Polyunsaturated Fatty Acid Levels in Maternal Erythrocytes of Japanese Women during Pregnancy and after Childbirth

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Blood Sampling
2.3. Fatty Acid Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Koletzko, B.; Lien, E.; Agostoni, C.; Bohles, H.; Campoy, C.; Cetin, I.; Decsi, T.; Dudenhausen, J.W.; Dupont, C.; Forsyth, S.; et al. The roles of long-chain polyunsaturated fatty acids in pregnancy, lactation and infancy: Review of current knowledge and consensus recommendations. J. Perinat. Med. 2008, 36, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M. Tissue levels of polyunsaturated fatty acids during early human development. J. Pediatr. 1992, 120, S129–S138. [Google Scholar] [CrossRef]
- Kuipers, R.S.; Luxwolda, M.F.; Offringa, P.J.; Boersma, E.R.; Dijck-Brouwer, D.A.; Muskiet, F.A. Gestational age dependent changes of the fetal brain, liver and adipose tissue fatty acid compositions in a population with high fish intakes. Prostaglandins Leukot Essent. Fat. Acids 2012, 86, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Bakker, E.C.; Hornstra, G.; Blanco, C.E.; Vles, J.S. Relationship between long-chain polyunsaturated fatty acids at birth and motor function at 7 years of age. Eur. J. Clin. Nutr. 2009, 63, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Bouwstra, H.; Dijck-Brouwer, J.; Decsi, T.; Boehm, G.; Boersma, E.R.; Muskiet, F.A.; Hadders-Algra, M. Neurologic condition of healthy term infants at 18 months: Positive association with venous umbilical DHA status and negative association with umbilical trans-fatty acids. Pediatr. Res. 2006, 60, 334–339. [Google Scholar] [CrossRef] [PubMed]
- The Ministry of Health, Labour and Welfare, Japan. National Health and Nutrition Survey Reports. Available online: http://www.mhlw.go.jp/stf/houdou/0000142359.html (accessed on 18 February 2017).
- Kawabata, T.; Hirota, S.; Hirayama, T.; Adachi, N.; Hagiwara, C.; Iwama, N.; Kamachi, K.; Araki, E.; Kawashima, H.; Kiso, Y. Age-related changes of dietary intake and blood eicosapentaenoic acid, docosahexaenoic acid, and arachidonic acid levels in Japanese men and women. Prostaglandins Leukot Essent. Fat. Acids 2011, 84, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, N.; Shimada, K.; Miyazaki, T.; Kume, A.; Kitamura, Y.; Ichikawa, R.; Ohmura, H.; Kiyanagi, T.; Hiki, M.; Fukao, K.; et al. Polyunsaturated fatty acid levels of serum and red blood cells in apparently healthy Japanese subjects living in an urban area. J. Atheroscler. Thromb. 2010, 17, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Hamazaki-Fujita, N.; Itomura, M.; Hamazaki, K.; Tohno, H.; Yomoda, S.; Terashima, Y.; Hamazaki, T. Relationships among skin conditions, mood, and polyunsaturated fatty acids of RBCs in healthy women. J. Cosmet. Sci 2012, 63, 303–310. [Google Scholar] [PubMed]
