Impact of Use of Gastric-Acid Suppressants and Oral Anti-Cancer Agents on Survival Outcomes: A Systematic Review and Meta-Analysis

 ,
, 
 ,
, 
Abstract
1. Introduction
2. Results
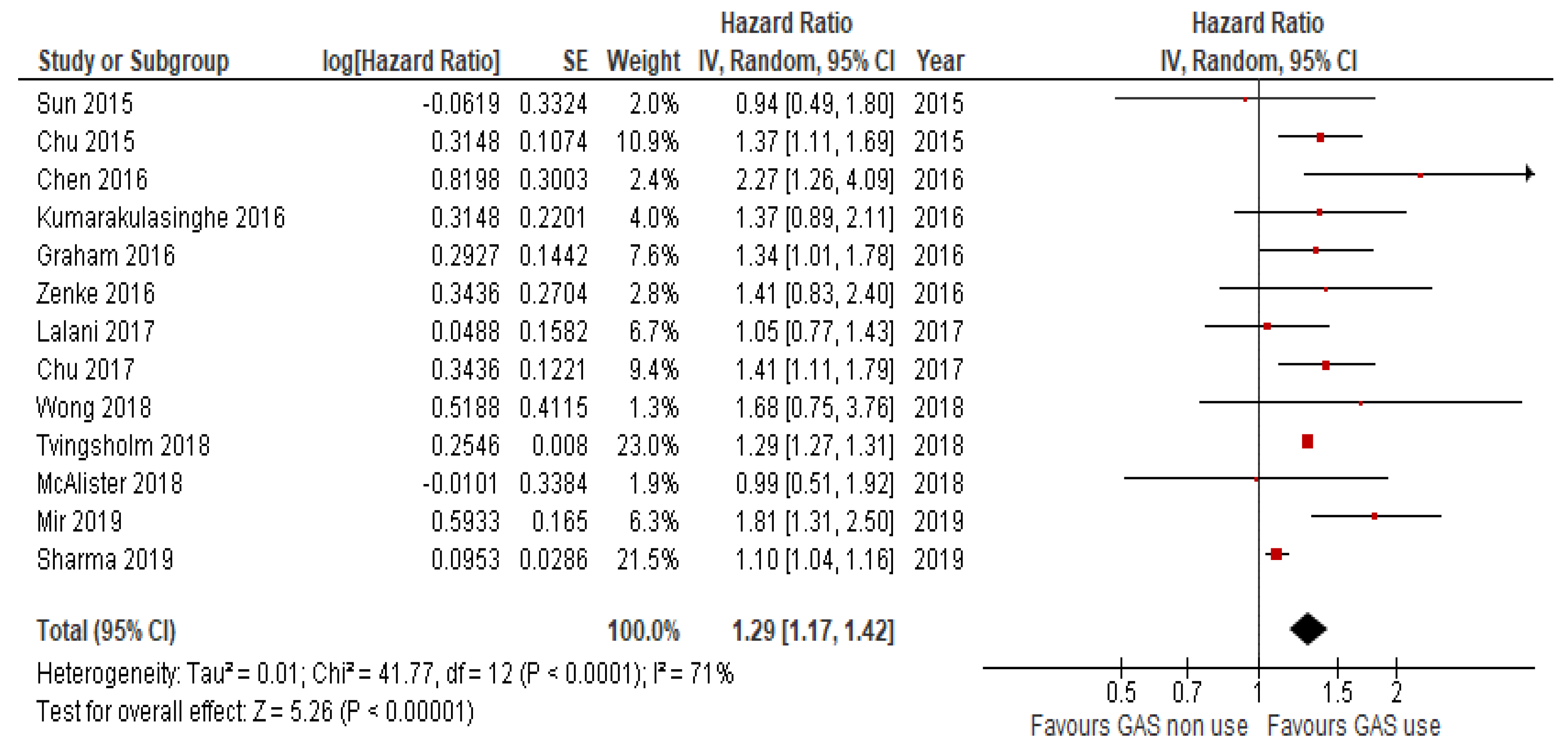
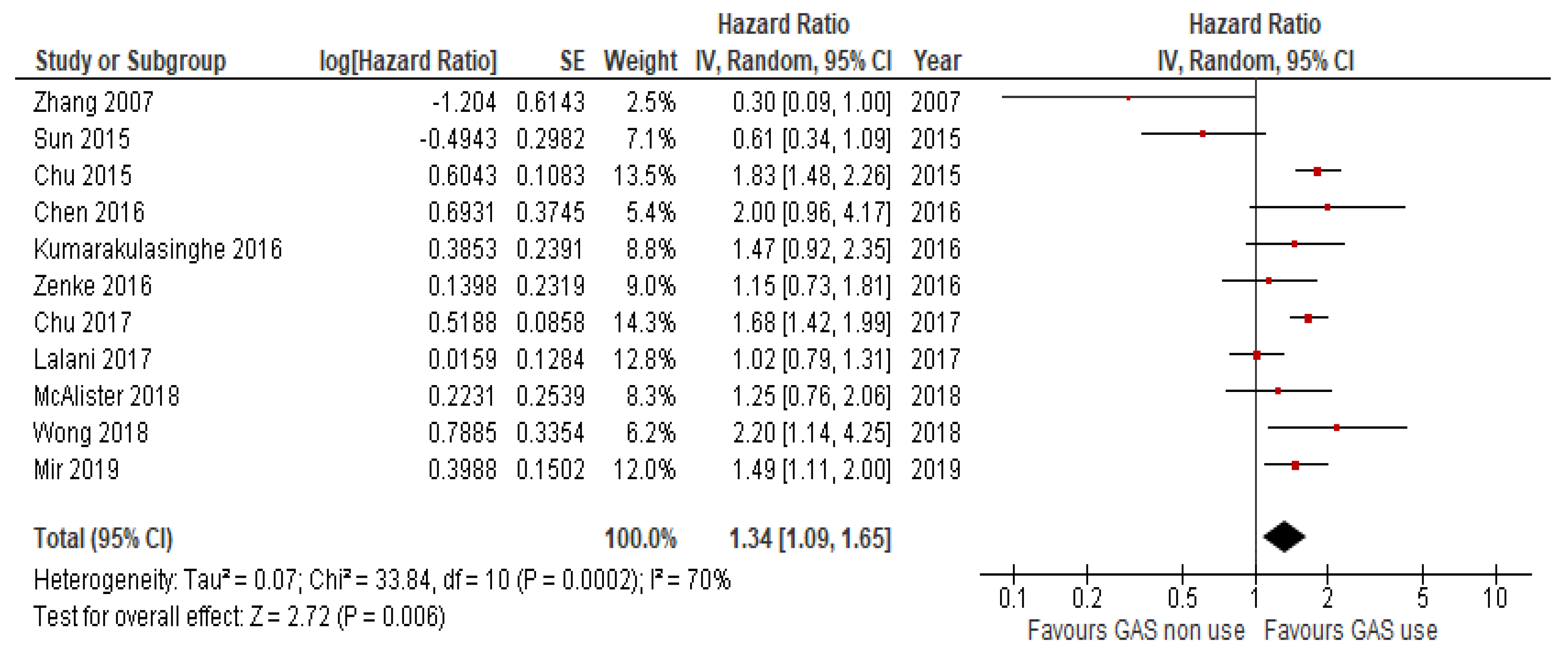
2.1. Overall Survival and Progression-Free Survival with GAS vs. no GAS
2.2. Subgroup Analysis
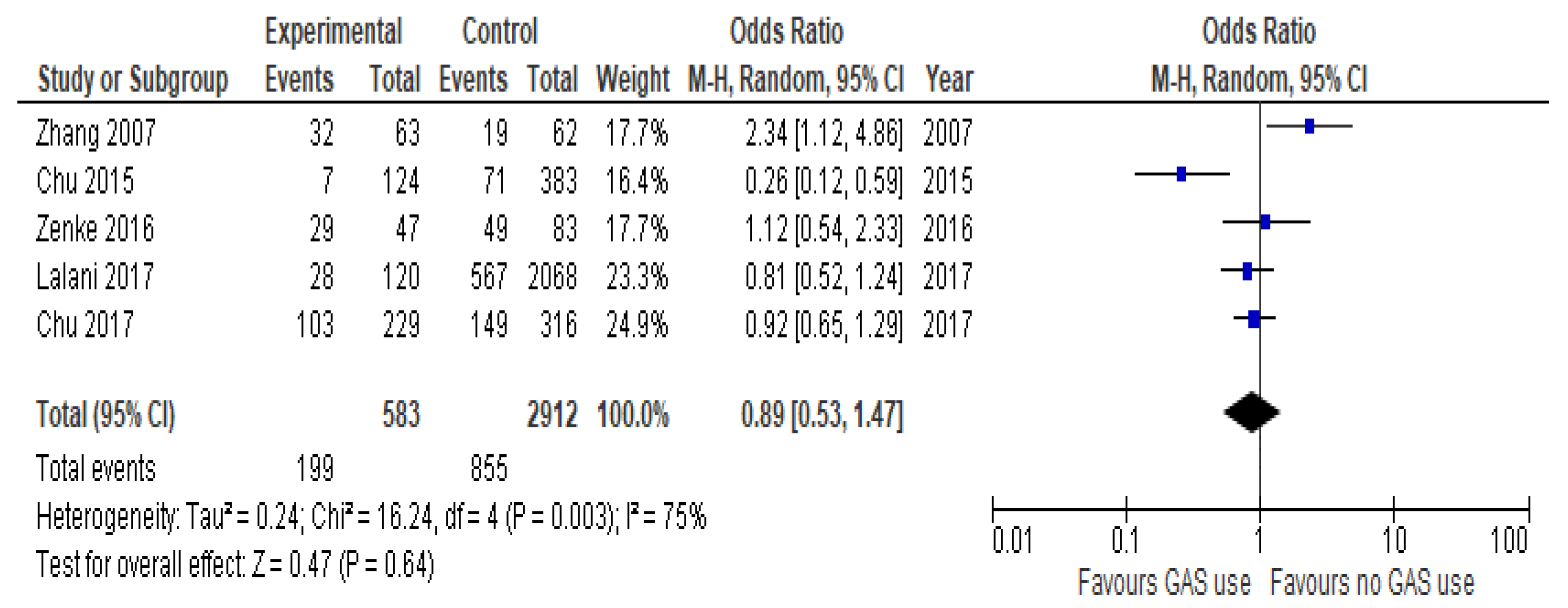
2.3. Overall Response Rate
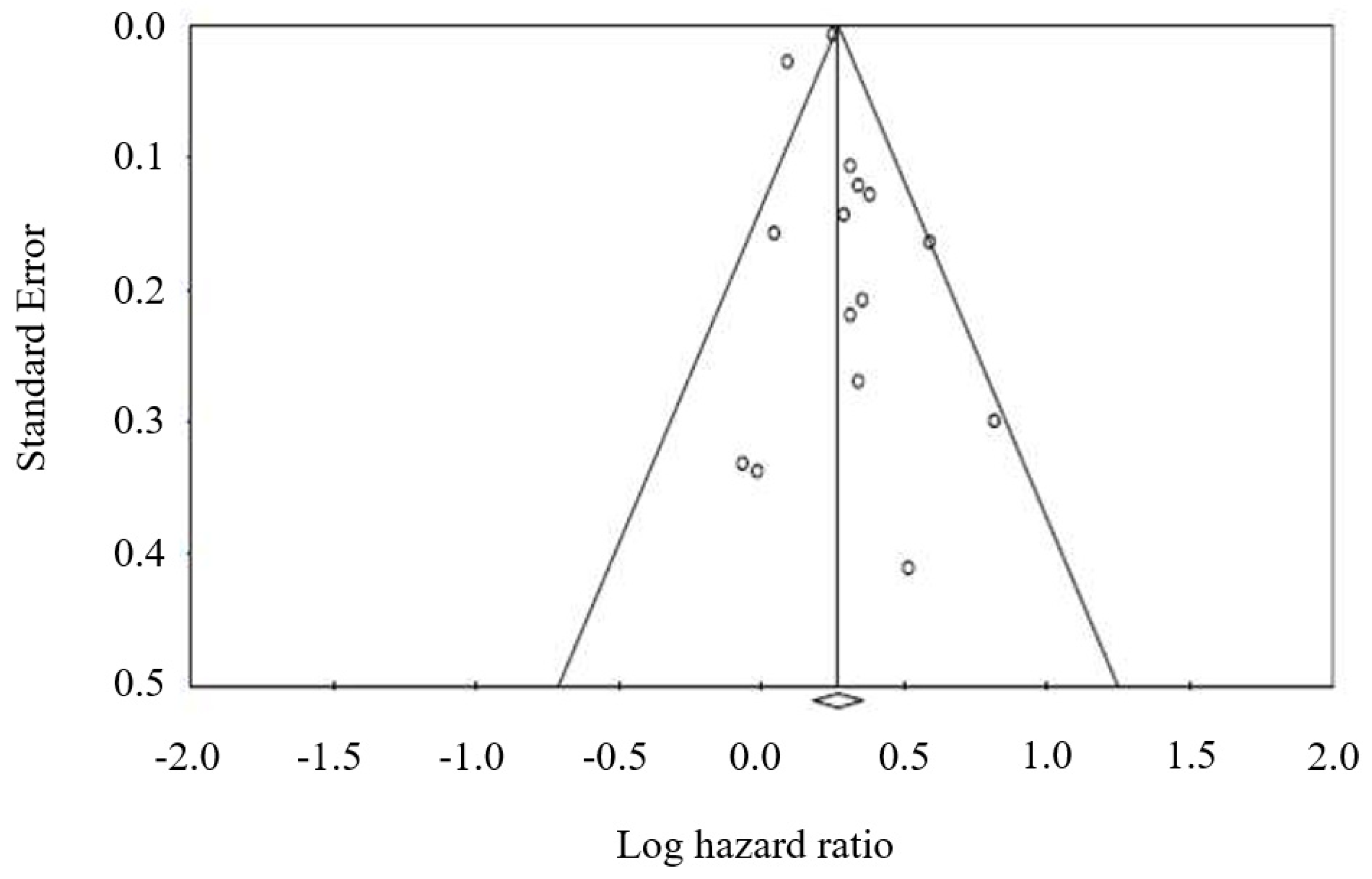
2.4. Publication Bias
3. Discussion
4. Materials and Methods
4.1. Data Extraction and Quality Assessment
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kaye, S.B. New antimetabolites in cancer chemotherapy and their clinical impact. Br. J. Cancer 1998, 78 (Suppl. 3), 1–7. [Google Scholar] [CrossRef]
- Marty, M.; Extra, J.M.; Espie, M.; Leandri, S.; Besenval, M.; Krikorian, A. Advances in vinca-alkaloids: Navelbine. Nouv Rev. Fr. d’Hematol. 1989, 31, 77–84. [Google Scholar]
- O’Reilly, S.M.; Newlands, E.S.; Glaser, M.G.; Brampton, M.; Rice-Edwards, J.M.; Illingworth, R.D.; Richards, P.G.; Kennard, C.; Colquhoun, I.R.; Lewis, P.; et al. Temozolomide: A new oral cytotoxic chemotherapeutic agent with promising activity against primary brain tumours. Eur. J. Cancer 1993, 29A, 940–942. [Google Scholar] [CrossRef]
- Hutson, T.E.; Lesovoy, V.; Al-Shukri, S.; Stus, V.P.; Lipatov, O.N.; Bair, A.H.; Rosbrook, B.; Chen, C.; Kim, S.; Vogelzang, N.J. Axitinib versus sorafenib as first-line therapy in patients with metastatic renal-cell carcinoma: A randomised open-label phase 3 trial. Lancet Oncol. 2013, 14, 1287–1294. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Davis, I.D.; Mardiak, J.; Szczylik, C.; Lee, E.; Wagstaff, J.; Barrios, C.H.; Salman, P.; Gladkov, O.A.; Kavina, A.; et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: Results of a randomized phase III trial. J. Clin. Oncol. 2010, 28, 1061–1068. [Google Scholar] [CrossRef]
- Van der Graaf, W.T.; Blay, J.Y.; Chawla, S.P.; Kim, D.W.; Bui-Nguyen, B.; Casali, P.G.; Schoffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- Savarino, V.; Dulbecco, P.; De Bortoli, N.; Ottonello, A.; Savarino, E. The appropriate use of proton pump inhibitors (PPIs): Need for a reappraisal. Eur. J. Intern. Med. 2017, 37, 19–24. [Google Scholar] [CrossRef]
