Botulinum Toxin A for Sialorrhoea Associated with Neurological Disorders: Evaluation of the Relationship between Effect of Treatment and the Number of Glands Treated


 ,
, 
Abstract
:1. Introduction
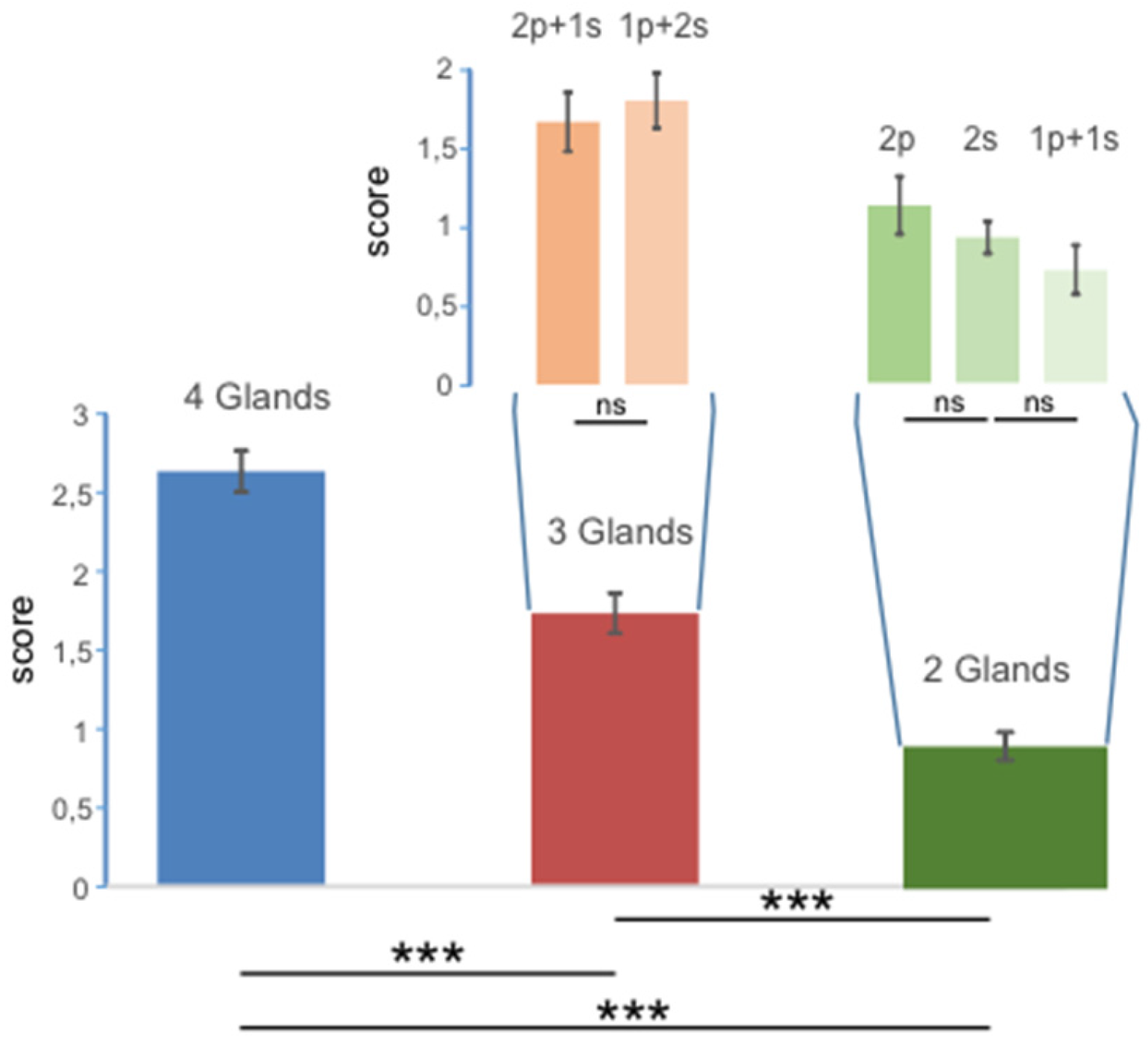
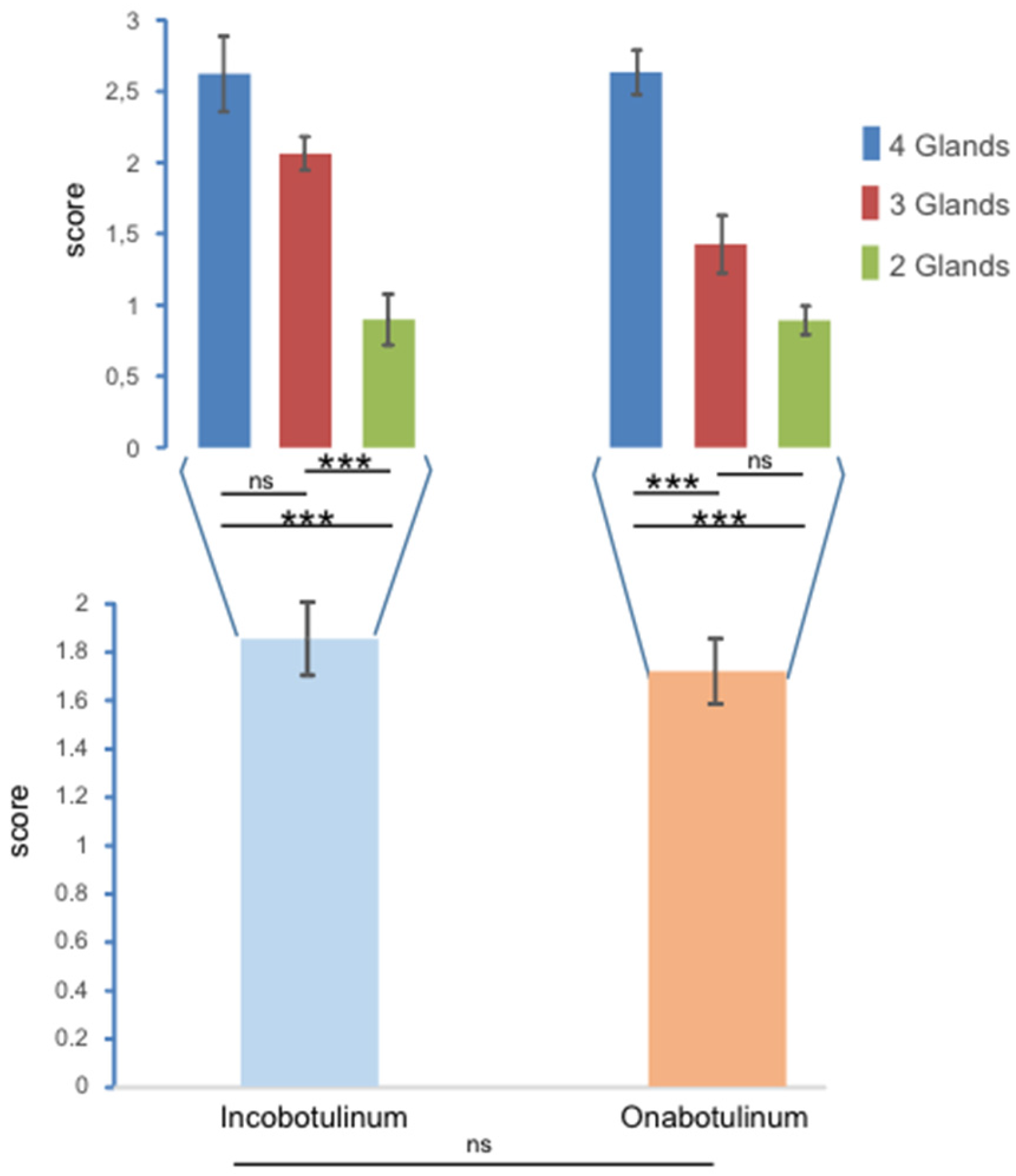
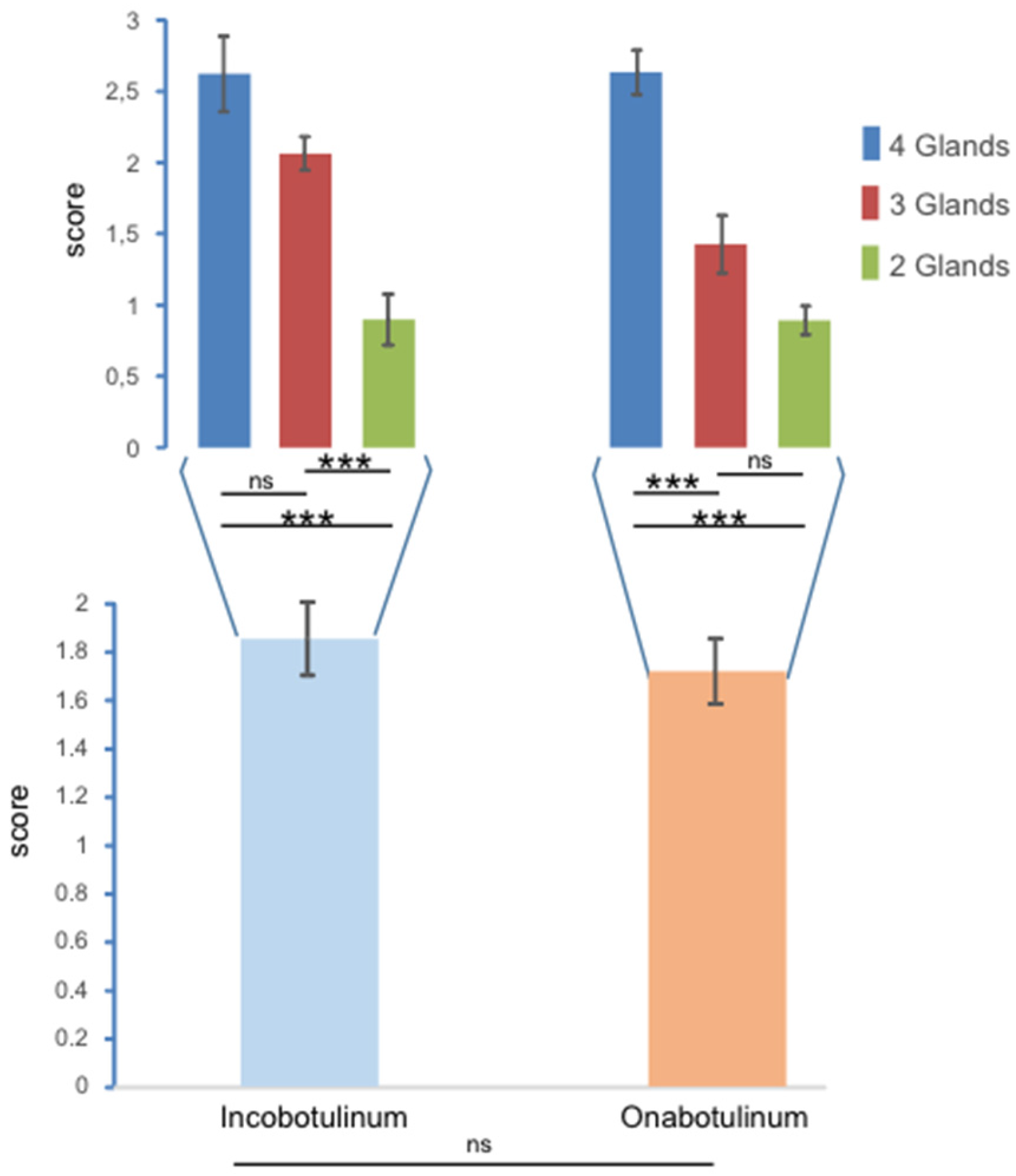
2. Results
3. Discussion
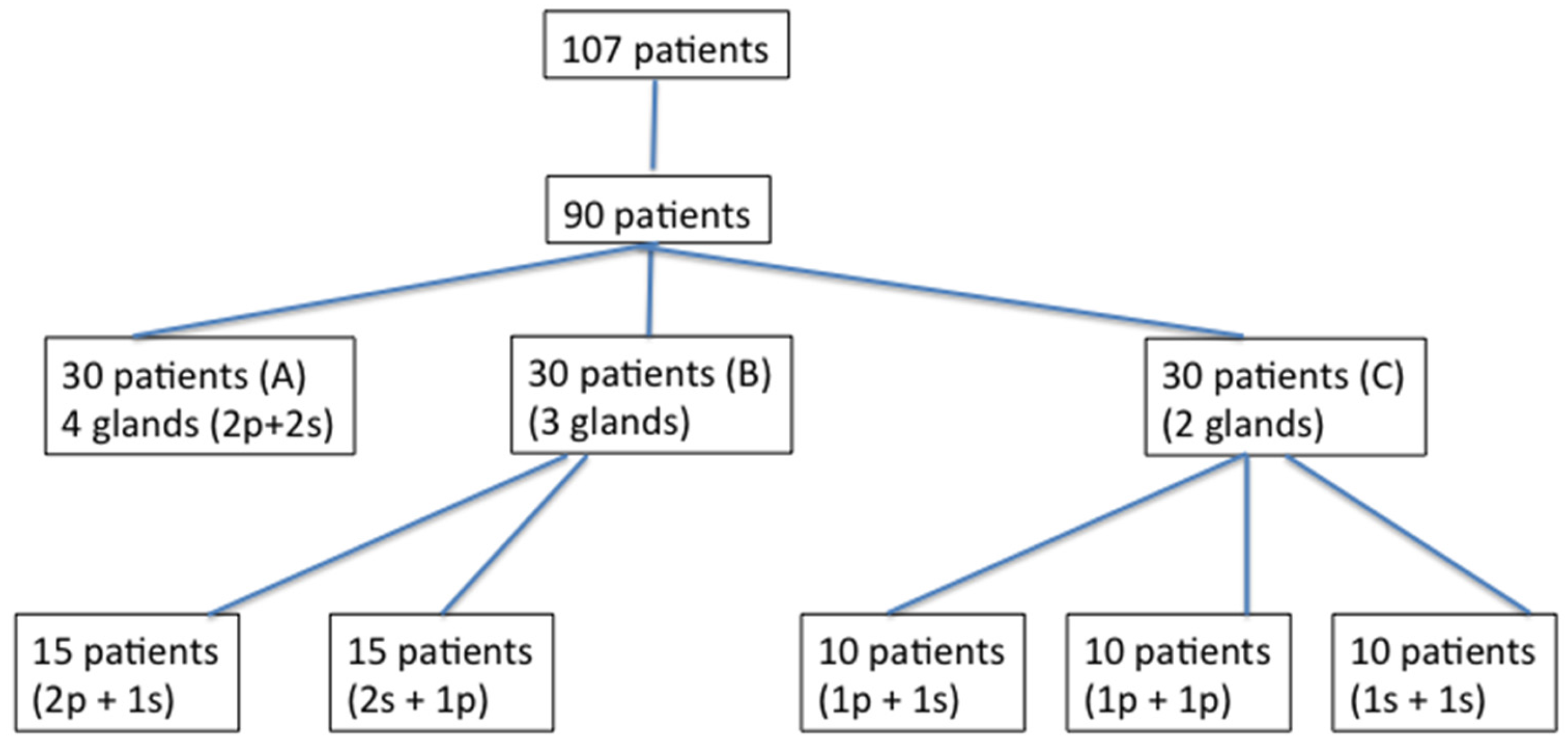
4. Materials and Methods
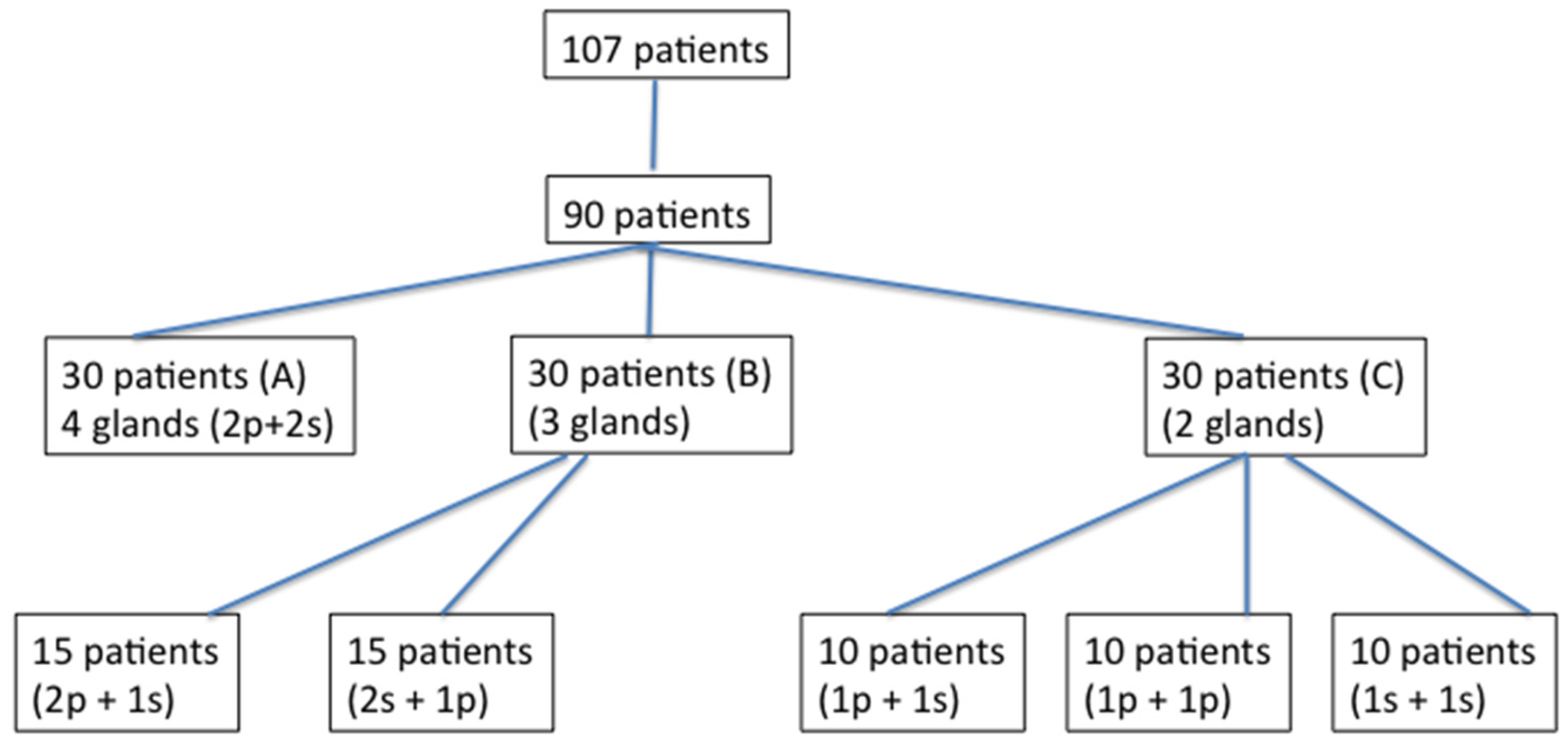
4.1. Patients
4.2. Inclusion criteria
4.3. Exclusion criteria
4.4. Treatment
4.5. Assessment
4.6. Statistical analysis
Author Contributions
Conflicts of Interest
References
- Banerjee, K.J.; Glasson, C.; O’Flaherty, S.J. Parotid and submandibular botulinum toxin a injections for sialorrhoea in children with cerebral palsy. Dev. Med. Child. Neurol. 2006, 48, 883–887. [Google Scholar] [CrossRef] [PubMed]
- Banfi, P.; Ticozzi, N.; Lax, A.; Guidugli, G.A.; Nicolini, A.; Silani, V. A review of options for treating sialorrhea in amyotrophic lateral sclerosis. Respir. Care 2015, 60, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Borg, M.; Hirst, F. The role of radiation therapy in the management of sialorrhoea. Int. J. Radiat. Oncol. Biol. Phys. 1998, 41, 1113–1119. [Google Scholar] [CrossRef]
