Validity of the Food Frequency Questionnaire Assessing the Folate Intake in Women of Reproductive Age Living in a Country without Food Fortification: Application of the Method of Triads

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
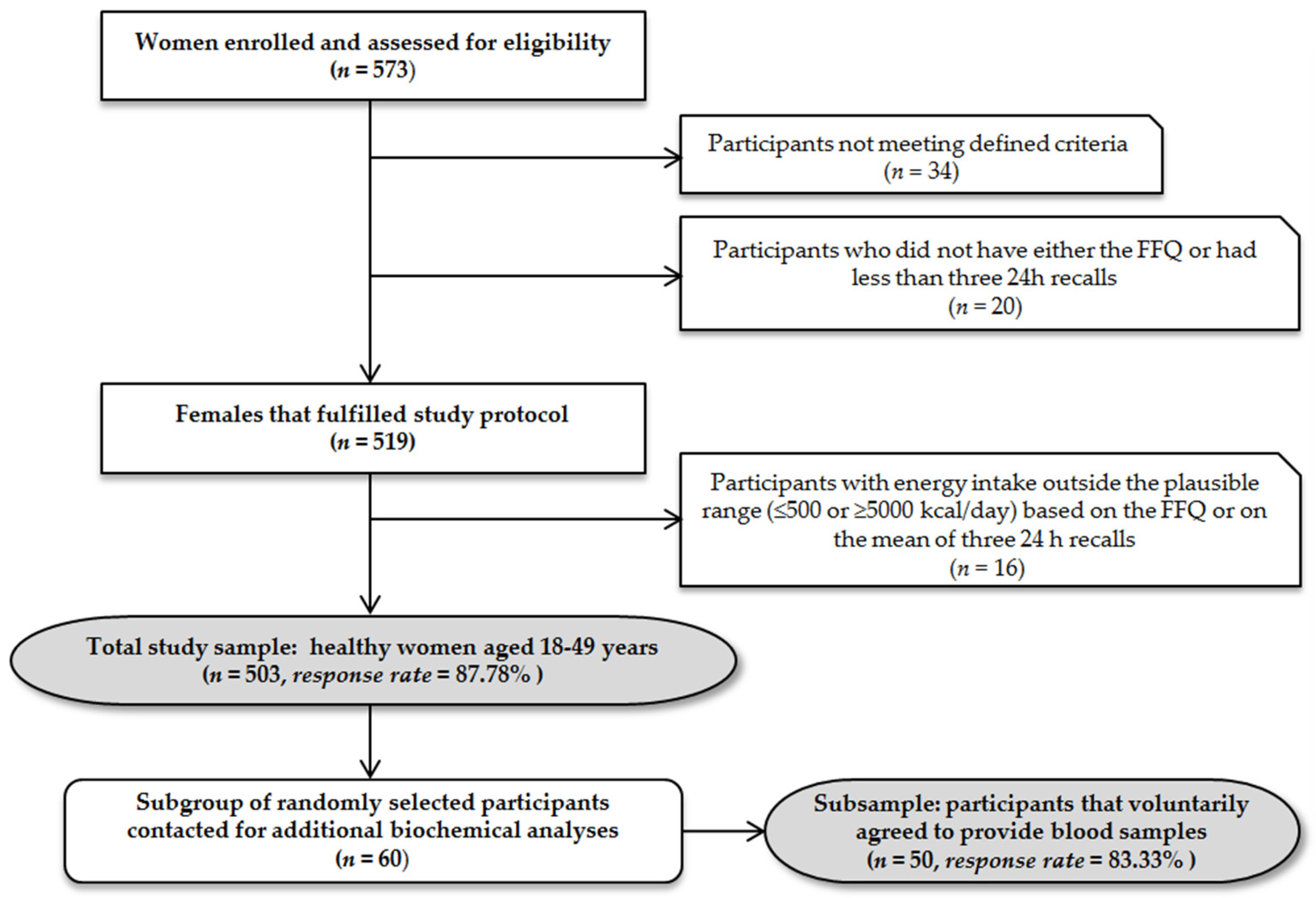
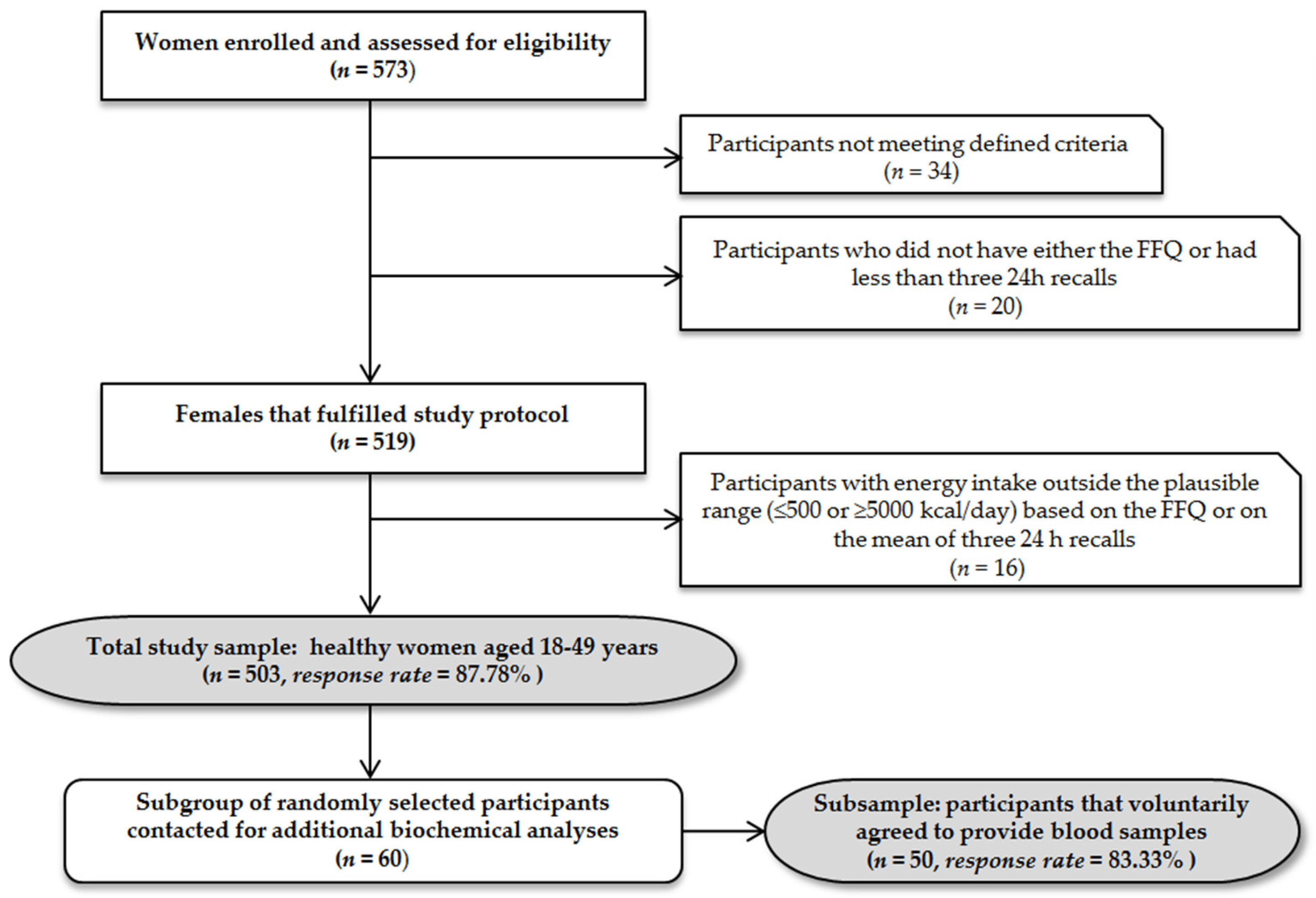
2.1. Study Participants
2.2. Anthropometry
2.3. Food Frequency Questionnaire
2.4. Twenty-Four-Hour Dietary Recalls
2.5. Dietary Data Assessment
2.6. Biochemical Assessment
2.7. Statistical Analyses
2.8. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Safi, J.; Joyeux, L.; Chalouhi, G.E.; Safi, J.; Joyeux, L.; Chalouhi, G.E. Periconceptional Folate Deficiency and Implications in Neural Tube Defects. J. Pregnancy 2012, 2012, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Eichholzer, M.; Tönz, O.; Zimmermann, R. Folic acid: A public-health challenge. Lancet 2006, 367, 1352–1361. [Google Scholar] [CrossRef]
- Lucock, M. Folic acid: Nutritional biochemistry, molecular biology, and role in disease processes. Mol. Genet. Metab. 2000, 71, 121–138. [Google Scholar] [CrossRef]
- Krishnaswamy, K.; Madhavan Nair, K. Importance of folate in human nutrition. Br. J. Nutr. 2001, 85 (Suppl. 2), S115–S124. [Google Scholar] [CrossRef] [PubMed]
- Crider, K.S.; Bailey, L.B.; Berry, R.J. Folic acid food fortification-its history, effect, concerns, and future directions. Nutrients 2011, 3, 370–384. [Google Scholar] [CrossRef] [PubMed]
- Mcnulty, H.; Pentieva, K. Folate bioavailability. Proc. Nutr. Soc. 2004, 63, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Wald, N.J.; Law, M.R.; Morris, J.K.; Wald, D.S. Quantifying the effect of folic acid. Lancet 2001, 358, 2069–2073. [Google Scholar] [CrossRef]
- Blom, H.J. Folic acid, methylation and neural tube closure in humans. Birth Defects Res. Part A Clin. Mol. Teratol. 2009, 85, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Sedgh, G.; Hussain, R. Unintended pregnancy: Worldwide levels, trends, and outcomes. Stud. Fam. Plan. 2010, 41, 241–250. [Google Scholar] [CrossRef]
- World Health Organization; Food and Agricultural Organization of the United Nations. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Gomes, S.; Lopes, C.; Pinto, E. Folate and folic acid in the periconceptional period: Recommendations from official health organizations in thirty-six countries worldwide and WHO. Public Health Nutr. 2016, 19, 176–189. [Google Scholar] [CrossRef] [PubMed]
- Gurinovic, M.; Kadvan, A.; Vukotic, M. The quality of nutrition of schoolchildren and adult members of families. In Yugoslav Study of Atherososclerosis Precursors in Schoolchildren in Serbia: Twenty Years Follow-Up; Nedeljkovic, S., Ed.; Medical Faculty University of Belgrade: Belgrade, Serbia, 2011; pp. 343–368. [Google Scholar]