- Okuno, M.; Hamazaki, K.; Ogura, T.; Kitade, H.; Matsuura, T.; Yoshida, R.; Hijikawa, T.; Kwon, M.; Arita, S.; Itomura, M.; et al. Abnormalities in fatty acids in plasma, erythrocytes and adipose tissue in Japanese patients with colorectal cancer. In Vivo 2013, 27, 203–210. [Google Scholar] [PubMed]
- Kawabata, T.; Hirota, S.; Hirayama, T.; Adachi, N.; Kaneko, Y.; Iwama, N.; Kamachi, K.; Araki, E.; Kawashima, H.; Kiso, Y. Associations between dietary n-6 and n-3 fatty acids and arachidonic acid compositions in plasma and erythrocytes in young and elderly Japanese volunteers. Lipids Health Dis. 2011, 10, 138. [Google Scholar] [CrossRef] [PubMed]
- Donahue, S.M.; Rifas-Shiman, S.L.; Olsen, S.F.; Gold, D.R.; Gillman, M.W.; Oken, E. Associations of maternal prenatal dietary intake of n-3 and n-6 fatty acids with maternal and umbilical cord blood levels. Prostaglandins Leukot Essent. Fat. Acids 2009, 80, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Zhou, T.; Wang, Q.; Liu, P.; Zhang, T.; Zetterstrom, R.; Strandvik, B. Fatty acid composition of diet, cord blood and breast milk in Chinese mothers with different dietary habits. Prostaglandins Leukot Essent. Fat. Acids 2009, 81, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, C.; Gao, Y.; Li, L.; Man, Q.; Song, P.; Meng, L.; Du, Z.Y.; Miles, E.A.; Lie, O.; et al. Different intakes of n-3 fatty acids among pregnant women in 3 regions of China with contrasting dietary patterns are reflected in maternal but not in umbilical erythrocyte phosphatidylcholine fatty acid composition. Nutr. Res. 2013, 33, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Lands, B.; Lamoreaux, E. Using 3–6 differences in essential fatty acids rather than 3/6 ratios gives useful food balance scores. Nutr. Metab. (Lond.) 2012, 9, 46. [Google Scholar] [CrossRef] [PubMed]
- Al, M.D.; van Houwelingen, A.C.; Kester, A.D.; Hasaart, T.H.; de Jong, A.E.; Hornstra, G. Maternal essential fatty acid patterns during normal pregnancy and their relationship to the neonatal essential fatty acid status. Br. J. Nutr. 1995, 74, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.J.; Houwelingen, A.C.; Antal, M.; Manninen, A.; Godfrey, K.; Lopez-Jaramillo, P.; Hornstra, G. Maternal and neonatal essential fatty acid status in phospholipids: An international comparative study. Eur. J. Clin. Nutr. 1997, 51, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Meher, A.; Randhir, K.; Mehendale, S.; Wagh, G.; Joshi, S. Maternal Fatty Acids and Their Association with Birth Outcome: A Prospective Study. PLoS ONE 2016, 11, e0147359. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, C.; Speake, B.K.; Cameron, A.; Sattar, N.; Weaver, L.T. Maternal docosahexaenoic acid supplementation and fetal accretion. Br. J. Nutr. 2003, 90, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Vlaardingerbroek, H.; Hornstra, G. Essential fatty acids in erythrocyte phospholipids during pregnancy and at delivery in mothers and their neonates: Comparison with plasma phospholipids. Prostaglandins Leukot Essent. Fat. Acids 2004, 71, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, J.A.; Mori, T.A.; Barden, A.; Beilin, L.J.; Holt, P.G.; Calder, P.C.; Taylor, A.L.; Prescott, S.L. Effects of n-3 polyunsaturated fatty acid supplementation in pregnancy on maternal and fetal erythrocyte fatty acid composition. Eur. J. Clin. Nutr. 2004, 58, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Dwarkanath, P.; Muthayya, S.; Thomas, T.; Vaz, M.; Parikh, P.; Mehra, R.; Kurpad, A.V. Polyunsaturated fatty acid consumption and concentration among South Indian women during pregnancy. Asia Pac. J. Clin. Nutr. 2009, 18, 389–394. [Google Scholar] [PubMed]
- Much, D.; Brunner, S.; Vollhardt, C.; Schmid, D.; Sedlmeier, E.M.; Bruderl, M.; Heimberg, E.; Bartke, N.; Boehm, G.; Bader, B.L.; et al. Effect of dietary intervention to reduce the n-6/n-3 fatty acid ratio on maternal and fetal fatty acid profile and its relation to offspring growth and body composition at 1 year of age. Eur. J. Clin. Nutr. 2013, 67, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Stewart, F.; Rodie, V.A.; Ramsay, J.E.; Greer, I.A.; Freeman, D.J.; Meyer, B.J. Longitudinal assessment of erythrocyte fatty acid composition throughout pregnancy and post partum. Lipids 2007, 42, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Stark, K.D.; Beblo, S.; Murthy, M.; Buda-Abela, M.; Janisse, J.; Rockett, H.; Whitty, J.E.; Martier, S.S.; Sokol, R.J.; Hannigan, J.H.; et al. Comparison of bloodstream fatty acid composition from African-American women at gestation, delivery, and postpartum. J. Lipid Res. 2005, 46, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.J.; van Houwelingen, A.C.; Badart-Smook, A.; Hornstra, G. Comparison of the peripartum and postpartum phospholipid polyunsaturated fatty acid profiles of lactating and nonlactating women. Am. J. Clin. Nutr. 2001, 73, 1074–1079. [Google Scholar] [PubMed]
