The Therapeutic Effect of Botulinum Toxin Type A on Trigeminal Neuralgia: Are There Any Differences between Type 1 versus Type 2 Trigeminal Neuralgia?

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
3. Discussion
Limitations of the Study
4. Conclusions
5. Methods
5.1. Study Design and Participants
5.2. Ethics
5.3. Treatment with BoNT/A
5.4. PFPS, PGIC, and VAS
5.5. Endpoints
5.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Melzack, R.; Terrence, C.; Fromm, G.; Amsel, R. Trigeminal Neuralgia and Atypical Facial Pain: Use of the McGill Pain Questionnaire for Discrimination and Diagnosis. Pain 1986, 27, 297–302. [Google Scholar] [CrossRef]
- Pareja, J.A.; Cuadrado, M.L.; Caminero, A.B.; Barriga, F.J.; Barón, M.; Sánchez-del-Río, M. Duration of Attacks of First Division Trigeminal Neuralgia. Cephalalgia 2005, 25, 305–308. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 1–211. [CrossRef] [PubMed]
- Mueller, D.; Obermann, M.; Yoon, M.-S.; Poitz, F.; Hansen, N.; Slomke, M.-A.; Dommes, P.; Gizewski, E.; Diener, H.-C.; Katsarava, Z. Prevalence of Trigeminal Neuralgia and Persistent Idiopathic Facial Pain: A Population-Based Study. Cephalalgia 2011, 31, 1542–1548. [Google Scholar] [CrossRef] [PubMed]
- Koopman, J.S.H.A.; Dieleman, J.P.; Huygen, F.J.; de Mos, M.; Martin, C.G.M.; Sturkenboom, M.C.J.M. Incidence of Facial Pain in the General Population. Pain 2009, 147, 122–127. [Google Scholar] [CrossRef]
- Katusic, S.; Beard, C.M.; Bergstralh, E.; Kurland, L.T. Incidence and Clinical Features of Trigeminal Neuralgia, Rochester, Minnesota, 1945–1984. Ann. Neurol. 1990, 27, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Hall, G.C.; Carroll, D.; Parry, D.; McQuay, H.J. Epidemiology and Treatment of Neuropathic Pain: The UK Primary Care Perspective. Pain 2006, 122, 156–162. [Google Scholar] [CrossRef]
- Jones, M.R.; Urits, I.; Ehrhardt, K.P.; Cefalu, J.N.; Kendrick, J.B.; Park, D.J.; Cornett, E.M.; Kaye, A.D.; Viswanath, O. A Comprehensive Review of Trigeminal Neuralgia. Curr. Pain Headache Rep. 2019, 23, 74. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Yi, D.I.; Perez, J.N.J.; Liu, M.; Chang, S.D.; Barad, M.J.; Lim, M.; Qian, X. The Molecular Basis and Pathophysiology of Trigeminal Neuralgia. Int. J. Mol. Sci. 2022, 23, 3604. [Google Scholar] [CrossRef]
- Gronseth, G.; Cruccu, G.; Alksne, J.; Argoff, C.; Brainin, M.; Burchiel, K.; Nurmikko, T.; Zakrzewska, J.M. Practice Parameter: The Diagnostic Evaluation and Treatment of Trigeminal Neuralgia (an Evidence-Based Review): Report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies. Neurology 2008, 71, 1183–1190. [Google Scholar] [CrossRef]
- Cruccu, G.; Gronseth, G.; Alksne, J.; Argoff, C.; Brainin, M.; Burchiel, K.; Nurmikko, T.; Zakrzewska, J.M. AAN-EFNS Guidelines on Trigeminal Neuralgia Management. Eur. J. Neurol. 2008, 15, 1013–1028. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, G.; Maarbjerg, S.; Truini, A. Trigeminal Neuralgia Secondary to Multiple Sclerosis: From the Clinical Picture to the Treatment Options. J. Headache Pain 2019, 20, 20. [Google Scholar] [CrossRef] [PubMed]