- Odalovic, M.; Vezmar Kovacevic, S.; Ilic, K.; Sabo, A.; Tasic, L. Drug use before and during pregnancy in Serbia. Int. J. Clin. Pharm. 2012, 34, 719–727. [Google Scholar] [CrossRef] [PubMed]
- McNulty, H.; Scott, J.M. Intake and status of folate and related B-vitamins: Considerations and challenges in achieving optimal status. Br. J. Nutr. 2008, 99 (Suppl. 3), S48–S54. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wahlqvist, M.L.; Li, D. Nutrition, One-Carbon Metabolism and Neural Tube Defects: A Review. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Khoshnood, B.; Loane, M.; de Walle, H.; Arriola, L.; Addor, M.-C.; Barisic, I.; Beres, J.; Bianchi, F.; Dias, C.; Draper, E.; et al. Long term trends in prevalence of neural tube defects in Europe: Population based study. BMJ 2015, 351, h5949. [Google Scholar] [CrossRef] [PubMed]
- Pietruszka, B.; Brzozowska, A. Folic acid supplementation practice in Europe-Plenary lecture. Polish J. Food Nutr. Sci. 2006, 15/56, 93–99. [Google Scholar]
- Willett, W.; Lenart, E. Reproducibility and Validity of Food Frequency Questionnaires. In Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 2013; pp. 96–141. [Google Scholar]
- Jain, M.G.; Rohan, T.E.; Soskolne, C.L.; Kreiger, N. Calibration of the dietary questionnaire for the Canadian Study of Diet, Lifestyle and Health cohort. Public Health Nutr. 2003, 6, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Ocké, M.C.; Kaaks, R.J. Biochemical markers as additional measurements in dietary validity studies: Application of the method of triads with examples from the European Prospective Investigation into Cancer and Nutrition. Am. J. Clin. Nutr. 1997, 65, 1240S–1245S. [Google Scholar] [PubMed]
- Kaaks, R.J. Biochemical markers as additional measurements in studies of the accuracy of dietary questionnaire measurements: Conceptual issues. Am. J. Clin. Nutr. 1997, 65, 1232S–1239S. [Google Scholar] [PubMed]
- Potischman, N. Biologic and methodologic issues for nutritional biomarkers. J. Nutr. 2003, 133 (Suppl.), 875S–880S. [Google Scholar] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Barić, I.C.; Šatalić, Z.; Keser, I.; Cecić, I.; Sučić, M. Validation of the folate food frequency questionnaire with serum and erythrocyte folate and plasma homocysteine. Int. J. Food Sci. Nutr. 2009, 60, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Subar, A.F. Estimates of nutrient intake from a food frequency questionnaire: The 1987 National Health Interview Survey. J. Am. Diet. Assoc. 1992, 92, 969–977. [Google Scholar] [PubMed]
