Iodine Status and Iodised Salt Consumption in Portuguese School-Aged Children: The Iogeneration Study


 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
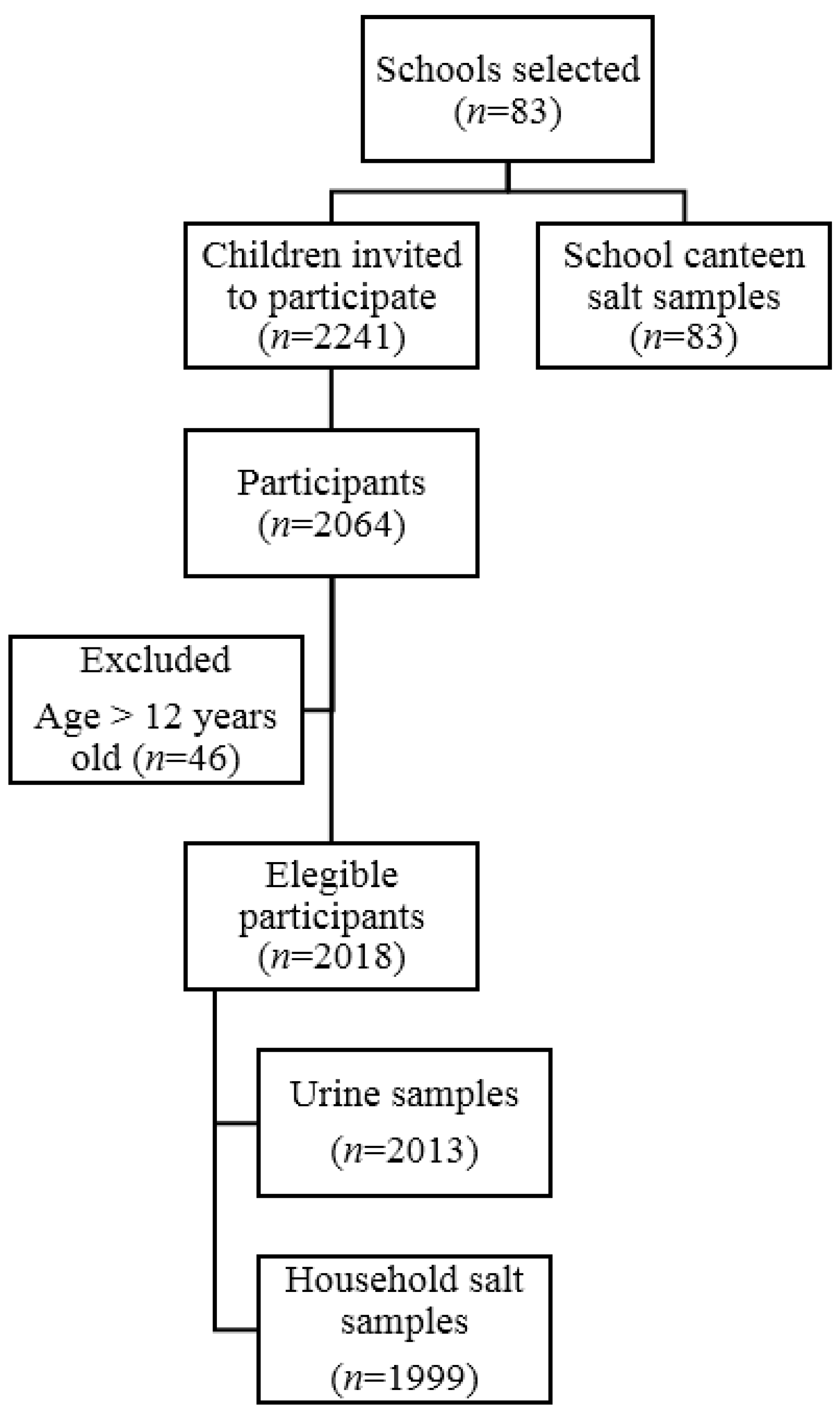
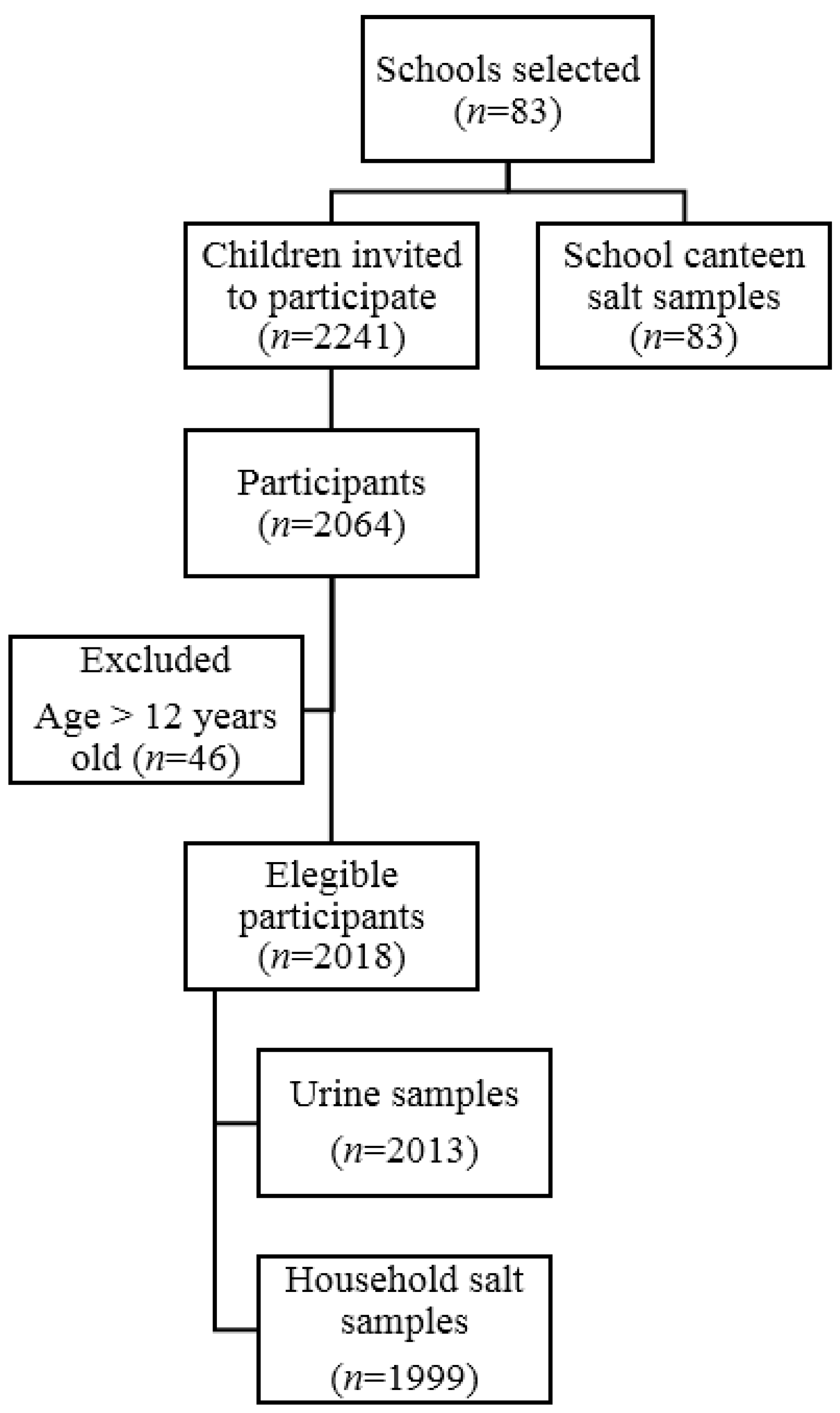
2.1. Participants and Study Design
2.2. Data Collection
2.3. Biochemical Analysis
2.3.1. Iodine Determination in Urine Samples
2.3.2. Creatinine, Sodium, and Potassium Determination
- (a)
- For men: predicted 24-h urinary sodium excretion (mg/day) = 23 × {25.46 + [0.46 × spot sodium (mmol/L)] − [2.75 × spot creatinine (mmol/L)] − [0.13 × spot potassium (mmol/L)] + [4.10 × BMI (kg/m2)] + [0.26 × age (y)]}
- (b)
- For women: predicted 24-h urinary sodium excretion (mg/day) = 23 × {5.07 + [0.34 × spot sodium (mmol/L)] − [2.16 × spot creatinine (mmol/L)] − [0.09 × spot potassium (mmol/L)] + [2.39 × BMI (kg/m2)] + [2.35 × age (y)] – [0.03 × age2 (y)]}
2.4. Iodine Determination in Salt Samples
2.5. Statistical Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Urinary Iodine Concentration
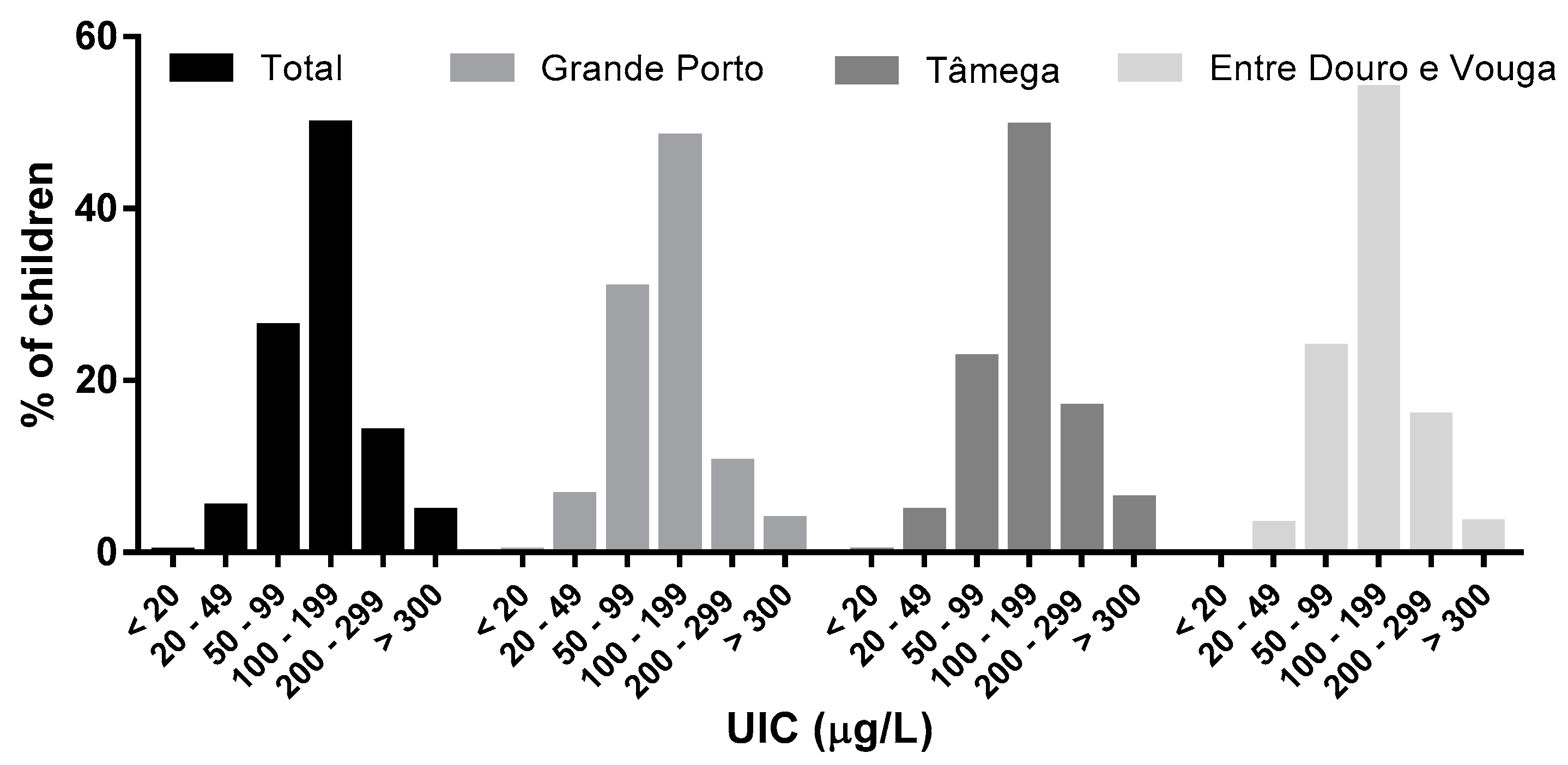
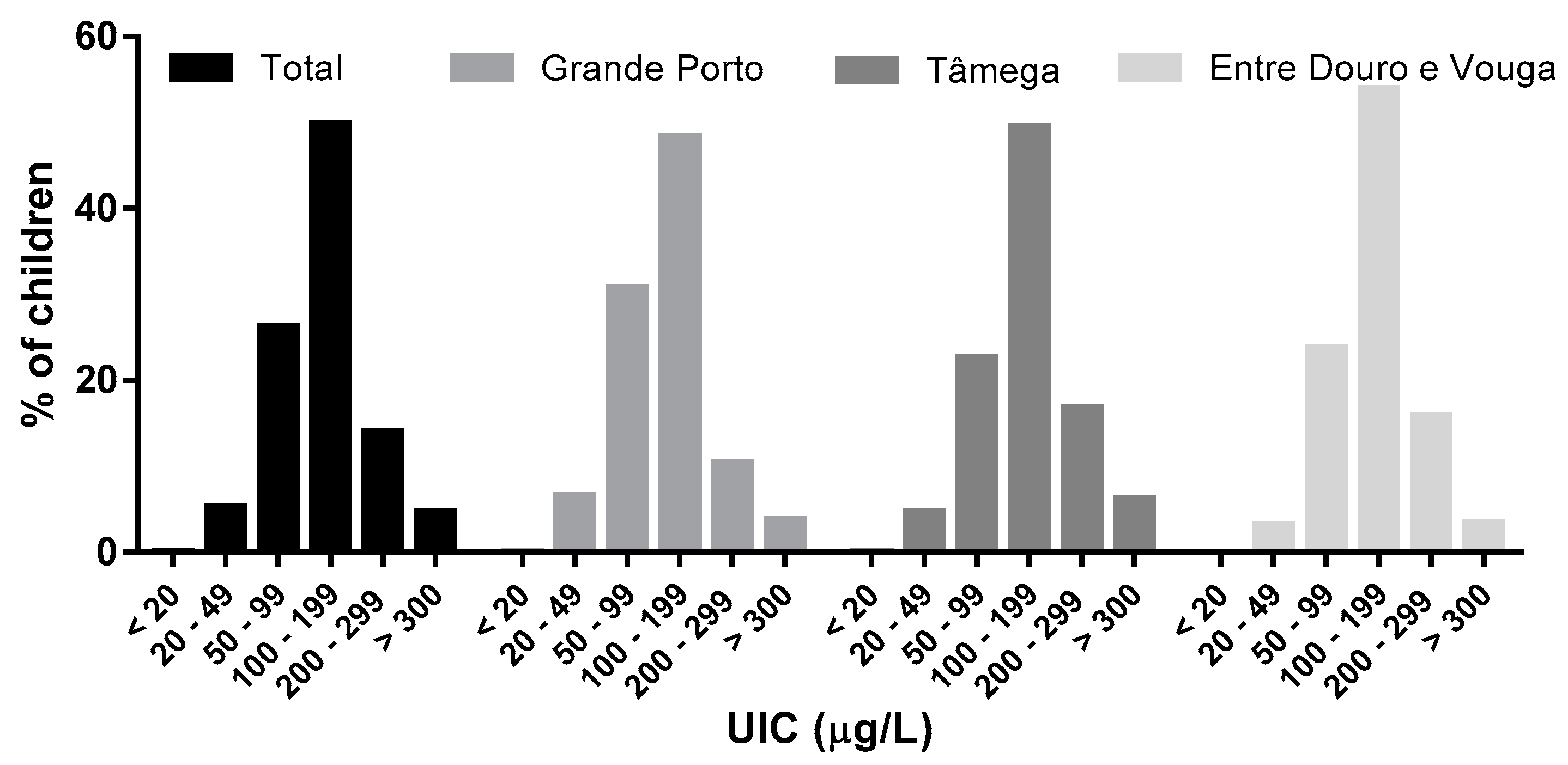
3.2.1. Iodine Status by Region
3.2.2. Iodine Status by Sex and Age Group
3.2.3. Iodine Status and Dietary Habits
4. Discussion
Acknowledgments
Author Contributions
Conflict of Interest
References