- Ohgami, M.; Kaburagi, T.; Kurosawa, A.; Doki, K.; Shiozawa, T.; Hizawa, N.; Homma, M. Effects of Proton Pump Inhibitor Coadministration on the Plasma Concentration of Erlotinib in Patients With Non-Small Cell Lung Cancer. Ther. Drug Monit. 2018, 40, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Vishwanathan, K.; Dickinson, P.A.; Bui, K.; Cassier, P.A.; Greystoke, A.; Lisbon, E.; Moreno, V.; So, K.; Thomas, K.; Weilert, D.; et al. The Effect of Food or Omeprazole on the Pharmacokinetics of Osimertinib in Patients With Non-Small-Cell Lung Cancer and in Healthy Volunteers. J. Clin. Pharmacol. 2018, 58, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Budha, N.R.; Frymoyer, A.; Smelick, G.S.; Jin, J.Y.; Yago, M.R.; Dresser, M.J.; Holden, S.N.; Benet, L.Z.; Ware, J.A. Drug absorption interactions between oral targeted anticancer agents and PPIs: Is pH-dependent solubility the Achilles heel of targeted therapy? Clin. Pharmacol. Ther. 2012, 92, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Suttle, A.B.; Ball, H.A.; Molimard, M.; Hutson, T.E.; Carpenter, C.; Rajagopalan, D.; Lin, Y.; Swann, S.; Amado, R.; Pandite, L. Relationships between pazopanib exposure and clinical safety and efficacy in patients with advanced renal cell carcinoma. Br. J. Cancer 2014, 111, 1909–1916. [Google Scholar] [CrossRef]
- Verheijen, R.B.; Swart, L.E.; Beijnen, J.H.; Schellens, J.H.M.; Huitema, A.D.R.; Steeghs, N. Exposure-survival analyses of pazopanib in renal cell carcinoma and soft tissue sarcoma patients: Opportunities for dose optimization. Cancer Chemother. Pharmacol. 2017, 80, 1171–1178. [Google Scholar] [CrossRef]
- Lalani, A.A.; McKay, R.R.; Lin, X.; Simantov, R.; Kaymakcalan, M.D.; Choueiri, T.K. Proton Pump Inhibitors and Survival Outcomes in Patients With Metastatic Renal Cell Carcinoma. Clin. Genitourin. Cancer 2017, 15, 724–732. [Google Scholar] [CrossRef]
- Mir, O.; Touati, N.; Lia, M.; Litiere, S.; Le Cesne, A.; Sleijfer, S.; Blay, J.Y.; Leahy, M.; Young, R.; Mathijssen, R.H.J.; et al. Impact of Concomitant Administration of Gastric Acid-Suppressive Agents and Pazopanib on Outcomes in Soft-Tissue Sarcoma Patients Treated within the EORTC 62043/62072 Trials. Clin. Cancer Res. 2019, 25, 1479–1485. [Google Scholar] [CrossRef]
- Chen, Y.M.; Lai, C.H.; Chang, H.C.; Chao, T.Y.; Tseng, C.C.; Fang, W.F.; Wang, C.C.; Chung, Y.H.; Wang, Y.H.; Su, M.C.; et al. Antacid Use and De Novo Brain Metastases in Patients with Epidermal Growth Factor Receptor-Mutant Non-Small Cell Lung Cancer Who Were Treated Using First-Line First-Generation Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors. PLoS ONE 2016, 11, e0149722. [Google Scholar] [CrossRef]
- Chu, M.P.; Ghosh, S.; Chambers, C.R.; Basappa, N.; Butts, C.A.; Chu, Q.; Fenton, D.; Joy, A.A.; Sangha, R.; Smylie, M.; et al. Gastric Acid suppression is associated with decreased erlotinib efficacy in non-small-cell lung cancer. Clin. Lung Cancer 2015, 16, 33–39. [Google Scholar] [CrossRef]
