Reduced Mortality in Maintenance Haemodialysis Patients on High versus Low Dialysate Magnesium: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Conduct
2.3. Inclusion and Exclusion Criteria
2.4. Treatment Groups
2.5. Endpoint Analysis
2.6. Matching
2.7. Statistical Analysis
3. Results
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Predictor | Unit | Hazard Ratio (95% CI) | p-Value |
|---|---|---|---|
| Age * | 1 year | 1.06 (1.02, 1.10) | 0.002 |
| Gender | Male | 1.92 (0.76, 4.88) | 0.17 |
| CCI * | 1 | 2.75 (1.80, 4.20) | <0.001 |
| Smoking status | Smoker | 0.04 (0.00, 3.94) | 0.17 |
| BMI | 1 kg/m2 | 1.04 (0.98, 1.11) | 0.24 |
| Kt/V | 1 | 0.34 (0.12, 0.99) | 0.047 |
| Total cholesterol | 1 mg/dL | 0.99 (0.98, 1.00) | 0.14 |
| LDL cholesterol | 1 mg/dL | 0.99 (0.98, 1.01) | 0.25 |
| Predictor | Unit | Regression Coefficient | Hazard Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Dialysate group | High dialysate magnesium | −1.06 | 0.35 (0.13, 0.97) | 0.044 |
| Age | 1 year | 0.04 | 1.04 (1.00, 1.09) | 0.08 |
| CCI * | 1 | 0.96 | 2.60 (1.58, 4.28) | <0.001 |
References
