Ensuring the Safety and Security of Frozen Lung Cancer Tissue Collections through the Encapsulation of Dried DNA

 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Introduction
2. Results
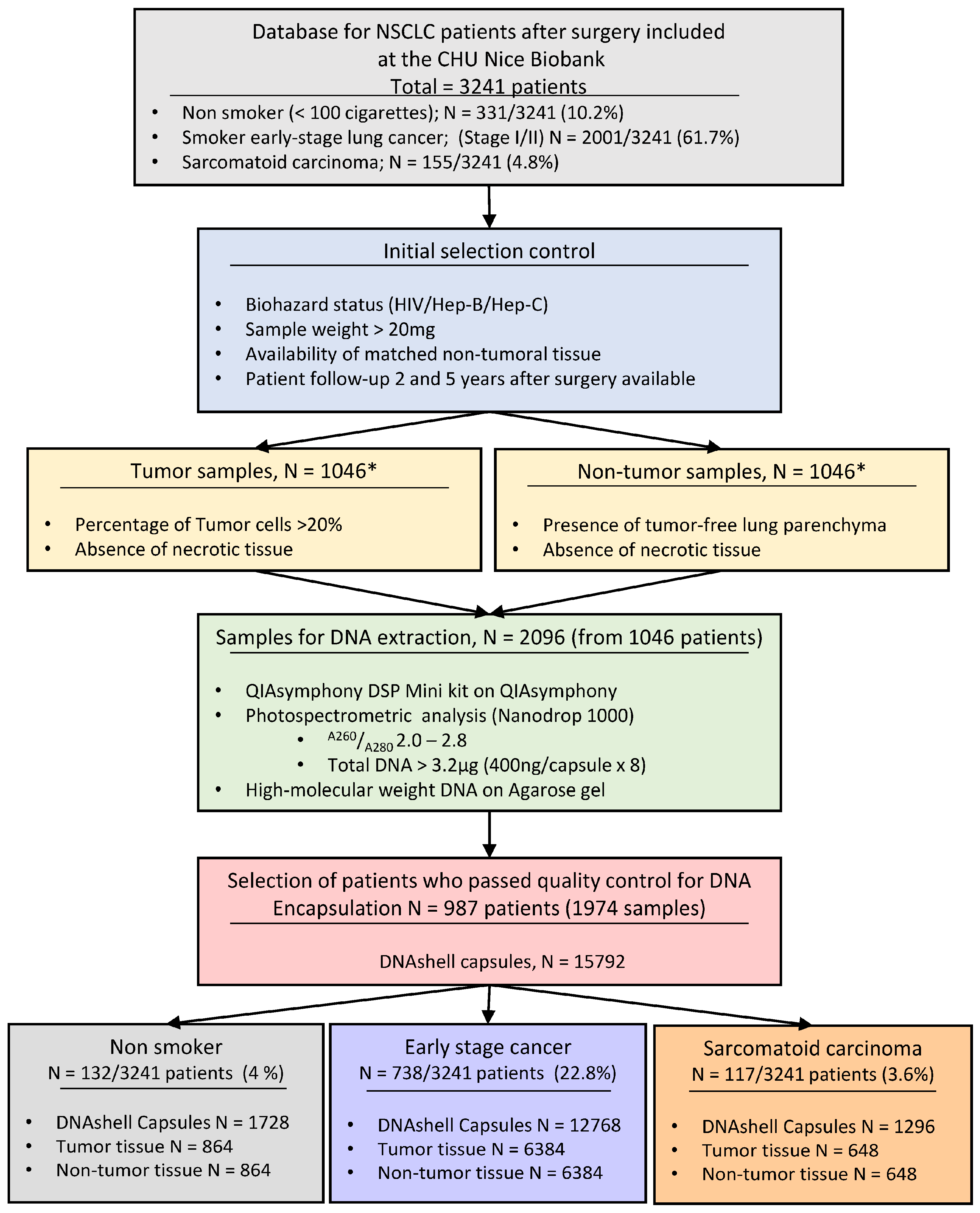
2.1. Patients and Selected Samples for DNA Extraction and Selection of DNA for the Biobank of the Nice University Hospital Center
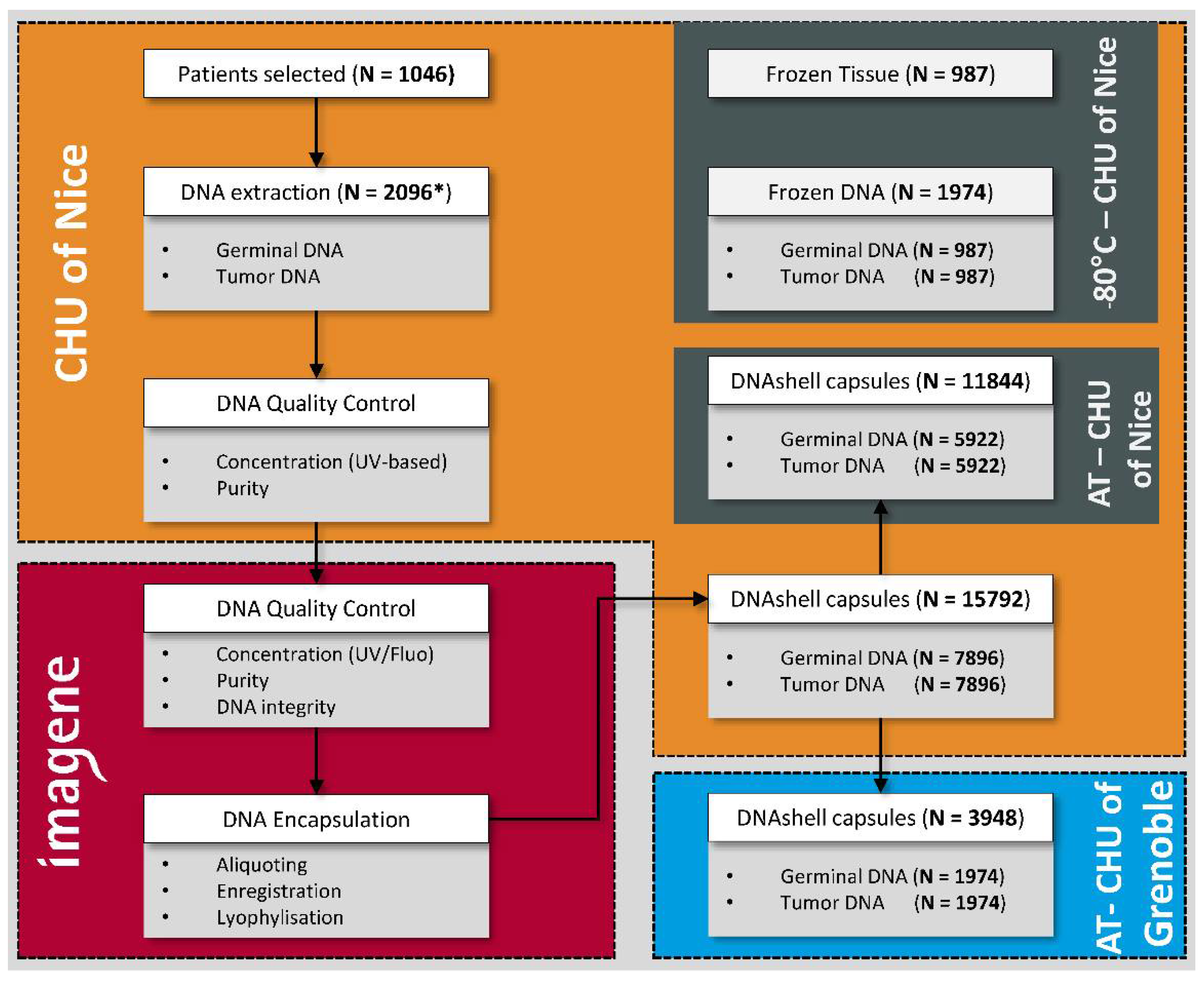
2.2. Encapsulation of DNA (Imagene, Evry)
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Didkowska, J.; Wojciechowska, U.; Mańczuk, M.; Łobaszewski, J. Lung cancer epidemiology: Contemporary and future challenges worldwide. Ann. Transl. Med. 2016, 4, 150. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Tiwari, R.C.; Murray, T.; Ghafoor, A.; Samuels, A.; Ward, E.; Feuer, E.J.; Thun, M.J. Cancer Statistics, 2004. CA Cancer J. Clin. 2004, 54, 8–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomarkers Prev. 2017, 26, 444–457. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, S.; Heederik, D.; Burdorf, A.; Colosio, C.; Cullinan, P.; Henneberger, P.K.; Olsson, A.; Raynal, A.; Rooijackers, J.; Santonen, T.; et al. European Respiratory Society Environment and Health Committee Current and new challenges in occupational lung diseases. Eur. Respir. Rev. 2017, 26. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, N.; Bansal, J.G. Risk factors of Lung Cancer in nonsmoker. Curr. Probl. Cancer 2017, 41, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Cui, H.; Gu, D.; Zhang, M.; Fang, Y.; Chen, S.; Tang, M.; Zhang, B.; Chen, H. Genetic polymorphisms and lung cancer risk: Evidence from meta-analyses and genome-wide association studies. Lung Cancer 2017, 113, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, Q.; Yuan, S.; Xie, W.; Liu, Y.; Xiang, Y.; Wu, N.; Wu, L.; Ma, X.; Cai, T.; et al. Genetic predisposition to lung cancer: Comprehensive literature integration, meta-analysis, and multiple evidence assessment of candidate-gene association studies. Sci. Rep. 2017, 7, 8371. [Google Scholar] [CrossRef] [PubMed]
- Attarian, S.; Rahman, N.; Halmos, B. Emerging uses of biomarkers in lung cancer management: Molecular mechanisms of resistance. Ann. Transl. Med. 2017, 5, 377. [Google Scholar] [CrossRef] [PubMed]
- Carper, M.B.; Claudio, P.P. Clinical potential of gene mutations in lung cancer. Clin. Transl. Med. 2015, 4, 33. [Google Scholar] [CrossRef] [PubMed]
- Costa-Pinheiro, P.; Montezuma, D.; Henrique, R.; Jerónimo, C. Diagnostic and prognostic epigenetic biomarkers in cancer. Epigenomics 2015, 7, 1003–1015. [Google Scholar] [CrossRef] [PubMed]
- Dey, N.; Williams, C.; Leyland-Jones, B.; De, P. Mutation matters in precision medicine: A future to believe in. Cancer Treat. Rev. 2017, 55, 136–149. [Google Scholar] [CrossRef] [PubMed]
