 0.04 (0.01, 0.08) * |
| Country | ||||
| Asia | −0.17 (−0.32, −0.03) * | −0.24 (−0.43,−0.06) ** | −0.27 (−0.45,−0.09) ** | 0.05 (−0.01, 0.11) |
| EU/N. America | −0.08 (−0.17, 0.01) | −0.04 (−0.15, 0.07) | −0.04 (−0.13, 0.06) | 0.04 (−0.00, 0.09) |
| BMI | ||||
| Normal | −0.06 (−0.16, 0.00) | −0.05 (−0.18, 0.08) | −0.02 (−0.13, 0.09) | 0.04 (−0.01, 0.09) |
| Overweight | −0.20 (−0.40, 0.01) | −0.07 (−0.31, 0.16) | −0.08 (−0.29, 0.13) | 0.03 (−0.61, 0.12) |
| Mixed | −0.14 (−0.27, −0.00) * | −0.23 (−0.40, −0.05) * | −0.28 (−0.46, −0.10) ** | 0.07 (0.01, 0.14) * |
| Disease | ||||
| With disease | −0.20 (−0.43, 0.04) | −0.13 (−0.33, 0.07) | −0.20 (−0.38, −0.02) * | 0.06 (−0.01, 0.12) |
| No disease | −0.08 (−0.17, 0.00) | −0.08 (−0.20, 0.02) | −0.05 (−0.15, 0.05) | 0.05 (0.00, 0.09) * |
| Baseline levels | ||||
| Normal | −0.21 (−0.43, 0.02) | −0.08 (−0.19, 0.04) | −0.08 (−0.18, 0.01) | 0.04 (−0.01, 0.09) |
| Dyslipidemia | −0.09 (−0.18, −0.01) * | −0.10 (−0.32, 0.12) | −0.1 (−0.30, 0.08) | 0.05 (0.00, 0.10) * |
| Factor Subgroups | TAG (mmol/L) DM (95% CI) 1 | TC (mmol/L) DM (95% CI) 1 | LDL (mmol/L) DM (95% CI) 1 | HDL (mmol/L) DM (95% CI) 1 |
|---|---|---|---|---|
| Compound | ||||
| Pure | −0.17 (−0.35, 0.00) * | −0.12 (−0.31, 0.06) | −0.18 (−0.34, 0.02) * | 0.06 (−0.01, 0.12) |
| Mixture | −0.10 (−0.18, −0.04) * | −0.09 (−0.20, 0.02) | −0.06 (−0.16, 0.04) | 0.04 (−0.00, 0.08) |
| Dose | ||||
| >200 (mg/day) | −0.22 (−0.18, 0.00) | −0.20 (−0.43, 0.03) | −0.27 (−0.48, −0.06) * | 0.06 (−0.02, 0.13) |
| <200 (mg/day) | −0.10 (−0.18, −0.02) * | −0.08 (−0.18, 0.03) | −0.05 (−0.15, 0.04) | 0.04 (−0.00, 0.08) * |
| Biomarker | n (NT/NC) | DM (95% CI), p Value | GRADE 1 |
|---|---|---|---|
| TAG (mmol/L) | 17 (467/456) | −0.10 (−0.18; −0.03) p = 0.007 | Low 2,3 |
| TC (mmol/L) | 18 (473/462) | −0.10 (−0.20; −0.01) p = 0.023 | Moderate 2 |
| LDL (mmol/L) | 18 (473/462) | −0.14 (−0.21; −0.07) p = 0.000 | Moderate 2 |
| HDL (mmol/L) | 18 (473/462) | 0.05 (0.02; 0.07) p = 0.000 | Moderate 2 |
| SBP (mmHg) | 16 (370/362) | −4.84 (−5.64; −4.04) p = 0.000 | Low 2,3 |
| DBP (mmHg) | 16 (370/362) | −3.32 (−4.09; −2.55) p = 0.000 | Low 2,3 |
| Glucose (mmol/L) | 12 (276/270) | −0.18 (−0.29; −0.07) p = 0.001 | Moderate 2 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menezes, R.; Rodriguez‐Mateos, A.; Kaltsatou, A.; González‐Sarrías, A.; Greyling, A.; Giannaki, C.; Andres‐Lacueva, C.; Milenkovic, D.; Gibney, E.R.; Dumont, J.; et al. Impact of Flavonols on Cardiometabolic Biomarkers: A Meta‐Analysis of Randomized Controlled Human Trials to Explore the Role of Inter‐Individual Variability. Nutrients 2017, 9, 117. https://doi.org/10.3390/nu9020117
Menezes R, Rodriguez‐Mateos A, Kaltsatou A, González‐Sarrías A, Greyling A, Giannaki C, Andres‐Lacueva C, Milenkovic D, Gibney ER, Dumont J, et al. Impact of Flavonols on Cardiometabolic Biomarkers: A Meta‐Analysis of Randomized Controlled Human Trials to Explore the Role of Inter‐Individual Variability. Nutrients. 2017; 9(2):117. https://doi.org/10.3390/nu9020117
Chicago/Turabian StyleMenezes, Regina, Ana Rodriguez‐Mateos, Antonia Kaltsatou, Antonio González‐Sarrías, Arno Greyling, Christoforos Giannaki, Cristina Andres‐Lacueva, Dragan Milenkovic, Eileen R. Gibney, Julie Dumont, and et al. 2017. "Impact of Flavonols on Cardiometabolic Biomarkers: A Meta‐Analysis of Randomized Controlled Human Trials to Explore the Role of Inter‐Individual Variability" Nutrients 9, no. 2: 117. https://doi.org/10.3390/nu9020117