Neutralizing Antibody Formation with OnabotulinumtoxinA (BOTOX®) Treatment from Global Registration Studies across Multiple Indications: A Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Frequency of NAb Formation
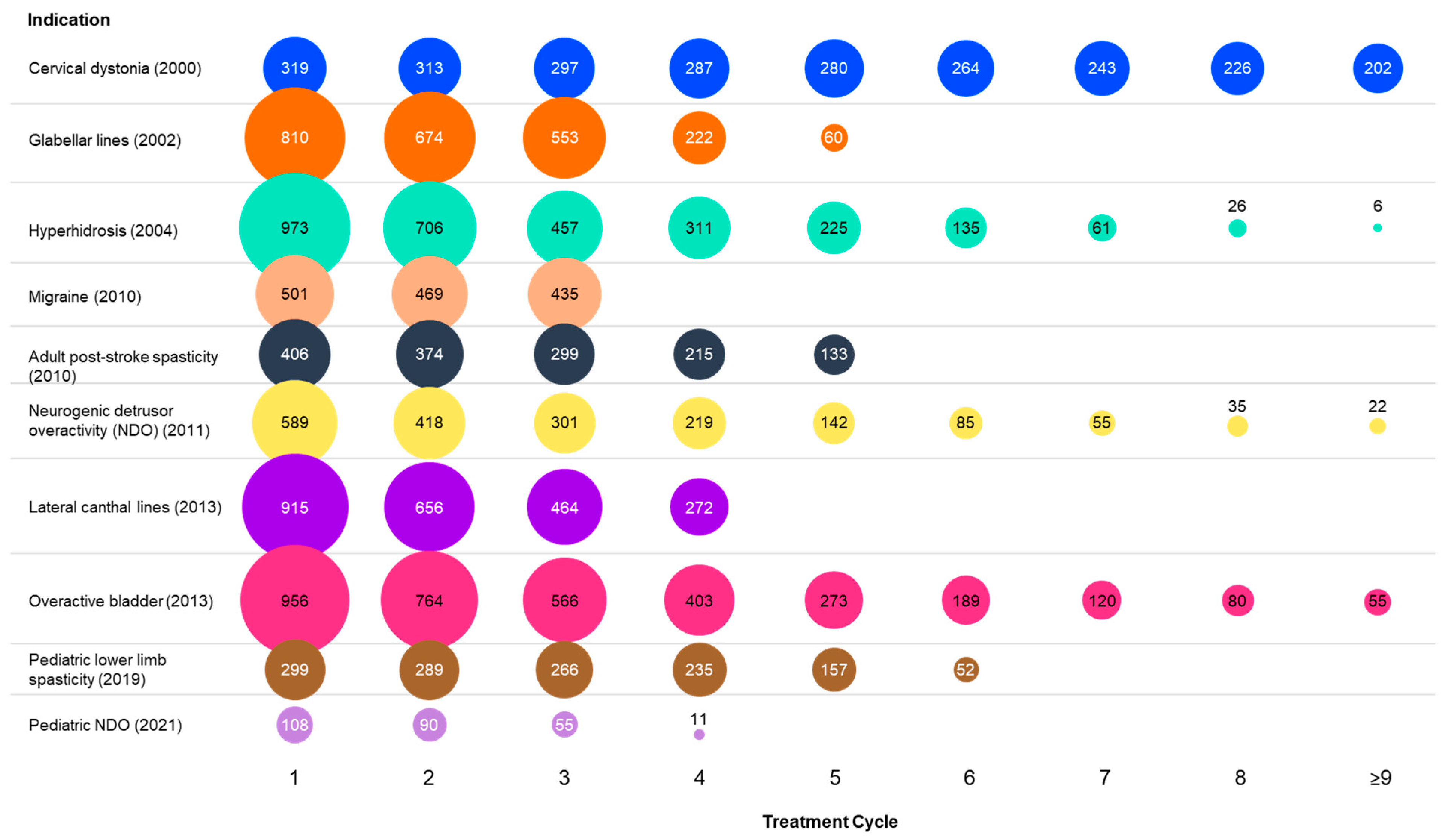
2.2. Effect of Dose Level, Dosing Interval, and Number of Treatment Cycles on Immunogenicity
2.3. Effect of NAb Formation on Efficacy
2.4. Effect of NAb Formation on Safety
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Designs and Subjects
5.2. NAb Evaluations
- All samples with NAb results (positive, negative, or inconclusive) were used to determine subjects’ NAb status;
- Subjects with a negative or inconclusive baseline were considered not to have NAb formation if all post-dose serum samples were negative or inconclusive (A), but were considered to have NAb formation if any post-dose sample was positive (B);
- Subjects with no baseline assessment were considered not to have NAb formation if all post-dose samples were negative or inconclusive (C), but were considered to have NAb formation if any post-dose sample was positive (D);
- Subjects were not included in the current analysis if they had positive baselines (E);
- Subjects were not included in the current analysis if they had no post-dose NAb results (F).