- Mino-Kenudson, M. Immunohistochemistry for predictive biomarkers in non-small cell lung cancer. Transl. Lung Cancer Res. 2017, 6, 570–587. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.N.; Ersek, J.L.; Kim, E.S. Lung cancer biomarkers, targeted therapies and clinical assays. Transl. Lung Cancer Res. 2015, 4, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Qiao, G.; Xu, E.; Xuan, Y.; Liao, M.; Yin, G. Biomarkers for early diagnosis, prognosis, prediction, and recurrence monitoring of non-small cell lung cancer. Onco Targets. Ther. 2017, 10, 4527–4534. [Google Scholar] [CrossRef] [PubMed]
- Vermaelen, K.; Waeytens, A.; Kholmanskikh, O.; Van den Bulcke, M.; Van Valckenborgh, E. Perspectives on the integration of Immuno-Oncology Biomarkers and drugs in a Health Care setting. Semin. Cancer Biol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Voong, K.R.; Feliciano, J.; Becker, D.; Levy, B. Beyond PD-L1 testing-emerging biomarkers for immunotherapy in non-small cell lung cancer. Ann. Transl. Med. 2017, 5, 376. [Google Scholar] [CrossRef] [PubMed]
- Zamay, T.; Zamay, G.; Kolovskaya, O.; Zukov, R.; Petrova, M.; Gargaun, A.; Berezovski, M.; Kichkailo, A. Current and Prospective Protein Biomarkers of Lung Cancer. Cancers 2017, 9, 155. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, R.E. Biobanking: The foundation of personalized medicine. Curr. Opin. Oncol. 2011, 23, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.Q.; Chen, L.; Cooper, G.F.; Young, J.D.; Lu, X. Precision Oncology beyond Targeted Therapy: Combining Omics Data with Machine Learning Matches the Majority of Cancer Cells to Effective Therapeutics. Mol. Cancer Res. 2018, 16, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Qian, F.; Shen, L.; Chen, F.; Chen, J.; Shen, B. Computer-aided biomarker discovery for precision medicine: Data resources, models and applications. Brief. Bioinform. 2017. [Google Scholar] [CrossRef] [PubMed]
- Bellazzi, R. Big data and biomedical informatics: A challenging opportunity. Yearb. Med. Inform. 2014, 9, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Choi, T.-M.; Lambert, J.H. Advances in Risk Analysis with Big Data. Risk Anal. 2017, 37, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.A.; Demicco, E.G.; Saltz, J.H.; Powell, R.T.; Rao, A.; Lazar, A.J. PanCancer insights from The Cancer Genome Atlas: The pathologist’s perspective. J. Pathol. 2018, 244, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Cai, N.; Pacheco, P.P.; Narrandes, S.; Wang, Y.; Xu, W. Applications of Support Vector Machine (SVM) Learning in Cancer Genomics. Cancer Genom. Proteom. 2018, 15, 41–51. [Google Scholar] [CrossRef]
