Assessing Cachexia Acutely after Autologous Stem Cell Transplant


Abstract
:1. Introduction
2. Results
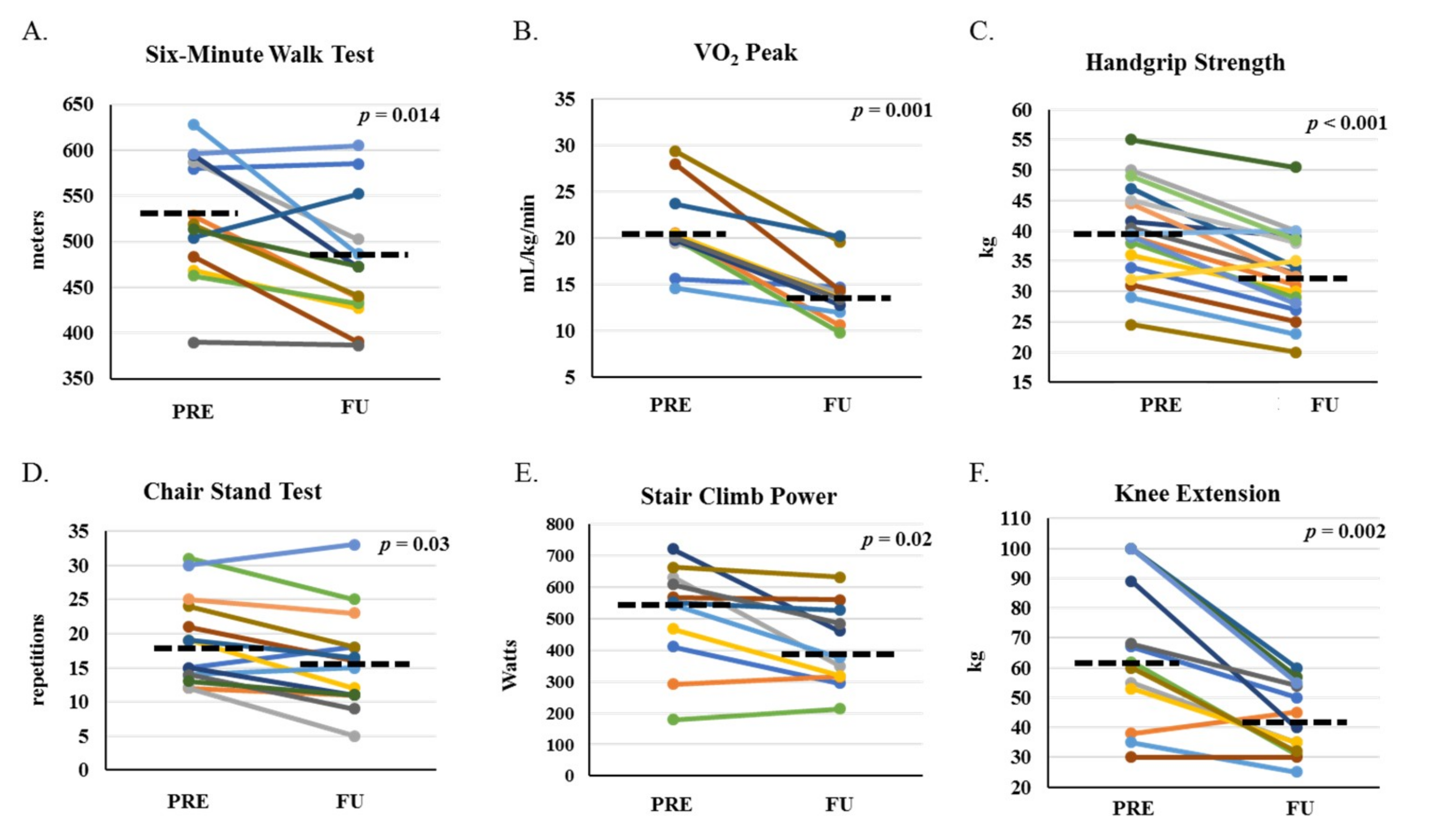
2.1. Physical Function
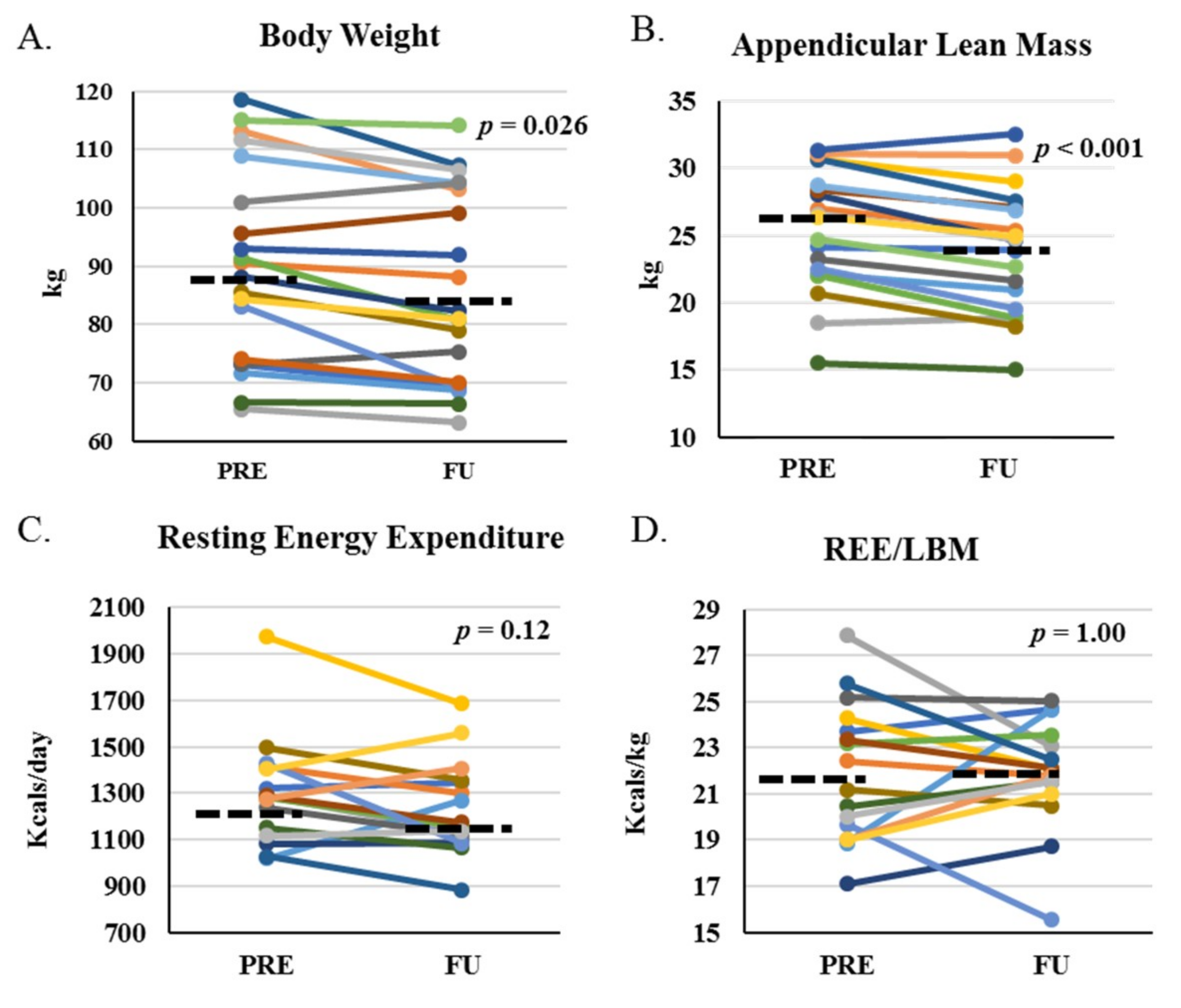
2.2. Body Composition and Energy Expenditure
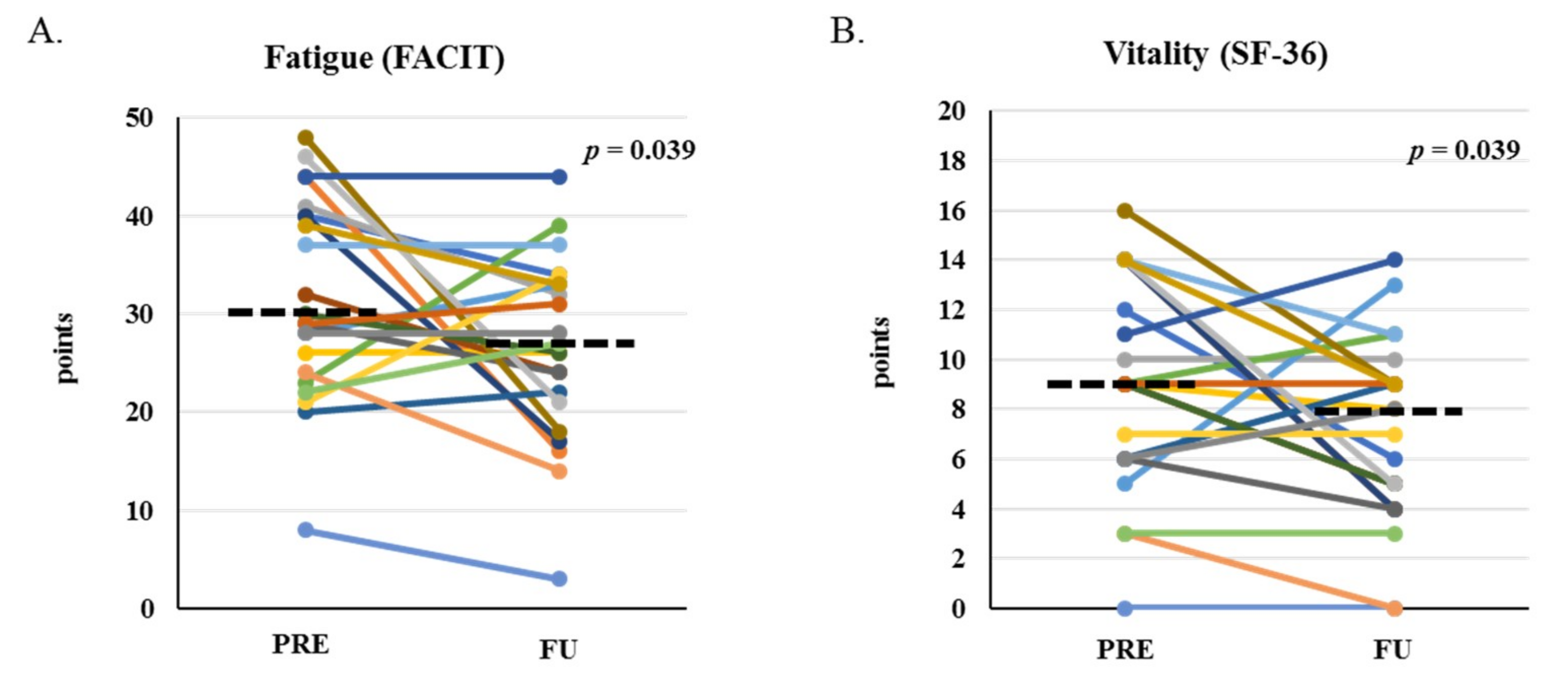
2.3. Patient-Reported Outcomes
2.4. Biomarkers
2.5. Regression
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Study Design and Protocol
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Niederwieser, D.; Baldomero, H.; Szer, J.; Gratwohl, M.; Aljurf, M.; Atsuta, Y.; Bouzas, L.F.; Confer, D.; Greinix, H.; Horowitz, M.; et al. Hematopoietic stem cell transplantation activity worldwide in 2012 and a SWOT analysis of the Worldwide Network for Blood and Marrow Transplantation Group including the global survey. Bone Marrow Transplant. 2016, 51, 778–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danaher, E.H.; Ferrans, C.; Verlen, E.; Ravandi, F.; van Besien, K.; Gelms, J.; Dieterle, N. Fatigue and physical activity in patients undergoing hematopoietic stem cell transplant. Oncol. Nurs. Forum. 2006, 33, 614–624. [Google Scholar] [PubMed]
- Fukushima, T.; Nakano, J.; Ishii, S.; Natsuzako, A.; Hirase, T.; Sakamoto, J.; Okita, M. Characteristics of muscle function and the effect of cachexia in patients with haematological malignancy. Eur. J. Cancer Care 2018, e12956. [Google Scholar] [CrossRef] [PubMed]
- Hung, Y.C.; Bauer, J.; Horsley, P.; Waterhouse, M.; Bashford, J.; Isenring, E. Changes in nutritional status, body composition, quality of life, and physical activity levels of cancer patients undergoing autologous peripheral blood stem cell transplantation. Supportive Care in Cancer. 2013, 21, 1579–1586. [Google Scholar] [CrossRef] [PubMed]
- Burney, B.O.; Hayes, T.G.; Smiechowska, J.; Cardwell, G.; Papusha, V.; Bhargava, P.; Konda, B.; Auchus, R.J.; Garcia, J.M. Low testosterone levels and increased inflammatory markers in patients with cancer and relationship with cachexia. J. Clin. Endocrinol. Metab. 2012, 97, E700–E709. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, E.; Hui, D.; Nooruddin, Z.I.; Dalal, S.; Dev, R.; Freer, G.; Roberts, L.; Palmer, J.L.; Bruera, E. Associations among hypogonadism, C-reactive protein, symptom burden, and survival in male cancer patients with cachexia: A preliminary report. J. Pain Symptom Manage. 