Impact of Botulinum Toxin Injections on Quality of Life of Patients with Long-Standing Peripheral Facial Palsy

 , , and
, , and
Abstract
:1. Introduction
2. Results
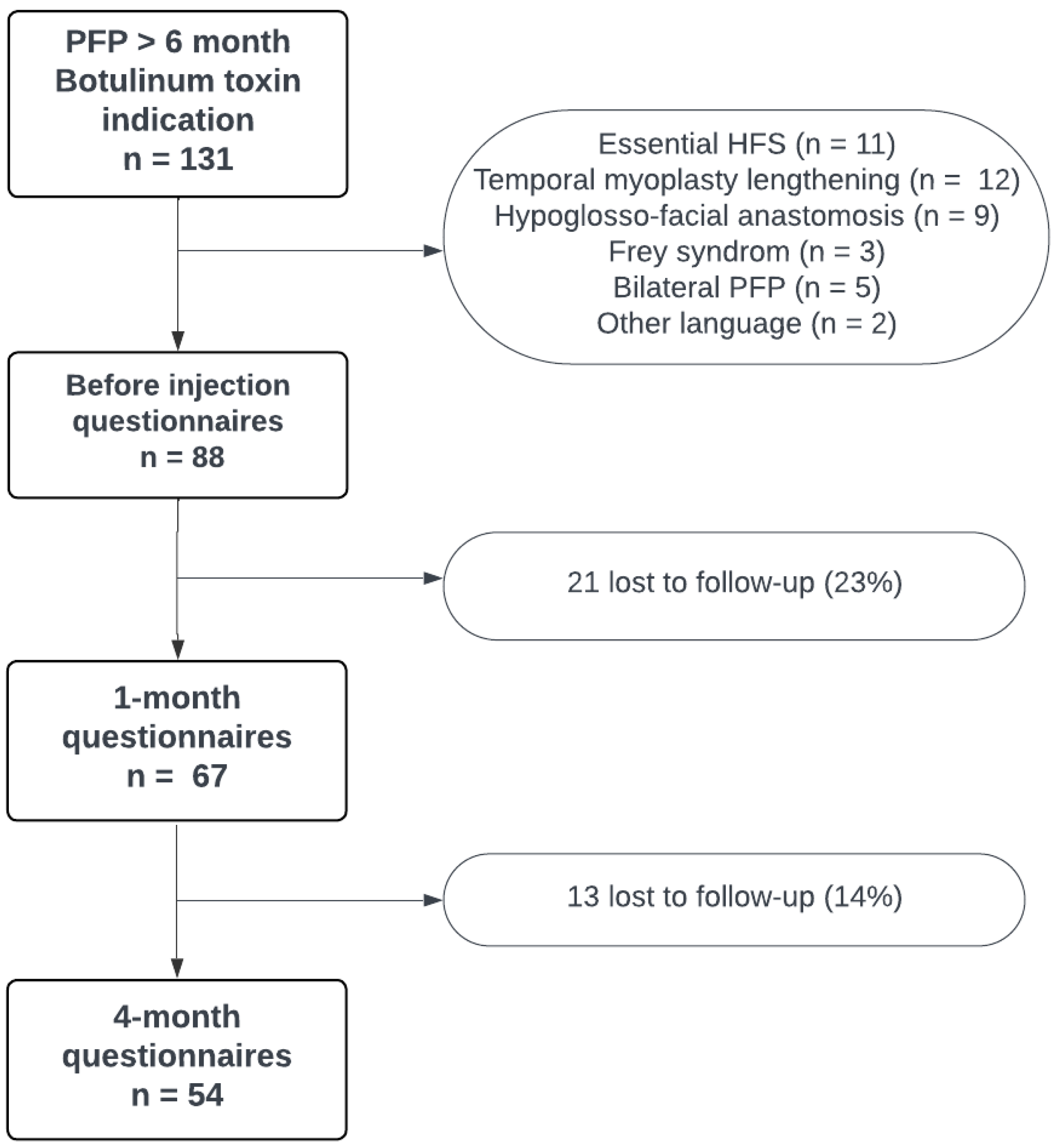
2.1. Demographic and Clinical Data
2.2. Longitudinal Evolution of QoL Questionnaires
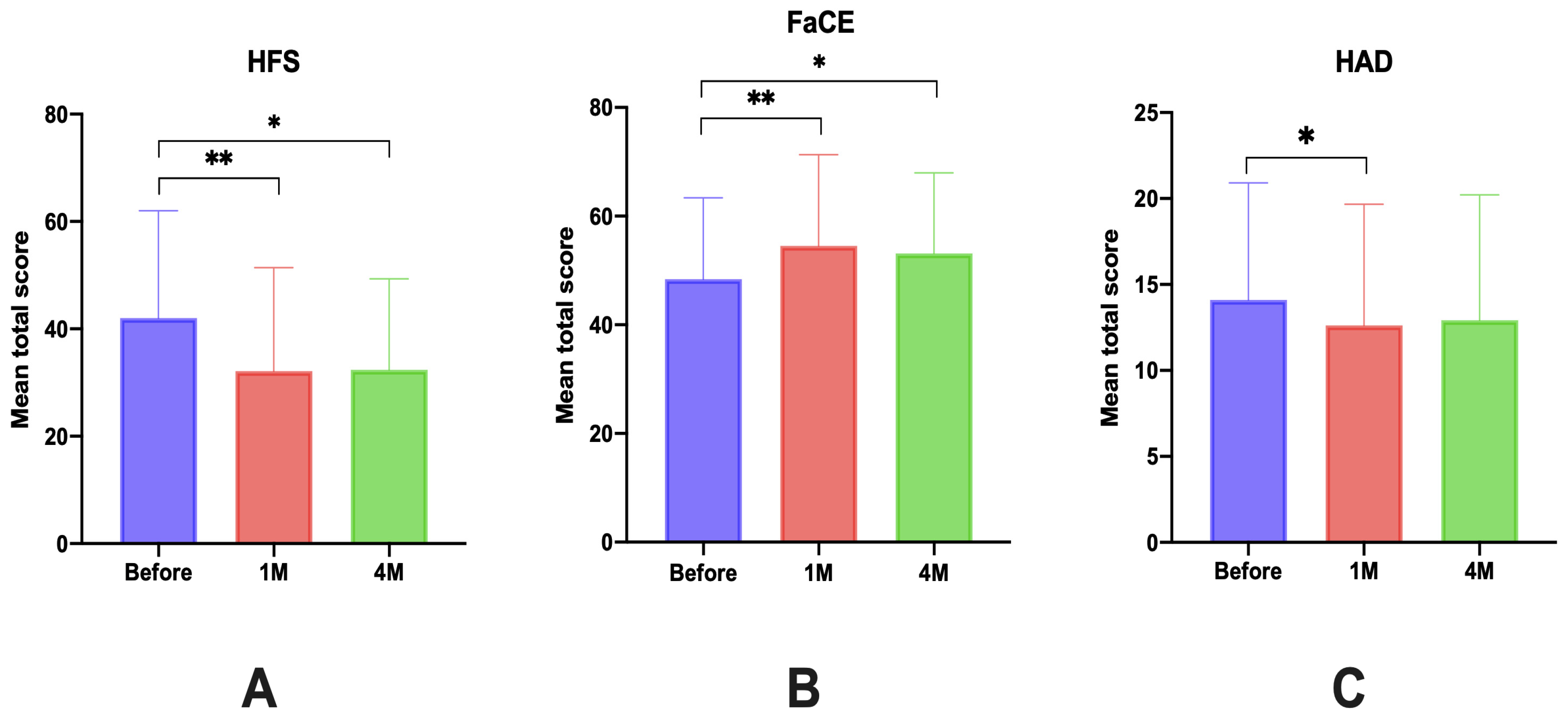
2.2.1. Total Scores
2.2.2. Total Score by Domains
2.2.3. Subgroup Analyses
Qualitative Data
Quantitative Data
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Population
5.2. Data Collection
5.3. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holland, N.J.; Bernstein, J.M. Bell’s palsy. BMJ Clin. Evid. 2014, 2014, 1204. [Google Scholar]
- Adour, K.K.; Byl, F.M.; Hilsinger, R.L.; Kahn, Z.M.; Sheldon, M.I. The true nature of Bell’s palsy: Analysis of 1000 consecutive patients. Laryngoscope 1978, 88, 787–801. [Google Scholar] [CrossRef]
- Kang, T.S.; Vrabec, J.T.; Giddings, N.; Terris, D.J. Facial nerve grading systems (1985–2002): Beyond the House-Brackmann scale. Otol. Neurotol. 2002, 23, 767–771. [Google Scholar] [CrossRef]
- Benichou, L.; Labbe, D.; Le Louarn, C.; Guerreschi, P. Facial palsy sequel and botulinum toxin. Ann. Chir. Plast. Esthet. 2015, 60, 377–392. [Google Scholar] [CrossRef] [PubMed]
- Guerreschi, P.; Labbé, D. Sequelae of Facial Palsy: A Comprehensive Treatment. Plast. Reconstr. Surg. 2019, 144, 682e–692e. [Google Scholar] [CrossRef] [PubMed]
- Salles, A.G.; da Costa, E.F.; Ferreira, M.C.; do Nascimento Remigio, A.F.; Moraes, L.B.; Gemperli, R. Epidemiologic Overview of Synkinesis in 353 Patients with Longstanding Facial Paralysis under Treatment with Botulinum Toxin for 11 Years. Plast. Reconstr. Surg. 2015, 136, 1289–1298. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, D.J.; Haas, L.P.; Tucker, S.M. Long-term Outcome After Acute Peripheral Facial Palsy. Ophthal. Plast. Reconstr. Surg. 2022, 38, 381–386. [Google Scholar] [CrossRef]
- Crumley, R.L. Mechanisms of synkinesis. Laryngoscope 1979, 89, 1847–1854. [Google Scholar] [CrossRef]
- Valls-Solé, J. Facial nerve palsy and hemifacial spasm. Handb. Clin. Neurol. 2013, 115, 367–380. [Google Scholar] [CrossRef]
- Saadi, R.; Shokri, T.; Schaefer, E.; Hollenbeak, C.; Lighthall, J.G. Depression Rates after Facial Paralysis. Ann. Plast. Surg. 2019, 83, 190–194. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Kong, I.G.; Oh, D.J.; Choi, H.G. Increased risk of depression in Bell’s palsy: Two longitudinal follow-up studies using a national sample cohort. J. Affect. Disord. 2019, 251, 256–262. [Google Scholar] [CrossRef]