- Chu, M.P.; Hecht, J.R.; Slamon, D.; Wainberg, Z.A.; Bang, Y.J.; Hoff, P.M.; Sobrero, A.; Qin, S.; Afenjar, K.; Houe, V.; et al. Association of Proton Pump Inhibitors and Capecitabine Efficacy in Advanced Gastroesophageal Cancer: Secondary Analysis of the TRIO-013/LOGiC Randomized Clinical Trial. JAMA Oncol. 2017, 3, 767–773. [Google Scholar] [CrossRef]
- Fang, Y.H.; Yang, Y.H.; Hsieh, M.J.; Hung, M.S.; Lin, Y.C. Concurrent proton-pump inhibitors increase risk of death for lung cancer patients receiving 1st-line gefitinib treatment—A nationwide population-based study. Cancer Manag Res. 2019, 11, 8539–8546. [Google Scholar] [CrossRef] [PubMed]
- Graham, C.; Orr, C.; Bricks, C.S.; Hopman, W.M.; Hammad, N.; Ramjeesingh, R. A retrospective analysis of the role of proton pump inhibitors in colorectal cancer disease survival. Curr. Oncol. 2016, 23, e583–e588. [Google Scholar] [CrossRef] [PubMed]
- Ha, V.H.; Ngo, M.; Chu, M.P.; Ghosh, S.; Sawyer, M.B.; Chambers, C.R. Does gastric acid suppression affect sunitinib efficacy in patients with advanced or metastatic renal cell cancer? J. Oncol. Pharm. Pract. 2015, 21, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Kumarakulasinghe, N.B.; Syn, N.; Soon, Y.Y.; Asmat, A.; Zheng, H.; Loy, E.Y.; Pang, B.; Soo, R.A. EGFR kinase inhibitors and gastric acid suppressants in EGFR-mutant NSCLC: A retrospective database analysis of potential drug interaction. Oncotarget 2016, 7, 85542–85550. [Google Scholar] [CrossRef][Green Version]
- McAlister, R.K.; Aston, J.; Pollack, M.; Du, L.; Koyama, T.; Chism, D.D. Effect of Concomitant pH-Elevating Medications with Pazopanib on Progression-Free Survival and Overall Survival in Patients with Metastatic Renal Cell Carcinoma. Oncologist 2018, 23, 686–692. [Google Scholar] [CrossRef]
- Sharma, M.; Holmes, H.M.; Mehta, H.B.; Chen, H.; Aparasu, R.R.; Shih, Y.T.; Giordano, S.H.; Johnson, M.L. The concomitant use of tyrosine kinase inhibitors and proton pump inhibitors: Prevalence, predictors, and impact on survival and discontinuation of therapy in older adults with cancer. Cancer 2019, 125, 1155–1162. [Google Scholar] [CrossRef]
- Sun, J.; Ilich, A.I.; Kim, C.A.; Chu, M.P.; Wong, G.G.; Ghosh, S.; Danilak, M.; Mulder, K.E.; Spratlin, J.L.; Chambers, C.R.; et al. Concomitant Administration of Proton Pump Inhibitors and Capecitabine is Associated With Increased Recurrence Risk in Early Stage Colorectal Cancer Patients. Clin. Colorectal. Cancer 2016, 15, 257–263. [Google Scholar] [CrossRef]
- Tvingsholm, S.A.; Dehlendorff, C.; Osterlind, K.; Friis, S.; Jaattela, M. Proton pump inhibitor use and cancer mortality. Int. J. Cancer 2018, 143, 1315–1326. [Google Scholar] [CrossRef]