2010, 39, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.M.; Li, H.; Mann, D.; Epner, D.; Hayes, T.G.; Marcelli, M.; Cunningham, G.R. Hypogonadism in male patients with cancer. Cancer 2006, 106, 2583–2591. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Crouch, R. Minimal clinically important difference for change in 6-minute walk test distance of adults with pathology: A systematic review. J. Eval. Clin. Pract. 2017, 23, 377–381. [Google Scholar] [CrossRef]
- Jatoi, A.; Daly, B.D.; Hughes, V.A.; Dallal, G.E.; Kehayias, J.; Roubenoff, R. Do patients with nonmetastatic non-small cell lung cancer demonstrate altered resting energy expenditure? Ann. Thorac. Surg. 2001, 72, 348–351. [Google Scholar] [CrossRef]
- Garcia, J.M.; Garcia-Touza, M.; Hijazi, R.A.; Taffet, G.; Epner, D.; Mann, D.; Smith, R.G.; Cunningham, G.R.; Marcelli, M. Active ghrelin levels and active to total ghrelin ratio in cancer-induced cachexia. J. Clin. Endocrinol. Metab. 2005, 90, 2920–2926. [Google Scholar] [CrossRef]
- Gagnon, B.; Murphy, J.; Jelowicki, M.; Morris, D.V. The effect of severe androgen deficiency on physical function in male patients with cancer. J. Pain Symptom Manage. 2013, 45, 892–900. [Google Scholar] [CrossRef] [PubMed]
- Veterans and Agent Orange: Update 2014. Mil. Med. 2017, 182, 1619–1620. [CrossRef] [PubMed] [Green Version]
- Zullig, L.L.; Sims, K.J.; McNeil, R.; Williams, C.D.; Jackson, G.L.; Provenzale, D.; Kelley, M.J. Cancer Incidence Among Patients of the U.S. Veterans Affairs Health Care System: 2010 Update. Mil. Med. 2017, 182, e1883–e1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morishita, S.; Kaida, K.; Yamauchi, S.; Wakasugi, T.; Ikegame, K.; Ogawa, H.; Domen, K. Relationship of physical activity with physical function and health-related quality of life in patients having undergone allogeneic haematopoietic stem-cell transplantation. Eur. J. Cancer Care. 2017, 26. [Google Scholar] [CrossRef] [PubMed]
- Wiskemann, J.; Dreger, P.; Schwerdtfeger, R.; Bondong, A.; Huber, G.; Kleindienst, N.; Ulrich, C.M.; Bohus, M. Effects of a partly self-administered exercise program before, during, and after allogeneic stem cell transplantation. Blood 2011, 117, 2604–2613. [Google Scholar] [CrossRef] [PubMed]