- Andersson, M.; Karumbunathan, V.; Zimmermann, M.B. Global iodine status in 2011 and trends over the past decade. J. Nutr. 2012, 142, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of inadequate iodine status in uk pregnant women on cognitive outcomes in their children: Results from the avon longitudinal study of parents and children (alspac). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Gordon, R.C.; Rose, M.C.; Skeaff, S.A.; Gray, A.R.; Morgan, K.M.; Ruffman, T. Iodine supplementation improves cognition in mildly iodine-deficient children. Am. J. Clin. Nutr. 2009, 90, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Connolly, K.; Bozo, M.; Bridson, J.; Rohner, F.; Grimci, L. Iodine supplementation improves cognition in iodine-deficient schoolchildren in Albania: A randomized, controlled, double-blind study. Am. J. Clin. Nutr. 2006, 83, 108–114. [Google Scholar] [PubMed]
- Zimmermann, M.B.; Jooste, P.L.; Pandav, C.S. Iodine-deficiency disorders. Lancet 2008, 372, 1251–1262. [Google Scholar] [CrossRef]
- Vanderpump, M.P.; Lazarus, J.H.; Smyth, P.P.; Laurberg, P.; Holder, R.L.; Boelaert, K.; Franklyn, J.A.; British Thyroid Association, U.K.I.S.G. Iodine status of uk schoolgirls: A cross-sectional survey. Lancet 2011, 377, 2007–2012. [Google Scholar] [CrossRef]