5.3. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Botox (OnabotulinumtoxinA) [Package Insert]; Allergan: Madison, NJ, USA, 2021.
- Schiavo, G.; Matteoli, M.; Montecucco, C. Neurotoxins affecting neuroexocytosis. Physiol. Rev. 2000, 80, 717–766. [Google Scholar] [CrossRef] [PubMed]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum neurotoxins: Biology, pharmacology, and toxicology. Pharmacol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef] [PubMed]
- Naumann, M.; Carruthers, A.; Carruthers, J.; Aurora, S.K.; Zafonte, R.; Abu-Shakra, S.; Boodhoo, T.; Miller-Messana, M.A.; Demos, G.; James, L.; et al. Meta-analysis of neutralizing antibody conversion with onabotulinumtoxinA (BOTOX®) across multiple indications. Mov. Disord. 2010, 25, 2211–2218. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Blumenfeld, A.M.; Silberstein, S.D.; Adams, A.M.; Brin, M.F. Mechanism of action of onabotulinumtoxinA in chronic migraine: A narrative review. Headache 2020, 60, 1259–1272. [Google Scholar] [CrossRef] [PubMed]
- Bellows, S.; Jankovic, J. Immunogenicity associated with botulinum toxin treatment. Toxins 2019, 11, 491. [Google Scholar] [CrossRef]
- Jinnah, H.A.; Goodmann, E.; Rosen, A.R.; Evatt, M.; Freeman, A.; Factor, S. Botulinum toxin treatment failures in cervical dystonia: Causes, management, and outcomes. J. Neurol. 2016, 263, 1188–1194. [Google Scholar] [CrossRef]
- Albrecht, P.; Jansen, A.; Lee, J.-I.; Moll, M.; Ringelstein, M.; Rosenthal, D.; Bigalke, H.; Aktas, O.; Hartung, H.-P.; Hefter, H. High prevalence of neutralizing antibodies after long-term botulinum neurotoxin therapy. Neurology 2019, 92, e48–e54. [Google Scholar] [CrossRef]
- Walter, U.; Mühlenhoff, C.; Benecke, R.; Dressler, D.; Mix, E.; Alt, J.; Wittstock, M.; Dudesek, A.; Storch, A.; Kamm, C. Frequency and risk factors of antibody-induced secondary failure of botulinum neurotoxin therapy. Neurology 2020, 94, e2109–e2120. [Google Scholar] [CrossRef]
- Brin, M.F.; Comella, C.L.; Jankovic, J.; Mmath, F.L.; Naumann, M. Long-term treatment with botulinum toxin type A in cervical dystonia has low immunogenicity by mouse protection assay. Mov. Disord. 2008, 23, 1353–1360. [Google Scholar] [CrossRef]
- Bellows, S.; Jankovic, J. Reply to comment on re-visiting immunogenicity associated with botulinum toxin treatment. Toxins 2019, 11, 491. Toxins 2020, 12, 72. [Google Scholar] [CrossRef]
- Carruthers, J.A.; Lowe, N.J.; Menter, M.A.; Gibson, J.; Nordquist, M.; Mordaunt, J.; Walker, P.; Eadie, N. MBAd BOTOX Glabellar Lines I Study Group. A multicenter, double-blind, randomized, placebo-controlled study of the efficacy and safety of botulinum toxin type A in the treatment of glabellar lines. J. Am. Acad. Dermatol. 2002, 46, 840–849. [Google Scholar] [CrossRef]
- Carruthers, A.; Carruthers, J.; Lowe, N.J.; Menter, A.; Gibson, J.; Nordquist, M.; Mordaunt, J. One-year, randomised, multicenter, two-period study of the safety and efficacy of repeated treatments with botulinum toxin type A in patients with glabellar lines. J. Clin. Res. 2004, 7, 1–20. [Google Scholar]