- Cabin, J.A.; Massry, G.G.; Azizzadeh, B. Botulinum toxin in the management of facial paralysis. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 272–280. [Google Scholar] [CrossRef] [PubMed]
- De Sanctis Pecora, C.; Shitara, D. Botulinum Toxin Type A to Improve Facial Symmetry in Facial Palsy: A Practical Guideline and Clinical Experience. Toxins 2021, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, V.F.; Vieira, A.P.S.; Paggiaro, A.O.; Salles, A.G.; Gemperli, R. Evaluation of the body image of patients with facial palsy before and after the application of botulinum toxin. Int. J. Dermatol. 2019, 58, 1175–1183. [Google Scholar] [CrossRef]
- Cuenca-Martínez, F.; Zapardiel-Sánchez, E.; Carrasco-González, E.; La Touche, R.; Suso-Martí, L. Assessing anxiety, depression and quality of life in patients with peripheral facial palsy: A systematic review. PeerJ 2020, 8, e10449. [Google Scholar] [CrossRef]
- Fu, L.; Bundy, C.; Sadiq, S.A. Psychological distress in people with disfigurement from facial palsy. Eye 2011, 25, 1322–1326. [Google Scholar] [CrossRef] [PubMed]
- Krane, N.A.; Genther, D.; Weierich, K.; Hanseler, H.; Liu, S.W.; Mowery, A.; Loyo, M. Degree of Self-Reported Facial Impairment Correlates with Social Impairment in Individuals with Facial Paralysis and Synkinesis. Facial Plast. Surg. Aesthetic Med. 2020, 22, 362–369. [Google Scholar] [CrossRef]
- Fujiwara, K.; Fukuda, A.; Morita, S.; Yanagi, H.; Hoshino, K.; Nakamaru, Y.; Furuta, Y.; Homma, A. Psychological evaluation for patients with non-cured facial nerve palsy. Auris. Nasus. Larynx 2022, 49, 53–57. [Google Scholar] [CrossRef]
- Ho, A.L.; Scott, A.M.; Klassen, A.F.; Cano, S.J.; Pusic, A.L.; Van Laeken, N. Measuring quality of life and patient satisfaction in facial paralysis patients: A systematic review of patient-reported outcome measures. Plast. Reconstr. Surg. 2012, 130, 91–99. [Google Scholar] [CrossRef]
- Kahn, J.B.; Gliklich, R.E.; Boyev, K.P.; Stewart, M.G.; Metson, R.B.; McKenna, M.J. Validation of a patient-graded instrument for facial nerve paralysis: The FaCE scale. Laryngoscope 2001, 111, 387–398. [Google Scholar] [CrossRef]
- VanSwearingen, J.M.; Brach, J.S. The Facial Disability Index: Reliability and validity of a disability assessment instrument for disorders of the facial neuromuscular system. Phys. Ther. 1996, 76, 1288–1298; discussion 1298–1300. [Google Scholar] [CrossRef]
