Effect of Botulinum Toxin on Masticatory Muscle Pain in Patients with Temporomandibular Disorders: A Randomized, Double-Blind, Placebo-Controlled Pilot Study


Abstract
:1. Introduction
2. Results
2.1. Participants
2.2. Differences between Groups
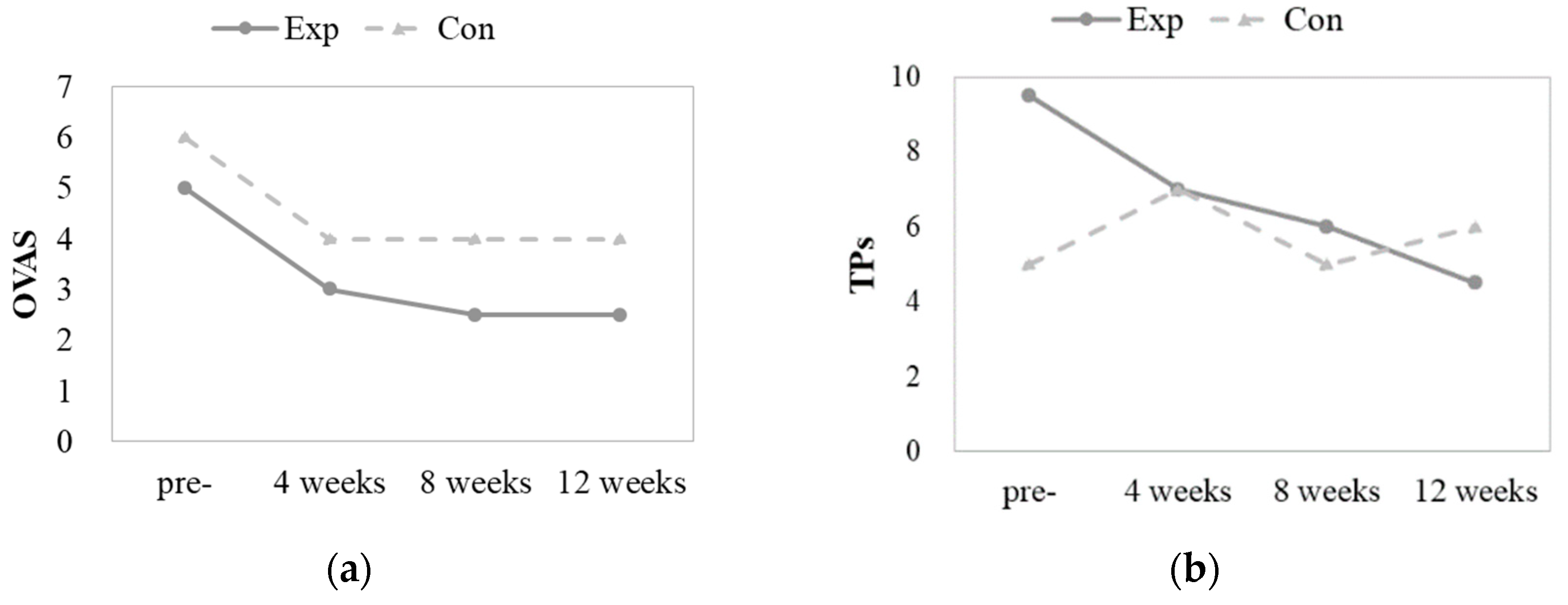
2.2.1. Comparison of Changes over Time within Groups
2.2.2. Comparison of Changes between Groups
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Subjects
5.2. Study Design
5.3. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral. Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Sunil Dutt, C.; Ramnani, P.; Thakur, D.; Pandit, M. Botulinum toxin in the treatment of muscle specific Oro-facial pain: A literature review. J. Maxillofac. Oral. Surg. 2015, 14, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Mor, N.; Tang, C.; Blitzer, A. Temporomandibular myofacial pain treated with botulinum toxin injection. Toxins 2015, 7, 2791–2800. [Google Scholar] [CrossRef] [PubMed]
- Steinkeler, A. Epidemiology, diagnosis, and treatment of temporomandibular disorders. Dent. Clin. 2013, 57, 465–479. [Google Scholar]
- Mohlin, B.; Kopp, S. A clinical study on the relationship between malocclusions, occlusal interferences and mandibular pain and dysfunction. Swed. Dent. J. 1978, 2, 105–112. [Google Scholar]
- Upton, L.G.; Scott, R.F.; Hayward, J.R. Major maxillomandibular malrelations and temporomandibular joint pain-dysfunction. J. Prosthet. Dent. 1984, 51, 686–690. [Google Scholar] [CrossRef]
- Bakke, M. Mandibular elevator muscles: Physiology, action, and effect of dental occlusion. Eur. J. Oral Sci. 1993, 101, 314–331. [Google Scholar] [CrossRef]
- Cioffi, I.; Landino, D.; Donnarumma, V.; Castroflorio, T.; Lobbezoo, F.; Michelotti, A. Frequency of daytime tooth clenching episodes in individuals affected by masticatory muscle pain and pain-free controls during standardized ability tasks. Clin. Oral Investig. 2017, 21, 1139–1148. [Google Scholar] [CrossRef]
- Abe, S.; Miyagi, A.; Yoshinaga, K.; Matsuka, Y.; Matsumoto, F.; Uyama, E.; Suzuki, Y.; Oshima, M.; Okura, K.; Tanaka, E. Immediate effect of masticatory muscle activity with transcutaneous electrical nerve stimulation in muscle pain of temporomandibular disorders patients. J. Clin. Med. 2020, 9, 3330. [Google Scholar] [CrossRef]
- Herb, K.; Cho, S.; Stiles, M.A. Temporomandibular joint pain and dysfunction. Curr. Pain Headache Rep. 2006, 10, 408–414. [Google Scholar] [CrossRef]
- Wieckiewicz, M.; Zietek, M.; Smardz, J.; Zenczak-Wieckiewicz, D.; Grychowska, N. Mental status as a common factor for masticatory muscle pain: A systematic review. Front. Psychol. 2017, 8, 646. [Google Scholar] [CrossRef] [PubMed]