- Gurinovic, M.; Milešević, J.; Kadvan, A.; Nikolić, M.; Djekić-Ivanković, M.; Dupouy, E.; Finglas, P.; Glibetić, M. Advances in capacity development by applying Diet Asses Plan-DAP platform and tools for public health nutrition research and policies implementation in Balkan region. In 11th International Food Data Conference (IFDC), Food Composition and Public Health Nutrition; Longvah, T., Ed.; National Institute of Nutrition: Hyderabad, India, 2015; p. 105. [Google Scholar]
- Gurinović, M.; Milešević, J.; Kadvan, A.; Nikolić, M.; Zeković, M.; Djekić-Ivanković, M.; Dupouy, E.; Finglas, P.; Glibetić, M. Development, features and application of Diet Assess&Plan (DAP) software in supporting public health nutrition research in Central Eastern European Countries (CEEC). Food Chem. 2016. [Google Scholar] [CrossRef]
- Gurinović, M.; Milešević, J.; Novaković, R.; Kadvan, A.; Djekić-Ivanković, M.; Šatalić, Z.; Korošec, M.; Spiroski, I.; Ranić, M.; Dupouy, E.; Oshaug, A.; Finglas, P.; Glibetić, M. Improving nutrition surveillance and public health research in Central and Eastern Europe/Balkan Countries using the Balkan Food Platform and dietary tools. Food Chem. 2016, 193, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Gavrieli, A.; Naska, A.; Konstantinidi, C.; Berry, R.; Roe, M.; Harvey, L.; Finglas, P.; Glibetic, M.; Gurinovic, M.; Trichopoulou, A. Dietary Monitoring Tools for Risk Assessment. EFSA Support. Publ. 2014, 11. [Google Scholar] [CrossRef]
- Gurinović, M.; Milešević, J.; Kadvan, A.; Djekić-Ivanković, M.; Debeljak-Martačić, J.; Takić, M.; Nikolić, M.; Ranković, S.; Finglas, P.; Glibetić, M. Establishment and advances in the online Serbian food and recipe data base harmonized with EuroFIRTM standards. Food Chem. 2016, 193, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Abbott Laboratoires. Operator Manual ARCHITECT i2000 SR Abbott Diagnostic Folate; Abbott Laboratories: Abbott Park, IL, USA, 2010. [Google Scholar]
- World Health Organization. Serum and Red Blood Cell Folate Concentrations for Assessing Folate Status in Populations; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. Guideline: Optimal Serum and Red Cell Folate Concentrations in Women of Reproductive Age for Prevention of Neural Tube Defects; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [PubMed]
- Van Belle, G.; Fisher, L.D.; Heagerty, P.J.; Lumley, T. Descriptive Statistics. In Biostatistics: A Methodology For the Health Sciences; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004; pp. 25–61. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Kabagambe, E.K.; Baylin, A.; Allan, D.A.; Siles, X.; Spiegelman, D.; Campos, H. Application of the method of triads to evaluate the performance of food frequency questionnaires and biomarkers as indicators of long-term dietary intake. Am. J. Epidemiol. 