- Wong, G.G.; Ha, V.; Chu, M.P.; Dersch-Mills, D.; Ghosh, S.; Chambers, C.R.; Sawyer, M.B. Effects of Proton Pump Inhibitors on FOLFOX and CapeOx Regimens in Colorectal Cancer. Clin. Colorectal. Cancer 2019, 18, 72–79. [Google Scholar] [CrossRef]
- Zenke, Y.; Yoh, K.; Matsumoto, S.; Umemura, S.; Niho, S.; Ohmatsu, H.; Goto, K.; Ohe, Y. Clinical Impact of Gastric Acid-Suppressing Medication Use on the Efficacy of Erlotinib and Gefitinib in Patients with Advanced Non-Small-Cell Lung Cancer Harboring EGFR Mutations. Clin. Lung Cancer 2016, 17, 412–418. [Google Scholar] [CrossRef]
- Zhang, J.L.; Liu, M.; Yang, Q.; Lin, S.Y.; Shan, H.B.; Wang, H.Y.; Xu, G.L. Effects of omeprazole in improving concurrent chemoradiotherapy efficacy in rectal cancer. World J. Gastroenterol. 2017, 23, 2575–2584. [Google Scholar] [CrossRef]
- Targownik, L.E.; Metge, C.; Roos, L.; Leung, S. The prevalence of and the clinical and demographic characteristics associated with high-intensity proton pump inhibitor use. Am. J. Gastroenterol. 2007, 102, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Corleto, V.D.; Festa, S.; Di Giulio, E.; Annibale, B. Proton pump inhibitor therapy and potential long-term harm. Curr. Opin. Endocrinol. Diabetes Obes. 2014, 21, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Egorin, M.J.; Shah, D.D.; Christner, S.M.; Yerk, M.A.; Komazec, K.A.; Appleman, L.R.; Redner, R.L.; Miller, B.M.; Beumer, J.H. Effect of a proton pump inhibitor on the pharmacokinetics of imatinib. Br. J. Clin. Pharmacol. 2009, 68, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Hilton, J.F.; Tu, D.; Seymour, L.; Shepherd, F.A.; Bradbury, P.A. An evaluation of the possible interaction of gastric acid suppressing medication and the EGFR tyrosine kinase inhibitor erlotinib. Lung Cancer 2013, 82, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, R.W.; Peric, R.; Hussaarts, K.G.; Kienhuis, E.; NS, I.J.; De Bruijn, P.; Van der Leest, C.; Codrington, H.; Kloover, J.S.; Van der Holt, B.; et al. Influence of the Acidic Beverage Cola on the Absorption of Erlotinib in Patients With Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 34, 1309–1314. [Google Scholar] [CrossRef]
- Xu, Z.Y.; Li, J.L. Comparative review of drug-drug interactions with epidermal growth factor receptor tyrosine kinase inhibitors for the treatment of non-small-cell lung cancer. Onco Targets Ther. 2019, 12, 5467–5484. [Google Scholar] [CrossRef]
- Cho, S.; Yee, J.; Kim, J.Y.; Jeong Rhie, S.; Gwak, H.S. Effects of Concomitant Medication Use on Gefitinib-Induced Hepatotoxicity. J. Clin. Pharmacol. 2018, 58, 263–268. [Google Scholar] [CrossRef]