- Sidebottom, A.J.; Patel, A.A.; Amin, J. Botulinum injection for the management of myofascial pain in the masticatory muscles. A prospective outcome study. Br. J. Oral Maxillofac. Surg. 2013, 51, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Ballegaard, V.; Thede-Schmidt-Hansen, P.; Svensson, P.; Jensen, R. Are headache and temporomandibular disorders related? A blinded study. Cephalalgia 2008, 28, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Glaros, A.; Urban, D.; Locke, J. Headache and temporomandibular disorders: Evidence for diagnostic and behavioural overlap. Cephalalgia 2007, 27, 542–549. [Google Scholar] [CrossRef]
- Coté, T.R.; Mohan, A.K.; Polder, J.A.; Walton, M.K.; Braun, M.M. Botulinum toxin type A injections: Adverse events reported to the US Food and Drug Administration in therapeutic and cosmetic cases. J. Am. Acad. Dermatol. 2005, 53, 407–415. [Google Scholar] [CrossRef]
- Song, P.; Schwartz, J.; Blitzer, A. The emerging role of botulinum toxin in the treatment of temporomandibular disorders. Oral Dis. 2007, 13, 253–260. [Google Scholar] [CrossRef]
- Mense, S. Neurobiological basis for the use of botulinum toxin in pain therapy. J. Neurol. 2004, 251, i1–i7. [Google Scholar] [CrossRef]
- Aoki, K.R. Evidence for antinociceptive activity of botulinum toxin type A in pain management. Headache 2003, 43, 9–15. [Google Scholar] [CrossRef]
- Delcanho, R.; Val, M.; Guarda Nardini, L.; Manfredini, D. Botulinum Toxin for Treating Temporomandibular Disorders: What is the Evidence? J. Oral Facial Pain Headache 2022, 36, 6–20. [Google Scholar] [CrossRef]
- De la Torre Canales, G.; Alvarez-Pinzon, N.; Muñoz-Lora, V.R.M.; Vieira Peroni, L.; Farias Gomes, A.; Sánchez-Ayala, A.; Haiter-Neto, F.; Manfredini, D.; Rizzatti-Barbosa, C.M. Efficacy and safety of botulinum toxin type A on persistent myofascial pain: A randomized clinical trial. Toxins 2020, 12, 395. [Google Scholar] [CrossRef]
- De Carli, B.M.G.; Magro, A.K.D.; Souza-Silva, B.N.; de Souza Matos, F.; De Carli, J.P.; Paranhos, L.R.; Magro, E.D. The effect of laser and botulinum toxin in the treatment of myofascial pain and mouth opening: A randomized clinical trial. J. Photochem. Photobiol. B 2016, 159, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Kütük, S.G.; Özkan, Y.; Kütük, M.; Özdaş, T. Comparison of the efficacies of dry needling and botox methods in the treatment of myofascial pain syndrome affecting the temporomandibular joint. J. Craniofac. Surg. 2019, 30, 1556–1559. [Google Scholar] [CrossRef] [PubMed]