- Dias, B.L.; Fernandes, A.R.; Maia Filho, H.S. Sialorrhea in children with cerebral palsy. J. Pediatr. 2016, 92, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Fuster Torres, M.A.; Berini Aytes, L.; Gay Escoda, C. Salivary gland application of botulinum toxin for the treatment of sialorrhea. Med. Oral Patol. Oral Cir. Bucal. 2007, 12, E511–E517. [Google Scholar] [PubMed]
- García Ron, A.; Miranda, M.C.; Garriga Braun, C.; Jensen Verón, J.; Torrens Martinez, J.; Diez Hanbino, M.P. Efficacy and safety of botulinum toxin in the treatment of sialorrhea in children with neurological disorders. An. Pediatr. 2012, 77, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Jeung, I.S.; Lee, S.; Kim, H.S.; Yeo, C.K. Effect of botulinum toxin a injection into the salivary glands for sialorrhea in children with neurologic disorders. Ann. Rehabil. Med. 2012, 36, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Lagalla, G.; Millevolte, M.; Capecci, M.; Provinciali, L.; Ceravolo, M.G. Botulinum toxin type a for drooling in Parkinson’s disease: A double-blind, randomized, placebo-controlled study. Mov. Disord. 2006, 5, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Lovato, A.; Restivo, D.A.; Ottaviano, G.; Marioni, G.; Marchese-Ragona, R. Botulinum toxin therapy: Functional silencing of salivary disorders. Acta Otorhinolaryngol. Ital. 2017, 37, 168–171. [Google Scholar] [PubMed]
- McGeachan, A.J.; Mcdermott, C.J. Management of oral secretions in neurological disease. Pract. Neurol. 2017, 17, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Naumann, M.; Jost, W.H.; Toyka, K.V. Botulinum toxin in the treatment of neurological disorders of the autonomic nervous system. Arch. Neurol. 1999, 56, 914–916. [Google Scholar] [CrossRef] [PubMed]
- Porta, M.; Gamba, M.; Bertacchi, G.; Vaj, P. Treatment of shialorrhoea with ultrasound guided botulinum toxin type a injection in patients with neurological disorders. J. Neurol. Neurosurg. Psychiatry 2001, 70, 538–540. [Google Scholar] [CrossRef] [PubMed]
- Potulska, A.; Friedman, A. Controlling sialorrhoea: A treatment options. Expert Opin. Pharmacother. 2005, 6, 1551–1554. [Google Scholar] [CrossRef] [PubMed]