- Markhus, M.W.; Rasinger, J.D.; Malde, M.K.; Froyland, L.; Skotheim, S.; Braarud, H.C.; Stormark, K.M.; Graff, I.E. Docosahexaenoic Acid Status in Pregnancy Determines the Maternal Docosahexaenoic Acid Status 3-, 6- and 12 Months Postpartum. Results from a Longitudinal Observational Study. PLoS ONE 2015, 10, e0136409. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, T.; Nitta, H.; Murata, K.; Toda, E.; Tsukamoto, N.; Hasegawa, M.; Yamagata, Z.; Kayama, F.; Kishi, R.; Ohya, Y.; et al. Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health 2014, 14, 25. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Kawabata, T.; Tatsuta, N.; Kimura, F.; Miyazawa, T.; Mizuno, S.; Nishigori, H.; Arima, T.; Kagawa, Y.; Yoshimasu, K.; et al. Determinants of polyunsaturated fatty acid concentrations in erythrocytes of pregnant Japanese women from a birth cohort study: Study protocol and baseline findings of an adjunct study of the Japan environment & children’s study. Environ. Health Prev. Med. 2017, in press. [Google Scholar]
- Rose, H.G.; Oklander, M. Improved procedure for the extraction of lipids from human erythrocytes. J. Lipid Res. 1965, 6, 428–431. [Google Scholar] [PubMed]
- Hirota, S.; Adachi, N.; Gomyo, T.; Kawashima, H.; Kiso, Y.; Kawabata, T. Low-dose arachidonic acid intake increases erythrocytes and plasma arachidonic acid in young women. Prostaglandins Leukot Essent. Fat. Acids 2010, 83, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, H.T.; Trasande, L.; Ge, H.; Yu, L.X.; Xu, G.S.; Bai, M.X.; Liu, J.M. DHA in Pregnant and Lactating Women from Coastland, Lakeland, and Inland Areas of China: Results of a DHA Evaluation in Women (DEW) Study. Nutrients 2015, 7, 8723–8732. [Google Scholar] [CrossRef] [PubMed]
- Haggarty, P. Effect of placental function on fatty acid requirements during pregnancy. Eur. J. Clin. Nutr. 2004, 58, 1559–1570. [Google Scholar] [CrossRef] [PubMed]
- Pontes, P.V.; Torres, A.G.; Trugo, N.M.; Fonseca, V.M.; Sichieri, R. n-6 and n-3 Long-chain polyunsaturated fatty acids in the erythrocyte membrane of Brazilian preterm and term neonates and their mothers at delivery. Prostaglandins Leukot Essent. Fat. Acids 2006, 74, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, R.S.; Luxwolda, M.F.; Sango, W.S.; Kwesigabo, G.; Dijck-Brouwer, D.A.; Muskiet, F.A. Maternal DHA equilibrium during pregnancy and lactation is reached at an erythrocyte DHA content of 8 g/100 g fatty acids. J. Nutr. 2011, 141, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Makrides, M.; Gibson, R.A. Long-chain polyunsaturated fatty acid requirements during pregnancy and lactation. Am. J. Clin. Nutr. 2000, 71, 307S–311S. [Google Scholar] [PubMed]
- Bakewell, L.; Burdge, G.C.; Calder, P.C. Polyunsaturated fatty acid concentrations in young men and women consuming their habitual diets. Br. J. Nutr. 2006, 96, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Giltay, E.J.; Gooren, L.J.; Toorians, A.W.; Katan, M.B.; Zock, P.L. Docosahexaenoic acid concentrations are higher in women than in men because of estrogenic effects. Am. J. Clin. Nutr. 2004, 80, 1167–1174. [Google Scholar] [PubMed]