- Khan, N.; Yaqoob, I.; Hashem, I.A.T.; Inayat, Z.; Ali, W.K.M.; Alam, M.; Shiraz, M.; Gani, A. Big data: Survey, technologies, opportunities, and challenges. Sci. World J 2014, 2014, 712826. [Google Scholar] [CrossRef] [PubMed]
- Bjugn, R.; Hansen, J. Learning by Erring: Fire! Biopreserv. Biobank. 2013, 11, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Hager, R. Biobanking Operations: Contingency Planning and Disaster Recovery of Research Samples. Bioprocess. J. 2014, 13, 56–58. [Google Scholar] [CrossRef]
- Henderson, M.K.; Simeon-Dubach, D.; Zaayenga, A. When bad things happen: Lessons learned from effective and not so effective disaster and recovery planning for biobanks. Biopreserv. Biobank. 2013, 11, 193. [Google Scholar] [CrossRef] [PubMed]
- Mintzer, J.L.; Kronenthal, C.J.; Kelly, V.; Seneca, M.; Butler, G.; Fecenko-Tacka, K.; Altamuro, D.; Madore, S.J. Preparedness for a natural disaster: How Coriell planned for hurricane Sandy. Biopreserv. Biobank. 2013, 11, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Morrin, H.R.; Robinson, B.A. Sustaining a Biobank Through a Series of Earthquake Swarms: Lessons Learned from our New Zealand Experience. Biopreserv. Biobank. 2013, 11, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Roswall, N.; Halkjær, J.; Overvad, K.; Tjønneland, A. Measures Taken to Restore the Danish Diet, Cancer and Health Biobank After Flooding: A Framework for Future Biobank Restorations. Biopreserv. Biobank. 2013, 11, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Baird, P.M.; Benes, F.M.; Chan, C.-H.; Eng, C.B.; Groover, K.H.; Prodanovic, Z.; Rawley-Payne, M.; Kizza, R.; Hia, C.; Abouhamze, A. How Is Your Biobank Handling Disaster Recovery Efforts? Biopreserv. Biobank. 2013, 11, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Parry-Jones, A.; Hansen, J.; Simeon-Dubach, D.; Bjugn, R. Crisis Management for Biobanks. Biopreserv. Biobank. 2017, 15, 253–263. [Google Scholar] [CrossRef] [PubMed]
- OECD Best Practices Guidelines for BRC. 2007. Available online: http://www.oecd.org/sti/biotech/38777417.pdf (accessed on 8 April 2018).
- Collection, Processing and Long-Term Storage of Biological Samples in UK Biobank. Available online: http://www.ukbiobank.ac.uk/wp-content/uploads/2014/06/1030-Tim-Peakman-10.30am-sample-collection.pdf (accessed on 9 April 2018).
- Choi, J.R.; Park, S.Y.; Noh, O.K.; Koh, Y.W.; Kang, D.R. Gene mutation discovery research of non-smoking lung cancer patients due to indoor radon exposure. Ann. Occup. Environ. Med. 2016, 28, 13. [Google Scholar] [CrossRef] [PubMed]