- Olafson, R.A.; Rushton, J.G.; Sayre, G.P. Trigeminal Neuralgia in a Patient with Multiple Sclerosis. An Autopsy Report. J. Neurosurg. 1966, 24, 755–759. [Google Scholar] [CrossRef] [PubMed]
- Truini, A.; Prosperini, L.; Calistri, V.; Fiorelli, M.; Pozzilli, C.; Millefiorini, E.; Frontoni, M.; Cortese, A.; Caramia, F.; Cruccu, G. A Dual Concurrent Mechanism Explains Trigeminal Neuralgia in Patients with Multiple Sclerosis. Neurology 2016, 86, 2094–2099. [Google Scholar] [CrossRef] [PubMed]
- Cruccu, G.; Biasiotta, A.; Galeotti, F.; Iannetti, G.D.; Truini, A.; Gronseth, G. Diagnostic Accuracy of Trigeminal Reflex Testing in Trigeminal Neuralgia. Neurology 2006, 66, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Hilton, D.A.; Love, S.; Gradidge, T.; Coakham, H.B. Pathological Findings Associated with Trigeminal Neuralgia Caused by Vascular Compression. Neurosurgery 1994, 35, 299–303; discussion 303. [Google Scholar] [CrossRef]
- Mackinnon, S.E.; Dellon, A.L.; Hudson, A.R.; Hunter, D.A. Chronic Human Nerve Compression--a Histological Assessment. Neuropathol. Appl. Neurobiol. 1986, 12, 547–565. [Google Scholar] [CrossRef]
- Marinković, S.; Gibo, H.; Todorović, V.; Antić, B.; Kovacević, D.; Milisavljević, M.; Cetković, M. Ultrastructure and Immunohistochemistry of the Trigeminal Peripheral Myelinated Axons in Patients with Neuralgia. Clin. Neurol. Neurosurg. 2009, 111, 795–800. [Google Scholar] [CrossRef]
- Leal, P.R.L.; Barbier, C.; Hermier, M.; Souza, M.A.; Cristino-Filho, G.; Sindou, M. Atrophic Changes in the Trigeminal Nerves of Patients with Trigeminal Neuralgia Due to Neurovascular Compression and Their Association with the Severity of Compression and Clinical Outcomes. J. Neurosurg. 2014, 120, 1484–1495. [Google Scholar] [CrossRef]
- Gambeta, E.; Chichorro, J.G.; Zamponi, G.W. Trigeminal Neuralgia: An Overview from Pathophysiology to Pharmacological Treatments. Mol. Pain 2020, 16, 1744806920901890. [Google Scholar] [CrossRef]
- Yadav, Y.R.; Nishtha, Y.; Sonjjay, P.; Vijay, P.; Shailendra, R.; Yatin, K. Trigeminal Neuralgia. Asian J. Neurosurg. 2017, 12, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, P. Facial Pain. IV. A Prospective Study of 1052 Patients with a View of: Precipitating Factors, Associated Symptoms, Objective Psychiatric and Neurological Symptoms. Acta Neurochir. (Wien) 1991, 108, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Shankland, W.E. 2nd Trigeminal Neuralgia: Typical or Atypical? Cranio 1993, 11, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, P. Facial Pain. I. A Prospective Survey of 1052 Patients with a View of: Definition, Delimitation, Classification, General Data, Genetic Factors, and Previous Diseases. Acta Neurochir. (Wien) 1990, 107, 112–120. [Google Scholar] [CrossRef]
- Zakrzewska, J.M.; Wu, J.; Mon-Williams, M.; Phillips, N.; Pavitt, S.H. Evaluating the Impact of Trigeminal Neuralgia. Pain 2017, 158, 1166–1174. [Google Scholar] [CrossRef]
- O’Callaghan, L.; Floden, L.; Vinikoor-Imler, L.; Symonds, T.; Giblin, K.; Hartford, C.; Zakrzewska, J.M. Burden of Illness of Trigeminal Neuralgia among Patients Managed in a Specialist Center in England. J. Headache Pain 2020, 21, 130. [Google Scholar] [CrossRef]