- Rothe, D.; Cox-Kennett, N.; Buijs, D.M.; Venner, C.P.; Paterson, D.I.; Gyenes, G.T.; Pituskin, E. Cardiac Rehabilitation in Patients with Lymphoma Undergoing Autologous Hematopoietic Stem Cell Transplantation: A Cardio-oncology Pilot Project. Can. J. Cardiol. 2018, 34, S263–S269. [Google Scholar] [CrossRef] [PubMed]
- Chetta, A.; Zanini, A.; Pisi, G.; Aiello, M.; Tzani, P.; Neri, M.; Olivieri, D. Reference values for the 6-min walk test in healthy subjects 20–50 years old. Respir. Med. 2006, 100, 1573–1578. [Google Scholar] [CrossRef] [PubMed]
- Hacker, E.D.; Collins, E.; Park, C.; Peters, T.; Patel, P.; Rondelli, D. Strength Training to Enhance Early Recovery after Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant 2017, 23, 659–669. [Google Scholar] [CrossRef] [Green Version]
- Jarden, M.; Baadsgaard, M.T.; Hovgaard, D.J.; Boesen, E.; Adamsen, L. The effect of a multimodal intervention on treatment-related symptoms in patients undergoing hematopoietic stem cell transplantation: A randomized controlled trial. J. Pain Symptom Manage 2009, 38, 174–190. [Google Scholar] [CrossRef]
- Stephens, N.A.; Gray, C.; MacDonald, A.J.; Tan, B.H.; Gallagher, I.J.; Skipworth, R.J.; Ross, J.A.; Fearon, K.C.; Greig, C.A. Sexual dimorphism modulates the impact of cancer cachexia on lower limb muscle mass and function. Clin. Nutr. 2012, 31, 499–505. [Google Scholar] [CrossRef]
- de Lima, F.D.; Bottaro, M.; de Oliveira, V.R.; Cruz, L.; Battaglini, C.L.; Vieira, C.A.; de Oliveira, R.J. Cancer-Related Fatigue and Muscle Quality in Hodgkin’s Lymphoma Survivors. Integr. Cancer Ther. 2018, 17, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.J.; Albrecht, E.D.; Garcia, J.M. Update on Management of Cancer-Related Cachexia. Curr. Oncol. Rep. 2017, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Crawford, E.D.; Heidenreich, A.; Lawrentschuk, N.; Tombal, B.; Pompeo, A.C.L.; Mendoza-Valdes, A.; Miller, K.; Debruyne, F.M.J.; Klotz, L. Androgen-targeted therapy in men with prostate cancer: Evolving practice and future considerations. Prostate Cancer Prostatic Dis. 2019, 22, 24–38. [Google Scholar] [CrossRef] [PubMed]