- Mazières, J.; Rouquette, I.; Lepage, B.; Milia, J.; Brouchet, L.; Guibert, N.; Beau-Faller, M.; Validire, P.; Hofman, P.; Fouret, P. Specificities of Lung Adenocarcinoma in Women Who Have Never Smoked. J. Thorac. Oncol. 2013, 8, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Noh, J.; Sohn, J.; Cho, J.; Kang, D.R.; Joo, S.; Kim, C.; Shin, D.C. Residential radon and environmental burden of disease among Non-smokers. Ann. Occup. Environ. Med. 2016, 28, 12. [Google Scholar] [CrossRef] [PubMed]
- Rahal, Z.; El Nemr, S.; Sinjab, A.; Chami, H.; Tfayli, A.; Kadara, H. Smoking and Lung Cancer: A Geo-Regional Perspective. Front. Oncol. 2017, 7, 194. [Google Scholar] [CrossRef] [PubMed]
- Rivera, G.A.; Wakelee, H. Lung Cancer in Never Smokers. Adv. Exp. Med. Biol. 2016, 893, 43–57. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Espinoza-Mercado, F.; Liu, H.; Sata, N.; Cui, X.; Soukiasian, H.J. Current status of research and treatment for non-small cell lung cancer in never-smoking females. Cancer Biol. Ther. 2017, 18, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Chansky, K.; Detterbeck, F.C.; Nicholson, A.G.; Rusch, V.W.; Vallières, E.; Groome, P.; Kennedy, C.; Krasnik, M.; Peake, M.; Shemanski, L.; et al. The IASLC Lung Cancer Staging Project: External Validation of the Revision of the TNM Stage Groupings in the Eighth Edition of the TNM Classification of Lung Cancer. J. Thorac. Oncol. 2017, 12, 1109–1121. [Google Scholar] [CrossRef] [PubMed]
- Borczuk, A.C. Prognostic considerations of the new World Health Organization classification of lung adenocarcinoma. Eur. Respir. Rev. 2016, 25, 364–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, X.; Wang, L.; Liu, X.; Sun, X.; Yu, J.; Meng, X. Genetic characterization drives personalized therapy for early-stage non-small-cell lung cancer (NSCLC) patients and survivors with metachronous second primary tumor (MST): A case report. Medicine 2017, 96, e6221. [Google Scholar] [CrossRef] [PubMed]
- Levallet, G.; Dubois, F.; Fouret, P.; Antoine, M.; Brosseau, S.; Bergot, E.; Beau-Faller, M.; Gounant, V.; Brambilla, E.; Debieuvre, D.; et al. MSH2/BRCA1 expression as a DNA-repair signature predicting survival in early-stage lung cancer patients from the IFCT-0002 Phase 3 Trial. Oncotarget 2017, 8, 4313–4329. [Google Scholar] [CrossRef] [PubMed]
- Rakha, E.; Pajares, M.J.; Ilie, M.; Pio, R.; Echeveste, J.; Hughes, E.; Soomro, I.; Long, E.; Idoate, M.A.; Wagner, S.; et al. Stratification of resectable lung adenocarcinoma by molecular and pathological risk estimators. Eur. J. Cancer 2015, 51, 1897–1903. [Google Scholar] [CrossRef] [PubMed]
- Van Schil, P.E. Non-small cell lung cancer: The new T1 categories. F1000Research 2017, 6, 174. [Google Scholar] [CrossRef] [PubMed]