- Luo, Y.; He, M.; Li, C.; Yang, H. A Research on Quality of Life Score (QOLS) of Patients with Trigeminal Neuralgia (TN). J. Infect. Public Health 2019, 12, 690–694. [Google Scholar] [CrossRef]
- Cruccu, G.; Di Stefano, G.; Truini, A. Trigeminal Neuralgia. N. Engl. J. Med. 2020, 383, 754–762. [Google Scholar] [CrossRef]
- Xu, R.; Xie, M.E.; Jackson, C.M. Trigeminal Neuralgia: Current Approaches and Emerging Interventions. J. Pain Res. 2021, 14, 3437–3463. [Google Scholar] [CrossRef]
- Tronnier, V.M.; Rasche, D.; Hamer, J.; Kienle, A.L.; Kunze, S. Treatment of Idiopathic Trigeminal Neuralgia: Comparison of Long-Term Outcome after Radiofrequency Rhizotomy and Microvascular Decompression. Neurosurgery 2001, 48, 1261–1268. [Google Scholar]
- Cheng, J.S.; Lim, D.A.; Chang, E.F.; Barbaro, N.M. A Review of Percutaneous Treatments for Trigeminal Neuralgia. Neurosurgery 2014, 10 (Suppl. S1), 25–33; discussion 33. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewska, J.M.; Jassim, S.; Bulman, S.J. A Prospective, Longitudinal Study on Patients with Trigeminal Neuralgia Who Underwent Radiofrequency Thermocoagulation of the Gasserian Ganglion. Pain 1999, 79, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Tuleasca, C.; Régis, J.; Sahgal, A.; De Salles, A.; Hayashi, M.; Ma, L.; Martínez-Álvarez, R.; Paddick, I.; Ryu, S.; Slotman, B.J.; et al. Stereotactic Radiosurgery for Trigeminal Neuralgia: A Systematic Review. J. Neurosurg. 2018, 130, 733–757. [Google Scholar] [CrossRef] [PubMed]
- Régis, J.; Tuleasca, C.; Resseguier, N.; Carron, R.; Donnet, A.; Yomo, S.; Gaudart, J.; Levivier, M. The Very Long-Term Outcome of Radiosurgery for Classical Trigeminal Neuralgia. Stereotact. Funct. Neurosurg. 2016, 94, 24–32. [Google Scholar] [CrossRef]
- Holste, K.; Chan, A.Y.; Rolston, J.D.; Englot, D.J. Pain Outcomes Following Microvascular Decompression for Drug-Resistant Trigeminal Neuralgia: A Systematic Review and Meta-Analysis. Neurosurgery 2020, 86, 182–190. [Google Scholar] [CrossRef]
- Morra, M.E.; Elgebaly, A.; Elmaraezy, A.; Khalil, A.M.; Altibi, A.M.A.; Vu, T.L.-H.; Mostafa, M.R.; Huy, N.T.; Hirayama, K. Therapeutic Efficacy and Safety of Botulinum Toxin A Therapy in Trigeminal Neuralgia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Headache Pain 2016, 17, 63. [Google Scholar] [CrossRef]
- Wu, S.; Lian, Y.; Zhang, H.; Chen, Y.; Wu, C.; Li, S.; Zheng, Y.; Wang, Y.; Cheng, W.; Huang, Z. Botulinum Toxin Type A for Refractory Trigeminal Neuralgia in Older Patients: A Better Therapeutic Effect. J. Pain Res. 2019, 12, 2177–2186. [Google Scholar] [CrossRef]
- Matak, I.; Rossetto, O.; Lacković, Z. Botulinum Toxin Type A Selectivity for Certain Types of Pain Is Associated with Capsaicin-Sensitive Neurons. Pain 2014, 155, 1516–1526. [Google Scholar] [CrossRef]
- Xiao, L.; Cheng, J.; Dai, J.; Zhang, D. Botulinum Toxin Decreases Hyperalgesia and Inhibits P2X3 Receptor Over-Expression in Sensory Neurons Induced by Ventral Root Transection in Rats. Pain Med. 2011, 12, 1385–1394. [Google Scholar] [CrossRef]
- Mika, J.; Rojewska, E.; Makuch, W.; Korostynski, M.; Luvisetto, S.; Marinelli, S.; Pavone, F.; Przewlocka, B. The Effect of Botulinum Neurotoxin A on Sciatic Nerve Injury-Induced Neuroimmunological Changes in Rat Dorsal Root Ganglia and Spinal Cord. Neuroscience 2011, 175, 358–366. [Google Scholar] [CrossRef]