- Dashtpour, K.; Bhidayasiri, R.; Chen, J.J.; Jabbari, B.; Lew, M.; Torres-Russotto, D. RimabotulinumtoxinB in sialorrhoea: Systematic review of clinical trials. J. Clin. Mov. Disord. 2017, 6. [Google Scholar] [CrossRef]
- Reid, S.M.; Johnstone, B.R.; Westbury, C.; Rawicki, B.; Reddihough, D.S. Randomized trial of botulinum toxin injections into the salivary glands to reduce drooling in children with neurological disorders. Dev. Med. Child. Neurol. 2008, 50, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Srivanitchapoom, P.; Pandey, S.; Hallett, M. Drooling in parkinson’s disease: A review. Parkinsonism Relat. Disord. 2014, 20, 1109–1118. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Sex | Disease | Injected Glands | Effects (2 Weeks) | Type of Toxin | Group |
|---|---|---|---|---|---|---|---|
| 1 | 40 | F | CP | 2p-2s | 2 | Ona | A |
| 2 | 56 | F | PD | 2p-2s | 3 | Inco | A |
| 3 | 73 | M | PD | 2p-2s | 3 | Inco | A |
| 4 | 71 | M | PD | 2p-2s | 3 | Inco | A |
| 5 | 67 | F | Stroke | 2p-2s | 2 | Ona | A |
| 6 | 72 | M | Stroke | 2p-2s | 3 | Ona | A |
| 7 | 63 | M | PD | 2p-2s | 3 | Ona | A |
| 8 | 65 | F | PD | 2p-2s | 3 | Ona | A |
| 9 | 50 | M | BI | 2p-2s | 2 | Ona | A |
| 10 | 28 | M | Stroke | 2p-2s | 3 | Ona | A |