- Togashi, Y.; Masago, K.; Masuda, S.; Mizuno, T.; Fukudo, M.; Ikemi, Y.; Sakamori, Y.; Nagai, H.; Kim, Y.H.; Katsura, T.; et al. Cerebrospinal fluid concentration of gefitinib and erlotinib in patients with non-small cell lung cancer. Cancer Chemother. Pharmacol. 2012, 70, 399–405. [Google Scholar] [CrossRef]
- Deng, Y.; Feng, W.; Wu, J.; Chen, Z.; Tang, Y.; Zhang, H.; Liang, J.; Xian, H.; Zhang, S. The concentration of erlotinib in the cerebrospinal fluid of patients with brain metastasis from non-small-cell lung cancer. Mol. Clin. Oncol. 2014, 2, 116–120. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2015, 25, 603–605. [Google Scholar]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Principal Institution(s) Involved | Study Design | Study Period | Number of Patients | Patients’ Disease Characteristics | Oral Anti-cancer Drug | Type of GAS |
|---|---|---|---|---|---|---|---|
| Ha, 2014 [23] | Cross Cancer Institute, Department of Oncology, Edmonton, Alberta, Canada | retrospective | 2006–2013 | 383 | mRCC | Sunitinib | PPI |
| Sun, 2016 [27] | Cross Cancer Institute, Department of Oncology, Edmonton, Alberta, Canada | retrospective | 2008–2012 | 298 | Early stage CRC | Capecitabine | PPI |
| Chu, 2015 [19] | Cross Cancer Institute, Department of Oncology, Edmonton, Alberta, Canada | retrospective | 2007–2012 | 507 | EGFR mutant advanced NSCLC | Erlotinib | PPI, H2RA |
| Zenke, 2016 [30] | Department of Thoracic Oncology, National Cancer Center Hospital East, Kashiwa, Japan | retrospective | 2008–2011 | 130 | EGFR mutant advanced NSCLC | Gefitinib Erlotinib | PPI, H2RA |
| Kumarakulasinghe, 2016 [24] | Department of Haematology-Oncology, National University Cancer Institute, Singapore | retrospective | 2008–2013 | 157 | EGFR mutant advanced NSCLC | Gefitinib Erlotinib | PPI, H2RA |
| Chen, 2016 [18] | Chang Gung Memorial Hospital-Kaohsiung Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan | retrospective | 2010–2013 | 269 | EGFR mutant advanced NSCLC | EGFR TKIs NOS | PPI |
| Graham, 2016 [21] | Department of Oncology, Cancer Centre of Southeastern Ontario, Queen’s University, Kingston | retrospective | 2005–2011 | 117 | CRC | NA | PPI |
| Chu, 2017 [20] | Cross Cancer Institute, Department of Oncology, Edmonton, Alberta, Canada | retrospective analysis (phase III trial) | 2008–2012 | 545 | GEJC | Capecitabine | PPI |
| Zhang, 2017 [31] | Guangdong Medical University Affiliated Longhua Central Hospital, Shenzhen, China | retrospective | 2008–2016 | 125 | CRC | Capecitabine | PPI |
| Lalani, 2017 [16] | Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, USA | pooled analysis (phase II/III studies) | 2003–2013 | 2188 | mRCC | Sunitinib Axitinib Sorafenib | PPI |