- Bruins, T.E.; van Veen, M.M.; Werker, P.M.N.; Dijkstra, P.U.; Broekstra, D.C. Associations Between Clinician-Graded Facial Function and Patient-Reported Quality of Life in Adults With Peripheral Facial Palsy: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 717–728. [Google Scholar] [CrossRef]
- Díaz-Aristizabal, U.; Valdés-Vilches, M.; Fernández-Ferreras, T.R.; Calero-Muñoz, E.; Bienzobas-Allué, E.; Moracén-Naranjo, T. Correlations between impairment, psychological distress, disability, and quality of life in peripheral facial palsy. Neurología 2019, 34, 423–428. [Google Scholar] [CrossRef]
- Tavares-Brito, J.; van Veen, M.M.; Dusseldorp, J.R.; Bahmad, F.; Hadlock, T.A. Facial Palsy-Specific Quality of Life in 920 Patients: Correlation With Clinician-Graded Severity and Predicting Factors. Laryngoscope 2019, 129, 100–104. [Google Scholar] [CrossRef]
- Györi, E.; Przestrzelski, C.; Pona, I.; Hagmann, M.; Rath, T.; Radtke, C.; Tzou, C.-H.J. Quality of life and functional assessment of facial palsy patients: A questionnaire study. Int. J. Surg. Lond. Engl. 2018, 55, 92–97. [Google Scholar] [CrossRef]
- Kleiss, I.J.; Beurskens, C.H.G.; Stalmeier, P.F.M.; Ingels, K.J.A.O.; Marres, H.A.M. Quality of life assessment in facial palsy: Validation of the Dutch Facial Clinimetric Evaluation Scale. Eur. Arch. Otorhinolaryngol. 2015, 272, 2055–2061. [Google Scholar] [CrossRef]
- Díaz-Aristizabal, U.; Valdés-Vilches, M.; Fernández-Ferreras, T.R.; Calero-Muñoz, E.; Bienzobas-Allué, E.; Aguilera-Ballester, L.; Carnicer-Cáceres, J. Effect of botulinum toxin typeA in functionality, synkinesis and quality of life in peripheral facial palsy sequelae. Neurología 2021, 38, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Bylund, N.; Hultcrantz, M.; Jonsson, L.; Marsk, E. Quality of Life in Bell’s Palsy: Correlation with Sunnybrook and House-Brackmann Over Time. Laryngoscope 2021, 131, E612–E618. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.F.F.; Peres, S.V.; Lazarini, P.R.; Cunha, M.C. Evaluation of the sensitivity of the Psychosocial Scale of Facial Appearance in peripheral facial paralysis. CoDAS 2018, 30, e20180072. [Google Scholar] [CrossRef] [PubMed]
