Cereal Consumption among Subjects with Celiac Disease: A Snapshot for Nutritional Considerations

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Berti, I.; Gerarduzzi, T.; Not, T.; Colletti, R.B.; Drago, S.; Elitsur, Y.; Green, P.H.; Guandalini, S.; Hill, I.D.; et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: A large multicenter study. Arch. Intern. Med. 2003, 163, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Hoffenberg, E.J.; MacKenzie, T.; Barriga, K.J.; Eisenbarth, G.S.; Bao, F.; Haas, J.E.; Erlich, H.; Bugawan, Tl.; Sokol, R.J.; Taki, I.; et al. A prospective study of the incidence of childhood celiac disease. J. Pediatr. 2003, 143, 308–314. [Google Scholar] [CrossRef]
- Lohi, S.; Mustalahti, K.; Kaukinen, K.; Laurila, K.; Collin, P.; Rissanen, H.; Lohi, O.; Bravi, E.; Gasparin, M.; Reunanen, A.; et al. Increasing prevalence of coeliac disease over time. Aliment. Pharmacol. Ther. 2007, 26, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Kyle, R.A.; Kaplan, E.L.; Johnson, D.R.; Page, W.; Erdtmann, F.; Brantner, T.L.; Kim, W.R.; Phelps, T.K.; Lahr, B.D.; et al. Increased prevalence and mortality in undiagnosed celiac disease. Gastroenterology 2009, 137, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Steele, R. Diagnosis and management of coeliac disease in children. Postgrad. Med. J. 2011, 87, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Lionetti, E. Case finding for celiac disease is okay, but is it enough? J. Pediatr. Gastroenterol. Nutr. 2013, 57, 415–417. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, V.; Kurppa, K.; Huhtala, H.; Collin, P.; Mäki, M.; Kaukinen, K. Factors associated with long diagnostic delay in celiac disease. Scand. J. Gastroenterol. 2014, 49, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Ukkola, A.; Mäki, M.; Kurppa, K.; Collin, P.; Huhtala, H.; Kekkonen, L.; Kaukinen, K. Patients’ experiences and perceptions of living with coeliac disease—Implications for optimizing care. J. Gastrointestin Liver Dis. 2012, 21, 17–22. [Google Scholar] [PubMed]
- Hall, N.J.; Rubin, G.; Charnock, A. Systematic review: Adherence to a gluten-free diet in adult patients with coeliac disease. Aliment. Pharmacol. Ther. 2009, 30, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.R.; Ng, D.L.; Zivin, J.; Green, P.H. Economic burden of a gluten-free diet. J. Hum. Nutr. Diet. 2007, 20, 423–430. [Google Scholar] [CrossRef] [PubMed]
- See, J.A.; Kaukinen, K.; Makharia, G.K.; Gibson, P.R.; Murray, J.A. Practical insights into gluten-free diets. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Fabiani, E.; Iacono, G.; D’Agate, C.; Francavilla, R.; Biagi, F.; Volta, U.; Accomando, S.; Picarelli, A.; De Vitis, I.; et al. A prospective, double-blind, placebo-controlled trial to establish a safe gluten threshold for patients with celiac disease. Am. J. Clin. Nutr. 2007, 85, 160–166. [Google Scholar] [PubMed]
- Niewinski, M.M. Advances in celiac disease and gluten-free diet. J. Am. Diet. Assoc. 2008, 108, 661–672. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Geisel, T.; Maresch, C.; Krieger, K.; Stein, J. Inadequate nutrient intake in patients with celiac disease: Results from a German dietary survey. Digestion 2013, 87, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, S.J.; Gibson, P.R. Nutritional inadequacies of the gluten-free diet in both recently-diagnosed and long-term patients with coeliac disease. J. Hum. Nutr. Diet. 2013, 26, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Mariani, P.; Viti, M.G.; Montuori, M.; La Vecchia, A.; Cipolletta, E.; Calvani, L.; Bosnamico, M. The gluten-free diet: A nutritional risk factor for adolescents with celiac disease? J. Pediatr. Gastroenterol. Nutr. 1998, 27, 519–523. [Google Scholar] [CrossRef] [PubMed]
- De Giorgio, R.; Volta, U.; Gibson, P.R. Sensitivity to wheat, gluten and FODMAPs in IBS: Facts or fiction? Gut 2016, 65, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Babio, N.; Alcázar, M.; Castillejo, G.; Recasens, M.; Martínez-Cerezo, F.; Gutiérrez-Pensado, V.; Masip, G.; Vaqué, C.; Vila-Martí, A.; Torres-Moreno, M.; et al. Patients With Celiac Disease Reported Higher Consumption of Added Sugar and Total Fat Than Healthy Individuals. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, H.M.; Gibson, P.R. How healthy is a gluten-free diet? Br. J. Nutr. 2015, 114, 1539–1541. [Google Scholar] [CrossRef] [PubMed]
- Van de Kamer, J.H.; Weijers, H.A.; Dicke, W.K. Coeliac disease. IV. An investigation into the injurious constituents of wheat in connection with their action on patients with coeliac disease. Acta Paediatr. 1953, 42, 223–231. [Google Scholar] [PubMed]
- Singh, J.; Whelan, K. Limited availability and higher cost of gluten-free foods. J. Hum. Nutr. Diet. 2011, 24, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Gluten-Free Products Market by type, Sales Channel and Geography: Global Trends and Forecasts to 2018. Available online: http://www.marketsandmarkets.com/Market-Reports/gluten-free-products-market-738.html (accessed on 14 February 2016).