- Carruthers, J.D.; Lowe, N.J.; Menter, M.A.; Gibson, J.; Eadie, N. Double-blind, placebo-controlled study of the safety and efficacy of botulinum toxin type A for patients with glabellar lines. Plast. Reconstr. Surg. 2003, 112, 21S–30S. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, M.; Harii, K. An open-label, randomized, 64-week study repeating 10- and 20-U doses of botulinum toxin type A for treatment of glabellar lines in Japanese subjects. Int. J. Dermatol. 2009, 48, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Lowe, N.J.; Glaser, D.A.; Eadie, N.; Daggett, S.; Kowalski, J.W.; Lai, P.-Y. Botulinum toxin type A in the treatment of primary axillary hyperhidrosis: A 52-week multicenter double-blind, randomized, placebo-controlled study of efficacy and safety. J. Am. Acad. Dermatol. 2007, 56, 604–611. [Google Scholar] [CrossRef]
- Glaser, D.A.; Loss, R.; Beddingfield, F.; Coleman, W. Four-year longitudinal data on the efficacy and safety of repeated botulinum toxin type A therapy for primary axillary hyperhidrosis [abstract]. J. Am. Acad. Dermatol. 2007, 56 (Suppl. S2), AB61. [Google Scholar]
- Glaser, D.A.; Pariser, D.M.; Hebert, A.A.; Landells, I.; Somogyi, C.; Weng, E.; Brin, M.F.; Beddingfield, F. A prospective, nonrandomized, open-label study of the efficacy and safety of onabotulinumtoxinA in adolescents with primary axillary hyperhidrosis. Pediatr. Dermatol. 2015, 32, 609–617. [Google Scholar] [CrossRef]
- Naumann, M.; Lowe, N.J. Botulinum toxin type A in treatment of bilateral primary axillary hyperhidrosis: Randomised, parallel group, double blind, placebo controlled trial. BMJ 2001, 323, 596. [Google Scholar] [CrossRef]
- Naumann, M.; Lowe, N.J.; Kumar, C.R.; Hamm, H. Botulinum toxin type a is a safe and effective treatment for axillary hyperhidrosis over 16 months: A prospective study. Arch. Dermatol. 2003, 139, 731–736. [Google Scholar] [CrossRef]
- Pariser, D.; Kowalski, J.; Ravelo, A.; Ill, D. Work productivity impairment in patients with severe primary axillary hyperhidrosis: Initial results from the work limitations questionnaire [poster]. In Proceedings of the Annual Meeting of the American Academy of Dermatology, New Orleans, LA, USA, 18–22 February 2005. [Google Scholar]
- Mathew, N.T.; Frishberg, B.M.; Gawel, M.; Dimitrova, R.; Gibson, J.; Turkel, C. Botulinum toxin type A (BOTOX) for the prophylactic treatment of chronic daily headache: A randomized, double-blind, placebo-controlled trial. Headache 2005, 45, 293–307. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Stark, S.R.; Lucas, S.M.; Christie, S.N.; Degryse, R.E.; Turkel, C.C. Botulinum toxin type A for the prophylactic treatment of chronic daily headache: A randomized, double-blind, placebo-controlled trial. Mayo Clin. Proc. 2005, 80, 1126–1137. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Gawel, M.; Brandes, J.L.; Pokta, S.; VanDenburgh, A.M.; for the BOTOX North American Episodic Migraine Study Group. Botulinum toxin type A prophylactic treatment of episodic migraine: A randomized, double-blind, placebo-controlled exploratory study. Headache 2007, 47, 486–499. [Google Scholar] [CrossRef] [PubMed]
- Brashear, A.; Gordon, M.F.; Elovic, E.; Kassicieh, V.D.; Marciniak, C.; Do, M.; Lee, C.-H.; Jenkins, S.; Turkel, C. Intramuscular injection of botulinum toxin for the treatment of wrist and finger spasticity after a stroke. N. Engl. J. Med. 2002, 347, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.F.; Brashear, A.; Elovic, E.; Kassicieh, D.; Marciniak, C.; Liu, J.; Turkel, C.; BOTOX Poststroke Spasticity Study Group. Repeated dosing of botulinum toxin type A for upper limb spasticity following stroke. Neurology 2004, 63, 1971–1973. [Google Scholar] [CrossRef]