- Shinn, J.R.; Nwabueze, N.N.; Du, L.; Patel, P.N.; Motamedi, K.K.; Norton, C.; Ries, W.R.; Stephan, S.J. Treatment Patterns and Outcomes in Botulinum Therapy for Patients With Facial Synkinesis. JAMA Facial Plast. Surg. 2019, 21, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Van Veen, M.M.; Tavares-Brito, J.; van Veen, B.M.; Dusseldorp, J.R.; Werker, P.M.N.; Dijkstra, P.U.; Hadlock, T.A. Association of Regional Facial Dysfunction With Facial Palsy-Related Quality of Life. JAMA Facial Plast. Surg. 2019, 21, 32–37. [Google Scholar] [CrossRef]
- Luijmes, R.E.; Pouwels, S.; Beurskens, C.H.G.; Kleiss, I.J.; Siemann, I.; Ingels, K.J.A.O. Quality of life before and after different treatment modalities in peripheral facial palsy: A systematic review. Laryngoscope 2017, 127, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.P.; Hadlock, T.A. Botulinum toxin and quality of life in patients with facial paralysis. Arch. Facial Plast. Surg. 2008, 10, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Salles, A.G.; Toledo, P.N.; Ferreira, M.C. Botulinum toxin injection in long-standing facial paralysis patients: Improvement of facial symmetry observed up to 6 months. Aesthetic Plast. Surg. 2009, 33, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Fuzi, J.; Taylor, A.; Sideris, A.; Meller, C. Does Botulinum Toxin Therapy Improve Quality of Life in Patients with Facial Palsy? Aesthetic Plast. Surg. 2020, 44, 1811–1819. [Google Scholar] [CrossRef]
- Borodic, G.; Bartley, M.; Slattery, W.; Glasscock, M.; Johnson, E.; Malazio, C.; Goodnough, M.; Acquadro, M.; McKenna, M. Botulinum toxin for aberrant facial nerve regeneration: Double-blind, placebo-controlled trial using subjective endpoints. Plast. Reconstr. Surg. 2005, 116, 36–43. [Google Scholar] [CrossRef]
- Do Nascimento Remigio, A.F.; Salles, A.G.; de Faria, J.C.M.; Ferreira, M.C. Comparison of the efficacy of onabotulinumtoxinA and abobotulinumtoxinA at the 1: 3 conversion ratio for the treatment of asymmetry after long-term facial paralysis. Plast. Reconstr. Surg. 2015, 135, 239–249. [Google Scholar] [CrossRef]
- Barry, P.; Mancini, J.; Alshukry, A.; Salburgo, F.; Lavieille, J.-P.; Montava, M. Validation of French versions of the Facial Disability Index and the Facial Clinimetric Evaluation Scale, specific quality of life scales for peripheral facial palsy patients. Clin. Otolaryngol. 2019, 44, 313–322. [Google Scholar] [CrossRef]
- Tan, E.-K.; Fook-Chong, S.; Lum, S.-Y.; Lim, E. Botulinum toxin improves quality of life in hemifacial spasm: Validation of a questionnaire (HFS-30). J. Neurol. Sci. 2004, 219, 151–155. [Google Scholar] [CrossRef]