- Xiao, L.; Cheng, J.; Zhuang, Y.; Qu, W.; Muir, J.; Liang, H.; Zhang, D. Botulinum Toxin Type A Reduces Hyperalgesia and TRPV1 Expression in Rats with Neuropathic Pain. Pain Med. 2013, 14, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Shibata, M.; Toriumi, H.; Iwashita, T.; Funakubo, M.; Sato, H.; Kuroi, T.; Ebine, T.; Koizumi, K.; Suzuki, N. Reduction of TRPV1 Expression in the Trigeminal System by Botulinum Neurotoxin Type-A. Neurobiol. Dis. 2012, 48, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Ovsepian, S.V.; Wang, J.; Pickering, M.; Sasse, A.; Aoki, K.R.; Lawrence, G.W.; Dolly, J.O. Activation of TRPV1 Mediates Calcitonin Gene-Related Peptide Release, Which Excites Trigeminal Sensory Neurons and Is Attenuated by a Retargeted Botulinum Toxin with Anti-Nociceptive Potential. J. Neurosci. Off. J. Soc. Neurosci. 2009, 29, 4981–4992. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.-H.; He, C.-H.; Zhang, H.-F.; Lian, Y.-J.; Chen, Y.; Wu, C.-J.; Ma, Y.-Q. Botulinum Toxin A in the Treatment of Trigeminal Neuralgia. Int. J. Neurosci. 2016, 126, 348–353. [Google Scholar] [CrossRef]
- De Stefano, G.; Litewczuk, D.; Mollica, C.; Di Pietro, G.; Galosi, E.; Leone, C.; Falco, P.; Tullo, M.G.; Caramia, F.; Truini, A.; et al. Sex Differences in Trigeminal Neuralgia: A Focus on Radiological and Clinical Characteristics. Neurol. Sci. 2023, 44, 4465–4472. [Google Scholar] [CrossRef] [PubMed]
- Cruccu, G.; Finnerup, N.B.; Jensen, T.S.; Scholz, J.; Sindou, M.; Svensson, P.; Treede, R.-D.; Zakrzewska, J.M.; Nurmikko, T. Trigeminal Neuralgia: New Classification and Diagnostic Grading for Practice and Research. Neurology 2016, 87, 220–228. [Google Scholar] [CrossRef]
- Maarbjerg, S.; Gozalov, A.; Olesen, J.; Bendtsen, L. Trigeminal Neuralgia—A Prospective Systematic Study of Clinical Characteristics in 158 Patients. Headache 2014, 54, 1574–1582. [Google Scholar] [CrossRef]
- Brisman, R. Typical versus Atypical Trigeminal Neuralgia and Other Factors That May Affect Results of Neurosurgical Treatment. World Neurosurg. 2013, 79, 649–650. [Google Scholar] [CrossRef]
- Burchiel, K.J.; Slavin, K.V. On the Natural History of Trigeminal Neuralgia. Neurosurgery 2000, 46, 152–155. [Google Scholar] [CrossRef]
- Sindou, M.; Leston, J.; Howeidy, T.; Decullier, E.; Chapuis, F. Micro-Vascular Decompression for Primary Trigeminal Neuralgia (Typical or Atypical). Long-Term Effectiveness on Pain; Prospective Study with Survival Analysis in a Consecutive Series of 362 Patients. Acta Neurochir. 2006, 148, 1235–1245; discussion 1245. [Google Scholar] [CrossRef]
- Zhang, H.; Lei, D.; You, C.; Mao, B.-Y.; Wu, B.; Fang, Y. The Long-Term Outcome Predictors of Pure Microvascular Decompression for Primary Trigeminal Neuralgia. World Neurosurg. 2013, 79, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Sandell, T.; Eide, P.K. Effect of Microvascular Decompression in Trigeminal Neuralgia Patients with or without Constant Pain. Neurosurgery 2008, 63, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Obermann, M.; Yoon, M.-S.; Ese, D.; Maschke, M.; Kaube, H.; Diener, H.-C.; Katsarava, Z. Impaired Trigeminal Nociceptive Processing in Patients with Trigeminal Neuralgia. Neurology 2007, 69, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Burchiel, K.J. A New Classification for Facial Pain. Neurosurgery 2003, 53, 1164–1167. [Google Scholar] [CrossRef] [PubMed]