- Muñoz Lora, V.; Del Bel Cury, A.; Jabbari, B.; Lacković, Z. Botulinum toxin type A in dental medicine. J. Dent. Res. 2019, 98, 1450–1457. [Google Scholar] [CrossRef] [PubMed]
- Govindarajan, R.; Shepard, K.M.; Moschonas, C.; Chen, J.J. Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Payment policy perspectives. Neurol. Clin. Pract. 2016, 6, 281–286. [Google Scholar] [CrossRef]
- Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef]
- Nixdorf, D.R.; Heo, G.; Major, P.W. Randomized controlled trial of botulinum toxin A for chronic myogenous orofacial pain. Pain 2002, 99, 465–473. [Google Scholar] [CrossRef]
- Ernberg, M.; Hedenberg-Magnusson, B.; List, T.; Svensson, P. Efficacy of botulinum toxin type A for treatment of persistent myofascial TMD pain: A randomized, controlled, double-blind multicenter study. Pain 2011, 152, 1988–1996. [Google Scholar] [CrossRef]
- Guarda-Nardini, L.; Manfredini, D.; Salamone, M.; Salmaso, L.; Tonello, S.; Ferronato, G. Efficacy of botulinum toxin in treating myofascial pain in bruxers: A controlled placebo pilot study. Cranio 2008, 26, 126–135. [Google Scholar] [CrossRef]
- Rollnik, J.D.; Tanneberger, O.; Schubert, M.; Schneider, U.; Dengler, R. Treatment of tension-type headache with botulinum toxin type A: A double-blind, placebo-controlled study. Headache 2000, 40, 300–305. [Google Scholar] [CrossRef]
- Schulte-Mattler, W.J.; Krack, P.; Group, B.S. Treatment of chronic tension-type headache with botulinum toxin A: A randomized, double-blind, placebo-controlled multicenter study. Pain 2004, 109, 110–114. [Google Scholar] [CrossRef]
- Jackson, J.L.; Kuriyama, A.; Hayashino, Y. Botulinum toxin A for prophylactic treatment of migraine and tension headaches in adults: A meta-analysis. JAMA 2012, 307, 1736–1745. [Google Scholar] [PubMed]
- Linde, M.; Hagen, K.; Salvesen, Ø.; Gravdahl, G.B.; Helde, G.; Stovner, L.J. Onabotulinum toxin A treatment of cervicogenic headache: A randomised, double-blind, placebo-controlled crossover study. Cephalalgia 2011, 31, 797–807. [Google Scholar] [CrossRef] [PubMed]
- de-la-Hoz, J.L.; de-Pedro, M.; Martín-Fontelles, I.; Mesa-Jimenez, J.; Chivato, T.; Bagües, A. Efficacy of botulinum toxin type A in the management of masticatory myofascial pain: A retrospective clinical study. J. Am. Dent. Assoc. 2022, 153, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, F.M.; Bearn, L.; Rothrock, R.; King, L. Evidence against trigger point injection technique for the treatment of cervicothoracic myofascial pain with botulinum toxin type A. Anesthesiology 2005, 103, 377–383. [Google Scholar] [CrossRef]