- Butterworth, J.R.; Banfield, L.M.; Iqbal, T.H.; Cooper, B.T. Factors relating to compliance with a gluten-free diet in patients with coeliac disease: Comparison of white Caucasian and South Asian patients. Clin. Nutr. 2004, 23, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Scazzina, F.; Dall’Asta, M.; Pellegrini, N.; Brighenti, F. Glycaemic index of some commercial gluten-free foods. Eur. J. Nutr. 2015, 54, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Valletta, E.; Fornaro, M.; Cipolli, M.; Conte, S.; Bissolo, F.; Danchielli, C. Celiac disease and obesity: Need for nutritional follow-up after diagnosis. Eur. J. Clin. Nutr. 2010, 64, 1371–1372. [Google Scholar] [CrossRef] [PubMed]
- Miele, L.; Valenza, V.; La Torre, G.; Montalto, M.; Cammarota, G.; Ricci, R.; Mascianà, R.; Forgione, A.; Gabrieli, M.L.; Perotti, G.; et al. Increased intestinal permeability and tight junction alterations in nonalcoholic fatty liver disease. Hepatology 2009, 49, 1877–1887. [Google Scholar] [CrossRef] [PubMed]
- Flores-Silva, P.C.; Rodriguez-Ambriz, S.L.; Bello-Pérez, L.A. Gluten-free snacks using plantain-chickpea and maize blend: Chemical composition, starch digestibility, and predicted glycemic index. J. Food Sci. 2015, 80, C961–C966. [Google Scholar] [CrossRef] [PubMed]
- Ente Nazionale Risi. Indagine Integrata sul Consumo di Riso in Italia 2004. Available online: http://www.enterisi.it/upload/enterisi/bilanci/consumoriso2004p_15916_27.pdf (accessed on 18 March 2016).
- Engelhardt, K.; Ahn, B.C.; Cho, S.I.; Joung, H. Predictors of interest in nutrition topics and willingness to participate in local nutrition programmes. J. Public Health 2007, 29, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Miranda, J.; Lasa, A.; Bustamante, M.A.; Churruca, I.; Simon, E. Nutritional differences between a gluten-free diet and a diet containing equivalent products with gluten. Plant Foods Hum. Nutr. 2014, 69, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E.; Goldberg, G.R.; Jebb, S.A.; Livingstone, M.B.; Cole, T.J.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 2. Evaluating the results of published surveys. Eur. J. Clin. Nutr. 1991, 45, 583–599. [Google Scholar] [PubMed]