- Nagasaka, M.; Gadgeel, S.M. Role of chemotherapy and targeted therapy in early-stage non-small cell lung cancer. Expert Rev. Anticancer Ther. 2018, 18, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D. Sarcomatoid neoplasms of the lung and pleura. Arch. Pathol. Lab. Med. 2010, 134, 1645–1658. [Google Scholar] [CrossRef] [PubMed]
- Pécuchet, N.; Vieira, T.; Rabbe, N.; Antoine, M.; Blons, H.; Cadranel, J.; Laurent-Puig, P.; Wislez, M. Molecular classification of pulmonary sarcomatoid carcinomas suggests new therapeutic opportunities. Ann. Oncol. 2017, 28, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Vieira, T.; Antoine, M.; Hamard, C.; Fallet, V.; Duruisseaux, M.; Rabbe, N.; Rodenas, A.; Cadranel, J.; Wislez, M. Sarcomatoid lung carcinomas show high levels of programmed death ligand-1 (PD-L1) and strong immune-cell infiltration by TCD3 cells and macrophages. Lung Cancer 2016, 98, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farkas, D.H.; Drevon, A.M.; Kiechle, F.L.; DiCarlo, R.G.; Heath, E.M.; Crisan, D. Specimen stability for DNA-based diagnostic testing. Diagn. Mol. Pathol. 1996, 5, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Hubel, A.; Spindler, R.; Skubitz, A.P.N. Storage of human biospecimens: Selection of the optimal storage temperature. Biopreserv. Biobank. 2014, 12, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Ji, X.; Wang, M.; Li, L.; Chen, F.; Zhang, Y.; Li, Q.; Zhou, J. The Impact of Repeated Freeze-Thaw Cycles on the Quality of Biomolecules in Four Different Tissues. Biopreserv. Biobank. 2017, 15, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Cayuela, J.-M.; Mauté, C.; Fabre, A.-L.; Nibourel, O.; Dulucq, S.; Delabesse, E.; Villarèse, P.; Hayette, S.; Mozziconacci, M.-J.; Macintyre, E. GBMHM A novel method for room temperature distribution and conservation of RNA and DNA reference materials for guaranteeing performance of molecular diagnostics in onco-hematology: A GBMHM study. Clin. Biochem. 2015, 48, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Clermont, D.; Santoni, S.; Saker, S.; Gomard, M.; Gardais, E.; Bizet, C. Assessment of DNA encapsulation, a new room-temperature DNA storage method. Biopreserv. Biobank. 2014, 12, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Frippiat, C.; Noel, F. Efficiency of a novel forensic room-temperature DNA storage medium. Forensic Sci. Int. Genet. 2014, 9, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.B.; Clabaugh, K.C.; Silva, B.; Odigie, K.O.; Coble, M.D.; Loreille, O.; Scheible, M.; Fourney, R.M.; Stevens, J.; Carmody, G.R.; et al. Assessing a novel room temperature DNA storage medium for forensic biological samples. Forensic Sci. Int. Genet. 