2001, 154, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Johansson, I.; Van Guelpen, B.; Hultdin, J.; Johansson, M.; Hallmans, G.; Stattin, P. Validity of food frequency questionnaire estimated intakes of folate and other B vitamins in a region without folic acid fortification. Eur. J. Clin. Nutr. 2010, 64, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Verkleij-Hagoort, A.C.; de Vries, J.H.M.; Stegers, M.P.G.; Lindemans, J.; Ursem, N.T.C.; Steegers-Theunissen, R.P.M. Validation of the assessment of folate and vitamin B12 intake in women of reproductive age: The method of triads. Eur. J. Clin. Nutr. 2007, 61, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Agodi, A.; Barchitta, M.; Quattrocchi, A.; Marchese, A.E.; Boffetta, P. Folate deficiency is not associated with increased mitochondrial genomic instability: Results from dietary intake and lymphocytic mtDNA 4977-bp deletion in healthy young women in Italy. Mutagenesis 2014, 29, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Brevik, A.; Vollset, S.E.; Tell, G.S.; Refsum, H.; Ueland, P.M.; Loeken, E.B.; Drevon, C.A.; Andersen, L.F. Plasma concentration of folate as a biomarker for the intake of fruit and vegetables: The Hordaland Homocysteine Study. Am. J. Clin. Nutr. 2005, 81, 434–439. [Google Scholar] [PubMed]
- Waśkiewicz, A.; Sygnowska, E.; Broda, G. Dietary intake of vitamins B6, B12 and folate in relation to homocysteine serum concentration in the adult Polish population - WOBASZ Project. Kardiol. Pol. 2010, 68, 275–282. [Google Scholar] [PubMed]
- Alfthan, G.; Laurinen, M.S.; Valsta, L.M.; Pastinen, T.; Aro, A. Folate intake, plasma folate and homocysteine status in a random Finnish population. Eur. J. Clin. Nutr. 2003, 57, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Manios, Y.; Moschonis, G.; Mavrogianni, C.; Bos, R.; Singh-Povel, C. Micronutrient intakes among children and adults in Greece: The role of age, sex and socio-economic status. Nutrients 2014, 6, 4073–4092. [Google Scholar] [CrossRef] [PubMed]
- Elmadfa, I.; Meyer, A.L. Austrian Nutrition Report 2012; Federal Ministry of Health, University of Vienna, Institute of Nutritional Sciences: Vienna, Austria, 2012. [Google Scholar]
- Planells, E.; Sánchez, C.; Montellano, M.A.; Mataix, J.; Llopis, J. Vitamins B6 and B12 and folate status in an adult Mediterranean population. Eur. J. Clin. Nutr. 2003, 57, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Nicolas, G.; Freisling, H.; Biessy, C.; Scalbert, A.; Romieu, I.; Chajès, V.; Chuang, S.-C.; Ericson, U.; Wallström, P.; et al. Comparison of standardised dietary folate intake across ten countries participating in the European Prospective Investigation into Cancer and Nutrition. Br. J. Nutr. 2012, 108, 552–569. [Google Scholar] [CrossRef] [PubMed]