| McAlister, 2018 [25] | Vanderbilt-Ingram Cancer Center, Nashville, USA | retrospective | 2010–2015 | 90 | mRCC | Pazopanib | PPI, H2RA |
| Tvingsholm, 2018 [28] | Danish Cancer Society Research Center, Copenhagen, Denmark (Danish Cancer Registry) | retrospective | 1995–2011 | 353,071 | Solid Tumors (Danish Cancer Registry) | NA | PPI |
| Wong, 2019 [29] | Cross Cancer Institute, Department of Oncology, Edmonton, Alberta, Canada | retrospective | 2004–2013 | 389 | stage II-III CRC | Capecitabine | PPI |
| Fang, 2019 [21] | Chang Gung Memorial Hospital, Chiayi Branch, Puzi City, Chiayi County, Taiwan | retrospective | 1997–2013 | 1278 | EGFR mutant advanced NSCLC | Gefitinib | PPI |
| Mir, 2019 [17] | Gustave Roussy, Sarcoma Group, Villejuif, France | retrospective | 2005–2007 2008–2010 | 333 | STS | Pazopanib | PPI, H2RA |
| Sharma, 2019 [26] | The University of Mississippi, Oxford, Mississippi, USA (SEER Database) | retrospective | 2007–2012 | 12,538 | Solid Tumors (SEER Database) | TKIs | PPI |
| Authors, Year | Median Follow-Up, Months | Criteria for Overlapping between GAS and Anti-cancer Treatment (Time Overlapping %) | Therapeutic Approach, n (%) | ORR | OS HR (95% CI) * | PFS HR (95% CI) * | Type of Analysis | Quality NOS Score |
|---|---|---|---|---|---|---|---|---|
| Ha, 2014 [23] | NA | GAS: 45 (20%) | NA | 1.43 (0.95–2.15) | 1.36 (0.92–2.01) | UVA | 5 | |
| 100 | No GAS: 186 (80%) | NA | ||||||
| Sun, 2016 [27] | NA | GAS: 77 (26%) | NA | 0.94 (0.49–1.78) | 0.61 (0.34–1.08) | MVA | 5 | |
| Any PPI prescription | No GAS: 202 (74%) | NA | ||||||
| Chu, 2015 [19] | NA | GAS: 124 (25%) | 5.6% | 1.37 (1.11–1.69) | 1.83 (1.48–2.25) | MVA | 6 | |
| ≥20 | No GAS: 383 (75%) | 18.5% | ||||||
| Zenke, 2016 [30] | 36 (10.1–85.2) | GAS: 47 (36%) | 64% | 1.41 (0.83–2.35) | 1.15 (0.73–1.79) | MVA | 7 | |
| PPI/H2RA sequentially or concurrently to anti-EGFR | No GAS: 83 (64%) | 63% | ||||||
| Kumarakulasinghe, 2016 [24] | 50 | GAS: 55 (35%) | NA | 1.37 (0.89–2.12) | 1.47 (0.92–2.35) | MVA | 7 | |
| ≥30 | No GAS: 102 (65%) | NA | ||||||
| Chen, 2016 [18] | 24.5 | GAS: 57 (21%) | NA | 2.27 (1.26–4.11) | 2.00 (0.96–4.17) | MVA | 6 | |
| ≥30 | No GAS: 212 (79%) | NA | ||||||
| Graham, 2016 [21] | NA | GAS: 117 (9%) | NA | 1.34 (1.01–1.79) | NA | MVA | 7 | |
| NA | No GAS: 1187 (91%) | NA | ||||||
| Chu, 2017 [20] | NA | GAS: 119 (44%) | 36% | 1.41 (1.11–1.71) | 1.68 (1.42–1.94) | MVA | 5 | |
| ≥20 | No GAS: 155 (56%) | 42% | ||||||
| Zhang, 2017 [31] | 66 | GAS: 29 (23%) | 52.2% | 0.30 (0.09–0.99) | 0.37 (0.11–1.23) * | UVA *, MVA | 7 | |
| ≥200 mg PPI | No GAS: 96 (77%) | 36.5% | ||||||