- Maarbjerg, S.; Gozalov, A.; Olesen, J.; Bendtsen, L. Concomitant Persistent Pain in Classical Trigeminal Neuralgia--Evidence for Different Subtypes. Headache 2014, 54, 1173–1183. [Google Scholar] [CrossRef]
- Di Stefano, G.; De Stefano, G.; Leone, C.; Cruccu, G.; Tardioli, S.; Cartocci, G.; Fiorelli, M.; Truini, A.; Caramia, F. Concomitant Continuous Pain in Patients with Trigeminal Neuralgia Is Associated with Trigeminal Nerve Root Atrophy. Cephalalgia 2020, 40, 1502–1510. [Google Scholar] [CrossRef]
- Ngeow, W.C.; Nair, R. Injection of Botulinum Toxin Type A (BOTOX) into Trigger Zone of Trigeminal Neuralgia as a Means to Control Pain. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e47–e50. [Google Scholar] [CrossRef]
- Lunde, H.M.B.; Torkildsen, Ø.; Bø, L.; Bertelsen, A.K. Botulinum Toxin as Monotherapy in Symptomatic Trigeminal Neuralgia. Headache 2016, 56, 1035–1039. [Google Scholar] [CrossRef]
- Caldera, M.C.; Senanayake, S.J.; Perera, S.P.; Perera, N.N.; Gamage, R.; Gooneratne, I.K. Efficacy of Botulinum Toxin Type A in Trigeminal Neuralgia in a South Asian Cohort. J. Neurosci. Rural Pract. 2018, 9, 100–105. [Google Scholar] [CrossRef]
- Crespi, J.; Bratbak, D.; Dodick, D.W.; Matharu, M.; Jamtøy, K.A.; Tronvik, E. Pilot Study of Injection of OnabotulinumtoxinA Toward the Sphenopalatine Ganglion for the Treatment of Classical Trigeminal Neuralgia. Headache 2019, 59, 1229–1239. [Google Scholar] [CrossRef]
- Asan, F.; Gündüz, A.; Tütüncü, M.; Uygunoğlu, U.; Savrun, F.K.; Saip, S.; Siva, A. Treatment of Multiple Sclerosis-Related Trigeminal Neuralgia with OnabotulinumtoxinA. Headache 2022, 62, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Yiangou, Y.; Anand, U.; Otto, W.R.; Sinisi, M.; Fox, M.; Birch, R.; Foster, K.A.; Mukerji, G.; Akbar, A.; Agarwal, S.K.; et al. Increased Levels of SV2A Botulinum Neurotoxin Receptor in Clinical Sensory Disorders and Functional Effects of Botulinum Toxins A and E in Cultured Human Sensory Neurons. J. Pain Res. 2011, 4, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Lacković, Z.; Filipović, B.; Matak, I.; Helyes, Z. Activity of Botulinum Toxin Type A in Cranial Dura: Implications for Treatment of Migraine and Other Headaches. Br. J. Pharmacol. 2016, 173, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, S.; Vacca, V.; Ricordy, R.; Uggenti, C.; Tata, A.M.; Luvisetto, S.; Pavone, F. The Analgesic Effect on Neuropathic Pain of Retrogradely Transported Botulinum Neurotoxin A Involves Schwann Cells and Astrocytes. PLoS ONE 2012, 7, e47977. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, R.; Lam, C.; Yaksh, T.L. Botulinum Toxin in Migraine: Role of Transport in Trigemino-Somatic and Trigemino-Vascular Afferents. Neurobiol. Dis. 2015, 79, 111–122. [Google Scholar] [CrossRef]
- Morenilla-Palao, C.; Planells-Cases, R.; García-Sanz, N.; Ferrer-Montiel, A. Regulated Exocytosis Contributes to Protein Kinase C Potentiation of Vanilloid Receptor Activity. J. Biol. Chem. 2004, 279, 25665–25672. [Google Scholar] [CrossRef]