- Fredrix, E.W.; Soeters, P.B.; Wouters, E.F.; Deerenberg, I.M.; von Meyenfeldt, M.F.; Saris, W.H. Effect of different tumor types on resting energy expenditure. Cancer Res. 1991, 51, 6138–6141. [Google Scholar] [PubMed]
- Elia, M. Organ. and tissue contribution to metabolic rate. In Energy Metabolism: Tissue Determinants and Cellular Corollaries; Kinney, J.M., Tucker, H.N., Eds.; Raven Press: New York, NY, USA, 1992. [Google Scholar]
- Wang, X.S.; Shi, Q.; Shah, N.D.; Heijnen, C.J.; Cohen, E.N.; Reuben, J.M.; Orlowski, R.Z.; Qazilbash, M.H.; Johnson, V.E.; Williams, L.A. Inflammatory markers and development of symptom burden in patients with multiple myeloma during autologous stem cell transplantation. Clin. Cancer Res. 2014, 20, 1366–1374. [Google Scholar] [CrossRef]
- Wang, X.S.; Shi, Q.; Williams, L.A.; Cleeland, C.S.; Mobley, G.M.; Reuben, J.M.; Lee, B.N.; Giralt, S.A. Serum interleukin-6 predicts the development of multiple symptoms at nadir of allogeneic hematopoietic stem cell transplantation. Cancer 2008, 113, 2102–2109. [Google Scholar] [CrossRef] [Green Version]
- Falconer, J.S.; Fearon, K.C.; Plester, C.E.; Ross, J.A.; Carter, D.C. Cytokines, the acute-phase response, and resting energy expenditure in cachectic patients with pancreatic cancer. Ann. Surg. 1994, 219, 325–331. [Google Scholar] [CrossRef]
- Argilés, J.M.; Fontes-Oliveira, C.C.; Toledo, M.; López-Soriano, J.F.; Busquets, S. Cachexia: A problem of energetic inefficiency. J. Cachexia Sarcopenia Muscle. 2014, 5, 279–286. [Google Scholar]
- Pereira, R.M.; de Carvalho, J.F. Glucocorticoid-induced myopathy. Joint Bone Spine. 2011, 78, 41–44. [Google Scholar] [CrossRef]
- Manni, A.; Pardridge, W.M.; Cefalu, W.; Nisula, B.C.; Bardin, C.W.; Santner, S.J.; Santen, R.J. Bioavailability of albumin-bound testosterone. J. Clin. Endocrinol. Metab. 1985, 61, 705–710. [Google Scholar] [CrossRef]
- Orio, F.; Muscogiuri, G.; Palomba, S.; Serio, B.; Sessa, M.; Giudice, V.; Ferrara, I.; Tauchmanovà, L.; Colao, A.; Selleri, C. Endocrinopathies after allogeneic and autologous transplantation of hematopoietic stem cells. ScientificWorldJournal 2014, 2014, 282147. [Google Scholar] [CrossRef] [PubMed]