- Kretsch, M.J.; Fong, A.K.; Green, M.W. Behavioral and body size correlates of energy intake underreporting by obese and normal-weight women. J. Am. Diet. Assoc. 1999, 99, 300–306. [Google Scholar] [CrossRef]
- Larkin, F.A.; Metzner, H.L.; Guire, K.E. Comparison of three consecutive-day and three random-day records of dietary intake. J. Am. Diet. Assoc. 1991, 91, 1538–1542. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Celiac Subjects | Control Subjects |
|---|---|---|
| M/F ratio | 14/68 | 20/57 |
| Median age (range) | 37 years (18–67) | 37 years (18–68) |
| Median weight (range) | 64.2 kg (47.2–88.6) | 69.3 kg (52.8–90.1) |
| Median height (range) | 168.9 cm (148.3–189.5) | 166.1 cm (146.8–192.0) |
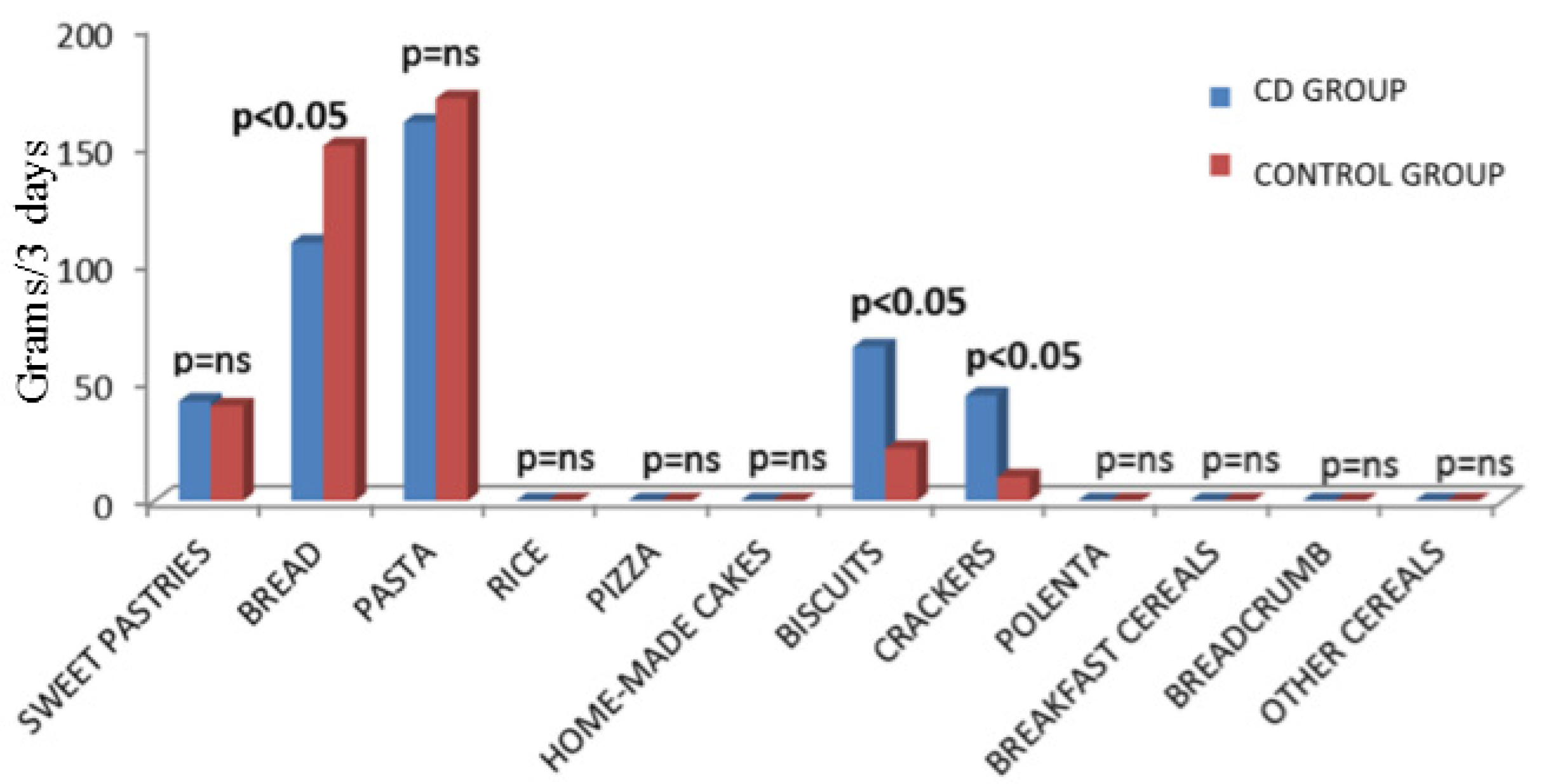
| Cereal-Based Products | Celiac Population | Control Population | Statistics |
|---|---|---|---|
| Sweet Pastries | 42.1 g (0–146) | 40.2 g (0–100) | p = ns |
| Bread | 109.5 g (50–226) | 150.7 g (80–234) | p < 0.05 |
| Pasta | 160.0 g (92–254) | 173.3 g (105–232) | p = ns |
| Rice | 0 g (0–99) | 0 g (0-60) | p = ns |
| Pizza | 0 g (0–200) | 0 g (0–248) | p = ns |
| Homemade Cakes | 0 g (0–0) | 0 g (0–0) | p = ns |
| Biscuits | 65.8 g (12–104) | 22.7 g (0–92) | p < 0.05 |
| Crackers | 44.7 g (0–85) | 10.6 g (0–65) | p < 0.05 |
| Polenta | 0 g (0–0) | 0 g (0–0) | p = ns |
| Breakfast Cereals | 0 g (0–57) | 0 g (0–50) | p = ns |
| Breadcrumb | 0 g (0–0) | 0 g (0–0) | p = ns |
| Other Cereals | 0 g (0–26) | 0 g (0–43) | p = ns |
| Cereal-Based Products | CD Subjects (Males) | Controls (Males) | Statistics |
|---|---|---|---|
| Sweet Pastries | 3.5 g (0–68.4) | 20.8 g (0–63) | p = ns |
| Bread | 69.1 g (47.2–125.6) | 67.6 g (34.2–118.9) | p = ns |
| Pasta | 58.4 g (48.2–150.9) | 108.3 g (90.1–156.9) | p = ns |
| Rice | 27.6 g (0–43.3) | 0 g (0–0) | p = ns |
| Pizza | 0 g (0–41.8) | 0 g (0–23.6) | p = ns |