- McMahon, H.T.; Foran, P.; Dolly, J.O.; Verhage, M.; Wiegant, V.M.; Nicholls, D.G. Tetanus Toxin and Botulinum Toxins Type A and B Inhibit Glutamate, Gamma-Aminobutyric Acid, Aspartate, and Met-Enkephalin Release from Synaptosomes. Clues to the Locus of Action. J. Biol. Chem. 1992, 267, 21338–21343. [Google Scholar] [CrossRef]
- Nakov, R.; Habermann, E.; Hertting, G.; Wurster, S.; Allgaier, C. Effects of Botulinum A Toxin on Presynaptic Modulation of Evoked Transmitter Release. Eur. J. Pharmacol. 1989, 164, 45–53. [Google Scholar] [CrossRef]
- Durham, P.L.; Cady, R.; Cady, R. Regulation of Calcitonin Gene-Related Peptide Secretion from Trigeminal Nerve Cells by Botulinum Toxin Type A: Implications for Migraine Therapy. Headache 2004, 44, 33–35. [Google Scholar] [CrossRef]
- Purkiss, J.; Welch, M.; Doward, S.; Foster, K. Capsaicin-Stimulated Release of Substance P from Cultured Dorsal Root Ganglion Neurons: Involvement of Two Distinct Mechanisms. Biochem. Pharmacol. 2000, 59, 1403–1406. [Google Scholar] [CrossRef]
- Sandhu, S.K.; Lee, J.Y.K. Measurement of Trigeminal Neuralgia Pain: Penn Facial Pain Scale. Neurosurg. Clin. N. Am. 2016, 27, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Scott, W.; McCracken, L.M. Patients’ Impression of Change Following Treatment for Chronic Pain: Global, Specific, a Single Dimension, or Many? J. pain 2015, 16, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Delgado, D.A.; Lambert, B.S.; Boutris, N.; McCulloch, P.C.; Robbins, A.B.; Moreno, M.R.; Harris, J.D. Validation of Digital Visual Analog Scale Pain Scoring With a Traditional Paper-Based Visual Analog Scale in Adults. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e088. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | TN | Type 1 TN (Mean ± SD or N°, /%) | Type 2 TN (Mean ± SD or N°, /%) | p-Value |
|---|---|---|---|---|
| Number of patients | 40 | 18 | 22 | |
| Age | 63.4 ± 18.4 | 59.9 ± 20.1 | 66.2 ± 16.9 | 0.282 |
| Female sex | 27/40 (67.5%) | 13/18 (72.2%) | 14/22 (63.6%) | 0.564 |
| TN duration (years) | 5.8 ± 4.6 | 4.2 ± 3.9 | 7.0 ± 4.8 | 0.027 |
| Previous oral prophylaxis | 1.3 ± 1.2 | 0.9 ± 1.0 | 1.6 ± 1.1 | 0.051 |
| TN characteristics | ||||
| Left side involved | 19/40 (47.5%) | 9/18 (50.0%) | 10/22 (45.5%) | 0.775 |
| Idiopathic TN | 22/40 (55.0%) | 11/18 (61.1%) | 11/22 (50.0%) | 0.482 |
| Classical TN | 18/40 (45.0%) | 7/18 (38.9%) | 11/22 (50.0%) | 0.537 |
| Only V1 involved | 4/40 (10.0%) | 0/18 (0%) | 4/22 (18.2%) | 0.114 |
| Only V2 involved | 10/40 (25.0%) | 6/18 (33.3%) | 4/22 (18.2%) | 0.300 |
| Only V3 involved | 8/40 (20.0%) | 3/18 (16.7%) | 5/22 (22.7%) | 0.709 |
| V1 + V2 involved | 6/40 (15.0%) | 4/18 (22.2%) | 2/22 (9.1%) | 0.381 |
| V2 + V3 involved | 12/40 (30.0%) | 5/18 (27.8%) | 7/22 (31.8%) | 0.781 |
| BoNT/A dose | 29.5 ± 11.1 | 29.7 ± 11.4 | 29.3 ± 11.0 | 0.967 |
| T0 | T1 | T2 | p (Post Hoc Comparison) | |
|---|---|---|---|---|
| All TN Patients | ||||
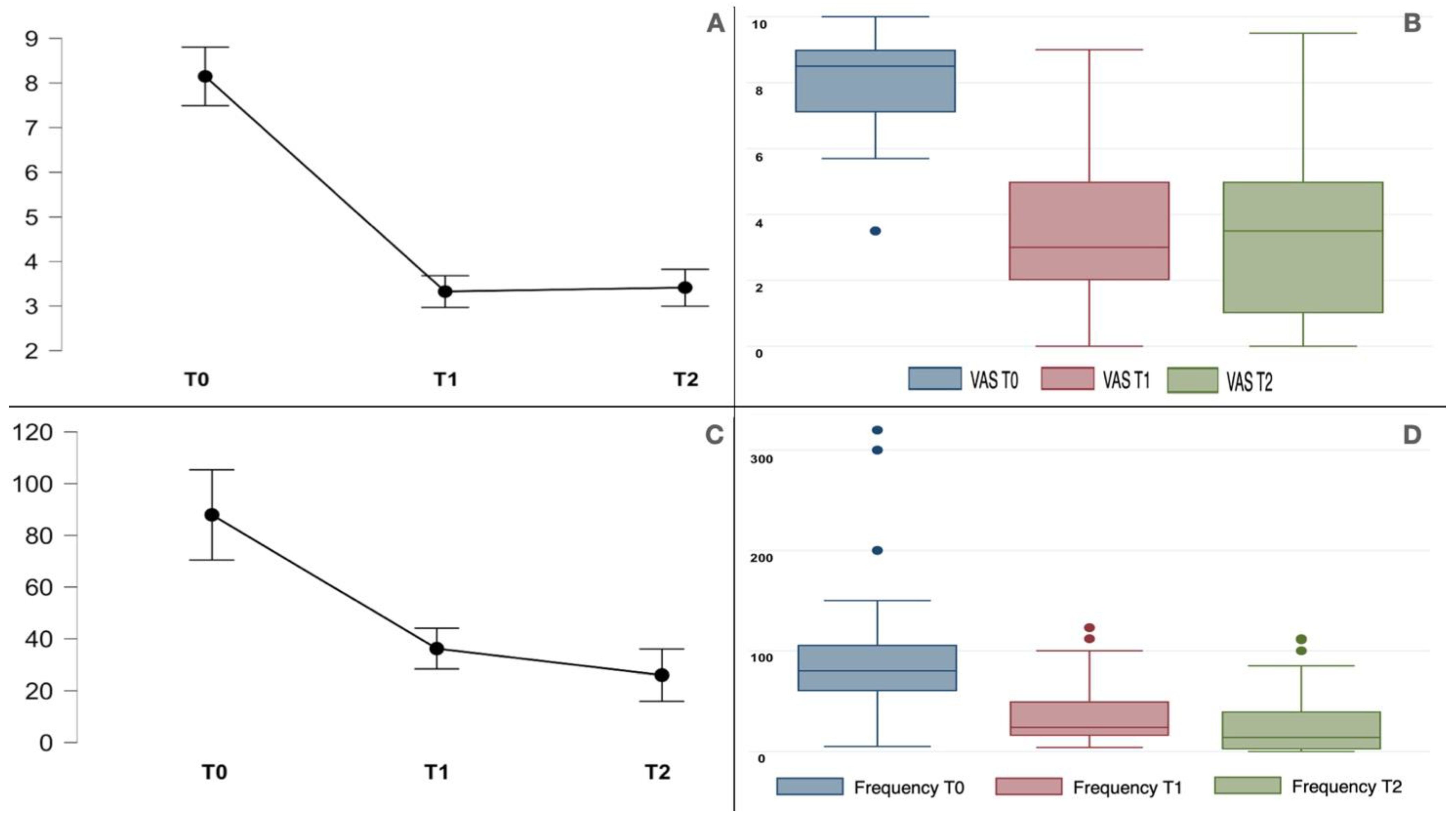
| Pain (VAS) | 8.1 ± 1.4 | 3.3 ± 2.3 | 3.4 ± 2.4 | *, ** < 0.001 *** NS |