- Limbert, E.; Prazeres, S.; Sao Pedro, M.; Madureira, D.; Miranda, A.; Ribeiro, M.; Jacome de Castro, J.; Carrilho, F.; Oliveira, M.J.; Reguengo, H.; et al. Iodine intake in portuguese pregnant women: Results of a countrywide study. Eur. J. Endocrinol. 2010, 163, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Limbert, E.; Prazeres, S.; Sao Pedro, M.; Madureira, D.; Miranda, A.; Ribeiro, M.; Carrilho, F.; Jacome de Castro, J.; Lopes, M.S.; Cardoso, J.; et al. Iodine intake in portuguese school children. Acta Medica Port. 2012, 25, 29–36. [Google Scholar]
- DGE. Orientações Sobre Ementas e Refeitórios Escolares–2013/2014. Available online: http://www.dge.mec.pt/refeitorios-escolares (accessed on 6 December 2016).
- Rito, A.; Breda, J.; Carmo, I. Guia de Avaliação Do Estado Nutricional Infantil e Juvenil; Instituto Nacional de Saúde Doutor Ricardo Jorge: Direção Geral de Saúde, Portugal, 2010. [Google Scholar]
- CDC. Iodine and Mercury in Urine: Nhanes 2011-2012: Method 3002.1. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_11_12/uiouhg_g_met_iodine_mercury.pdf (accessed on 6 December 2016).
- Cogswell, M.E.; Wang, C.Y.; Chen, T.C.; Pfeiffer, C.M.; Elliott, P.; Gillespie, C.D.; Carriquiry, A.L.; Sempos, C.T.; Liu, K.; Perrine, C.G. Validity of predictive equations for 24-h urinary sodium excretion in adults aged 18–39 y. Am. J. Clin. Nutr. 2013, 98, 1502–1513. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.R.; Dary, O.; Cappuccio, F.P.; Neufeld, L.M.; Harding, K.B.; Zimmermann, M.B. Need for coordinated programs to improve global health by optimizing salt and iodine intake. Rev. Panam. Salud Publica 2012, 32, 281–286. [Google Scholar] [CrossRef]
- Correia-Costa, L.; Cosme, D.; Nogueira-Silva, L.; Morato, M.; Sousa, T.; Moura, C.; Mota, C.; Guerra, A.; Albino-Teixeira, A.; Areias, J.C.; et al. Gender and obesity modify the impact of salt intake on blood pressure in children. Pediatr. Nephrol. 2016, 31, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Ibm Spss Statistics for Windows, version 23.0; IBM Corporation: Armonk, NY, USA, 2014.
- Mendes, H.; Zagalo-Cardoso, J.A. Estudo epidemiológico de prevalência do bócio endémico em oleiros. Acta Medica Port. 2002, 15, 101–111. [Google Scholar]
- Johner, S.A.; Thamm, M.; Nothlings, U.; Remer, T. Iodine status in preschool children and evaluation of major dietary iodine sources: A german experience. Eur. J. Nutr. 2013, 52, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Benoist, B.; Darnton-Hill, I.; Delange, F. Iodine Deficiency in Europe: A Continuing Public Health Problem; WHO/UNICEF: Geneva, Switzerland, 2007. [Google Scholar]