- Elmadfa, I.; Meyer, A.; Nowak, V.; Hasenegger, V.; Putz, P.; Verstraeten, R.; Remaut-DeWinter, A.M.; Kolsteren, P.; Dostálová, J.; Dlouhý, P.; et al. European Nutrition and Health Report 2009. Forum Nutr. 2009, 62, 1–405. [Google Scholar] [PubMed]
- Hoey, L.; McNulty, H.; Duffy, M.E.; Hughes, C.F.; Strain, J.J. EURRECA-Estimating folate requirements for deriving dietary reference values. Crit. Rev. Food Sci. Nutr. 2013, 53, 1041–1050. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, S.; Doperé, I.; Huybrechts, I.; Godderis, L.; Koppen, G.; Vansant, G. Reproducibility and validity of an FFQ to assess usual intake of methyl-group donors. Public Health Nutr. 2015, 18, 2530–2539. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.D.; Walker, S.P.; Younger, N.M.; Bennett, F.I. Use of a food frequency questionnaire to assess diets of Jamaican adults: Validation and correlation with biomarkers. Nutr. J. 2011, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Pufulete, M.; Emery, P.W.; Nelson, M.; Sanders, T.A.B. Validation of a short food frequency questionnaire to assess folate intake. Br. J. Nutr. 2002, 87, 383–390. [Google Scholar] [CrossRef] [PubMed]
- French, M.R.; Langdon, C.; Levy-Milne, R. Development of a validated food frequency questionnaire to determine folate intake. Can. J. Diet. Pract. Res. Publ. Dietit. Can. 2001, 62, 82–86. [Google Scholar]
- Coathup, V.; Wheeler, S.; Smith, L. A method comparison of a food frequency questionnaire to measure folate, choline, betaine, vitamin C and carotenoids with 24 h dietary recalls in women of reproductive age. Eur. J. Clin. Nutr. 2015, 70, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Fayet, F.; Flood, V.; Petocz, P.; Samman, S. Relative and biomarker-based validity of a food frequency questionnaire that measures the intakes of vitamin B 12, folate, iron, and zinc in young women. Nutr. Res. 2011, 31, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Brantsaeter, A.L.; Haugen, M.; Alexander, J.; Meltzer, H.M. Validity of a new food frequency questionnaire for pregnant women in the Norwegian Mother and Child Cohort Study (MoBa). Matern. Child Nutr. 2008, 4, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.B.; Stover, P.J.; Mcnulty, H.; Fenech, M.F.; Iii, J.F.G.; Mills, J.L.; Pfeiffer, C.M.; Fazili, Z.; Zhang, M.; Ueland, P.M.; et al. Biomarkers of Nutrition for Development—Folate Review 1–5. J. Nutr. 2015, 145, 1636S–1680S. [Google Scholar] [CrossRef] [PubMed]
- Flood, V.M.; Smith, W.T.; Webb, K.L.; Mitchell, P. Issues in assessing the validity of nutrient data obtained from a food-frequency questionnaire: Folate and vitamin B12 examples. Public Health Nutr. 2007, 7, 751–756. [Google Scholar] [CrossRef]