- De la Torre Canales, G.; Poluha, R.L.; Pinzón, N.A.; Da Silva, B.R.; Almeida, A.M.; Ernberg, M.; Manso, A.C.; Bonjardim, L.R.; Rizzatti-Barbosa, C.M. Efficacy of botulinum toxin type-A I in the improvement of mandibular motion and muscle sensibility in myofascial pain TMD Subjects: A randomized controlled trial. Toxins 2022, 14, 441. [Google Scholar] [CrossRef]
- von Lindern, J.J.; Niederhagen, B.; Bergé, S.; Appel, T. Type A botulinum toxin in the treatment of chronic facial pain associated with masticatory hyperactivity. J. Oral Maxillofac. Surg. 2003, 61, 774–778. [Google Scholar] [CrossRef]
- Patel, A.A.; Lerner, M.Z.; Blitzer, A. IncobotulinumtoxinA injection for temporomandibular joint disorder: A randomized controlled pilot study. Ann. Otol. Rhinol. Laryngol. 2017, 126, 328–333. [Google Scholar] [CrossRef]
- Kurtoglu, C.; Gur, O.H.; Kurkcu, M.; Sertdemir, Y.; Guler-Uysal, F.; Uysal, H. Effect of botulinum toxin-A in myofascial pain patients with or without functional disc displacement. J. Oral Maxillofac. Surg. 2008, 66, 1644–1651. [Google Scholar] [CrossRef]
- Thambar, S.; Kulkarni, S.; Armstrong, S.; Nikolarakos, D. Botulinum toxin in the management of temporomandibular disorders: A systematic review. Br. J. Oral Maxillofac. Surg. 2020, 58, 508–519. [Google Scholar] [CrossRef]
- Anderson, G.C.; John, M.T.; Ohrbach, R.; Nixdorf, D.R.; Schiffman, E.L.; Truelove, E.S.; List, T. Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain. Pain 2011, 152, 765–771. [Google Scholar] [CrossRef]
- Golanska, P.; Saczuk, K.; Domarecka, M.; Kuć, J.; Lukomska-Szymanska, M. Temporomandibular Myofascial Pain Syndrome—Aetiology and Biopsychosocial Modulation. A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 7807. [Google Scholar] [CrossRef] [PubMed]
- Freund, B.; Schwartz, M.; Symington, J.M. The use of botulinum toxin for the treatment of temporomandibular disorders: Preliminary findings. J. Oral Maxillofac. Surg. 1999, 57, 916–920. [Google Scholar] [CrossRef] [PubMed]
- Sandrini, G.; De Icco, R.; Tassorelli, C.; Smania, N.; Tamburin, S. Botulinum neurotoxin type A for the treatment of pain: Not just in migraine and trigeminal neuralgia. J. Headache Pain 2017, 18, 38. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Effects of botulinum toxin type A on pain among trigeminal neuralgia, myofascial temporomandibular disorders, and oromandibular dystonia. Toxins 2021, 13, 605. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Exp (n = 14) | Con (n = 7) | Total (n = 21) | p-Value |
|---|---|---|---|---|
| Sex | ||||
| Male | 2(14.3) | 0(0.0) | 2(9.5) | 0.293 |
| Female | 12(85.7) | 7(100.0) | 19(90.5) | |
| Age (M ± SD) | 34.71 ± 9.73 | 32.43 ± 10.23 | 33.95 ± 9.70 | 0.623 |
| Variables | Group | Time | M ± SD | Q1 | Median | Q3 | p-Value |