- Stark, K.D.; Holub, B.J. Differential eicosapentaenoic acid elevations and altered cardiovascular disease risk factor responses after supplementation with docosahexaenoic acid in postmenopausal women receiving and not receiving hormone replacement therapy. Am. J. Clin. Nutr. 2004, 79, 765–773. [Google Scholar] [PubMed]
- Agostoni, C.; Galli, C.; Riva, E.; Rise, P.; Colombo, C.; Giovannini, M.; Marangoni, F. Whole blood fatty acid composition at birth: From the maternal compartment to the infant. Clin. Nutr. 2011, 30, 503–505. [Google Scholar] [CrossRef] [PubMed]
- Courville, A.B.; Keplinger, M.R.; Judge, M.P.; Lammi-Keefe, C.J. Plasma or red blood cell phospholipids can be used to assess docosahexaenoic acid status in women during pregnancy. Nutr. Res. 2009, 29, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Schlormann, W.; Kramer, R.; Lochner, A.; Rohrer, C.; Schleussner, E.; Jahreis, G.; Kuhnt, K. Foetal cord blood contains higher portions of n-3 and n-6 long-chain PUFA but lower portions of trans C18:1 isomers than maternal blood. Food Nutr. Res. 2015, 59, 29348. [Google Scholar] [CrossRef] [PubMed]
- Kilari, A.S.; Mehendale, S.S.; Dangat, K.D.; Yadav, H.R.; Gupta, A.; Taralekar, V.S.; Joshi, S.R. Long chain polyunsaturated fatty acids in mothers of preterm babies. J. Perinat. Med. 2010, 38, 659–664. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n (%) | Median | (Inter-Quartile Range) | |
|---|---|---|---|
| Maternal age (years) | 29.6 | (25.9–33.9) | |
| Prepregnancy height (cm) | 158 | (152.8–162.1) | |
| Prepregnancy weight (kg) | 53.1 | (48.5–60.7) | |
| Prepregnancy body mass index (kg/cm2) | 21.8 | (19.9–24.4) | |
| Body weight gain (kg) | 11.6 | (8.9–14.2) | |
| Gestational period (day) | 278 | (274–285) | |
| Birth height (cm) | 49.5 | (48–50.5) | |
| Birth weight (g) | 3170 | (3004–3494) | |
| Head circumference (cm) | 34 | (33–35) | |
| Chest circumference (cm) | 32 | (31–33) | |
| Sex, female | 42 (56.8) | ||
| male | 32 (43.2) | ||
| Nursing, breast-feeding | 13 (17.6) | ||
| bottle-feeding | 4 (5.4) | ||
| mixed-feeding | 57 (77.0) |
| Umbilical Cord Erythrocytes (n = 74) | Maternal Erythrocytes | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 27 Weeks of Gestation (n = 74) | 30 Weeks of Gestation (n = 74) | 36 Weeks of Gestation (n = 74) | 2 Days after Delivery (n = 74) | 1 Month after Delivery (n = 74) | p 2 | ||||||||||||
| Median (Inter, Quartile Range) | Correlation Umbilical Cord vs. Maternal | Median (Inter, Quartile Range) | Correlation Umbilical Cord vs. Maternal | Median (Inter, Quartile Range) | Correlation Umbilical Cord vs. Maternal | Median (Inter, Quartile Range) | Correlation Umbilical Cord vs. Maternal | Median (Inter, Quartile Range) | Correlation Umbilical Cord vs. Maternal | ||||||||