- Alciato, L.; Simon, F.; Hervochon, R.; Trunet, S.; Nouet, A.; Tankéré, F. Quality of life after hemifacial spasm surgery: French versions of the HFS-8 and HFS-30 questionnaires. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2021, 138, 425–430. [Google Scholar] [CrossRef]
- Cheng, J.; Lei, D.; Hui, X.; Zhang, H. Improvement of Quality of Life in Patients with Hemifacial Spasm after Microvascular Decompression: A Prospective Study. World Neurosurg. 2017, 107, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Pouwels, S.; Sanches, E.E.; Chaiet, S.R.; de Jongh, F.W.; Beurskens, C.H.G.; Monstrey, S.J.; Luijmes, R.E.; Siemann, I.; Ramnarain, D.; Marres, H.A.M.; et al. Association between duration of peripheral facial palsy, severity, and age of the patient, and psychological distress. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 3048–3054. [Google Scholar] [CrossRef] [PubMed]
- Ross, B.G.; Fradet, G.; Nedzelski, J.M. Development of a sensitive clinical facial grading system. Otolaryngol. Head Neck Surg. 1996, 114, 380–386. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Data | Value |
|---|---|
| Men (n, %)/Women (n, %) | 25 (28%)/63 (72%) |
| Age (mean ± DS [rank]) | 53 ± 15.8 [26–90] |
| PFP etiology (n, %) | |
| - Idiopathic | 49 (55%) |
| - Zoster | 8 (9%) |
| - Traumatic | 20 (23%) |
| - Tumoral and traumatic | 6 (7%) |
| - General disease | 4 (5%) |
| - Other | 1 (1%) |
| Initial HBS | |
| - III (n, %) | 2 (2.2%) |
| - IV (n, %) | 4 (4.5%) |
| - V (n, %) | 43 (48%) |
| - VI (n, %) | 30 (34%) |
| Actual Sunnybrook score (mean ± DS) | 62.9 ± 33 [17–91] (n = 40) |
| Nb of months since last injection | 7.2 ± 3.39 [2.8–22.3] |
| Mean ± SD [range] | |
| Nb of years since the beginning of PFP | 5.7 ± 7 [0.45–45] |
| Mean ± SD [range] |
| Questionnaire (Mean ± SD) | HFS-30 | FaCE | HAD | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Delay after Injection | Before | 1 Month | 4 Months | Before | 1 Month | 4 Months | Before | 1 Month | 4 Months |
| Mean value (±SD) | 42.0 ± 20.0 | 32.1 ± 19.2 | 32.4 ± 17.0 | 48.4 ± 15.0 | 54.4 ± 16.8 | 53.1 ± 14.5 | 14.1 ± 6.8 | 12.7 ± 7.0 | 12.9 ± 7.3 |
| ∆ Score 1 | 9.9 | 9.6 | −6.1 | −4.7 | 1.4 | 0.78 | |||
| p | <0.0001 ** | <0.0001 ** | <0.0001 ** | <0.003 ** | 0.0032 * | 0.38 | |||
| Domains (Mean ± SD) | Before Injection | 1 Month | ∆ Score 1 | p |
|---|---|---|---|---|
| Mobility | 5.1 ± 4.0 | 3.9 ± 3.6 | 1.2 | 0.0021 * |