- Gharwan, H.; Neary, N.M.; Link, M.; Hsieh, M.M.; Fitzhugh, C.D.; Sherins, R.J.; Tisdale, J.F. Successful fertility restoration after allogeneic hematopoietic stem cell transplantation. Endocr Pract. 2014, 20, e157–e161. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Chemaitilly, W.; Chen, M.; Chow, E.J.; Duncan, C.N.; Jones, L.W.; Pulsipher, M.A.; Remaley, A.T.; Rovo, A.; Salooja, N. National Institutes of Health Hematopoietic Cell Transplantation Late Effects Initiative: The Cardiovascular Disease and Associated Risk Factors Working Group Report. Biol Blood Marrow Transplant. 2017, 23, 201–210. [Google Scholar] [CrossRef] [PubMed]
- DeFilipp, Z.; Duarte, R.F.; Snowden, J.A.; Majhail, N.S.; Greenfield, D.M.; Miranda, J.L.; Arat, M.; Baker, K.S.; Burns, L.J.; Duncan, C.N.; et al. Metabolic Syndrome and Cardiovascular Disease after Hematopoietic Cell Transplantation: Screening and Preventive Practice Recommendations from the CIBMTR and EBMT. Biol Blood Marrow Transplant. 2016, 22, 1493–1503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFilipp, Z.; Troschel, F.M.; Qualls, D.A.; Li, S.; Kuklinski, M.W.; Kempner, M.E.; Hochberg, E.; Chen, Y.B.; El-Jawahri, A.; Fintelmann, F.J. Evolution of Body Composition Following Autologous and Allogeneic Hematopoietic Cell Transplantation: Incidence of Sarcopenia and Association with Clinical Outcomes. Biol Blood Marrow Transplant. 2018, 24, 1741–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eston, R.G.; Williams, J.G. Reliability of ratings of perceived effort regulation of exercise intensity. Br. J. Sports Med. 1988, 22, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Vandewalle, H.; Pérès, G.; Monod, H. Standard anaerobic exercise tests. Sports Med. 1987, 4, 268–289. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Arena, R. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2014; p. 96. [Google Scholar]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Feurer, I.D.; Crosby, L.O.; Buzby, G.P.; Rosato, E.F.; Mullen, J.L. Resting energy expenditure in morbid obesity. Ann. Surg. 1983, 197, 17–21. [Google Scholar] [CrossRef]