|---|---|---|---|---|---|---|---|
| OVAS | Exp | Pre-injection | 5.00 ± 1.45 | 4.00 | 5.00 a | 6.13 | 0.003 * |
| 4 weeks | 2.64 ± 2.02 | 0.00 | 3.00 b | 4.25 | |||
| 8 weeks | 2.39 ± 2.24 | 0.00 | 2.50 b | 4.00 | |||
| 12 weeks | 2.50 ± 2.31 | 0.00 | 2.50 b | 4.25 | |||
| Con | Pre-injection | 5.36 ± 1.44 | 4.00 | 6.00 | 6.50 | 0.256 | |
| 4 weeks | 3.64 ± 2.06 | 2.00 | 4.00 | 5.00 | |||
| 8 weeks | 3.79 ± 2.00 | 3.00 | 4.00 | 5.00 | |||
| 12 weeks | 3.43 ± 1.81 | 3.00 | 4.00 | 4.00 | |||
| TPs | Exp | Pre-injection | 10.07 ± 3.79 | 7.50 | 9.50 a | 12.75 | <0.001 * |
| 4 weeks | 6.86 ± 3.61 | 3.00 | 7.00 b | 10.25 | |||
| 8 weeks | 5.86 ± 4.66 | 2.50 | 6.00 b | 8.50 | |||
| 12 weeks | 5.07 ± 4.03 | 1.50 | 4.50 b | 9.25 | |||
| Con | Pre-injection | 7.43 ± 4.54 | 4.00 | 5.00 | 10.00 | 0.588 | |
| 4 weeks | 6.86 ± 4.06 | 4.00 | 7.00 | 7.00 | |||
| 8 weeks | 5.57 ± 3.21 | 4.00 | 5.00 | 8.00 | |||
| 12 weeks | 5.86 ± 4.60 | 1.00 | 6.00 | 11.00 | |||
| MMO | Exp | Pre-injection | 46.57 ± 7.18 | 41.75 | 46.50 | 50.25 | 0.189 |
| 4 weeks | 45.71 ± 7.96 | 40.00 | 43.00 | 50.25 | |||
| 8 weeks | 46.57 ± 7.97 | 40.75 | 44.50 | 52.75 | |||
| 12 weeks | 47.21 ± 8.09 | 40.75 | 46.50 | 52.75 | |||
| Con | Pre-injection | 48.00 ± 6.61 | 42.00 | 47.00 | 52.00 | 0.242 | |
| 4 weeks | 47.00 ± 5.72 | 42.00 | 46.00 | 50.00 | |||
| 8 weeks | 46.29 ± 5.02 | 41.00 | 46.00 | 50.00 | |||
| 12 weeks | 46.43 ± 3.95 | 43.00 | 46.00 | 50.00 | |||
| HVAS | Exp | Pre-injection | 3.61 ± 2.63 | 0.00 | 4.50 a | 6.00 | 0.005 * |
| 4 weeks | 2.00 ± 2.18 | 0.00 | 1.50 b | 4.00 | |||
| 8 weeks | 1.64 ± 2.10 | 0.00 | 0.00 b | 4.00 | |||
| 12 weeks | 1.46 ± 2.45 | 0.00 | 0.00 b | 4.13 | |||
| Con | Pre-injection | 4.79 ± 1.15 | 4.00 | 5.00 | 5.00 | 0.768 | |
| 4 weeks | 2.36 ± 2.46 | 0.00 | 2.00 | 5.00 | |||
| 8 weeks | 3.36 ± 2.63 | 0.00 | 4.00 | 5.50 | |||
| 12 weeks | 3.00 ± 1.94 | 1.00 | 3.00 | 4.50 | |||
| HF | Exp | Pre-injection | 5.71 ± 8.43 | 0.00 | 2.00 a | 12.00 | 0.002 * |
| 4 weeks | 2.00 ± 3.92 | 0.00 | 1.00 ab | 2.00 | |||
| 8 weeks | 1.29 ± 2.64 | 0.00 | 0.00 b | 2.00 | |||
| 12 weeks | 1.36 ± 2.53 | 0.00 | 0.00 b | 2.50 | |||
| Con | Pre-injection | 8.00 ± 10.15 | 2.00 | 4.00 | 10.00 | 0.119 | |
| 4 weeks | 5.43 ± 10.95 | 0.00 | 1.00 | 4.00 | |||
| 8 weeks | 2.71 ± 3.45 | 0.00 | 2.00 | 3.00 | |||
| 12 weeks | 1.93 ± 1.17 | 1.00 | 2.00 | 3.00 |
| Variables | Time | Group | M ± SD | Q1 | Median | Q3 | p-Value |
|---|---|---|---|---|---|---|---|
| OVAS | 4 weeks—pre-injection | Exp | −2.36 ± 2.38 | −4.00 | −2.75 | 0.00 | 0.474 |
| Con | −1.71 ± 2.69 | −3.00 | −1.00 | 0.00 | |||