| 11 | 55 | M | PD | 2p-2s | 3 | Ona | A |
| 12 | 55 | F | Stroke | 2p-2s | 3 | Ona | A |
| 13 | 67 | F | PD | 2p-2s | 3 | Ona | A |
| 14 | 72 | M | PD | 2p-2s | 2 | Ona | A |
| 15 | 63 | M | PD | 2p-2s | 3 | Ona | A |
| 16 | 65 | F | Stroke | 2p-2s | 2 | Ona | A |
| 17 | 73 | M | PD | 2p-2s | 3 | Ona | A |
| 18 | 71 | M | PD | 2p-2s | 3 | Inco | A |
| 19 | 67 | M | BI | 2p-2s | 1 | Inco | A |
| 20 | 55 | M | PD | 2p-2s | 3 | Inco | A |
| 21 | 63 | M | PD | 2p-2s | 3 | Ona | A |
| 22 | 65 | M | PD | 2p-2s | 3 | Ona | A |
| 23 | 50 | F | Stroke | 2p-2s | 3 | Ona | A |
| 24 | 45 | F | CP | 2p-2s | 3 | Ona | A |
| 25 | 19 | F | CP | 2p-2s | 3 | Ona | A |
| 26 | 71 | M | PD | 2p-2s | 0 | Ona | A |
| 27 | 72 | M | PD | 2p-2s | 2 | Inco | A |
| 28 | 66 | M | Stroke | 2p-2s | 3 | Inco | A |
| 29 | 18 | M | BI | 2p-2s | 3 | Ona | A |
| 30 | 18 | M | CP | 2p-2s | 3 | Ona | A |
| 31 | 61 | M | PD | 2p-1s | 1 | Ona | B |
| 32 | 59 | M | ALS | 2p-1s | 0 | Ona | B |
| 33 | 71 | M | PD | 2p-1s | 2 | Ona | B |
| 34 | 48 | M | PD | 2p-1s | 1 | Ona | B |
| 35 | 55 | M | BI | 2p-1s | 2 | Inco | B |
| 36 | 67 | M | PD | 2p-1s | 2 | Inco | B |