- Kusic, Z.; Jukic, T.; Rogan, S.A.; Juresa, V.; Dabelic, N.; Stanicic, J.; Boric, M.; Lukinac, L.; Mihaljevic, I.; Punda, A.; et al. Current status of iodine intake in Croatia--the results of 2009 survey. Coll. Antropol. 2012, 36, 123–128. [Google Scholar] [PubMed]
- Laurberg, P.; Jorgensen, T.; Perrild, H.; Ovesen, L.; Knudsen, N.; Pedersen, I.B.; Rasmussen, L.B.; Carle, A.; Vejbjerg, P. The danish investigation on iodine intake and thyroid disease, danthyr: Status and perspectives. Eur. J. Endocrinol. 2006, 155, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.L.; Meirelles, C.J.; Oliveira, L.A.; Costa, T.M.; Navarro, A.M. Excessive iodine intake in schoolchildren. Eur. J. Nutr. 2012, 51, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.M.; Braverman, L.E. Consequences of excess iodine. Nat. Rev. Endocrinol. 2014, 10, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Emder, P.J.; Jack, M.M. Iodine-induced neonatal hypothyroidism secondary to maternal seaweed consumption: A common practice in some asian cultures to promote breast milk supply. J. Paediatr. Child Health 2011, 47, 750–752. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guideline: Fortification of Food-Grade Salt With Iodine for the Prevention and Control of Iodine Deficiency Disorders. Geneva. Available online: http://www.who.int/nutrition/publications/guidelines/ fortification_foodgrade_saltwithiodine/en/ (accessed on 6 December 2016).