- Turkel, C.; Dru, R.; Liu, J. Double-blind, randomized, dose-ranging study of BOTOX purified neurotoxin complex for treating focal spasticity post-stroke [abstract 155]. Naunyn. Shmiedebergs Arch. Pharmacol. 2002, 365 (Suppl. S2), R47. [Google Scholar]
- Elovic, E.P.; Brashear, A.; Kaelin, D.; Liu, J.; Millis, S.R.; Barron, R.; Turkel, C. Repeated treatments with botulinum toxin type A produce sustained decreases in the limitations associated with focal upper-limb poststroke spasticity for caregivers and patients. Arch. Phys. Med. Rehabil. 2008, 89, 799–806. [Google Scholar] [CrossRef]
- Schurch, B.; de Sèze, M.; Denys, P.; Chartier-Kastler, E.; Haab, F.; Everaert, K.; Plante, P.; Perrouin-Verbe, B.; Kumar, C.; Fraczek, S.; et al. Botulinum toxin type a is a safe and effective treatment for neurogenic urinary incontinence: Results of a single treatment, randomized, placebo controlled 6-month study. J. Urol. 2005, 174, 196–200. [Google Scholar] [CrossRef]
- Ginsberg, D.; Cruz, F.; Herschorn, S.; Gousse, A.; Keppenne, V.; Aliotta, P.; Sievert, K.-D.; Brin, M.F.; Jenkins, B.; Thompson, C.; et al. OnabotulinumtoxinA is effective in patients with urinary incontinence due to neurogenic detrusor overactivity [corrected] regardless of concomitant anticholinergic use or neurologic etiology. Adv Ther. 2013, 30, 819–833. [Google Scholar] [CrossRef]
- Ginsberg, D.; Gousse, A.; Keppenne, V.; Sievert, K.-D.; Thompson, C.; Lam, W.; Brin, M.F.; Jenkins, B.; Haag-Molkenteller, C. Phase 3 efficacy and tolerability study of onabotulinumtoxinA for urinary incontinence from neurogenic detrusor overactivity. J. Urol. 2012, 187, 2131–2139. [Google Scholar] [CrossRef]
- Cruz, F.; Herschorn, S.; Aliotta, P.; Brin, M.; Thompson, C.; Lam, W.; Daniell, G.; Heesakkers, J.; Haag-Molkenteller, C. Efficacy and safety of onabotulinumtoxinA in patients with urinary incontinence due to neurogenic detrusor overactivity: A randomised, double-blind, placebo-controlled trial. Eur. Urol. 2011, 60, 742–750. [Google Scholar] [CrossRef]
- Kennelly, M.; Dmochowski, R.; Schulte-Baukloh, H.; Ethans, K.; Del Popolo, G.; Moore, C.; Jenkins, B.; Guard, S.; Zheng, Y.; Karsenty, G.; et al. Efficacy and safety of onabotulinumtoxinA therapy are sustained over 4 years of treatment in patients with neurogenic detrusor overactivity: Final results of a long-term extension study. Neurourol. Urodyn. 2015, 36, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, A.; Bruce, S.; De Coninck, A.; Connolly, S.; Cox, S.E.; Davis, P.G.; Campo, A.; Lei, X.; Somogyi, C.; Lee, E.; et al. Efficacy and safety of onabotulinumtoxinA for the treatment of crow’s feet lines: A multicenter, randomized, controlled trial. Dermatol. Surg. 2014, 40, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Moers-Carpi, M.; Carruthers, J.; Fagien, S.; Lupo, M.; Delmar, H.; Jones, D.; Somogyi, C.; Lee, E.; Lei, X.; MacKinnon, S.M.; et al. Efficacy and safety of onabotulinumtoxinA for treating crow’s feet lines alone or in combination with glabellar lines: A multicenter, randomized, controlled trial. Dermatol. Surg. 2015, 41, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, J.; Rivkin, A.; Donofrio, L.; Bertucci, V.; Somogyi, C.; Lei, X.; Davis, P.; Campo, A.; Beddingfield, F. A multicenter, randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of repeated onabotulinumtoxinA treatments in subjects with crow’s feet lines and glabellar lines. Dermatol. Surg. 2015, 41, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Chapple, C.; Sievert, K.