- Goodman, W.G.; Goldin, J.; Kuizon, B.D.; Yoon, C.; Gales, B.; Sider, D.; Wang, Y.; Chung, J.; Emerick, A.; Greaser, L.; et al. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N. Engl. J. Med. 2000, 342, 1478–1483. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Epidemiology of cardiovascular disease in chronic renal disease. J. Am. Soc. Nephrol. 1998, 9, S16–S23. [Google Scholar] [CrossRef] [PubMed]
- Reffelmann, T.; Ittermann, T.; Dorr, M.; Volzke, H.; Reinthaler, M.; Petersmann, A.; Felix, S.B. Low serum magnesium concentrations predict cardiovascular and all-cause mortality. Atherosclerosis 2011, 219, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Isaka, Y. Hypomagnesemia is a significant predictor of cardiovascular and non-cardiovascular mortality in patients undergoing hemodialysis. Kidney Int. 2014, 85, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Joao Matias, P.; Azevedo, A.; Laranjinha, I.; Navarro, D.; Mendes, M.; Ferreira, C.; Amaral, T.; Jorge, C.; Aires, I.; Gil, C.; et al. Lower serum magnesium is associated with cardiovascular risk factors and mortality in haemodialysis patients. Blood Purif. 2014, 38, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Ishimura, E.; Okuno, S.; Yamakawa, T.; Inaba, M.; Nishizawa, Y. Serum magnesium concentration is a significant predictor of mortality in maintenance hemodialysis patients. Magnes. Res. 2007, 20, 237–244. [Google Scholar] [PubMed]