| Frequency | 87.9 ± 64.6 | 36.2 ± 29.5 | 26.0 ± 31.9 | *, ** < 0.001 *** NS |
| Type 1 TN group | ||||
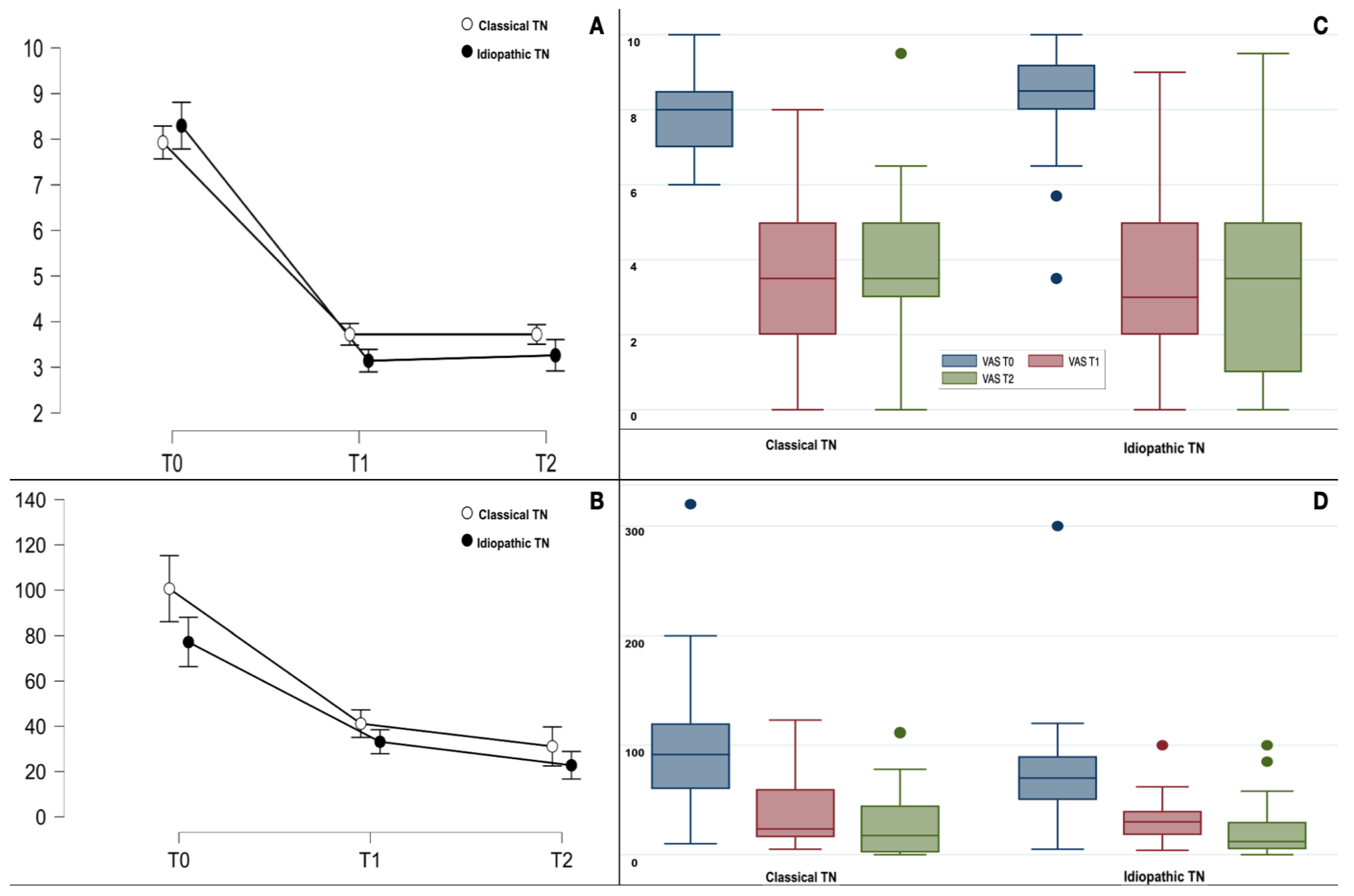
| Pain (VAS) | 7.8 ± 1.6 | 3.1 ± 2.3 | 3.2 ± 2.5 | *, ** < 0.001 *** NS |
| Frequency | 86.7 ± 69.3 | 35.2 ± 32.3 | 26.0 ± 34.4 | * 0.002 ** < 0.001 *** NS |
| Type 2 TN group | ||||
| Pain (VAS) | 8.4 ± 1.1 | 3.5 ± 2.3 | 3.6 ± 2.5 | *, ** < 0.001 *** NS |
| Frequency | 88.9 ± 62.2 | 36.9 ± 27.8 | 26.0 ± 30.7 | *, ** < 0.001 *** NS |
| Background pain (VAS) | 5.9 ± 1.9 | 2.1 ± 1.9 | <0.001 |
| T0 Type 1 TN | T1 Type 1 TN | p | T0 Type 2 TN | T1 Type 2 TN | p | T0 TN | T1 TN | p | |
|---|---|---|---|---|---|---|---|---|---|
| General activity | 7.5 ± 2.3 | 2.7 ± 3.0 | <0.001 | 7.8 ± 2.0 | 3.0 ± 2.7 | <0.001 | 7.7 ± 2.1 | 2.9 ± 2.8 | <0.001 |
| Mood | 7.6 ± 2.6 | 2.7 ± 2.9 | <0.001 | 8.4 ± 2.3 | 3.0 ± 3.0 | <0.001 | 8.0 ± 2.5 | 2.9 ± 2.9 | <0.001 |
| Walking | 2.9 ± 3.9 | 0.6 ± 1.9 | 0.033 | 2.5 ± 3.8 | 0.8 ± 2.2 | 0.022 | 2.7 ± 3.8 | 0.7 ± 2.1 | 0.002 |
| Work | 5.6 ± 3.1 | 2.3 ± 2.7 | 0.002 | 6.2 ± 3.3 | 2.3 ± 2.7 | <0.001 | 5.9 ± 3.2 | 2.3 ± 2.7 | <0.001 |
| Relationship | 6.6 ± 2.6 | 2.1 ± 2.6 | <0.001 | 7.0 ± 2.8 | 3.1 ± 2.6 | <0.001 | 6.8 ± 2.7 | 2.7 ± 2.6 | <0.001 |
| Sleep | 4.8 ± 3.3 | 2.1 ± 2.8 | 0.004 | 5.5 ± 3.9 | 1.5 ± 2.4 | <0.001 | 5.2 ± 3.6 | 1.8 ± 2.5 | <0.001 |
| Enjoyment of life | 7.4 ± 2.3 | 2.9 ± 3.1 | <0.001 | 8.2 ± 1.4 | 3.3 ± 2.3 | <0.001 | 7.9 ± 1.8 | 3.1 ± 2.7 | <0.001 |
| Eat | 6.0 ± 3.0 | 2.4 ± 2.9 | 0.002 | 6.9 ± 3.7 | 3.0 ± 3.0 | <0.001 | 6.5 ± 3.4 | 2.8 ± 3.0 | <0.001 |
| Touch your face | 5.9 ± 3.4 | 3.7 ± 3.0 | <0.001 | 7.6 ± 3.1 | 3.1 ± 3.2 | <0.001 | 6.9 ± 3.3 | 3.4 ± 3.1 | <0.001 |
| Brush your teeth | 5.6 ± 3.5 | 3.1 ± 3.1 | 0.002 | 6.5 ± 4.0 | 3.5 ± 3.2 | 0.001 | 6.1 ± 3.7 | 3.3 ± 3.1 | <0.001 |
| Smile or laugh | 5.2 ± 3.6 | 2.7 ± 2.9 | 0.003 | 5.1 ± 4.0 | 2.6 ± 3.1 | 0.002 | 5.1 ± 3.8 | 2.7 ± 3.0 | <0.001 |
| Talk | 5.6 ± 3.8 | 1.8 ± 2.3 | <0.001 | 6.1 ± 3.8 | 3.5 ± 2.9 | <0.001 | 5.9 ± 3.8 | 2.8 ± 2.7 | <0.001 |
| Open your mouth wide | 5.7 ± 3.5 | 2.6 ± 2.4 | <0.001 | 5.3 ± 4.0 | 2.6 ± 3.2 | 0.002 | 5.5 ± 3.8 | 2.6 ± 2.8 | <0.001 |
| Eat hard food | 7.5 ± 2.6 | 4.2 ± 3.8 | 0.004 | 8.4 ± 2.4 | 5.0 ± 3.1 | <0.001 | 8.0 ± 2.5 | 4.6 ± 3.4 | <0.001 |
| Worst NRS | 9.3 ± 1.7 | 4.7 ± 3.4 | 0.001 | 9.6 ± 1.0 | 5.2 ± 2.7 | <0.001 | 9.5 ± 1.4 | 5.0 ± 3.0 | <0.001 |
| Least NRS | 5.3 ± 2.2 | 2.1 ± 1.9 | <0.001 | 6.0 ± 2.1 | 2.3 ± 2.1 | <0.001 | 5.7 ± 2.2 | 2.2 ± 2.0 | <0.001 |
| Mean NRS | 7.4 ± 1.5 | 3.1 ± 2.3 | <0.001 | 7.9 ± 1.4 | 3.5 ± 2.3 | <0.001 | 7.7 ± 15 | 3.3 ± 2.3 | <0.001 |
| Pain now | 4.4 ± 3.6 | 1.0 ± 2.2 | 0.006 | 5.5 ± 2.7 | 1.7 ± 2.5 | <0.001 | 5.0 ± 3.1 | 1.4 ± 2.4 | <0.001 |
| PFPS Total score | 110.3 ± 30.0 | 46.4 ± 37.5 | <0.001 | 120.3 ± 29.5 | 53.1 ± 39.6 | <0.001 | 115.8 ± 29.8 | 50.1 ± 38.3 | <0.001 |
| T0 Type 1 TN | T0 Type 2 TN | p | T1 Type 1 TN | T1 Type 2 TN | p | Mean Reduction Type 1 TN | Mean Reduction Type 2 TN | p | |
|---|---|---|---|---|---|---|---|---|---|
| PFPS total | 110.3 ± 30.0 | 120.3 ± 29.5 | 0.293 | 46.4 ± 37.5 | 53.1 ± 39.6 | 0.549 | 63.3 ± 38.9 | 67.3 ± 32.1 | 0.764 |
| General activity | 7.5 ± 2.3 | 7.8 ± 2.0 | 0.646 | 2.7 ± 3.0 | 3.0 ± 2.7 | 0.598 | 4.8 ± 3.3 | 4.8 ± 2.4 | 0.987 |
