Glycodelin as a Serum and Tissue Biomarker for Metastatic and Advanced NSCLC

 , ,
, ,
Abstract
:1. Introduction
2. Results
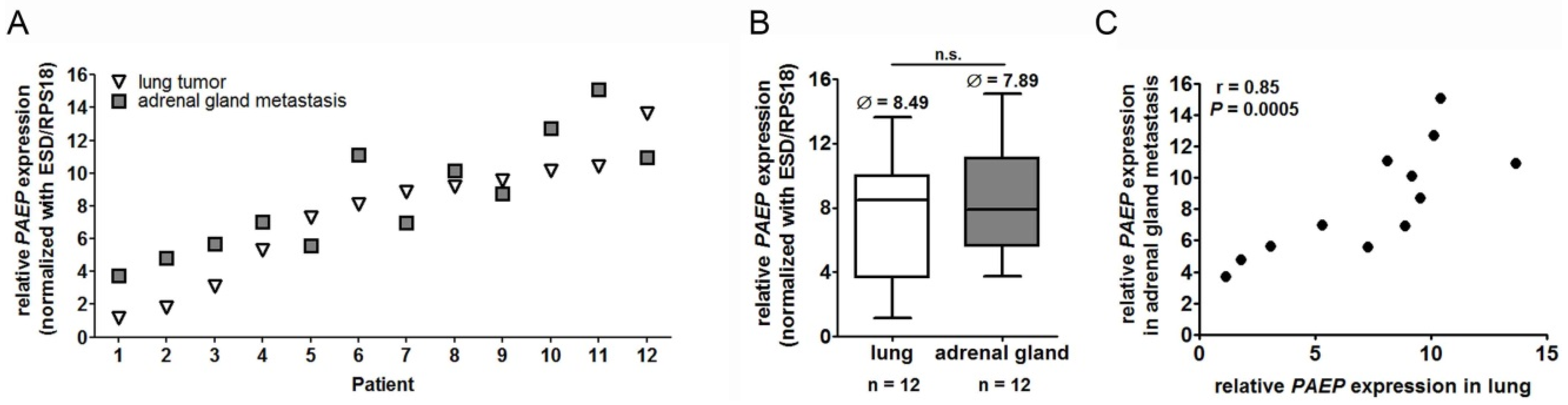
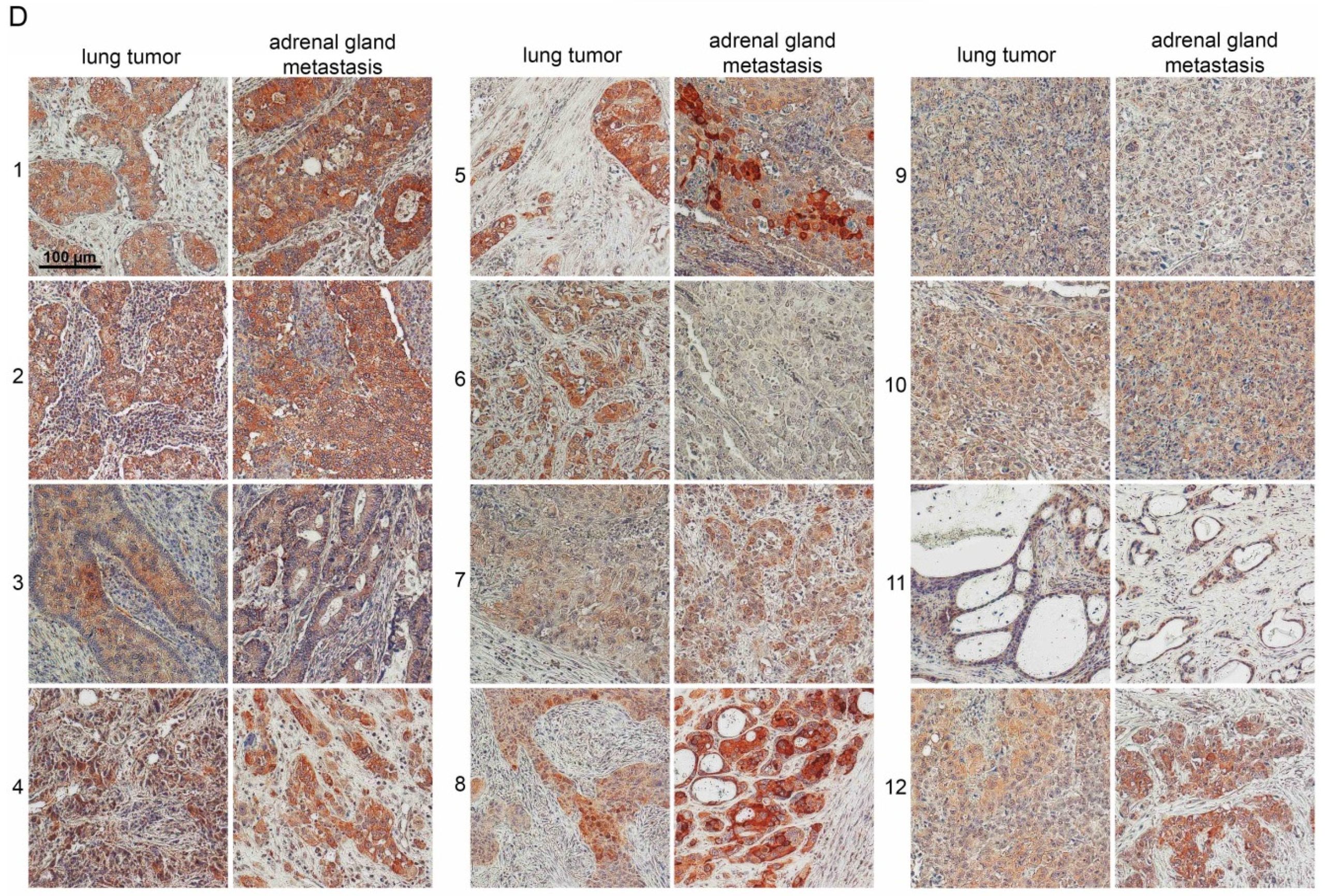
2.1. Glycodelin Expression in Primary Lung Tumor and Adrenal Gland Metastasis
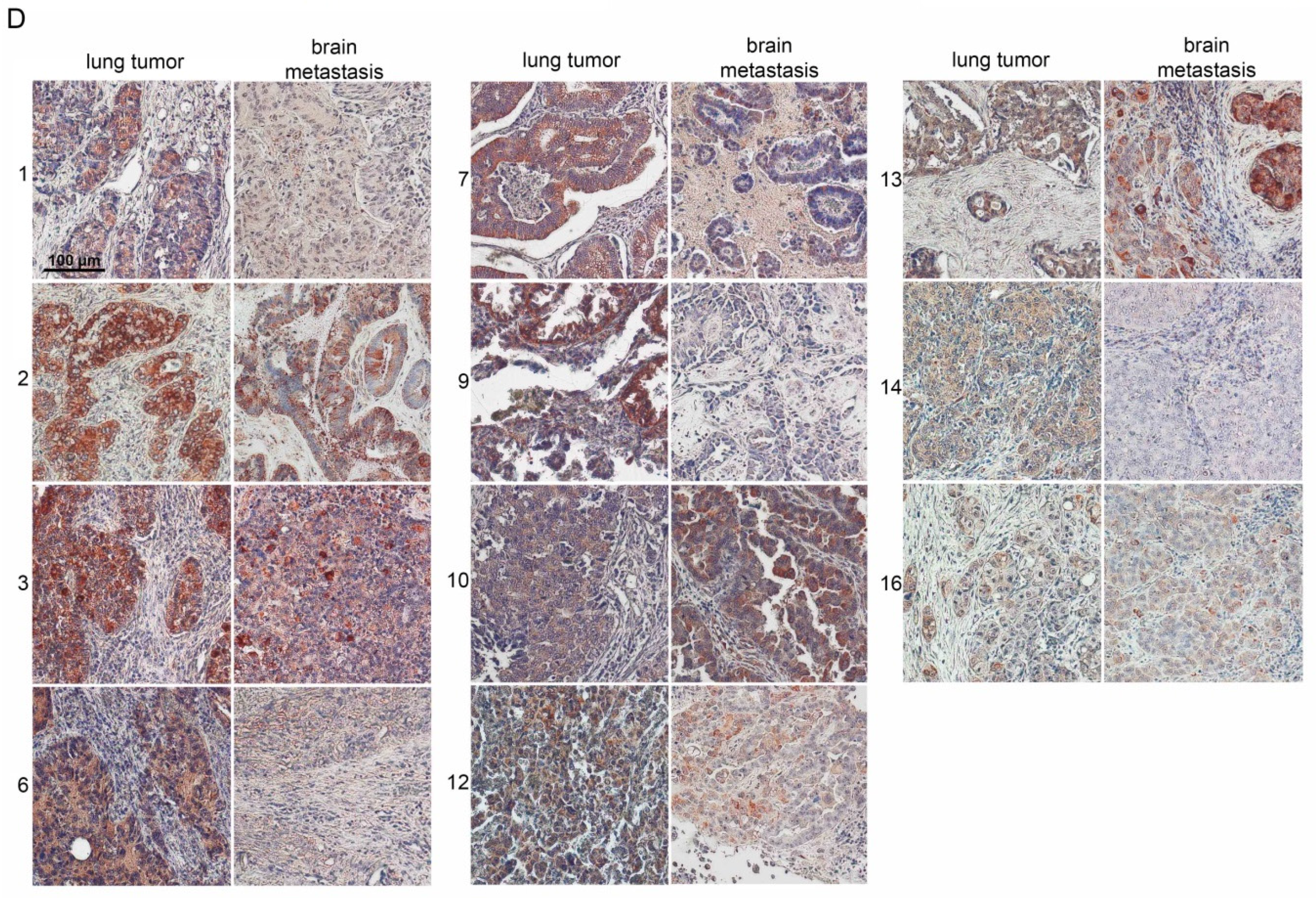
2.2. Glycodelin Expression in Primary Lung Tumor and Brain Metastasis
2.3. Glycodelin Expression in Cryo-Conserved Biopsies of Advanced Stage NSCLC Patients Correlated with Measured Glycodelin Serum Concentrations
2.4. Glycodelin Serum Concentration Is a Prognostic Factor for the Survival of NSCLC Patients
2.5. Glycodelin as a Follow-Up Biomarker for Monitoring of Advanced Stage NSCLC Patients
3. Discussion
4. Materials and Methods
4.1. Sampling of Biomaterial
4.2. Total RNA Isolation and cDNA Synthesis
4.3. Quantitative Real-Time PCR
4.4. Immunohistochemistry
4.5. Detection of Glycodelin in Human Sera
4.6. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC lung cancer staging project: Proposals for revision of the tnm stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Krapcho, M.; Miller, D.; Bishop, K.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. (Eds.) Seer Cancer Statistics Review, 1975–2014; National Cancer Institute: Bethesda, MD, USA, 2017.
- Ebert, W.; Hoppe, M.; Muley, T.; Drings, P. Monitoring of therapy in inoperable lung cancer patients by measurement of CYFRA 21-1, TPA-TP CEA, and NSE. Anticancer Res. 1997, 17, 2875–2878. [Google Scholar] [PubMed]
- Muley, T.; Rolny, V.; He, Y.; Wehnl, B.; Escherich, A.; Warth, A.; Stolp, C.; Schneider, M.A.; Dienemann, H.; Meister, M.; et al. The combination of the blood based tumor biomarkers cytokeratin 19 fragments (CYFRA 21-1) and carcinoembryonic antigen (CEA) as a potential predictor of benefit from adjuvant chemotherapy in early stage squamous cell carcinoma of the lung (SCC). Lung Cancer 2018, 120, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Shi, C.; Qian, J.; Teng, J.; Zhong, H.; Han, B. Comparison of plasma and tissue samples