- De Roij van Zuijdewijn, C.L.; Grooteman, M.P.; Bots, M.L.; Blankestijn, P.J.; Steppan, S.; Buchel, J.; Groenwold, R.H.; Brandenburg, V.; van den Dorpel, M.A.; Ter Wee, P.M.; et al. Serum magnesium and sudden death in european hemodialysis patients. PLoS ONE 2015, 10, e0143104. [Google Scholar]
- Lacson, E., Jr.; Wang, W.; Ma, L.; Passlick-Deetjen, J. Serum magnesium and mortality in hemodialysis patients in the united states: A cohort study. Am. J. Kidney Dis. 2015, 66, 1056–1066. [Google Scholar] [CrossRef] [PubMed]
- Kanbay, M.; Yilmaz, M.I.; Apetrii, M.; Saglam, M.; Yaman, H.; Unal, H.U.; Gok, M.; Caglar, K.; Oguz, Y.; Yenicesu, M.; et al. Relationship between serum magnesium levels and cardiovascular events in chronic kidney disease patients. Am. J. Nephrol. 2012, 36, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Cai, K.; Luo, Q.; Dai, Z.; Zhu, B.; Fei, J.; Xue, C.; Wu, D. Hypomagnesemia is associated with increased mortality among peritoneal dialysis patients. PLoS ONE 2016, 11, e0152488. [Google Scholar] [CrossRef] [PubMed]
- Markell, M.S.; Altura, B.T.; Sarn, Y.; Delano, B.G.; Ifudu, O.; Friedman, E.A.; Altura, B.M. Deficiency of serum ionized magnesium in patients receiving hemodialysis or peritoneal dialysis. ASAIO J. 1993, 39, M801–M804. [Google Scholar] [PubMed]