- Salt Reduction and Iodine Fortification Strategies in Public Health: REPORT of a Joint Technical Meeting. Available online: http://apps.who.int/iris/handle/10665/101509 (accessed on 6 December 2016).
- McLean, R.M. Measuring population sodium intake: A review of methods. Nutrients 2014, 6, 4651–4662. [Google Scholar] [CrossRef] [PubMed]
- Peter, F.; Podoba, J.; Muzsnai, A. Iodine status of schoolchildren in hungary: Improvement a decade on. Eur. Thyroid. J. 2015, 4, 71–72. [Google Scholar] [CrossRef] [PubMed]
- Kassim, I.A.; Moloney, G.; Busili, A.; Nur, A.Y.; Paron, P.; Jooste, P.; Gadain, H.; Seal, A.J. Iodine intake in somalia is excessive and associated with the source of household drinking water. J. Nutr. 2014, 144, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Combet, E.; Scully, P.; Zimmermann, M.B.; Hampshire-Jones, K.H.; Rayman, M.P. A multi-centre pilot study of iodine status in uk schoolchildren, aged 8–10 years. Eur. J. Nutr. 2015, 55, 2001–2009. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.; Lu, T.; Dary, O.; Legetic, B.; Campbell, N.R.; Cappuccio, F.P. Systematic review of studies evaluating urinary iodine concentration as a predictor of 24-hour urinary iodine excretion for estimating population iodine intake. Rev. Panam. Salud Publica 2015, 38, 73–81. [Google Scholar] [PubMed]
- Vila, L.; Donnay, S.; Arena, J.; Arrizabalaga, J.J.; Pineda, J.; Garcia-Fuentes, E.; Garcia-Rey, C.; Marin, J.L.; Serra-Prat, M.; Velasco, I.; et al. Iodine status and thyroid function among spanish schoolchildren aged 6–7 years: The tirokid study. Br. J. Nutr. 2016, 115, 1623–1631. [Google Scholar] [CrossRef] [PubMed]
- Watutantrige Fernando, S.; Barollo, S.; Nacamulli, D.; Pozza, D.; Giachetti, M.; Frigato, F.; Redaelli, M.; Zagotto, G.; Girelli, M.E.; Mantero, F.; et al. Iodine status in schoolchildren living in northeast italy: The importance of iodized-salt use and milk consumption. Eur. J. Clin. Nutr. 2013, 67, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Opsahl, J.A.; Meltzer, H.M.; Julshamn, K. Iodine concentration in norwegian milk and dairy products. Br. J. Nutr. 2003, 90, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Reaching Optimal Iodine Nutrition in Pregnant and Lactating Women and Young Children: A Joint Statement by WHO and UNICEF. Geneva, World Health Organization. 2007. Available online: http://www.who.int/nutrition/publications/micronutrients/WHOStatement__IDD_pregnancy.pdf (accessed on 6 December 2016).