| Homemade Cakes | 0 g (0–0) | 0 g (0–0) | p = ns |
| Biscuits | 41.2 g (18.7–65.1) | 0 g (0–27.1) | p ˂ 0.05 |
| Crackers | 13.8 g (0–29.2) | 0 g (0–0) | p ˂ 0.05 |
| Polenta | 0 g (0–0) | 0 g (0–0) | p = ns |
| Breakfast Cereals | 0 g (0–16.3) | 0 g (0–58.5) | p = ns |
| Breadcrumb | 0 g (0–0) | 0 g (0–0) | p = ns |
| Other Cereals | 0 g (0–0) | 0 g (0–11.3) | p = ns |
| Cereal-Based Products | CD Subjects (Females) | Controls (Females) | Statistics |
|---|---|---|---|
| Sweet Pastries | 16.6 g (0–44.7) | 13.2 g (0–26.8) | p = ns |
| Bread | 33.2 g (14.3–68.6) | 50.6 g (27.2–80.4) | p ˂ 0.05 |
| Pasta | 53.3 g (31.0–84.6) | 51.6 g (33.1–71.9) | p = ns |
| Rice | 0 g (0–31.1) | 0 g (0–23.6) | p = ns |
| Pizza | 0 g (0–86.6) | 0 g (0–83.2) | p = ns |
| Homemade Cakes | 0 g (0–0) | 0 g (0–0) | p = ns |
| Biscuits | 19.6 g (0–33.0) | 6.9 g (0–32.1) | p = ns |
| Crackers | 14.8 g (0–29.6) | 6.6 g (0–22.1) | p = ns |
| Polenta | 0 g (0–0) | 0 g (0–0) | p = ns |
| Breakfast Cereals | 0 g (0–34.1) | 0 g (0–16.4) | p = ns |
| Breadcrumb | 0 g (0–2.5) | 0 g (0–0) | p = ns |
| Other Cereals | 0 g (0–21.4) | 0 g (0–34.6) | p = ns |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valitutti, F.; Iorfida, D.; Anania, C.; Trovato, C.M.; Montuori, M.; Cucchiara, S.; Catassi, C. Cereal Consumption among Subjects with Celiac Disease: A Snapshot for Nutritional Considerations. Nutrients 2017, 9, 396. https://doi.org/10.3390/nu9040396
Valitutti F, Iorfida D, Anania C, Trovato CM, Montuori M, Cucchiara S, Catassi C. Cereal Consumption among Subjects with Celiac Disease: A Snapshot for Nutritional Considerations. Nutrients. 2017; 9(4):396. https://doi.org/10.3390/nu9040396
Chicago/Turabian StyleValitutti, Francesco, Donatella Iorfida, Caterina Anania, Chiara Maria Trovato, Monica Montuori, Salvatore Cucchiara, and Carlo Catassi. 2017. "Cereal Consumption among Subjects with Celiac Disease: A Snapshot for Nutritional Considerations" Nutrients 9, no. 4: 396. https://doi.org/10.3390/nu9040396