- Wyskida, K.; Witkowicz, J.; Chudek, J.; Wiecek, A. Daily magnesium intake and hypermagnesemia in hemodialysis patients with chronic kidney disease. J. Ren. Nutr. 2012, 22, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Luis, D.; Zlatkis, K.; Comenge, B.; Garcia, Z.; Navarro, J.F.; Lorenzo, V.; Carrero, J.J. Dietary quality and adherence to dietary recommendations in patients undergoing hemodialysis. J. Ren. Nutr. 2016, 26, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, Y.; Hamano, T.; Isaka, Y. Effects of magnesium on the phosphate toxicity in chronic kidney disease: Time for intervention studies. Nutrients 2017, 9, 112. [Google Scholar] [CrossRef] [PubMed]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the united states: Are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Küchle, C.; Suttmann, Y.; Reichelt, A.L.; Apfelböck, J.; Zoller, V.; Heemann, U. Correcting low magnesia levels in hemodialysis by higher dialysate magnesium. Cogent Med. 2017, 4. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Iseki, K.; Tsubakihara, Y.; Isaka, Y. Magnesium modifies the cardiovascular mortality risk associated with hyperphosphatemia in patients undergoing hemodialysis: A cohort study. PLoS ONE 2014, 9, e116273. [Google Scholar] [CrossRef] [PubMed]