-D.; MacDiarmid, S.; Khullar, V.; Radziszewski, P.; Nardo, C.; Thompson, C.; Zhou, J.; Haag-Molkenteller, C. OnabotulinumtoxinA 100 U significantly improves all idiopathic overactive bladder symptoms and quality of life in patients with overactive bladder and urinary incontinence: A randomised, double-blind, placebo-controlled trial. Eur. Urol. 2013, 64, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Nitti, V.W.; Dmochowski, R.; Herschorn, S.; Sand, P.; Thompson, C.; Nardo, C.; Yan, X.; Haag-Molkenteller, C.; EMBARK Study Group. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: Results of a phase 3, randomized, placebo controlled trial. J. Urol. 2013, 189, 2186–2193. [Google Scholar] [CrossRef]
- Nitti, V.W.; Ginsberg, D.; Sievert, K.D.; Sussman, D.; Radomski, S.; Sand, P.; De Ridder, D.; Jenkins, B.; Magyar, A.; Chapple, C. Durable efficacy and safety of long-term onabotulinumtoxinA treatment in patients with overactive bladder syndrome: Final results of a 3.5-year study. J. Urol. 2016, 196, 791–800. [Google Scholar] [CrossRef]
- Ginsberg, D.A.; Drake, M.J.; Kaufmann, A.; Radomski, S.; Gousse, A.E.; Chermansky, C.J.; Magyar, A.; Nicandro, J.P.; Nitti, V.; 191622-096 Investigators. Long-term treatment with onabotulinumtoxinA results in consistent, durable improvements in health related quality of life in patients with overactive bladder. J. Urol. 2017, 198, 897–904. [Google Scholar] [CrossRef]
- Dimitrova, R.; Kim, H.; Meilahn, J.; Chambers, H.G.; Racette, B.A.; Bonikowski, M.; Park, E.S.; McCusker, E.; Liu, C.; Brin, M.F. Efficacy and safety of onabotulinumtoxinA with standardized physiotherapy for the treatment of pediatric lower limb spasticity: A randomized, placebo-controlled, phase III clinical trial. Neurorehabilitation 2022, 50, 33–46. [Google Scholar] [CrossRef]
- Dimitrova, R.; McCusker, E.; Gormley, M.; Fehlings, D.; Alter, K.E.; Greaves, S.; Liu, C.; Brin, M.F. Efficacy and safety of onabotulinumtoxinA with standardized occupational therapy for treatment of pediatric upper limb spasticity: Phase III placebo-controlled randomized trial. Neurorehabilitation 2021, 49, 469–479. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Smith, M.B. interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef] [PubMed]
- Botox Cosmetic [Package Insert]; Allergan plc: Dublin, Ireland, 2020.
- Kessler, K.R.; Benecke, R. The EBD test—A clinical test for the detection of antibodies to botulinum toxin type A. Mov. Disord. 1997, 12, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Cordivari, C.; Misra, V.P.; Vincent, A.; Catania, S.; Bhatia, K.P.; Lees, A.J. Secondary nonresponsiveness to botulinum toxin A in cervical dystonia: The role of electromyogram-guided injections, botulinum toxin A antibody assay, and the extensor digitorum brevis test. Mov. Disord. 2006, 21, 1737–1741. [Google Scholar] [CrossRef] [PubMed]
- Hanna, P.A.; Jankovic, J.; Vincent, A. Comparison of mouse bioassay and immunoprecipitation assay for botulinum toxin antibodies. J. Neurol. Neurosurg. Psychiatry 1999, 66, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Schwartz, K. Response and immunoresistance to botulinum toxin injections. Neurology 1995, 45, 1743–1746. [Google Scholar] [CrossRef]
- Aimovig [package Insert]; Amgen Inc.: Thousand Oaks, CA, USA; Novartis Pharmaceuticals Corporation: East Hanover, NJ, USA, 2021.
- Ajovy [Package Insert]; Teva Pharmaceuticals USA, Inc.: North Wales, PA, USA, 2021.
- Emgality [Package Insert]; Eli Lilly and Company: Indianapolis, IN, USA, 2021.