| Lalani, 2017 [16] | NA | GAS: 120 (5%) | 23.3% | 1.05 (0.77–1.44) | 1.02 (0.79–1.30) | MVA | 5 | |
| ≥1 dose PPI | No GAS: 2068(95%) | 27.4% | ||||||
| McAlister, 2018 [25] | NA | GAS: 66 (73%) | NA | 0.99 (0.51–1.93) | 1.25 (0.76–2.07) | MVA | 5 | |
| ≥90 days | No GAS: 24 (27%) | NA | ||||||
| Tvingsholm, 2018 [28] | 1.52 (0.50–3.89) | GAS: 41,218 (11.7%) | NA | 1.29 (1.27–1.31) | NA | MVA | 7 | |
| ≥2 prescriptions within 6 months | No GAS: 311,853 (88.3%) | NA | ||||||
| Wong, 2019 [29] | NA | GAS: 50 (23.4%) | NA | 1.68 (0.75–3.80) | 2.20 (1.14–4.25) | MVA | 5 | |
| Any time PPI during capecitabine | No GAS: 164 (76.6%) | NA | ||||||
| Fang, 2019 [21] | NA | GAS: 309 (24%) | NA | 1.67 (1.33–2.09) | 0.99 (0.80–1.23) | MVA | 7 | |
| ≥20 | No GAS: 969 (76%) | NA | ||||||
| Mir, 2019 [17] | 27.6 (22.9–35.4) | GAS: 59 (18%) | NA | 1.81 (1.31–2.49) | 1.49 (1.11–1.99) | MVA | 6 | |
| ≥80 | No GAS: 273 (82%) | NA | ||||||
| Sharma, 2019 [26] | NA | GAS: 2843 (22.7%) | NA | 1.10 (1.04–1.17) | NA | MVA | 8 | |
| ≥30 days within 3 months | No GAS: 9695 (77.3%) | NA |
| Item No | Recommendation | Reported on Page No |
|---|---|---|
| Reporting of background should include | ||
| 1 | Problem definition | 1,2 |
| 2 | Hypothesis statement | 1,2 |
| 3 | Description of study outcome(s) | 11 |
| 4 | Type of exposure or intervention used | 11 |
| 5 | Type of study designs used | 11 |
| 6 | Study population | 11 |
| Reporting of search strategy should include | ||
| 7 | Qualifications of searchers (e.g., librarians and investigators) | 1 |
| 8 | Search strategy, including time period included in the synthesis and key words | 11 |
| 9 | Effort to include all available studies, including contact with authors | 11 |
| 10 | Databases and registries searched | 11 |
| 11 | Search software used, name and version, including special features used (e.g., explosion) | 11 |
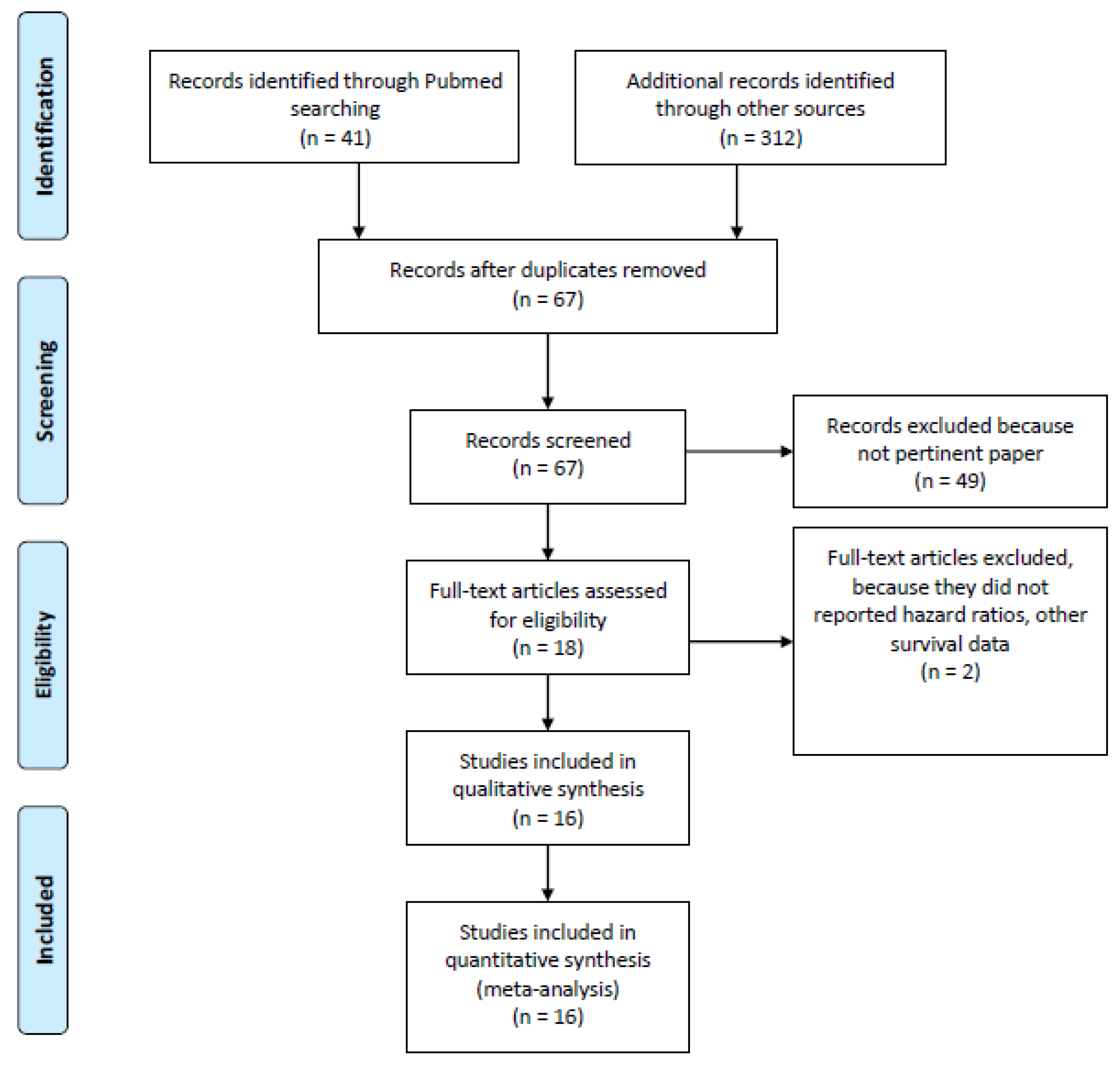
| 12 | Use of hand searching (e.g., reference lists of obtained articles) | 11, Figure 1 |
| 13 | List of citations located and those excluded, including justification | 11, Figure 1 |
| 14 | Method of addressing articles published in languages other than English | 11 |
| 15 | Method of handling abstracts and unpublished studies | 11 |
| 16 | Description of any contact with authors | 11 |
| Reporting of methods should include | ||
| 17 | Description of relevance or appropriateness of studies assembled for assessing the hypothesis to be tested | 11 |
| 18 | Rationale for the selection and coding of data (e.g., sound clinical principles or convenience) | 11 |
| 19 | Documentation of how data were classified and coded (e.g., multiple raters, blinding and interrater reliability) | 11 |