- Altura, B.T.; Shirey, T.L.; Young, C.C.; Dell’Orfano, K.; Hiti, J.; Welsh, R.; Yeh, Q.; Barbour, R.L.; Altura, B.M. Characterization of a new ion selective electrode for ionized magnesium in whole blood, plasma, serum, and aqueous samples. Scand. J. Clin. Lab. Invest. 1994, 217, 21–36. [Google Scholar] [CrossRef]
- Huijgen, H.J.; Sanders, R.; van Olden, R.W.; Klous, M.G.; Gaffar, F.R.; Sanders, G.T. Intracellular and extracellular blood magnesium fractions in hemodialysis patients; is the ionized fraction a measure of magnesium excess? Clin. Chem. 1998, 44, 639–648. [Google Scholar] [PubMed]
- Liu, J.; Huang, Z.; Gilbertson, D.T.; Foley, R.N.; Collins, A.J. An improved comorbidity index for outcome analyses among dialysis patients. Kidney Int. 2010, 77, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Matching. BMJ 1994, 309, 1128. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials. 1996, 17, 343–346. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: http://www.R-project.org/ (accessed on 17 July 2017).
- Pasch, A.; Farese, S.; Gräber, S.; Wald, J.; Richtering, W.; Floege, J.; Jahnen-Dechent, W. Nanoparticle-based test measures overall propensity for calcification in serum. JASN 2012, 23, 1744–1752. [Google Scholar] [CrossRef] [PubMed]