| Mood | 7.6 ± 2.7 | 8.4 ± 2.3 | 0.241 | 2.7 ± 2.9 | 3.0 ± 3.0 | 0.812 | 4.9 ± 3.5 | 5.3 ± 3.0 | 0.680 |
| Walking | 2.9 ± 3.9 | 2.5 ± 3.8 | 0.913 | 0.6 ± 1.9 | 0.8 ± 2.2 | 0.795 | 2.4 ± 3.8 | 1.7 ± 3.3 | 0.987 |
| Work | 5.6 ± 3.1 | 6.2 ± 3.3 | 0.492 | 2.3 ± 2.7 | 2.3 ± 2.7 | 0.988 | 3.3 ± 2.8 | 3.9 ± 3.1 | 0.552 |
| Relationship | 6.6 ± 2.6 | 7.0 ± 2.8 | 0.475 | 2.1 ± 2.6 | 3.1 ± 2.6 | 0.193 | 4.5 ± 3.2 | 3.9 ± 2.8 | 0.509 |
| Sleep | 4.8 ± 3.3 | 5.5 ± 3.9 | 0.400 | 2.1 ± 2.8 | 1.5 ± 2.4 | 0.581 | 2.7 ± 2.8 | 4.0 ± 3.4 | 0.243 |
| Enjoyment of life | 7.4 ± 2.3 | 8.2 ± 1.4 | 0.318 | 2.9 ± 3.1 | 3.3 ± 2.3 | 0.391 | 4.6 ± 3.1 | 5.0 ± 2.1 | 0.631 |
| Eat | 6.0 ± 3.0 | 6.9 ± 3.7 | 0.176 | 2.4 ± 3.0 | 3.04 ± 3.0 | 0.505 | 3.6 ± 3.1 | 3.9 ± 3.2 | 0.825 |
| Touch your face | 5.9 ± 3.4 | 7.6 ± 3.1 | 0.034 | 3.7 ± 3.1 | 3.1 ± 3.2 | 0.585 | 1.9 ± 4.6 | 3.4 ± 4.5 | 0.315 |
| Brush your teeth | 5.6 ± 3.5 | 6.5 ± 4.0 | 0.281 | 3.1 ± 3.1 | 3.5 ± 3.2 | 0.779 | 2.6 ± 2.6 | 3.1 ± 3.2 | 0.626 |
| Smile or laugh | 5.2 ± 3.6 | 5.1 ± 4.0 | 0.945 | 2.7 ± 2.9 | 2.6 ± 3.1 | 0.830 | 2.5 ± 3.1 | 2.5 ± 3.0 | 0.944 |
| Talk | 5.6 ± 3.8 | 6.1 ± 3.8 | 0.572 | 1.8 ± 2.3 | 3.5 ± 2.9 | 0.058 | 3.7 ± 3.7 | 2.6 ± 3.0 | 0.294 |
| Open your mouth wide | 5.7 ± 3.5 | 5.3 ± 4.1 | 0.858 | 2.6 ± 2.4 | 2.6 ± 3.2 | 0.712 | 3.2 ± 3.0 | 2.7 ± 3.0 | 0.538 |
| Eat hard food | 7.5 ± 2.6 | 8.4 ± 2.4 | 0.142 | 4.2 ± 3.8 | 5.0 ± 3.1 | 0.573 | 3.3 ± 3.4 | 3.4 ± 2.3 | 0.601 |
| Worst NRS | 9.3 ± 1.7 | 9.6 ± 1.0 | 0.985 | 4.7 ± 3.4 | 5.2 ± 2.7 | 0.650 | 4.7 ± 3.8 | 4.4 ± 2.8 | 0.956 |
| Least NRS | 5.3 ± 2.2 | 6.0 ± 2.1 | 0.297 | 2.1 ± 1.9 | 2.3 ± 2.1 | 0.835 | 3.2 ± 2.8 | 3.7 ± 2.8 | 0.271 |
| Mean NRS | 7.4 ± 1.5 | 7.9 ± 1.4 | 0.293 | 3.1 ± 2.3 | 3.5 ± 2.3 | 0.600 | 4.3 ± 2.7 | 4.3 ± 2.4 | 0.985 |
| Pain now | 4.4 ± 3.6 | 5.5 ± 2.7 | 0.358 | 1.0 ± 2.2 | 1.7 ± 2.5 | 0.185 | 3.4 ± 3.5 | 3.8 ± 2.4 | 0.450 |
| PGIC 1/7 | PGIC 2/7 | PGIC 3/7 | PGIC 4/7 | PGIC 5/7 | PGIC 6/7 | PGIC 7/7 | |
|---|---|---|---|---|---|---|---|
| Type 1 TN | 0 | 0 | 2 | 0 | 1 | 11 | 4 |
| Type 2 TN | 0 | 0 | 2 | 1 | 2 | 15 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tereshko, Y.; Valente, M.; Belgrado, E.; Dalla Torre, C.; Dal Bello, S.; Merlino, G.; Gigli, G.L.; Lettieri, C. The Therapeutic Effect of Botulinum Toxin Type A on Trigeminal Neuralgia: Are There Any Differences between Type 1 versus Type 2 Trigeminal Neuralgia? Toxins 2023, 15, 654. https://doi.org/10.3390/toxins15110654
Tereshko Y, Valente M, Belgrado E, Dalla Torre C, Dal Bello S, Merlino G, Gigli GL, Lettieri C. The Therapeutic Effect of Botulinum Toxin Type A on Trigeminal Neuralgia: Are There Any Differences between Type 1 versus Type 2 Trigeminal Neuralgia? Toxins. 2023; 15(11):654. https://doi.org/10.3390/toxins15110654
Chicago/Turabian StyleTereshko, Yan, Mariarosaria Valente, Enrico Belgrado, Chiara Dalla Torre, Simone Dal Bello, Giovanni Merlino, Gian Luigi Gigli, and Christian Lettieri. 2023. "The Therapeutic Effect of Botulinum Toxin Type A on Trigeminal Neuralgia: Are There Any Differences between Type 1 versus Type 2 Trigeminal Neuralgia?" Toxins 15, no. 11: 654. https://doi.org/10.3390/toxins15110654