- Dodick, D.W.; Turkel, C.C.; DeGryse, M.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.-C.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache, J. Head Face Pain 2010, 50, 921–936. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Stark, R.J.; Freeman, M.C.; Orejudos, A.; Adams, A.M. Long-term study of the efficacy and safety of onabotulinumtoxinA for the prevention of chronic migraine: COMPEL study. J. Headache Pain 2018, 19, 1–12. [Google Scholar] [CrossRef]
- Vyepti [Package Insert]; Lundbeck Seattle BioPharmaceuticals, Inc.: Bothell, WA, USA, 2021.
- Goessaert, A.-S.O.; Everaert, K.C. Onabotulinum toxin A for the treatment of neurogenic detrusor overactivity due to spinal cord injury or multiple sclerosis. Expert Rev. Neurother. 2012, 12, 763–775. [Google Scholar] [CrossRef]
- Cross, A.; Riley, C. Treatment of multiple sclerosis. Continuum (Minneap Minn). 2022, 28, 1025–1051. [Google Scholar] [CrossRef]
- Carr, W.W.; Jain, N.; Sublett, J.W. Immunogenicity of botulinum toxin formulations: Potential therapeutic implications. Adv. Ther. 2021, 38, 5046–5064. [Google Scholar] [CrossRef]
- Albrecht, P.; Jansen, A.; Lee, J.-I.; Ringelstein, M.; Aktas, O.; Hartung, H.-P.; Bigalke, H.; Hefter, H. Author response: High prevalence of neutralizing antibodies after long-term botulinum neurotoxin therapy. Neurology 2019, 93, 767–768. [Google Scholar] [PubMed]
- Xeomin [Package Insert]; Merz Pharmaceuticals: Raleigh, NC, USA, 2021.
- Greene, P.; Fahn, S.; Diamond, B. Development of resistance to botulinum toxin type A in patients with torticollis. Mov. Disord. 1994, 9, 213–217. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Inclusion Criteria Related to Prior BoNT Treatment | Design |
|---|---|---|
| Cervical dystonia | ||
| Brin 2008 [10] | BoNT naive | OL |
| Glabellar lines | ||
| Carruthers 2002 [12] | No requirement | DBPC |
| Carruthers 2004 [13] | No requirement | OL |
| Carruthers 2003 [14] | No requirement | DBPC |
| Kawashima 2009 [15] | BoNT naive | OL |
| Primary axillary hyperhidrosis | ||
| Lowe 2007 [4,16] | No BoNT for this condition previously | DBPC |
| Glaser 2007 [4,17] | Only in past BoNT study | OL |
| Glaser 2015 [18] | BoNT naive | OL |
| Naumann 2001 [19] | No BoNT ≤4 months | DBPC |
| Naumann 2003 [20] | No requirement | OL |
| Pariser 2005 [4,21] | BoNT naive | OL |
| Migraine | ||
| Mathew 2005 [22] | BoNT naive | DBPC |
| Silberstein 2005 [23] | BoNT naive | DBPC |
| Aurora 2007 [24] | BoNT naive | DBPC |
| Adult post-stroke spasticity | ||
| Brashear 2002 [25] | BoNT naive | DBPC |
| Gordon 2004 [26] | No requirement | OL |
| Turkel 2002 [4,27] | No BoNT ≤4 months | DBPC |
| Elovic 2008 [28] | No BoNT ≤4 months | OL |
| Neurogenic detrusor overactivity | ||
| Schurch 2005 [29] | No BoNT for urologic condition; no BoNT for any indication ≤3 months | DBPC |
| Cruz 2011, Ginsberg 2012, Ginsberg 2013 [30,31,32], a | No BoNT for urologic condition; no BoNT for any indication ≤3 months | DBPC |
| Kennelly 2017 [33], a | Only in past BoNT study | OL |