- Pippias, M.; Stel, V.S.; Abad Diez, J.M.; Afentakis, N.; Herrero-Calvo, J.A.; Arias, M.; Tomilina, N.; Bouzas Caamano, E.; Buturovic-Ponikvar, J.; Cala, S.; et al. Renal replacement therapy in europe: A summary of the 2012 era-edta registry annual report. Clin. Kidney J. 2015, 8, 248–261. [Google Scholar] [CrossRef] [PubMed]
| Dialysate Magnesium | |||
|---|---|---|---|
| High 0.75 mmol/L (n = 25) | Low 0.50 mmol/L (n = 50) | p-Value | |
| Age (years) | 66.3 (48.5–73.5) | 67.9 (49.2–73.9) | 0.86 |
| Gender (males) | 16 (64.0) | 32 (64.0) | 1.0 |
| BMI (kg/m2) | 28.1 (25.0–34.7) | 24.4 (22.2–29.2) | 0.034 |
| Follow-up (days) | 1121 (1047.5–1138.5) | 1200 (550.8–1200.0) | 0.06 |
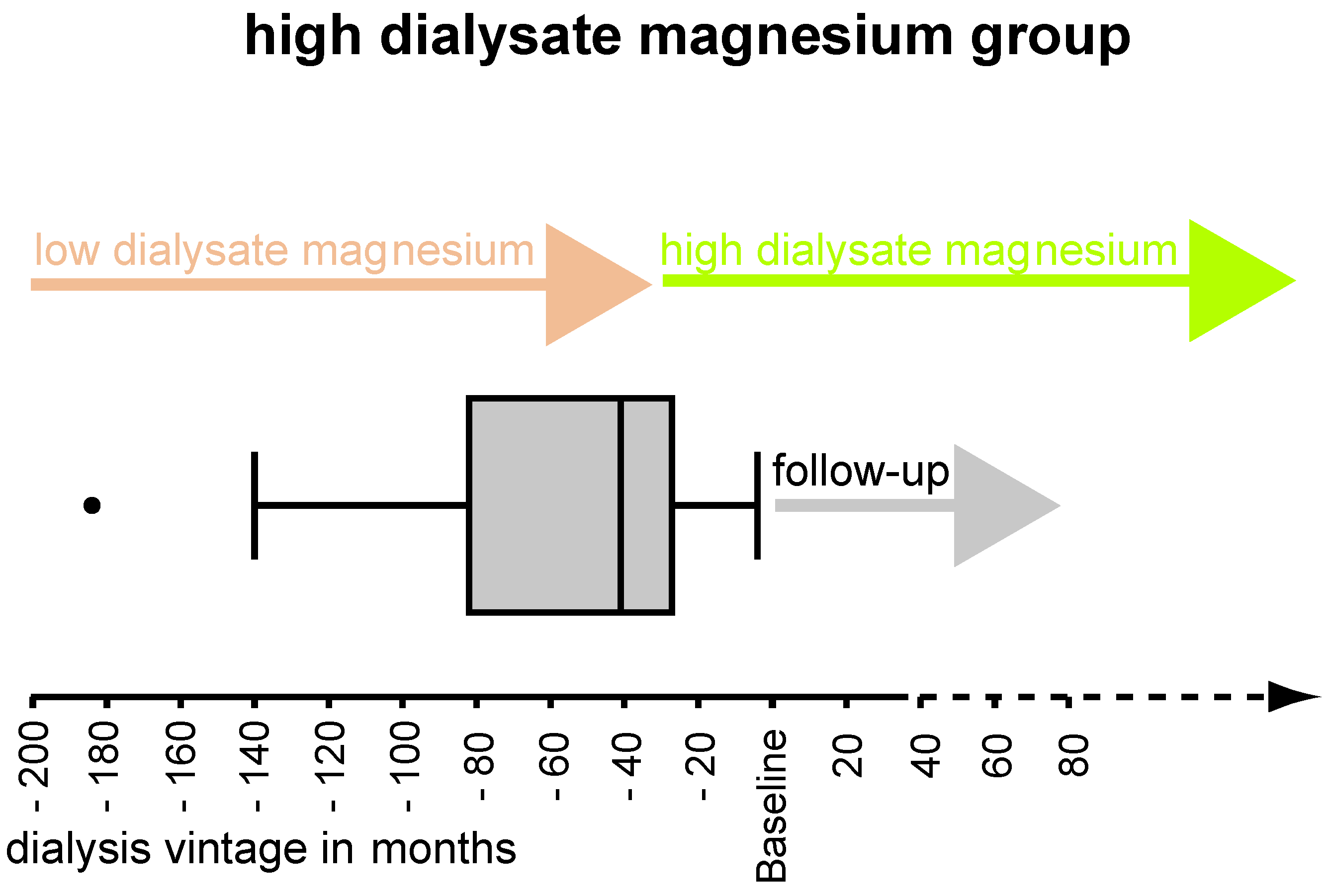
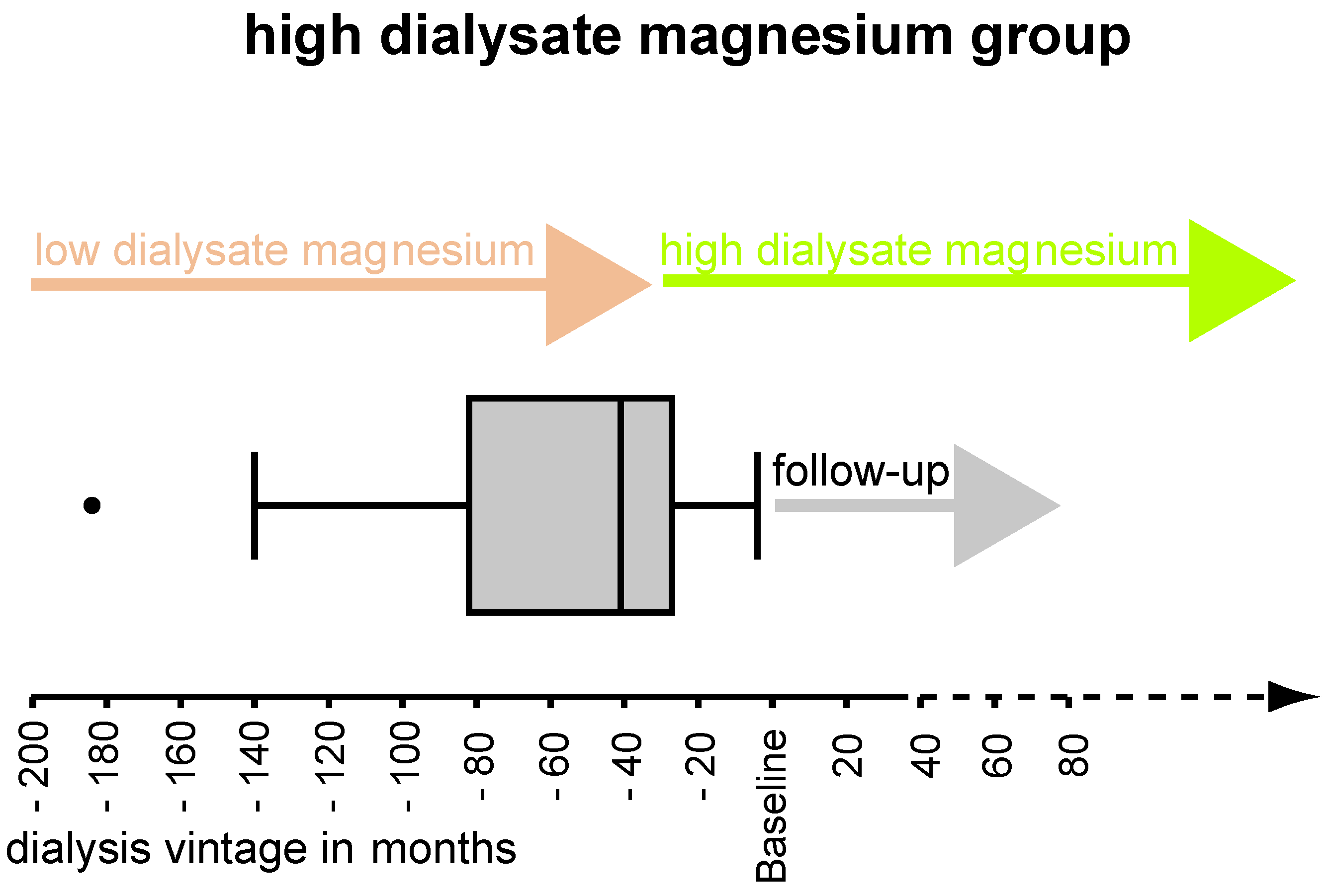
| Dialysis vintage (months) | 41.0 (30.0–96.5) | 47.0 (26.5–99.3) | 0.86 |
| Ultrafiltration rate per hour | 563.6 ± 283.0 | 478.7 ± 263.5 | 0.37 |
| Volume reduction per session (L) | 1.9 ± 1.7 | 1.6 ± 1.2 | 0.37 |
| Kt/V | 1.53 ± 0.29 | 1.37 ± 0.43 | 0.07 |
| Dialysis duration per session (h) | 4.5 (4.0–4.5) | 4.2 (4.0–4.5) | 0.88 |
| Systolic arterial pressure (mmHg) | 137.7 ± 18.1 | 129.9 ± 27.0 | 0.20 |
| Diastolic arterial pressure (mmHg) | 66.7 ± 17.1 | 68.5 ± 13.3 | 0.63 |
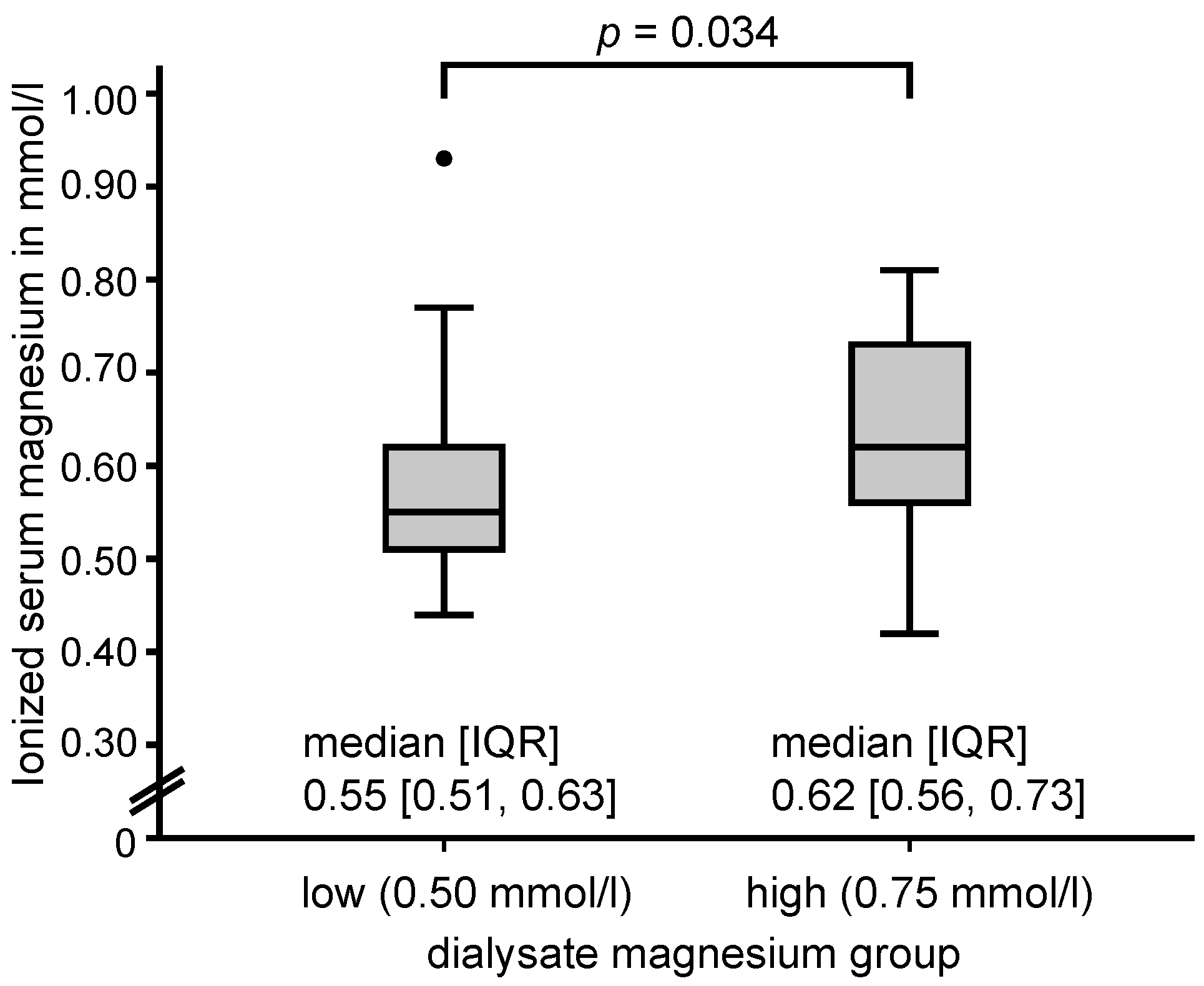
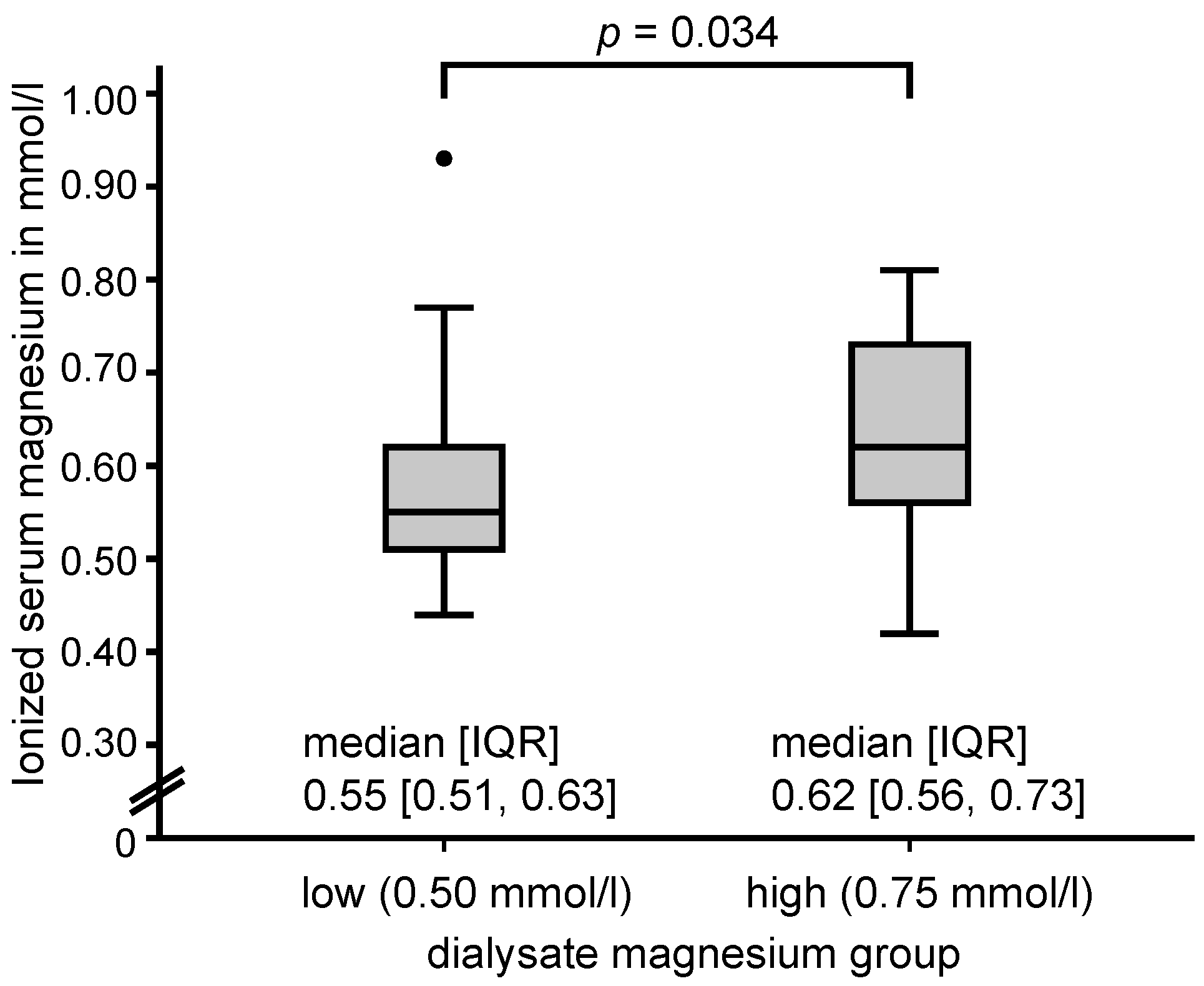
| Ionized magnesium in serum (mmol/L) | 0.64 ± 0.12 | 0.57 ± 0.10 | 0.034 |