- Djekic-Ivankovic, M.; Weiler, H.A.; Nikolic, M.; Kadvan, A.; Gurinovic, M.; Mandic, L.M.; Glibetic, M. Validity of an FFQ assessing the vitamin D intake of young Serbian women living in a region without food fortification: The method of triads model. Public Health Nutr. 2015, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Combet, E.; Lean, M.E.J. Validation of a short food frequency questionnaire specific for iodine in U.K. females of childbearing age. J. Hum. Nutr. Diet. 2014, 27, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, S.; Doperé, I.; Huybrechts, I.; Godderis, L.; Koppen, G.; Vansant, G. Validation of a food-frequency questionnaire assessment of methyl-group donors using estimated diet records and plasma biomarkers: The method of triads. Int. J. Food Sci. Nutr. 2014, 65, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Shai, I.; Rosner, B.A.; Shahar, D.R.; Vardi, H.; Azrad, A.B.; Kanfi, A.; Schwarzfuchs, D.; Fraser, D. Dietary evaluation and attenuation of relative risk: Multiple comparisons between blood and urinary biomarkers, food frequency, and 24-h recall questionnaires: The DEARR study. J. Nutr. 2005, 135, 573–579. [Google Scholar] [PubMed]
- McNaughton, S.A.; Marks, G.C.; Gaffney, P.; Williams, G.; Green, A. Validation of a food-frequency questionnaire assessment of carotenoid and vitamin E intake using weighed food records and plasma biomarkers: The method of triads model. Eur. J. Clin. Nutr. 2005, 59, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Shuaibi, A.M.; Sevenhuysen, G.P.; House, J.D. Validation of a Food Choice Map with a 3-Day Food Record and Serum Values to Assess Folate and Vitamin B-12 Intake in College-Aged Women. J. Am. Diet. Assoc. 2008, 108, 2041–2050. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Frost Andersen, L.; Henríque-Sánchez, P.; Doreste-Alonso, J.; Sánchez-Villegas, A.; Ortiz-Andrelluchi, A.; Negri, E.; La Vecchia, C. Evaluating the quality of dietary intake validation studies. Br. J. Nutr. 2009, 102, S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Teufel, N.I. Development of culturally competent food-frequency questionnaires. Am. J. Clin. Nutr. 1997, 65, 1173S–1178S. [Google Scholar] [PubMed]
- Altman, D.G. Practical Statistics For Medical Research; Chapman & Hall/CRC: London, UK, 1991. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nutrient | Total Sample (n = 503) | Pearson Correlation Coefficient | Validation Group (n = 50) | Pearson Correlation Coefficient | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F-FFQ | 24 h Recalls | F-FFQ | 24 h Recalls | |||||||