in epidermal growth factor receptor mutation by arms in advanced non-small cell lung cancer. Gene 2016, 591, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Chai, X.; Ren, P.; Wei, B.; Ma, J.; Mai, L.; Cram, D.S.; Song, Y.; Guo, Y. A comparative study of EGFR oncogenic mutations in matching tissue and plasma samples from patients with advanced non-small cell lung carcinoma. Clin. Chim. Acta 2016, 457, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Bersinger, N.A.; Birkhauser, M.H.; Yared, M.; Wunder, D.M. Serum glycodelin pattern during the menstrual cycle in healthy young women. Acta Obstet. Gynecol. Scand. 2009, 88, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Alok, A.; Karande, A.A. The role of glycodelin as an immune-modulating agent at the feto-maternal interface. J. Reprod. Immunol. 2009, 83, 124–127. [Google Scholar] [CrossRef]
- Seppala, M.; Taylor, R.N.; Koistinen, H.; Koistinen, R.; Milgrom, E. Glycodelin: A major lipocalin protein of the reproductive axis with diverse actions in cell recognition and differentiation. Endocr. Rev. 2002, 23, 401–430. [Google Scholar] [CrossRef]
- Lam, K.K.; Chiu, P.C.; Chung, M.K.; Lee, C.L.; Lee, K.F.; Koistinen, R.; Koistinen, H.; Seppala, M.; Ho, P.C.; Yeung, W.S. Glycodelin-A as a modulator of trophoblast invasion. Hum. Reprod. 2009, 24, 2093–2103. [Google Scholar] [CrossRef] [Green Version]
- Mandelin, E.; Lassus, H.; Seppala, M.; Leminen, A.; Gustafsson, J.A.; Cheng, G.; Butzow, R.; Koistinen, R. Glycodelin in ovarian serous carcinoma: Association with differentiation and survival. Cancer Res. 2003, 63, 6258–6264. [Google Scholar] [PubMed]
- Hautala, L.C.; Greco, D.; Koistinen, R.; Heikkinen, T.; Heikkila, P.; Aittomaki, K.; Blomqvist, C.; Koistinen, H.; Nevanlinna, H. Glycodelin expression associates with differential tumour phenotype and outcome in sporadic and familial non-BRCA1/2 breast cancer patients. Breast Cancer Res. Treat. 2011, 128, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Koistinen, H.; Seppala, M.; Nagy, B.; Tapper, J.; Knuutila, S.; Koistinen, R. Glycodelin reduces carcinoma-associated gene expression in endometrial adenocarcinoma cells. Am. J. Obstet. Gynecol. 2005, 193, 1955–1960. [Google Scholar] [CrossRef] [PubMed]