2012, 6, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Li, Q.; Wang, X.; Zhou, X.; He, X.; Liao, Q.; Zhu, F.; Cheng, L.; Zhang, Y. Evaluation of DNA/RNAshells for room temperature nucleic acids storage. Biopreserv. Biobank. 2015, 13, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Lou, J.J.; Mirsadraei, L.; Sanchez, D.E.; Wilson, R.W.; Shabihkhani, M.; Lucey, G.M.; Wei, B.; Singer, E.J.; Mareninov, S.; Yong, W.H. A review of room temperature storage of biospecimen tissue and nucleic acids for anatomic pathology laboratories and biorepositories. Clin. Biochem. 2014, 47, 267–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, R.; Betsou, F.; Barnes, M.G.; Harding, K.; Bonnet, J.; Kofanova, O.; Crowe, J.H.; International Society for Biological and Environmental Repositories (ISBER) Biospecimen Science Working Group. Preservation of Biospecimens at Ambient Temperature: Special Focus on Nucleic Acids and Opportunities for the Biobanking Community. Biopreserv. Biobank. 2016, 14, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.H.; Sahin, A.A.; Myers, J.N. Biobanking in Genomic Medicine. Arch. Pathol. Lab. Med. 2015, 139, 812–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bass, B.P.; Engel, K.B.; Greytak, S.R.; Moore, H.M. A review of preanalytical factors affecting molecular, protein, and morphological analysis of formalin-fixed, paraffin-embedded (FFPE) tissue: How well do you know your FFPE specimen? Arch. Pathol. Lab. Med. 2014, 138, 1520–1530. [Google Scholar] [CrossRef] [PubMed]
- Guyard, A.; Boyez, A.; Pujals, A.; Robe, C.; Tran Van Nhieu, J.; Allory, Y.; Moroch, J.; Georges, O.; Fournet, J.-C.; Zafrani, E.-S.; et al. DNA degrades during storage in formalin-fixed and paraffin-embedded tissue blocks. Virchows Arch. 2017, 471, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Hashida, S.; Yamamoto, H.; Matsubara, T.; Ohtsuka, T.; Suzawa, K.; Maki, Y.; Soh, J.; Asano, H.; Tsukuda, K.; et al. Estimation of age-related DNA degradation from formalin-fixed and paraffin-embedded tissue according to the extraction methods. Exp. Ther. Med. 2017, 14, 2683–2688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borman, A.M.; Linton, C.J.; Miles, S.-J.; Campbell, C.K.; Johnson, E.M. Ultra-rapid preparation of total genomic DNA from isolates of yeast and mould using Whatman FTA filter paper technology—A reusable DNA archiving system. Med. Mycol. 2006, 44, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Cohen, L.; Martinez, H.; Iverson, B.; Nunez, R. GenTegra RNA Preserves the Quality and Integrity of Purified RNA during Ambient Temperature Transport. Available online: http://integenx.com/wp-content/uploads/2013/03/gentegra-rna-preserves-the-quality-andintegrity-of-purified-rna-during-ambient-temperature-transport.pdf (accessed on 9 April 2018).