| r | p 1 | r | p 1 | r | p 1 | r | p 1 | r | p 1 | ||||||||
| SFA | 51.5 (50.3–52.6) | 46.7 (46.2–47.6) | 0.070 | 0.553 | 46.5 (45.7–47.5) | 0.071 | 0.548 | 46.9 (46.2–47.6) | 0.183 | 0.118 | 47.1 (46.1–47.9) | 0.277 | 0.017 | 47.0 (46.1–47.9) | -0.004 | 0.971 | 0..091 |
| 16:0 | 26.9 (26.3–27.6) | 24.6 a (24.2–25.2) | -0.128 | 0.279 | 24.9 ab (24.3–25.6) | 0.107 | 0.365 | 25.0 b (24.4–25.6) | 0.202 | 0.085 | 25.4 c (24.7–26.0) | 0.152 | 0.196 | 24.5 a (24.1–25.1) | -0.076 | 0.520 | <0.001 |
| 18:0 | 17.9 (17.5–19.4) | 16.0 ac (15.4–16.8) | 0.085 | 0.473 | 15.6 ab (15.1–16.5) | -0.109 | 0.355 | 15.7 b (15.0–16.3) | -0.082 | 0.490 | 15.5 b (14.9–16.2) | 0.186 | 0.112 | 16.4 c (15.9–17.3) | -0.027 | 0.818 | <0.001 |
| 22:0 | 1.05 (0.99–1.17) | 1.21 a (1.10–1.32) | 0.127 | 0.281 | 1.21 a (1.10–1.33) | -0.038 | 0.746 | 1.29 b (1.16–1.41) | 0.215 | 0.066 | 1.17 a (1.10–1.32) | 0.304 | 0.009 | 1.20 a (1.12–1.30) | 0.089 | 0.450 | <0.001 |
| 24:0 | 3.73 (3.43–4.08) | 3.37 a (3.20–3.65) | 0.096 | 0.417 | 3.44 a (3.25–3.66) | 0.028 | 0.814 | 3.56 b (3.31–3.80) | 0.102 | 0.388 | 3.44 a (3.21–3.59) | 0.250 | 0.032 | 3.31 a (3.13–3.53) | 0.092 | 0.438 | <0.001 |
| MUFA | 15.1 (14.5–15.9) | 18.4 a (17.7–19.1) | 0.037 | 0.756 | 18.9 bc (18.0–19.6) | 0.043 | 0.719 | 19.0 c (18.5–19.6) | -0.027 | 0.820 | 19.0 bc (18.3–19.6) | 0.068 | 0.568 | 18.6 ab (17.9–19.1) | 0.010 | 0.930 | <0.001 |
| 18:1n-9 | 9.90 (9.40–10.4) | 12.6 a (12.0–13.1) | 0.168 | 0.153 | 13.0 b (12.3–13.5) | 0.170 | 0.149 | 13.1 b (12.5–13.6) | 0.052 | 0.661 | 13.1 b (12.5–13.6) | 0.112 | 0.343 | 12.8 b (12.4–13.5) | 0.065 | 0.583 | <0.001 |
| 18:1n-7 | 1.59 (1.44–1.72) | 1.08 ab (1.02–1.15) | 0.241 | 0.039 | 1.10 a (1.04–1.18) | 0.337 | 0.003 | 1.07 b (1.00–1.15) | 0.294 | 0.011 | 1.04 b (0.99–1.12) | 0.331 | 0.004 | 1.11 a (1.03–1.17) | 0.119 | 0.311 | <0.001 |
| 24:1n-9 | 2.99 (2.74–3.34) | 4.10 ac (3.82–4.36) | 0.067 | 0.570 | 4.18 ab (3.76–4.50) | 0.101 | 0.390 | 4.25 b (4.04–4.49) | 0.089 | 0.450 | 4.13 ab (3.90–4.40) | 0.155 | 0.187 | 3.97 c (3.68–4.20) | 0.066 | 0.577 | <0.001 |
| PUFA | 33.3 (32.5–34.4) | 34.7 a (34.0–35.4) | 0.146 | 0.216 | 34.6 ab (33.4–35.6) | 0.304 | 0.009 | 34.1 b (33.4–35.0) | 0.314 | 0.006 | 33.8 b (33.1–35.1) | 0.217 | 0.064 | 34.3 ab (33.7–35.3) | 0.202 | 0.085 | <0.001 |
| n-3 PUFA | 7.85 (6.92–8.87) | 9.98 a (8.84–11.2) | 0.573 | <0.001 | 9.54 ab (8.38–10.7) | 0.463 | <0.001 | 9.37 bc (8.67–10.6) | 0.550 | <0.001 | 9.46 bc (8.83–10.6) | 0.543 | <0.001 | 9.44 c (8.35–10.6) | 0.639 | <0.001 | <0.001 |