{kind=link}
{kind=link}
| Variables | Total | Grande Porto | Tâmega | Entre Douro e Vouga | p Value |
|---|---|---|---|---|---|
| Whole (n) | 2018 | 837 | 831 | 350 | |
| Gender | 0.153 a | ||||
| Boys (n; %) | 1050; 52 | 450; 54% | 411; 49% | 189; 54% | |
| Girls (n; %) | 968; 48 | 387; 46% | 420; 51% | 161; 46% | |
| Age group (n; %) | 0.160 a | ||||
| 5–6 years old | 162; 8 | 72; 9% | 65; 8% | 25; 7% | |
| 7–8 years old | 713; 35 | 284; 34% | 286; 34% | 143; 41% | |
| 9–10 years old | 655; 32 | 275; 33% | 286; 34% | 94; 27% | |
| 11–12 years old | 488; 24 | 206; 25% | 194; 23% | 88; 25% | |
| Age (year; mean ± sd) | 8.9 ± 1.8 | 8.9 ± 1.8 | 8.9 ± 1.7 | 8.9 ± 1.9 | 0.839 b |
| Weight (kg; mean ± sd) | 35.8 ± 11.1 | 36.4 ± 11.9 | 35.6 ± 10.4 | 35.1 ± 10.7 | 0.123 b |
| Height (cm; mean ± sd) | 137.0 ± 11.7 | 136.8 ±12.0 | 136.6 ± 11.3 | 136.4 ± 12.0 | 0.900 b |
| BMI (kg/m2; mean ± sd) | 18.8 ± 3.4 | 19.0 ± 3.6 | 18.7 ± 3.3 | 18.5 ± 3.0 | 0.021 b |
| Urinary iodine (µg/L; median (P25; P75)) | 129 (88; 181) | 116 (79; 164) | 137 (99; 194) | 138 (96; 189) | 0.000 c |
| Urinary iodine/creatinine (µg/g; median (P25; P75)) | 126 (83; 183) | 114 (78; 165) | 132 (87; 192) | 142 (93; 205) | 0.000 c |
| Urinary sodium, est. (mg/day; mean ± sd) | 2576 ± 782 | 2587 ± 790 | 2558 ± 778 | 2593 ± 770 | 0.684 b |
| Salt intake, est. (g/day; mean ± sd) [12] | 6.4 ± 2.0 | 6.5 ± 2.0 | 6.4 ± 1.9 | 6.5 ± 1.9 | 0.684 b |
| Variables | UIC (µg/L) | p Value | UIC < 100 µg/L | UIC > 300 µg/L (%) | p Value | Iodine-to-Creatinine Ratio (µg/g) | p Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | P25 | Median | P75 | n | % | n | % | P25 | Median | P75 | ||||
| Boys | 1050 | 84 | 134 | 177 | 0.002 b | 303 | 29 | 63 | 6 | 0.005 c | 89 | 131 | 185 | 0.002 b |
| Girls | 968 | 91 | 123 | 188 | 331 | 34 | 32 | 3 | 79 | 117 | 182 | |||
| 5–6 years old | 161 | 110 | 157 | 208 | <0.001 a | 32 | 20 | 16 | 10 | <0.001 c | 128 | 189 | 262 | <0.001 a |
| 7–8 years old | 711 | 94 | 138 | 192 | 194 | 27 | 42 | 6 | 104 | 149 | 218 | |||
| 9–10 years old | 654 | 84 | 125 | 174 | 220 | 34 | 26 | 4 | 81 | 121 | 169 | |||
| 11-12 years old | 487 | 7 | 115 | 160 | 188 | 39 | 11 | 2 | 66 | 89 | 133 | |||
| Food Consumption | UIC (µg/L) | UIC < 100 µg/L | UIC > 300 µg/L | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | P25 | Median | P75 | p Value | n | % | n | % | p Value | |
| Ilk *,# | ||||||||||
| <1 glass/day | 142 (23) | 68 | 96 | 151 | <0.001 a | 72 | 50 | 0 | 0 | <0.001 c |
| 1 glass/day | 242 (39) | 83 | 120 | 173 | 86 | 36 | 8 | 3 | ||
| ≥2 glasses/day | 231 (38) | 107 | 149 | 207 | 47 | 20 | 19 | 8 | ||
| Yogurt # | ||||||||||
| <1 yogurt/day | 294 (48) | 79 | 117 | 171 | 0.010 a | 112 | 38 | 10 | 3 | 0.018 c |
| 1 yogurt/day | 221 (36) | 91 | 129 | 186 | 70 | 32 | 11 | 5 | ||
| ≥2 yogurts/day | 100 (16) | 102 | 147 | 192 | 8 | 8 | 6 | 6 | ||
| Eggs # | ||||||||||
| <1 egg/week | 181 (29) | 88 | 131 | 184 | 0.326 b | 53 | 29 | 5 | 3 | 0.138 c |
| ≥1 egg/week | 434 (71) | 82 | 124 | 181 | 152 | 35 | 22 | 5 | ||