| 37 | 72 | F | Stroke | 2p-1s | 2 | Inco | B |
| 38 | 55 | F | ALS | 2p-1s | 2 | Inco | B |
| 39 | 63 | M | Stroke | 2p-1s | 2 | Ona | B |
| 40 | 65 | M | Stroke | 2p-1s | 2 | Ona | B |
| 41 | 50 | M | PD | 2p-1s | 1 | Ona | B |
| 42 | 67 | F | PD | 2p-1s | 2 | Inco | B |
| 43 | 70 | M | PD | 2p-1s | 2 | Inco | B |
| 44 | 53 | M | PD | 2p-1s | 3 | Inco | B |
| 45 | 22 | M | CP | 2p-1s | 1 | Ona | B |
| 46 | 53 | M | ALS | 1p-2s | 1 | Inco | B |
| 47 | 47 | M | Stroke | 1p-2s | 2 | Inco | B |
| 48 | 59 | F | PD | 1p-2s | 2 | Inco | B |
| 49 | 72 | M | Stroke | 1p-2s | 2 | Inco | B |
| 50 | 61 | F | PD | 1p-2s | 1 | Ona | B |
| 51 | 18 | F | CP | 1p-2s | 2 | Inco | B |
| 52 | 21 | M | CP | 1p-2s | 2 | Inco | B |
| 53 | 18 | F | CP | 1p-2s | 2 | Ona | B |
| 54 | 69 | M | PD | 1p-2s | 2 | Inco | B |
| 55 | 49 | F | CP | 1p-2s | 3 | Inco | B |
| 56 | 29 | F | CP | 1p-2s | 2 | Ona | B |
| 57 | 46 | F | CP | 1p-2s | 2 | Ona | B |
| 58 | 68 | F | ALS | 1p-2s | 0 | Ona | B |
| 59 | 29 | F | CP | 1p-2s | 2 | Ona | B |
| 60 | 57 | M | Stroke | 1p-2s | 2 | Ona | B |
| 61 | 66 | F | ALS | 2p | 0 | Inco | C |
| 62 | 38 | M | BI | 2p | 1 | Ona | C |
| 63 | 66 | F | ALS | 2p | 1 | Ona | C |