- Colotte, M.; Coudy, D.; Tuffet, S.; Bonnet, J. Adverse effect of air exposure on the stability of DNA stored at room temperature. Biopreserv. Biobank. 2011, 9, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, J.; Colotte, M.; Coudy, D.; Couallier, V.; Portier, J.; Morin, B.; Tuffet, S. Chain and conformation stability of solid-state DNA: Implications for room temperature storage. Nucleic Acids Res. 2010, 38, 1531–1546. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, N.V.; Kuzmina, M.L. Protocols for dry DNA storage and shipment at room temperature. Mol. Ecol. Resour. 2013, 13, 890–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nederhand, R.J.; Droog, S.; Kluft, C.; Simoons, M.L.; de Maat, M.P.M. Investigators of the EUROPA trial Logistics and quality control for DNA sampling in large multicenter studies. J. Thromb. Haemost. 2003, 1, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Röder, B.; Frühwirth, K.; Vogl, C.; Wagner, M.; Rossmanith, P. Impact of long-term storage on stability of standard DNA for nucleic acid-based methods. J. Clin. Microbiol. 2010, 48, 4260–4262. [Google Scholar] [CrossRef] [PubMed]
- Baker, M. Biorepositories: Building better biobanks. Nature 2012, 486, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Meredith, A.J.; Slotty, A.; Matzke, L.; Babinszky, S.; Watson, P.H. A Model to Estimate Frozen Tissue Collection Targets in Biobanks to Support Cancer Research. Biopreserv. Biobank. 2015, 13, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Wan, E.; Akana, M.; Pons, J.; Chen, J.; Musone, S.; Kwok, P.-Y.; Liao, W. Green technologies for room temperature nucleic acid storage. Curr. Issues Mol. Biol. 2010, 12, 135–142. [Google Scholar] [PubMed]
- Ciaburri, M.; Napolitano, M.; Bravo, E. Business Planning in Biobanking: How to Implement a Tool for Sustainability. Biopreserv. Biobank. 2017, 15, 46–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doucet, M.; Yuille, M.; Georghiou, L.; Dagher, G. Biobank sustainability: Current status and future prospects. J. Biorepository Sci. Appl. Med. 2017, 5, 1–7. [Google Scholar] [CrossRef]
- Vaught, J.; Rogers, J.; Carolin, T.; Compton, C. Biobankonomics: Developing a sustainable business model approach for the formation of a human tissue biobank. J. Natl. Cancer Inst. Monogr. 2011, 2011, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Yuille, M.M.; Feller, P.I.; Georghiou, L.; Laredo, P.; Welch, E.W. Financial Sustainability of Biobanks: From Theory to Practice. Biopreserv. Biobank. 2017, 15, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. WHO Panel The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Fabre, A.-L.; Colotte, M.; Luis, A.; Tuffet, S.; Bonnet, J. An efficient method for long-term room temperature storage of RNA. Eur. J. Hum. Genet. 2014, 22, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wang, X.; Liu, X.; Liao, Q.; Sun, J.; He, X.; Yang, T.; Yin, J.; Jia, J.; Li, X.; et al. Long-Term Room Temperature Storage of Dry Ribonucleic Acid for Use in RNA-Seq Analysis. Biopreserv. Biobank. 2017, 15, 502–511. [Google Scholar] [CrossRef] [PubMed]
- Seelenfreund, E.; Robinson, W.A.; Amato, C.M.; Tan, A.-C.; Kim, J.; Robinson, S.E. Long term storage of dry versus frozen RNA for next generation molecular studies. PLoS ONE 2014, 9, e111827. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Age (Years) | |
| Mean (range) | 62 (36–82) |
| Sex | |
| Male | 72 (55%) |
| Female | 60 (45%) |
| Tumor Size (cm) | |
| Mean (range) | 3.5 (1–9) |
| pTNM Stage | |
| I | 42 (32%) |
| II | 61 (46%) |
| III | 30 (23%) |
| IV | 9 (7%) |
| Histological Subtype | |
| Adenocarcinoma | 117 (87%) |
| Squamous cell carcinoma | 8 (6%) |
| Other | 7 (7%) |
| Mutational Status | |
| EGFR mutation | 26 (20%) |
| ALK rearrangement | 15 (11%) |
| ROS1 rearrangement | 5 (4%) |
| BRAF mutation | 5 (4%) |
| Variables | n (%) |
|---|---|
| Age (Years) | |
| Mean (range) | 67 (38–81) |
| Sex | |
| Male | 525 (71%) |
| Female | 213 (29%) |
| Smoking Status | |
| Current | 631 (85%) |
| Former | 107 (15%) |
| Tumor Size (cm) | |
| Mean (range) | 3.5 (1-5.5) |
| pTNM Stage | |
| Ia | 37 (5%) |
| Ib | 146 (20%) |
| Ic | 160 (21%) |
| IIa | 203 (28%) |
| IIb | 192 (26%) |
| Histological Subtype | |
| Adenocarcinoma | 461 (62%) |
| Squamous cell carcinoma | 196 (27%) |
| Other | 81 (11%) |
| Follow-Up 2 Years after Surgery | |
| Metastasis | 28 (3%) |