- Palmer, J.L.; Fisch, M.J. Association between symptom distress and survival in outpatients seen in a palliative care cancer center. J. Pain Symptom Manage. 2005, 29, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Butt, Z.; Lai, J.S.; Rao, D.; Allen, W.H.; Bill, A.; Cella, D. Measurement of fatigue in cancer, stroke, and HIV using the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) scale. J. Psychosom Res. 2013, 74, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.R.; Henry, J.D. The positive and negative affect schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2004, 43, 245–265. [Google Scholar] [CrossRef] [PubMed]
- Salaffi, F.; Stancati, A.; Silvestri, C.A.; Ciapetti, A.; Grassi, W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur. J. Pain. 2004, 8, 283–291. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- McQuellon, R.P.; Russell, G.B.; Cella, D.F.; Craven, B.L.; Brady, M.; Bonomi, A.; Hurd, D.D. Quality of life measurement in bone marrow transplantation: Development of the Functional Assessment of Cancer Therapy-Bone Marrow Transplant (FACT-BMT) scale. Bone Marrow Transplant. 1997, 19, 357–368. [Google Scholar] [CrossRef]
- Topolski, T.D.; LoGerfo, J.; Patrick, D.L.; Williams, B.; Walwick, J.; Patrick, M.B. The Rapid Assessment of Physical Activity (RAPA) among older adults. Prev. Chronic Dis. 2006, 3, A118. [Google Scholar]
- Harrington, L.B.; Marck, B.T.; Wiggins, K.L.; McKnight, B.; Heckbert, S.R.; Woods, N.F.; LaCroix, A.Z.; Blondon, M.; Psaty, B.M.; Rosendaal, F.R. Cross-sectional association of endogenous steroid hormone, sex hormone-binding globulin, and precursor steroid levels with hemostatic factor levels in postmenopausal women. J. Thromb Haemost. 2017, 15, 80–90. [Google Scholar] [CrossRef]
- Vermeulen, A.; Verdonck, L.; Kaufman, J.M. A critical evaluation of simple methods for the estimation of free testosterone in serum. J. Clin. Endocrinol. Metab. 1999, 84, 3666–3672. [Google Scholar] [CrossRef]
- Gremeaux, V.; Iskandar, M.; Kervio, G.; Deley, G.; Pérénnou, D.; Casillas, J.M. Comparative analysis of oxygen uptake in elderly subjects performing two walk tests: The six-minute walk test and the 200-m fast walk test. Clin. Rehabil. 2008, 22, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.S.; Hui, D.; Bruera, E.; Janku, F.; Naing, A.; Falchook, G.S.; Piha-Paul, S.; Wheler, J.J.; Fu, S.; Tsimberidou, A.M.; et al. MABp1, a first-in-class true human antibody targeting interleukin-1alpha in refractory cancers: An open-label, phase 1 dose-escalation and expansion study. Lancet Oncol. 2014, 15, 656–666. [Google Scholar] [CrossRef]