| Mean | SD | Mean | SD | r | Mean | SD | Mean | SD | r | |
| Energy (kcal) | 1724.62 | 330.02 | 1734.20 | 318.50 | 0.53 ** | 1727.29 | 200.36 | 1718.93 | 219.40 | 0.59 ** |
| Carbohydrates (% TEI) | 52.23 | 9.21 | 50.94 | 7.23 | 51.02 | 5.51 | 49.88 | 6.08 | ||
| Carbohydrates (g) | 225.19 | 42.72 | 220.85 | 59.78 | 0.51 * | 220.31 | 23.58 | 214.35 | 28.21 | 0.52 ** |
| Fat (% TEI) | 27.81 | 10.61 | 28.30 | 7.21 | 29.34 | 6.74 | 31.41 | 6.30 | ||
| Fat (g) | 53.29 | 23.90 | 54.53 | 23.72 | 0.41 ** | 56.31 | 14.90 | 59.99 | 14.85 | 0.47 * |
| Protein (% TEI) | 19.52 | 2.93 | 20.22 | 3.50 | 19.20 | 2.05 | 18.49 | 2.62 | ||
| Protein (g) | 84.16 | 13.87 | 87.66 | 17.51 | 0.39 ** | 82.91 | 7.38 | 79.46 | 8.92 | 0.40 * |
| Folate (µg/1000 kcal) | 118.98 | 35.44 | 121.66 | 42.73 | 0.53 ** | 123.95 | 32.27 | 119.90 | 35.76 | 0.53 ** |
| Folate (µg) | 205.20 | 61.30 | 211.00 | 81.06 | 0.56 ** | 214.10 | 60.78 | 206.10 | 65.31 | 0.57 ** |
| Food Groups | Intake of the Food Group (g/Day) | Contribution to Total Folate Intake | |||
|---|---|---|---|---|---|
| Median | P5 | P95 | % | Folate Intake (µg/Day) | |
| Vegetables and vegetable products | 175.07 | 63.95 | 318.20 | 37.35 | 79.66 |
| Grains and grain products | 195.91 | 90.68 | 338.82 | 23.39 | 49.89 |
| Fruits and fruit products | 130.75 | 9.31 | 378.17 | 11.52 | 24.57 |
| Milk and milk products | 241.69 | 15.68 | 481.12 | 10.48 | 22.35 |
| Meat and meat products | 95.62 | 12.31 | 200.87 | 5.77 | 12.31 |
| Nuts, seeds and kernel products | 6.00 | 0.00 | 66.00 | 3.01 | 6.42 |
| Beverages (non-milk) | 1.14 | 0.04 | 32.59 | 2.6 | 5.55 |
| Miscellaneous | 5.87 | 0.00 | 78.48 | 2.3 | 4.91 |
| Eggs and egg products | 8.88 | 0.00 | 64.10 | 1.45 | 3.09 |
| Sea food and related products | 0.00 | 0.00 | 107.45 | 1.11 | 2.37 |
| Sugar and sugar products | 17.55 | 0.75 | 64.97 | 0.98 | 2.09 |
| Fat and oil | 11.69 | 0.00 | 32.62 | 0.04 | 0.09 |
| Food | 24 h Dietary Recall (n = 503) | F-FFQ (n = 503) | |||
|---|---|---|---|---|---|
| µg DFE/Day (Total Sample) | µg DFE/Day (Consumers Only) | Number of Consumers | % of Consumers | Average Frequency of Consumption | |
| Bread white | 15.67 | 30.11 | 328 | 65.21 | every day |
| Beans | 10.08 | 218.38 | 434 | 86.28 | 2–3 times per month |
| Tomato, raw | 9.45 | 18.75 | 482 | 95.83 | 4–6 times a week |
| Yoghurt 2.8% mf | 7.65 | 16.05 | 419 | 83.30 | once a week |
| Chicken, liver | 7.14 | 251.19 | 456 | 90.66 | once a week |
| Peas, green | 6.11 | 93.57 | 422 | 83.90 | 2–3 times per month |
| Banana, raw | 6.06 | 48.38 | 492 | 97.81 | 2–3 times per week |
| Egg, hen, whole | 5.78 | 22.45 | 487 | 96.82 | 2–3 times per week |
| Pepper, red | 5.03 | 51.07 | 321 | 63.82 | 2–3 times per month |