| Activities of daily living | 5.2 ± 4.6 | 4.1 ± 3.8 | 1.1 | 0.040 * |
| Emotional well-being | 9.6 ± 5.7 | 7.0 ± 5.6 | 2.5 | 0.0001 ** |
| Stigma | 9.5 ± 4.0 | 6.9 ± 4.0 | 2.5 | <0.0001 ** |
| Social support | 3.8 ± 3.3 | 3.8 ± 3.1 | 0.05 | 0.97 |
| Cognition | 4.2 ± 2.8 | 3.3 ± 2.6 | 0.9 | 0.0049 * |
| Communication | 4.7 ± 2.8 | 3.4 ± 2.6 | 1.3 | 0.0014 * |
| Domains (Mean ± SD) | Before Injection | 1 Month | ∆ Score 1 | p |
|---|---|---|---|---|
| Facial movement | 40.8 ± 22.2 | 41.5 ± 21.44 | −0.7 | 0.85 |
| Facial comfort | 31.4 ± 22.1 | 44.0 ± 26.2 | −12.6 | <0.0001 ** |
| Oral function | 60.1 ± 28.7 | 67.2 ± 25.7 | −7.1 | 0.0010 ** |
| Eye comfort | 45.9 ± 28.4 | 49.4 ± 29.8 | −3.6 | 0.0128 * |
| Lacrimal control | 52.8 ± 31.3 | 59.3 ± 31.9 | −6.5 | 0.1 |
| Social function | 61.3 ± 24.0 | 68.6 ± 23.5 | −7.3 | 0.0002 ** |
| HFS30 | FaCE | |||
|---|---|---|---|---|
| ∆ Score 1 | p | ∆ Score 1 | p | |
| Male (n = 17) | 1.19 | −1.35 | ||
| Female (n = 50) | 12.54 | 0.0164 * | −8.16 | 0.08 |
| Orbito-palpebral surgery | ||||
| Yes (n = 54) | 5.15 | −4.10 | ||
| No (n = 13) | 11.43 | 0.18 | −7.24 | 0.39 |
| Nb of anterior injections | ||||
| 0 (n = 16) | 17.5 | −9.44 | ||
| 1 (n = 8) | 4.25 | 0.0736 2 | −2.50 | 0.21 2 |
| 2 (n = 14) | 10.86 | 0.28 2 | −3.80 | 0.23 2 |
| ≥3 (n = 29) | 6.83 | 0.0458 *2 | −7.13 | 0.56 2 |
| HFS-30 | FaCE | |||
|---|---|---|---|---|
| Clinical Data | r | p | r | p |
| Age | −0.46 | <0.0001 ** | 0.27 | 0.03 * |
| BMI | −0.028 | 0.82 | 0.0038 | 0.98 |
| Sunnybrook | 0.19 | 0.23 | 0.13 | 0.41 |
| Sum of sequelae | 0.011 | 0.93 | −0.07 | 0.58 |
| Duration of PFP | −0.34 | 0.008 * | −0.21 | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amar, J.; Tankere, F.; Picard, D.; Alciato, L.; Carré, F.; Foirest, C. Impact of Botulinum Toxin Injections on Quality of Life of Patients with Long-Standing Peripheral Facial Palsy. Toxins 2024, 16, 140. https://doi.org/10.3390/toxins16030140
Amar J, Tankere F, Picard D, Alciato L, Carré F, Foirest C. Impact of Botulinum Toxin Injections on Quality of Life of Patients with Long-Standing Peripheral Facial Palsy. Toxins. 2024; 16(3):140. https://doi.org/10.3390/toxins16030140
Chicago/Turabian StyleAmar, Jérémy, Frédéric Tankere, Diane Picard, Lauranne Alciato, Fabienne Carré, and Claire Foirest. 2024. "Impact of Botulinum Toxin Injections on Quality of Life of Patients with Long-Standing Peripheral Facial Palsy" Toxins 16, no. 3: 140. https://doi.org/10.3390/toxins16030140