| Phosphate (mmol/L) | 1.53 (1.37–1.94) | 1.75 (1.40–2.11) | 0.16 |
| Total calcium in serum (mmol/L) | 2.28 ± 0.24 | 2.27 ± 0.20 | 0.89 |
| Ionized calcium in serum (mmol/L) | 1.22 ± 0.18 | 1.21 ± 0.13 | 0.86 |
| Calcium x phosphate (mmol2/L2) | 3.78 (2.87–4.51) | 3.90 (3.14–4.74) | 0.23 |
| Alkaline phosphatase (U/L) | 74 (56–90) | 88 (66–113) | 0.10 |
| Intact parathyroid hormone (pg/mL) | 152.48 (51.00–189.50) | 191.10 (86.55–361.00) | 0.11 |
| High resolution CRP (mg/L) | 0.68 (0.16–1.28) | 0.55 (0.16–1.37) | 0.94 |
| Albumin (g/dL) | 3.94 (3.78–4.33) | 3.96 (3.70–4.10) | 0.24 |
| Blood urea nitrogen (mg/dL) | 59.48 ± 16.61 | 63.23 ± 17.37 | 0.70 |
| Hematocrit (%) | 35.74 ± 4.29 | 34.69 ± 4.79 | 0.34 |
| Haemoglobin (g/dL) | 11.72 ± 1.35 | 11.61 ± 1.45 | 0.74 |
| Total cholesterol (mg/dL) | 167.0 ± 48.2 | 190.0 ± 48.5 | 0.08 |
| HDL cholesterol (mg/dL) | 41.0 (37.8–55.8) | 45.0 (37.8–55.8) | 0.21 |
| LDL cholesterol (mg/dL) | 91.1 ± 39.4 | 117.8 ± 36.6 | 0.012 |
| Charlson Comorbidity Index (1–4) | 1.0 (0–1.5) | 1.0 (0–1.0) | 0.27 |
| Diabetes mellitus | 16 (64.0) | 24 (48.0) | 0.23 |
| History of myocardial infarction | 7 (28.0) | 12 (24.0) | 0.78 |
| Peripheral artery disease | 9 (36.0) | 14 (28.0) | 0.60 |
| Smoking (ever) | 4 (16.0) | 8 (16.0) | 1.0 |