| 64 | 38 | M | BI | 2p | 1 | Ona | C |
| 65 | 36 | M | CP | 2p | 2 | Ona | C |
| 66 | 28 | M | CP | 2p | 1 | Inco | C |
| 67 | 63 | M | ALS | 2p | 1 | Ona | C |
| 68 | 71 | F | Stroke | 2p | 2 | Inco | C |
| 69 | 70 | M | ALS | 2p | 1 | Ona | C |
| 70 | 69 | M | Stroke | 2p | 1 | Ona | C |
| 71 | 58 | M | Stroke | 2s | 1 | Inco | C |
| 72 | 61 | M | PD | 2s | 1 | Inco | C |
| 73 | 70 | F | ALS | 2s | 1 | Inco | C |
| 74 | 65 | F | ALS | 2s | 0 | Ona | C |
| 75 | 25 | F | Stroke | 2s | 1 | Ona | C |
| 76 | 22 | M | CP | 2s | 1 | Ona | C |
| 77 | 37 | M | BI | 2s | 1 | Inco | C |
| 78 | 54 | M | BI | 2s | 1 | Ona | C |
| 79 | 70 | M | Stroke | 2s | 1 | Ona | C |
| 80 | 59 | M | Stroke | 2s | 1 | Ona | C |
| 81 | 22 | M | CP | 1p-1s | 1 | Ona | C |
| 82 | 24 | M | CP | 1p-1s | 1 | Inco | C |
| 83 | 49 | F | ALS | 1p-1s | 0 | Inco | C |
| 84 | 21 | M | CP | 1p-1s | 1 | Ona | C |
| 85 | 73 | M | PD | 1p-1s | 1 | Inco | C |
| 86 | 69 | F | PD | 1p-1s | 0 | Ona | C |
| 87 | 26 | F | CP | 1p-1s | 1 | Ona | C |
| 88 | 68 | M | Stroke | 1p-1s | 1 | Ona | C |
| 89 | 65 | F | Stroke | 1p-1s | 0 | Ona | C |