| Study 082P (data on file) | No BoNT for urologic condition; no BoNT for any indication ≤3 months | DBPC |
| Lateral canthal lines | ||
| Carruthers 2014 [34], a | BoNT naive | DBPC |
| Moers-Carpi 2015 [35], a | BoNT naive | DBPC |
| Carruthers 2015 [36], a | Only in past BoNT study | DBPC |
| Overactive bladder b | ||
| Chapple 2013 [37], a | No BoNT for urologic condition; no BoNT for any indication ≤12 weeks | DBPC |
| Nitti 2013 [38], a | No BoNT for urologic condition; no BoNT for any indication ≤12 weeks | DBPC |
| Nitti 2016 [39], a | No requirement | OL |
| Ginsberg 2017 [40], a | No requirement | OL |
| Pediatric spasticity | ||
| Dimitrova 2022 [41], a | No BoNT for any indication ≤6 months | DBPC |
| Dimitrova 2021 [42], a | No requirement | DBPC |
| Pediatric neurogenic detrusor overactivity | ||
| Austin 2021 | No previous/current BoNT for any urologic condition | DBPC |
| Study 121R (data on file) | No requirement | OL |
| Indication | Subjects, n | Gender (M, F), n (%) | Maximum No. of Treatment Cycles | Mean (SD) No. of Treatment Cycles | Dose Range, U | Mean (SD) Dose, U | Dosing Route |
|---|---|---|---|---|---|---|---|
| Cervical dystonia | 326 | 98 (30), 228 (70) | 15 | 8.4 (3.22) | 20–500 | 187.3 (76.47) | IM |
| Glabellar lines | 846 | 100 (12), 746 (88) | 5 | 2.8 (1.15) | 10–20 | 17.2 (4.51) | IM |
| Hyperhidrosis | 1077 | 439 (41), 638 (59) | 14 | 2.8 (1.97) | 100–150 | 102.8 (11.41) | ID |
| Migraine | 501 | 69 (14), 432 (86) | 3 | 2.8 (0.53) | 75–260 | 165.2 (57.00) | IM |
| Adult post-stroke spasticity | 449 | 224 (50), 225 (50) | 5 | 3.3 (1.42) | 100–600 | 307.3 (79.18) | IM |
| NDO | 619 | 256 (41), 363 (59) | 13 | 3.1 (2.28) | 200–300 | 238.2 (48.59) | IM |
| Lateral canthal lines | 916 | 109 (12), 807 (88) | 4 | 2.5 (1.19) | 24–44 | 33.8 (10.00) | IM |
| Overactive bladder a | 974 | 108, (11), 866 (89) | 13 | 3.6 (2.48) | 20–200 | 108.7 (19.26) | IM |
| Pediatric lower limb spasticity | 325 | 173 (53), 152 (47) | 6 | 4.2 (1.37) | 40–340.5 | 177.7 (76.23) | IM |
| Pediatric NDO | 113 | 65 (58), 48 (42) | 4 | 2.4 (0.92) | 50–200 | 128.4 (59.85) | IM |
| Total | 6146 | M: 1641 (27), F: 4505 (73) | 3–15 | 3.3 (2.25) | 10–600 | 134.8 (94.89) | ID, IM |
| Indication | Subjects, n | Post-Treatment NAb-Positive Subjects, n (%) [95% CI] | Post-Treatment NAb-Positive Subjects by Gender | NAb-Positive Subjects at Study Exit, n (%) [95% CI] | |
|---|---|---|---|---|---|
| Male, n (%) [95% CI] | Female, n (%) [95% CI] | ||||
| Cervical dystonia | 319 | 4 (1.3) [0, 2.5] | 2 (2.1) [0, 4.9] | 2 (0.9) [0, 2.1] | 1 (0.3) [0, 0.9] |
| Glabellar lines | 810 | 3 (0.4) [0, 0.8] | 0 (0.0) | 3 (0.4) [0, 0.9] | 0 (0.0) |
| Hyperhidrosis | 973 | 4 (0.4) [0, 0.8] | 1 (0.3) [0, 0.8] | 3 (0.5) [0, 1.1] | 2 (0.2) [0, 0.5] |
| Migraine | 501 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Adult poststroke spasticity | 406 | 2 (0.5) [0, 1.2] | 1 (0.5) [0, 1.4] | 1 (0.5) [0, 1.5] | 2 (0.5) [0, 1.2] |
| NDO | 589 | 8 (1.4) [0.4, 2.3] | 8 (3.3) [1.0, 5.5] | 0 (0.0) | 7 (1.2) [0.3, 2.1] |