| 20:5n-3 | 0.25 (0.18–0.33) | 0.65 a (0.47–0.89) | 0.819 | <0.001 | 0.64 a (0.45–0.89) | 0.791 | <0.001 | 0.55 b (0.46–0.80) | 0.811 | <0.001 | 0.61 ab (0.50–0.81) | 0.858 | <0.001 | 0.87 c (0.62–1.17) | 0.630 | <0.001 | <0.001 |
| 22:5n-3 | 0.65 (0.54–0.85) | 1.85 a (1.66–2.05) | 0.544 | <0.001 | 1.74 ab (1.63–1.95) | 0.441 | <0.001 | 1.76 ab (1.62–1.94) | 0.529 | <0.001 | 1.78 b (1.62–1.92) | 0.520 | <0.001 | 1.79 ab (1.63–2.06) | 0.564 | <0.001 | <0.001 |
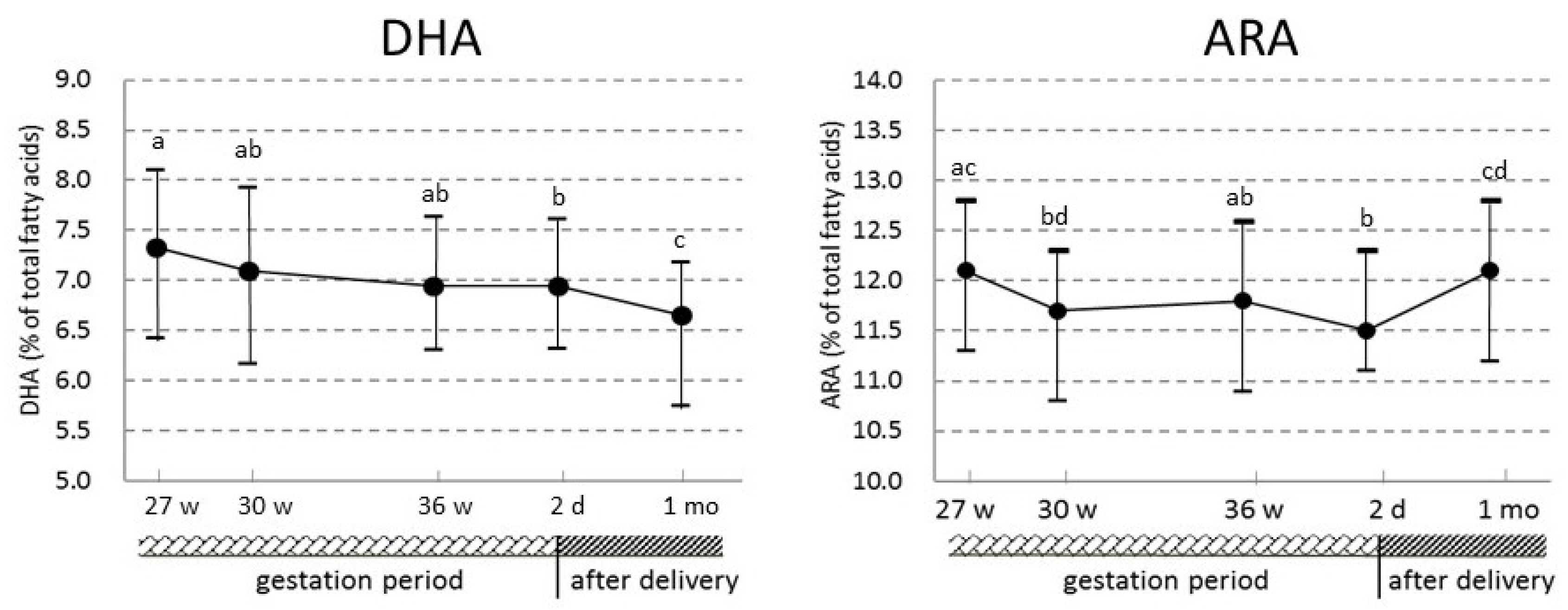
| 22:6n-3 | 6.92 (6.14–7.45) | 7.33 a (6.43–8.11) | 0.440 | <0.001 | 7.10 ab (6.17–7.93) | 0.370 | <0.001 | 6.95 ab (6.31–7.64) | 0.410 | <0.001 | 6.95 b (6.32–7.62) | 0.432 | <0.001 | 6.66 c (5.75–7.19) | 0.539 | <0.001 | <0.001 |
| n-6 PUFA | 25.2 (24.2–26.3) | 24.6 ab (23.5–25.8) | 0.362 | 0.002 | 24.6 ab (23.3–25.7) | 0.443 | <0.001 | 24.5 ab (23.4–25.3) | 0.485 | <0.001 | 24.4 a (23.2–25.3) | 0.516 | <0.001 | 24.6 b (23.2–25.6) | 0.380 | 0.001 | 0.002 |
| 18:2n-6 | 4.03 (3.56–4.34) | 8.88 a (8.39–9.41) | 0.444 | <0.001 | 9.08 bc (8.64–9.90) | 0.440 | <0.001 | 8.95 ab (8.39–9.52) | 0.478 | <0.001 | 9.08 b (8.51–9.73) | 0.615 | <0.001 | 9.25 c (8.58–9.96) | 0.420 | <0.001 | <0.001 |
| 20:3n-6 | 2.38 (2.05–2.69) | 1.36 ac (1.22–1.50) | 0.392 | 0.001 | 1.38 ab (1.23–1.53) | 0.437 | <0.001 | 1.34 c (1.19–1.52) | 0.509 | <0.001 | 1.35 c (1.19–1.49) | 0.456 | <0.001 | 1.17 d (1.02–1.36) | 0.404 | <0.001 | <0.001 |
| 20:4n-6 | 15.4 (14.7–16.4) | 12.1 ac (11.3–12.8) | 0.349 | 0.002 | 11.7 bd (10.8–12.3) | 0.414 | <0.001 | 11.8 ab (10.9–12.6) | 0.361 | 0.002 | 11.5 b (11.1–12.3) | 0.379 | 0.001 | 12.1 cd (11.2–12.8) | 0.247 | 0.034 | <0.001 |
| 22:4n-6 | 2.93 (2.61–3.30) | 2.06 a (1.77–2.33) | 0.471 | <0.001 | 1.99 ab (1.71–2.25) | 0.561 | <0.001 | 1.98 ab (1.67–2.30) | 0.539 | <0.001 | 1.94 b (1.65–2.26) | 0.588 | <0.001 | 1.83 c (1.60–2.09) | 0.566 | <0.001 | <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawabata, T.; Kagawa, Y.; Kimura, F.; Miyazawa, T.; Saito, S.; Arima, T.; Nakai, K.; Yaegashi, N. Polyunsaturated Fatty Acid Levels in Maternal Erythrocytes of Japanese Women during Pregnancy and after Childbirth. Nutrients 2017, 9, 245. https://doi.org/10.3390/nu9030245
Kawabata T, Kagawa Y, Kimura F, Miyazawa T, Saito S, Arima T, Nakai K, Yaegashi N. Polyunsaturated Fatty Acid Levels in Maternal Erythrocytes of Japanese Women during Pregnancy and after Childbirth. Nutrients. 2017; 9(3):245. https://doi.org/10.3390/nu9030245
Chicago/Turabian StyleKawabata, Terue, Yasuo Kagawa, Fumiko Kimura, Teruo Miyazawa, Shoji Saito, Takahiro Arima, Kunihiko Nakai, and Nobuo Yaegashi. 2017. "Polyunsaturated Fatty Acid Levels in Maternal Erythrocytes of Japanese Women during Pregnancy and after Childbirth" Nutrients 9, no. 3: 245. https://doi.org/10.3390/nu9030245