| 8 weeks—pre-injection | Exp | −2.61 ± 2.28 | −4.00 | −2.75 | 0.00 | 0.244 | |
| Con | −1.57 ± 2.71 | −2.50 | −1.00 | 0.50 | |||
| 12 weeks—pre-injection | Exp | −2.50 ± 2.45 | −4.00 | −2.00 | −1.00 | 0.430 | |
| Con | −1.93 ± 2.62 | −3.00 | −1.00 | 0.00 | |||
| TPs | 4 weeks—pre-injection | Exp | −3.21 ± 1.58 | −4.25 | −3.00 | −2.00 | 0.009 * |
| Con | −0.57 ± 2.23 | −2.00 | −1.00 | 2.00 | |||
| 8 weeks—pre-injection | Exp | −4.21 ± 3.17 | −6.00 | −4.00 | −2.00 | 0.076 | |
| Con | −1.86 ± 3.53 | −4.00 | 0.00 | 0.00 | |||
| 12 weeks—pre-injection | Exp | −5.00 ± 2.15 | −6.00 | −5.00 | −3.75 | 0.032 * | |
| Con | −1.57 ± 5.32 | −4.00 | 1.00 | 2.00 | |||
| MMO | 4 weeks—pre-injection | Exp | −0.86 ± 1.99 | −3.00 | 0.00 | 0.00 | 0.696 |
| Con | −1.00 ± 1.15 | −2.00 | −1.00 | 0.00 | |||
| 8 weeks—pre-injection | Exp | 0.00 ± 2.45 | −2.25 | 0.00 | 1.25 | 0.121 | |
| Con | −1.71 ± 2.36 | −5.00 | −1.00 | 0.00 | |||
| 12 weeks—pre-injection | Exp | 0.64 ± 2.84 | −1.25 | 0.00 | 3.00 | 0.240 | |
| Con | −1.57 ± 3.15 | −5.00 | 0.00 | 1.00 | |||
| HVAS | 4 weeks—pre-injection | Exp | −1.61 ± 2.42 | −2.63 | −0.50 | 0.00 | 0.647 |
| Con | −2.43 ± 2.95 | −4.00 | −3.00 | 0.50 | |||
| 8 weeks—pre-injection | Exp | −1.96 ± 2.34 | −3.25 | −1.50 | 0.00 | 0.377 | |
| Con | −1.43 ± 2.28 | −4.00 | 0.00 | 0.50 | |||
| 12 weeks—pre-injection | Exp | −2.14 ± 2.26 | −4.25 | −2.00 | 0.00 | 0.548 | |
| Con | −1.79 ± 2.53 | −4.00 | −2.00 | 0.50 | |||
| HF | 4 weeks—pre-injection | Exp | −3.71 ± 8.52 | −4.00 | 0.00 | 0.00 | 0.489 |
| Con | −2.57 ± 3.26 | −6.00 | −2.00 | 0.00 | |||
| 8 weeks—pre-injection | Exp | −4.43 ± 8.30 | −5.50 | −1.00 | 0.00 | 0.493 | |
| Con | −5.29 ± 7.02 | −7.00 | −4.00 | 0.00 | |||
| 12 weeks—pre-injection | Exp | −4.36 ± 7.22 | −6.00 | −1.50 | 0.00 | 0.567 | |
| Con | −6.07 ± 9.44 | −8.00 | −3.00 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.R.; Chang, M.; Kim, A.H.; Kim, S.T. Effect of Botulinum Toxin on Masticatory Muscle Pain in Patients with Temporomandibular Disorders: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Toxins 2023, 15, 597. https://doi.org/10.3390/toxins15100597
Kim SR, Chang M, Kim AH, Kim ST. Effect of Botulinum Toxin on Masticatory Muscle Pain in Patients with Temporomandibular Disorders: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Toxins. 2023; 15(10):597. https://doi.org/10.3390/toxins15100597
Chicago/Turabian StyleKim, So Ra, Min Chang, Alec Hyung Kim, and Seong Taek Kim. 2023. "Effect of Botulinum Toxin on Masticatory Muscle Pain in Patients with Temporomandibular Disorders: A Randomized, Double-Blind, Placebo-Controlled Pilot Study" Toxins 15, no. 10: 597. https://doi.org/10.3390/toxins15100597