| Lateral canthal lines | 915 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Overactive bladder | 956 | 3 (0.3) [0, 0.7] | 0 (0.0) | 3 (0.4) [0, 0.7] | 1 (0.1) [0, 0.3] |
| Pediatric lower limb spasticity | 299 | 3 (1.0) [0, 2.1] | 2 (1.3) [0, 3.1] | 1 (0.7) [0, 2.1] | 3 (1.0) [0, 2.1] |
| Pediatric NDO | 108 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Total | 5876 | 27 (0.5% of total) [0.3, 0.6] | 14 (0.9) [0.4, 1.4] | 13 (0.3) [0.1, 0.5] | 16 (0.3% of total) [0.1, 0.4] |
| Treatment Cycle | Number of Patients with Positive NAb for the First Time | Total Number of Patients Receiving OnabotulinumtoxinA a | Incidence of Positive NAb Onset (%) [95% CI] |
|---|---|---|---|
| 1 | 6 | 4278 | 0.1 [0, 0.3] |
| 2 | 5 | 2959 | 0.2 [0, 0.3] |
| 3 | 0 | 2584 | 0 |
| 4 | 3 | 1624 | 0.2 [0, 0.4] |
| 5 | 2 | 1001 | 0.2 [0, 0.5] |
| 6 | 5 | 610 | 0.8 [0.1, 1.5] |
| 7 | 1 | 422 | 0.2 [0, 0.7] |
| 8 | 4 | 334 | 1.2 [0, 2.4] |
| 9 | 1 | 259 | 0.4 [0, 1.1] |
| 10 | 0 | 176 | 0 |
| 11 | 0 | 116 | 0 |
| 12 | 0 | 49 | 0 |
| 13 | 0 | 17 | 0 |
| 14 | 0 | 6 | 0 |
| 15 | 0 | 1 | 0 |
| NAb Formation | Lower Quartile | Median | Upper Quartile |
|---|---|---|---|
| No (n = 4449) | 96.5 | 119 | 196 |
| Yes (n = 21) a | 101 | 134 | 186 |
| Indications | Initial Responders | Nonresponders Both Prior to and after Nab Formation [D] c | Total | ||
|---|---|---|---|---|---|
| Lost Response after Nab Formation (Secondary Nonresponders) [A] | Continued to Respond after Nab Formation [B] | No Efficacy Results Available after Nab Formation [C] | |||
| Cervical dystonia | 3 | 1 | 0 | 0 | 4 |
| Glabellar lines | 0 | 3 b | 0 | 0 | 3 |
| Hyperhidrosis | 0 | 3 | 1 | 0 | 4 |
| Adult post-stroke spasticity | 0 | 1 | 0 | 1 | 2 |
| Neurogenic detrusor overactivity | 2 | 4 | 2 | 0 | 8 |
| Overactive bladder | 0 | 1 | 0 | 2 | 3 |
| Pediatric lower limb spasticity | 0 | 2 | 0 | 1 | 3 |
| Total | 5 | 15 | 3 | 4 | 27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jankovic, J.; Carruthers, J.; Naumann, M.; Ogilvie, P.; Boodhoo, T.; Attar, M.; Gupta, S.; Singh, R.; Soliman, J.; Yushmanova, I.; et al. Neutralizing Antibody Formation with OnabotulinumtoxinA (BOTOX®) Treatment from Global Registration Studies across Multiple Indications: A Meta-Analysis. Toxins 2023, 15, 342. https://doi.org/10.3390/toxins15050342
Jankovic J, Carruthers J, Naumann M, Ogilvie P, Boodhoo T, Attar M, Gupta S, Singh R, Soliman J, Yushmanova I, et al. Neutralizing Antibody Formation with OnabotulinumtoxinA (BOTOX®) Treatment from Global Registration Studies across Multiple Indications: A Meta-Analysis. Toxins. 2023; 15(5):342. https://doi.org/10.3390/toxins15050342
Chicago/Turabian StyleJankovic, Joseph, Jean Carruthers, Markus Naumann, Patricia Ogilvie, Terry Boodhoo, Mayssa Attar, Swati Gupta, Ritu Singh, John Soliman, Irina Yushmanova, and et al. 2023. "Neutralizing Antibody Formation with OnabotulinumtoxinA (BOTOX®) Treatment from Global Registration Studies across Multiple Indications: A Meta-Analysis" Toxins 15, no. 5: 342. https://doi.org/10.3390/toxins15050342