| Death related to lung cancer | 27 (3%) |
| Follow-Up 5 Years after Surgery | |
| Metastasis | 99 (12%) |
| Death related to lung cancer | 68 (8%) |
| Variables | n (%) |
|---|---|
| Age (Years) | |
| Mean (range) | 68 (41–79) |
| Sex | |
| Male | 80 (68%) |
| Female | 37 (22%) |
| Tobacco Status | |
| Current/former | 95 (81%) |
| Former | 22 (19%) |
| Tumor Size (cm) | |
| Mean (range) | 4.2 (2.3–9) |
| pTNM stage | |
| I | 12 (%) |
| II | 55 (%) |
| III | 35 (%) |
| IV | 15 (%) |
| Histological Subatype | 37 (32%) |
| Pleomorphic carcinoma | 35 (30%) |
| Spindle cell carcinoma | 26 (22%) |
| Giant cell carcinoma | 8 (7%) |
| Carcinosarcoma | 6 (5%) |
| Pulmonary blastoma | 5 (4%) |
| DNA Storage at Room Temperature | Frozen DNA Storage | ||
|---|---|---|---|
| DNA Shells | DNA Stabilization Matrices | DNA Cards | |
| Dried DNA stored encapsulated in minicapsules. | Dried DNA stored in tubes. | Dried DNA stored in cards. | DNA stored in water or low concentrated TE buffer at −80 °C. |
| Chemical Stability | |||
| Solid state reduces chemical reactivity and limits hydrolysis and oxidation. Encapsulation completely protects DNA from moisture and oxygen. Long DNA fragments and a broad range of DNA amount can be stored. | Solid state reduces chemical reactivity and limits hydrolysis and oxidation. Trace amounts of DNA can be stored BUT DNA is exposed to atmospheric influences. Moisture and temperature have to be controlled. | Solid state reduces chemical reactivity and limits hydrolysis and oxidation. BUT DNA is exposed to atmospheric influences. Moisture and temperature have to be controlled. | Reduced chemical reactivity due to reduced storage temperature BUT Storage in aqueous solution potentially allows hydrolysis and oxidation. |
| Storage | |||
| Energy saving and automation friendly Standalone storage system. | Energy saving and automation friendly. Standalone storage system. | Energy saving and automation friendly. Standalone storage system. | Storage devices are usually already available BUT Energy consuming and high-maintenance devices are needed. Backup systems need to be provided and maintained. |
| Sample Shipment | |||
| Samples can easily be shipped. | Samples can easily be shipped but moisture should be controlled if long transportation time is expected. | Samples can easily be shipped but moisture should be controlled if long transportation time is expected. | Shipment is complicated and risky as the low temperature has to be maintained during shipment. |
| Handling | |||
| Easy and quantitative recovery possible BUT Dehydration and encapsulation have to be performed by external service providers and initial costs are high. | Easy and quantitative recovery possible. DNA drying can be easily performed at the customer lab without additional devices needed BUT Special tubes are needed and storage location has to be controlled for temperature and moisture. | DNA preservation can easily be performed at the customer lab without additional devices needed. BUT Quantitative recovery is not possible and storage location has to be controlled for temperature and moisture. | Normal and cheap cryotubes can be used for storage and freezing of DNA is quite easy BUT The protocol is not adapted to trace amounts of DNA and sample concentrates over time due to sublimation of storage buffer. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Washetine, K.; Kara-Borni, M.; Heeke, S.; Bonnetaud, C.; Félix, J.-M.; Ribeyre, L.; Bence, C.; Ilié, M.; Bordone, O.; Pedro, M.; et al. Ensuring the Safety and Security of Frozen Lung Cancer Tissue Collections through the Encapsulation of Dried DNA. Cancers 2018, 10, 195. https://doi.org/10.3390/cancers10060195
Washetine K, Kara-Borni M, Heeke S, Bonnetaud C, Félix J-M, Ribeyre L, Bence C, Ilié M, Bordone O, Pedro M, et al. Ensuring the Safety and Security of Frozen Lung Cancer Tissue Collections through the Encapsulation of Dried DNA. Cancers. 2018; 10(6):195. https://doi.org/10.3390/cancers10060195
Chicago/Turabian StyleWashetine, Kevin, Mehdi Kara-Borni, Simon Heeke, Christelle Bonnetaud, Jean-Marc Félix, Lydia Ribeyre, Coraline Bence, Marius Ilié, Olivier Bordone, Marine Pedro, and et al. 2018. "Ensuring the Safety and Security of Frozen Lung Cancer Tissue Collections through the Encapsulation of Dried DNA" Cancers 10, no. 6: 195. https://doi.org/10.3390/cancers10060195