| Fish | ||||||||||
| ≤1 times/week | 413 (21) | 88 | 128 | 190 | 0.569 b | 118 | 29 | 26 | 6 | 0.284 c |
| >1 times/week | 1533 (79) | 87 | 129 | 180 | 493 | 32 | 69 | 5 | ||
| Premade baby cereal | ||||||||||
| ≤1 times/week | 1708 (89) | 87 | 124 | 180 | 0.002 b | 551 | 32 | 69 | 4 | <0.001 c |
| >1 times/week | 215 (11) | 101 | 140 | 201 | 51 | 24 | 23 | 11 | ||
| Household iodised salt | ||||||||||
| Self-reported | ||||||||||
| No | 1085 (56) | 87 | 129 | 180 | 0.646 a | 344 | 32 | 48 | 4 | 0.921 c |
| Yes | 162 (8) | 80 | 129 | 184 | 52 | 32 | 10 | 6 | ||
| Unknown | 677 (35) | 92 | 130 | 182 | ||||||
| Measured ** | ||||||||||
| No | 130 (83) | 74 | 120 | 181 | 0.001 b | 46 | 35 | 7 | 5 | 0.118 c |
| Yes | 26 (17) | 137 | 173 | 255 | 3 | 12 | 3 | 12 | ||
| Variables | Crude a OR b (95% CI) | p Value | Adjusted a OR b (95% CI) | p Value | |
|---|---|---|---|---|---|
| Milk (n = 615) | ≥2 glasses/day | 1.0 | <0.001 | 1.0 | <0.001 |
| 1 glass/day | 2.16 (1.43–3.27) | 2.20 (1.45–3.34) | |||
| <1 glass/day | 4.03 (2.54–6.37) | 3.85 (2.42–6.13) | |||
| Yogurt (n = 615) | ≥2 yogurts/day | 1.0 | 0.019 | ||
| 1 yogurt/day | 1.55 (0.90–2.68) | ||||
| <1 yogurt/day | 2.06 (1.22–3.47) | ||||
| Fish (n = 1946) | >1 times/week | 1.0 | 0.164 | ||
| ≤1 times/week | 0.84 (0.67–1.07) | ||||
| Eggs (n = 615) | ≥1 egg/week | 1.0 | 0.169 | ||
| <1 egg/week | 0.77 (0.53–1.12) | ||||
| Premade baby cereal (n = 1923) | ≥1 times/month | 1.0 | 0.001 | ||
| <1 times/month | 1.54 (1.20–1.99) | ||||
| Age | <1 Glass/Day | 1 Glass/Day | ≥2 Glasses/Day | Total | p Value | |||
|---|---|---|---|---|---|---|---|---|
| n | % per Age Group | n | % per Age Group | n | % per Age Group | |||
| 5–6 years old | 4 | 10% | 19 | 45% | 19 | 45% | 42 | 0.045 a |
| 7–8 years old | 54 | 21% | 109 | 42% | 98 | 38% | 261 | |
| 9–10 years old | 57 | 31% | 60 | 32% | 68 | 37% | 185 | |
| 11–12 years old | 28 | 22% | 54 | 42% | 46 | 36% | 128 | |
| Total | 143 | 242 | 231 | 616 | ||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa Leite, J.; Keating, E.; Pestana, D.; Cruz Fernandes, V.; Maia, M.L.; Norberto, S.; Pinto, E.; Moreira-Rosário, A.; Sintra, D.; Moreira, B.; et al. Iodine Status and Iodised Salt Consumption in Portuguese School-Aged Children: The Iogeneration Study. Nutrients 2017, 9, 458. https://doi.org/10.3390/nu9050458
Costa Leite J, Keating E, Pestana D, Cruz Fernandes V, Maia ML, Norberto S, Pinto E, Moreira-Rosário A, Sintra D, Moreira B, et al. Iodine Status and Iodised Salt Consumption in Portuguese School-Aged Children: The Iogeneration Study. Nutrients. 2017; 9(5):458. https://doi.org/10.3390/nu9050458
Chicago/Turabian StyleCosta Leite, João, Elisa Keating, Diogo Pestana, Virgínia Cruz Fernandes, Maria Luz Maia, Sónia Norberto, Edgar Pinto, André Moreira-Rosário, Diana Sintra, Bárbara Moreira, and et al. 2017. "Iodine Status and Iodised Salt Consumption in Portuguese School-Aged Children: The Iogeneration Study" Nutrients 9, no. 5: 458. https://doi.org/10.3390/nu9050458