| 90 | 34 | M | BI | 1p-1s | 1 | Ona | C |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Restivo, D.A.; Panebianco, M.; Casabona, A.; Lanza, S.; Marchese-Ragona, R.; Patti, F.; Masiero, S.; Biondi, A.; Quartarone, A. Botulinum Toxin A for Sialorrhoea Associated with Neurological Disorders: Evaluation of the Relationship between Effect of Treatment and the Number of Glands Treated. Toxins 2018, 10, 55. https://doi.org/10.3390/toxins10020055
Restivo DA, Panebianco M, Casabona A, Lanza S, Marchese-Ragona R, Patti F, Masiero S, Biondi A, Quartarone A. Botulinum Toxin A for Sialorrhoea Associated with Neurological Disorders: Evaluation of the Relationship between Effect of Treatment and the Number of Glands Treated. Toxins. 2018; 10(2):55. https://doi.org/10.3390/toxins10020055
Chicago/Turabian StyleRestivo, Domenico A., Mariangela Panebianco, Antonino Casabona, Sara Lanza, Rosario Marchese-Ragona, Francesco Patti, Stefano Masiero, Antonio Biondi, and Angelo Quartarone. 2018. "Botulinum Toxin A for Sialorrhoea Associated with Neurological Disorders: Evaluation of the Relationship between Effect of Treatment and the Number of Glands Treated" Toxins 10, no. 2: 55. https://doi.org/10.3390/toxins10020055