| Potato | 4.98 | 12.91 | 225 | 44.73 | 2–3 times per month |
| Strawberries, raw | 4.84 | 26.95 | 419 | 83.30 | once a week |
| String beans | 4.43 | 67.11 | 248 | 49.30 | 2–3 times per month |
| Lettuce, green leaf | 4.29 | 17.98 | 354 | 70.38 | 2–3 times per month |
| Orange juice, fresh | 3.17 | 62.16 | 232 | 46.12 | once a week |
| Cabbage, white | 2.71 | 12.06 | 393 | 78.13 | 2–3 times per month |
| Quartiles | Folate Intake (µg/Day) | n | Serum Folate (nmol/L) | RBC Folate (nmol/L) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | 95% CI | p for Trend | Mean | 95% CI | p for Trend | |||
| 1st quartile | <168.43 (147.31) | 13 | 9.54 | 5.73–13.35 | 378.29 | 304.73–451.84 | ||
| 2nd quartile | 168.43–194.12 (182,60) | 13 | 11.48 | 7.51–15.45 | 399.05 | 306.61–491.48 | ||
| 3rd quartile | 194.12–245.62 (217.37) | 12 | 12.18 | 8.78–15.58 | 447.27 | 358.51–536.02 | ||
| 4th quartile | 245.62–362.34 (306.81) | 12 | 15.90 | 11.51–20.29 | 0.0139 | 526.05 | 444.62–607.48 | 0.0113 |
| Folate Intake/Status Assessed by | Folate Intake Assessed by F-FFQ | |||
|---|---|---|---|---|
| Same Quartile | Same or Adjacent Quartile | Opposite Quartile | Grossly Misclassified | |
| 24 h recall | 68 | 84 | 12 | 4 |
| Folate RBC | 50 | 82 | 14 | 4 |
| Folate serum | 48 | 82 | 12 | 6 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zekovic, M.; Djekic-Ivankovic, M.; Nikolic, M.; Gurinovic, M.; Krajnovic, D.; Glibetic, M. Validity of the Food Frequency Questionnaire Assessing the Folate Intake in Women of Reproductive Age Living in a Country without Food Fortification: Application of the Method of Triads. Nutrients 2017, 9, 128. https://doi.org/10.3390/nu9020128
Zekovic M, Djekic-Ivankovic M, Nikolic M, Gurinovic M, Krajnovic D, Glibetic M. Validity of the Food Frequency Questionnaire Assessing the Folate Intake in Women of Reproductive Age Living in a Country without Food Fortification: Application of the Method of Triads. Nutrients. 2017; 9(2):128. https://doi.org/10.3390/nu9020128
Chicago/Turabian StyleZekovic, Milica, Marija Djekic-Ivankovic, Marina Nikolic, Mirjana Gurinovic, Dusanka Krajnovic, and Marija Glibetic. 2017. "Validity of the Food Frequency Questionnaire Assessing the Folate Intake in Women of Reproductive Age Living in a Country without Food Fortification: Application of the Method of Triads" Nutrients 9, no. 2: 128. https://doi.org/10.3390/nu9020128
APA StyleZekovic, M., Djekic-Ivankovic, M., Nikolic, M., Gurinovic, M., Krajnovic, D., & Glibetic, M. (2017). Validity of the Food Frequency Questionnaire Assessing the Folate Intake in Women of Reproductive Age Living in a Country without Food Fortification: Application of the Method of Triads. Nutrients, 9(2), 128. https://doi.org/10.3390/nu9020128