- Lenhard, M.; Heublein, S.; Kunert-Keil, C.; Vrekoussis, T.; Lomba, I.; Ditsch, N.; Mayr, D.; Friese, K.; Jeschke, U. Immunosuppressive glycodelin a is an independent marker for poor prognosis in endometrial cancer. BMC Cancer 2013, 13, 616. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Liu, S.; Howell, P.M., Jr.; Zhang, G.; Pannell, L.; Samant, R.; Shevde-Samant, L.; Tucker, J.A.; Fodstad, O.; Riker, A.I. Functional characterization of the progestagen-associated endometrial protein gene in human melanoma. J. Cell. Mol. Med. 2010, 14, 1432–1442. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.A.; Granzow, M.; Warth, A.; Schnabel, P.A.; Thomas, M.; Herth, F.J.; Dienemann, H.; Muley, T.; Meister, M. Glycodelin: A new biomarker with immunomodulatory functions in non-small cell lung cancer. Clin. Cancer Res. 2015, 21, 3529–3540. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.A.; Muley, T.; Kahn, N.C.; Warth, A.; Thomas, M.; Herth, F.J.; Dienemann, H.; Meister, M. Glycodelin is a potential novel follow-up biomarker for malignant pleural mesothelioma. Oncotarget 2016, 7, 71285–71297. [Google Scholar] [CrossRef]
- Hida, T.; Nokihara, H.; Kondo, M.; Kim, Y.H.; Azuma, K.; Seto, T.; Takiguchi, Y.; Nishio, M.; Yoshioka, H.; Imamura, F.; et al. Alectinib versus crizotinib in patients with ALK-positive non-small-cell lung cancer (J-ALEX): An open-label, randomised phase 3 trial. Lancet 2017, 390, 29–39. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.; et al. Osimertinib or platinum-pemetrexed in EGFR t790m-positive lung cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef]
- Shaw, A.T.; Kim, D.W.; Mehra, R.; Tan, D.S.; Felip, E.; Chow, L.Q.; Camidge, D.R.; Vansteenkiste, J.; Sharma, S.; De Pas, T.; et al. Ceritinib in ALK-rearranged non-small-cell lung cancer. N. Engl. J. Med. 2014, 370, 1189–1197. [Google Scholar] [CrossRef]