- Dobs, A.S.; Boccia, R.V.; Croot, C.C.; Gabrail, N.Y.; Dalton, J.T.; Hancock, M.L.; Johnston, M.A.; Steiner, M.S. Effects of enobosarm on muscle wasting and physical function in patients with cancer: A double-blind, randomised controlled phase 2 trial. Lancet Oncol. 2013, 14, 335–345. [Google Scholar] [CrossRef]
- Stewart, C.A.J.; Ho, G.F.; Prabhash, K.; von Haehling, S.; Tilson, J.; Brown, R.; Beadle, J.; Anker, S.D.; for and on behalf of the ACT-ONE study group. Espindolol for the treatment and prevention of cachexia in patients with stage III/IV non-small cell lung cancer or colorectal cancer: A randomized, double-blind, placebo-controlled, international multicentre phase II study (the ACT-ONE trial). J. Cachexia Sarcopenia Muscle. 2016, 7, 355–365. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 21 | Med (95% CI) |
|---|---|
| Age (yr) | 68 (57, 68) |
| Ht (cm) | 174.6 (170.4, 178.0) |
| Wt (kg) | 88.7 (83.6, 100.7) |
| BMI (kg/m2) | 28.3 (27.8, 32.3) |
| ASMI (kg/m2) | 8.6 (8.0, 9.1) |
| HCT-CI range (0–7) a | 3.0 (1.9, 3.9) |
| N (%) | |
| Men | 19 (90.5) |
| Ethnicity | |
| White Non-Hispanic | 13 (61.9) |
| White Hispanic | 1 (4.8) |
| Black | 3 (14.3) |
| Asian/Pacific Islander | 2 (9.5) |
| Mixed | 2 (9.5) |
| Diagnosis | |
| Multiple Myeloma | 15 (71.4) |
| T-cell Lymphoma | 1 (4.8) |
| Hodgkin Lymphoma | 1 (4.8) |
| B-cell non-Hodgkin Lymphoma | 4 (19.0) |
| Recent chemotherapy exposure (y) b | |
| Alkylating Agents | 2 (9.5) |
| Topoisomerase Inhibitors | 6 (28.6) |
| Immunomodulators | 6 (28.6) |
| Proteasome Inhibitors | 7 (33.3) |
| None | 10 (47.6) |
| Glucocorticoid exposure (y) c | 10 (47.6) |
| Med (95% CI) | Absolute Change | Relative Change | p-Value a |
|---|---|---|---|
| Physical Function | |||
| 6MWT (m) | −40.8 (−85.8, −11.8) | −8.3 (−15.3, −2.3) | 0.014 |
| HGS (kg) | −6.5 (−8.2, −3.5) | −16.7 (−20.2, −8.6) | 0.001 |
| SCP (W) | −73.7 (−186.0, −19.7) | −17.1 (−31.6, −0.8) | 0.024 |
| CST (reps) | −3.0 (−5.1, −0.4) | −17.4 (−29.1, −1.7) | 0.025 |