| Predictor | Unadjusted | Adjusted * | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
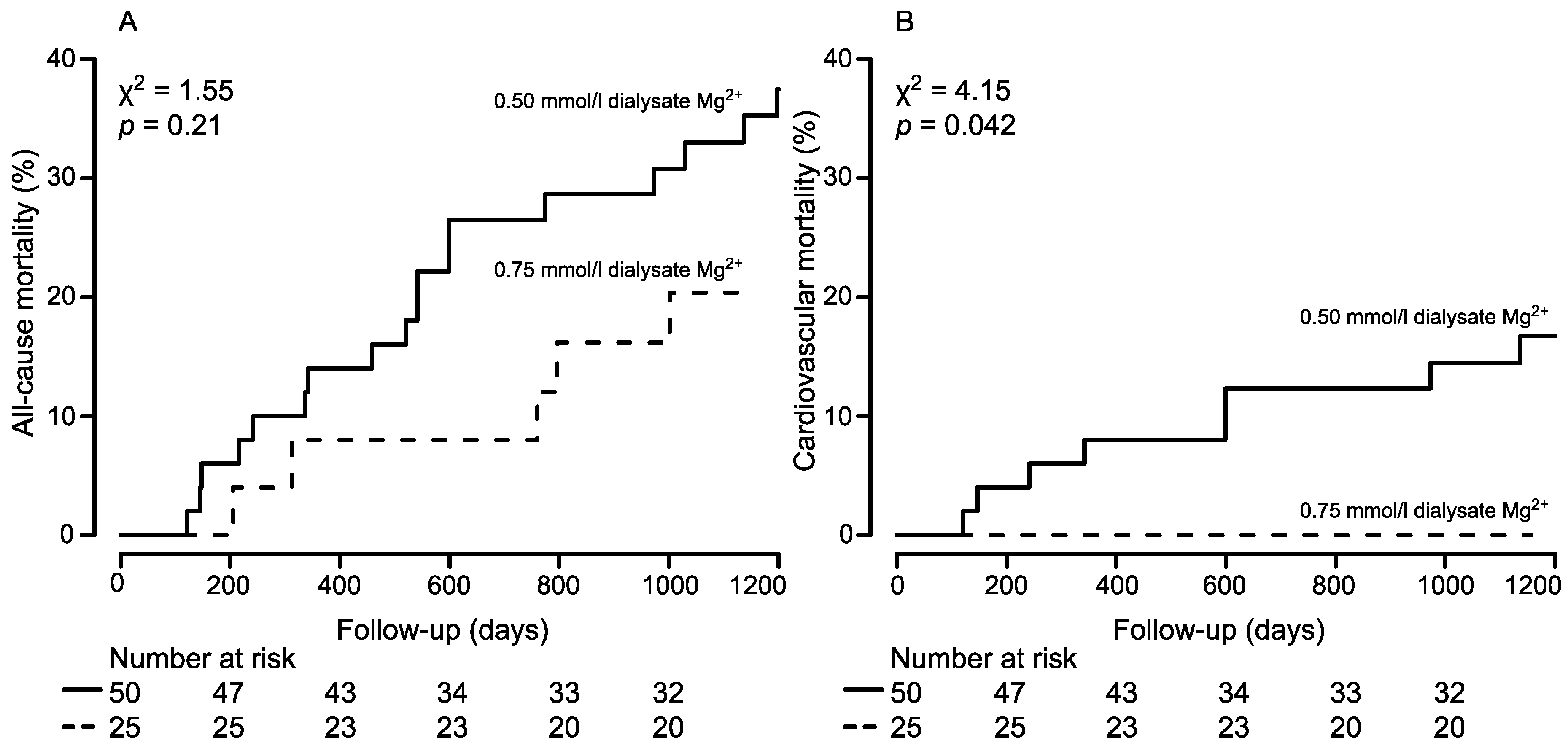
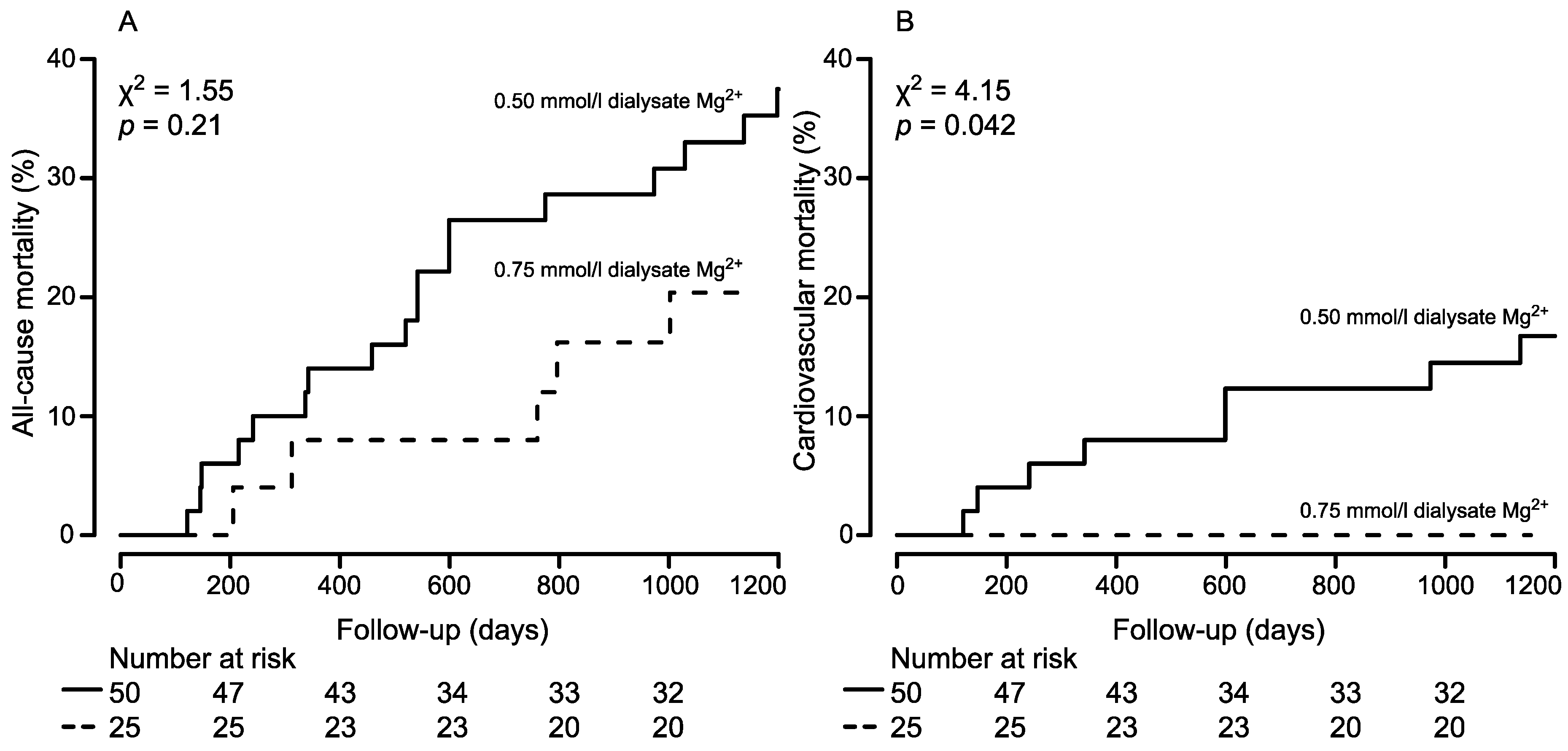
| High dialysate magnesium | 0.54 (0.20, 1.46) | 0.24 | 0.35 (0.13, 0.97) | 0.044 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmaderer, C.; Braunisch, M.C.; Suttmann, Y.; Lorenz, G.; Pham, D.; Haller, B.; Angermann, S.; Matschkal, J.; Renders, L.; Baumann, M.; et al. Reduced Mortality in Maintenance Haemodialysis Patients on High versus Low Dialysate Magnesium: A Pilot Study. Nutrients 2017, 9, 926. https://doi.org/10.3390/nu9090926
Schmaderer C, Braunisch MC, Suttmann Y, Lorenz G, Pham D, Haller B, Angermann S, Matschkal J, Renders L, Baumann M, et al. Reduced Mortality in Maintenance Haemodialysis Patients on High versus Low Dialysate Magnesium: A Pilot Study. Nutrients. 2017; 9(9):926. https://doi.org/10.3390/nu9090926
Chicago/Turabian StyleSchmaderer, Christoph, Matthias C. Braunisch, Yana Suttmann, Georg Lorenz, Dang Pham, Bernhard Haller, Susanne Angermann, Julia Matschkal, Lutz Renders, Marcus Baumann, and et al. 2017. "Reduced Mortality in Maintenance Haemodialysis Patients on High versus Low Dialysate Magnesium: A Pilot Study" Nutrients 9, no. 9: 926. https://doi.org/10.3390/nu9090926