- Tamura, T.; Kurishima, K.; Nakazawa, K.; Kagohashi, K.; Ishikawa, H.; Satoh, H.; Hizawa, N. Specific organ metastases and survival in metastatic non-small-cell lung cancer. Mol. Clin. Oncol. 2015, 3, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Popper, H.H. Progression and metastasis of lung cancer. Cancer Metast. Rev. 2016, 35, 75–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mujoomdar, A.; Austin, J.H.; Malhotra, R.; Powell, C.A.; Pearson, G.D.; Shiau, M.C.; Raftopoulos, H. Clinical predictors of metastatic disease to the brain from non-small cell lung carcinoma: Primary tumor size, cell type, and lymph node metastases. Radiology 2007, 242, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Bischof, A.; Briese, V.; Richter, D.U.; Bergemann, C.; Friese, K.; Jeschke, U. Measurement of glycodelin A in fluids of benign ovarian cysts, borderline tumours and malignant ovarian cancer. Anticancer Res. 2005, 25, 1639–1644. [Google Scholar] [PubMed]
- Kamarainen, M.; Halttunen, M.; Koistinen, R.; von Boguslawsky, K.; von Smitten, K.; Andersson, L.C.; Seppala, M. Expression of glycodelin in human breast and breast cancer. Int. J. Cancer 1999, 83, 738–742. [Google Scholar] [CrossRef] [Green Version]
- Muley, T.R.; Herth, F.J.; Schnabel, P.A.; Dienemann, H.; Meister, M. From tissue to molecular phenotyping: Pre-analytical requirements heidelberg experience. Transl. Lung Cancer Res. 2012, 1, 111–121. [Google Scholar] [PubMed]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Reporting recommendations for tumour marker prognostic studies (REMARK). Eur. J. Cancer 2005, 41, 1690–1696. [Google Scholar] [CrossRef]
- Dinse, G.E.; Lagakos, S.W. Nonparametric estimation of lifetime and disease onset distributions from incomplete observations. Biometrics 1982, 38, 921–932. [Google Scholar] [CrossRef]
- Mann, H.B.; Whitney, D.R. On a test whether one of two random variables is stochastically larger than the other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Spearman, C. The proof and measurement of association between two things. Am. J. Psychol. 1904, 15, 72–101. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | n | (%) | Parameter | n | (%) |