| KE (kg) | −20.0 (−3.5, −10.9) | −36.4 (−46.4, −16.4) | 0.002 |
| KF (kg) | −15.0 (−21.4, −5.0) | −22.4 (−31.4, −7.6) | 0.005 |
| HE (kg) | −4.5 (−11.8, −0.4) | −13.0 (−29.7, −3.7) | 0.038 |
| VO2 peak (mL/kg/min) | −6.7 (−8.8, −3.6) | −33.3 (−41.0, −18.1) | 0.001 |
| Body Composition | |||
| BW (kg) | −3.9 (−6.3, −2.0) | −4.2 (−6.6, −2.2) | 0.001 |
| LBM (kg) | −2.9 (−4.0, −1.0) | −4.9 (−6.7, −1.6) | 0.002 |
| ALM (kg) | −1.6 (−2.1, −0.9) | −6.1 (−8.6, −3.6) | <0.001 |
| ASMI (kg/m2) | −0.5 (−0.7, −0.3) | −6.0 (−8.7, −3.6) | 0.001 |
| FM (kg) | −0.7 (−1.5, −0.1) | −2.3 (−7.1, −0.4) | 0.02 |
| PBF (%) | 0.5 (−0.6, 0.8) | n/a | 0.78 |
| Energy Expenditure | |||
| REE (kcals/d) | −113 (−148,18) | −8.4 (−11, 2) | 0.12 |
| REE (% predicted) | −1.5 (−6.1, 3.9) | n/a | 0.64 |
| RQ (VCO2/VO2) | −0.04 (−0.08, 0.02) | −4.1 (−8.5, 2.5) | 0.22 |
| REE/LBM (kcals/kg) | 0.1 (−1.5, 1.4) | 0.5 (−6.1, 7.6) | 1.00 |
| REE/ALM (kcals/kg) | 1.6 (−2.9, 4.1) | 2.8 (−4.8, 9.4) | 0.56 |
| Biomarkers | |||
| IL−6 (pg/mL) | 0.26 (−1.67, 1.61) | 13.7 (−12.3, 154.2) | 0.33 |
| TNF (pg/mL) | 0.65 (−0.37, 1.71) | 52.4 (8.0, 109.0) | 0.09 |
| TT (ng/mL) b | 1.3 (0.3, 1.9) | 25.3 (19.5, 107.5) | 0.02 |
| cBT (ng/dL) b | −35.4 (−51.2, 8.1) | −13.3 (−26.9, 29.6) | 0.16 |
| SHBG (nmol/L) b | 41.2 (22.8, 44.1) | 122.8 (79.3, 145.9) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anderson, L.J.; Yin, C.; Burciaga, R.; Lee, J.; Crabtree, S.; Migula, D.; Geiss-Wessel, K.; Liu, H.M.; Graf, S.A.; Chauncey, T.R.; et al. Assessing Cachexia Acutely after Autologous Stem Cell Transplant. Cancers 2019, 11, 1300. https://doi.org/10.3390/cancers11091300
Anderson LJ, Yin C, Burciaga R, Lee J, Crabtree S, Migula D, Geiss-Wessel K, Liu HM, Graf SA, Chauncey TR, et al. Assessing Cachexia Acutely after Autologous Stem Cell Transplant. Cancers. 2019; 11(9):1300. https://doi.org/10.3390/cancers11091300
Chicago/Turabian StyleAnderson, Lindsey J., Chelsea Yin, Raul Burciaga, Jonathan Lee, Stephanie Crabtree, Dorota Migula, Kelsey Geiss-Wessel, Haiming M. Liu, Solomon A. Graf, Thomas R. Chauncey, and et al. 2019. "Assessing Cachexia Acutely after Autologous Stem Cell Transplant" Cancers 11, no. 9: 1300. https://doi.org/10.3390/cancers11091300