|---|---|---|---|---|---|
| Surgical Cohort | 28 | Biopsy Cohort (Malignant Only) | 55 | ||
| Median age | 61 (40–77) | Median age | 66 (50–81) | ||
| Gender | 28 | 100 | Gender | 55 | 100 |
| Male | 18 | 64 | Male | 35 | 64 |
| Female | 10 | 36 | Female | 20 | 36 |
| ECOG | 28 | 100 | ECOG | 55 | 100 |
| 0 | 25 | 89 | 0 | 16 | 29 |
| 1 | 2 | 7 | 1 | 30 | 55 |
| 2 | 1 | 4 | 2 | 8 | 15 |
| n.d. | 1 | 1 | |||
| Histology | 28 | 100 | Histology | 55 | 100 |
| Adenocarcinoma | 15 | 54 | Adenocarcinoma | 28 | 51 |
| Squamous cell Carcinoma | 3 | 11 | Squamous cell Carcinoma | 19 | 35 |
| Large cell Carcinoma | 5 | 18 | Large cell Carcinoma | 4 | 7 |
| Other | 5 | 18 | Other | 4 | 7 |
| Initial clinical stage (7th edition) | 28 | 100 | Clinical stage (7th edition) | 55 | 100 |
| Stage IB | 1 | 4 | Stage IIIA | 7 | 13 |
| Stage IIA | 6 | 21 | Stage IIIB | 11 | 20 |
| Stage IIB | 2 | 7 | Stage IV | 37 | 67 |
| Stage IIIA | 5 | 18 | |||
| Stage IIIB | 3 | 11 | |||
| Stage IV | 11 | 39 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider, M.A.; Muley, T.; Weber, R.; Wessels, S.; Thomas, M.; Herth, F.J.F.; Kahn, N.C.; Eberhardt, R.; Winter, H.; Heussel, G.; et al. Glycodelin as a Serum and Tissue Biomarker for Metastatic and Advanced NSCLC. Cancers 2018, 10, 486. https://doi.org/10.3390/cancers10120486
Schneider MA, Muley T, Weber R, Wessels S, Thomas M, Herth FJF, Kahn NC, Eberhardt R, Winter H, Heussel G, et al. Glycodelin as a Serum and Tissue Biomarker for Metastatic and Advanced NSCLC. Cancers. 2018; 10(12):486. https://doi.org/10.3390/cancers10120486
Chicago/Turabian StyleSchneider, Marc A., Thomas Muley, Rebecca Weber, Sabine Wessels, Michael Thomas, Felix J. F. Herth, Nicolas C. Kahn, Ralf Eberhardt, Hauke Winter, Gudula Heussel, and et al. 2018. "Glycodelin as a Serum and Tissue Biomarker for Metastatic and Advanced NSCLC" Cancers 10, no. 12: 486. https://doi.org/10.3390/cancers10120486