| 20 | Assessment of confounding (e.g., comparability of cases and controls in studies where appropriate) | 11 |
| 21 | Assessment of study quality, including blinding of quality assessors, stratification or regression on possible predictors of study results | 11 |
| 22 | Assessment of heterogeneity | 7,8, Figure 5 |
| 23 | Description of statistical methods (e.g., complete description of fixed or random effects models, justification of whether the chosen models account for predictors of study results, dose-response models, or cumulative meta-analysis) in sufficient detail to be replicated | 12 |
| 24 | Provision of appropriate tables and graphics | Figure 1 |
| Reporting of results should include | ||
| 25 | Graphic summarizing individual study estimates and overall estimate | Table 1 and Table 2 |
| 26 | Table giving descriptive information for each study included | Table 1 and Table 2 |
| 27 | Results of sensitivity testing (e.g., subgroup analysis) | 2, 6–8, Figure 2, Figure 3 and Figure 4 |
| 28 | Indication of statistical uncertainty of findings | 7,8, Figure 5 |
| 29 | Quantitative assessment of bias (e.g., publication bias) | 7,8, Figure 5 |
| 30 | Justification for exclusion (e.g., exclusion of non-English language citations) | Figure 1, 11 |
| 31 | Assessment of quality of included studies | 11 |
| Reporting of conclusions should include | ||
| 32 | Consideration of alternative explanations for observed results | 8,9 |
| 33 | Generalization of the conclusions (i.e., appropriate for the data presented and within the domain of the literature review) | 12 |
| 34 | Guidelines for future research | 8,9,11 |
| 35 | Disclosure of funding source | 12 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Indini, A.; Petrelli, F.; Tomasello, G.; Rijavec, E.; Facciorusso, A.; Grossi, F.; Ghidini, M. Impact of Use of Gastric-Acid Suppressants and Oral Anti-Cancer Agents on Survival Outcomes: A Systematic Review and Meta-Analysis. Cancers 2020, 12, 998. https://doi.org/10.3390/cancers12040998
Indini A, Petrelli F, Tomasello G, Rijavec E, Facciorusso A, Grossi F, Ghidini M. Impact of Use of Gastric-Acid Suppressants and Oral Anti-Cancer Agents on Survival Outcomes: A Systematic Review and Meta-Analysis. Cancers. 2020; 12(4):998. https://doi.org/10.3390/cancers12040998
Chicago/Turabian StyleIndini, Alice, Fausto Petrelli, Gianluca Tomasello, Erika Rijavec, Antonio Facciorusso, Francesco Grossi, and Michele Ghidini. 2020. "Impact of Use of Gastric-Acid Suppressants and Oral Anti-Cancer Agents on Survival Outcomes: A Systematic Review and Meta-Analysis" Cancers 12, no. 4: 998. https://doi.org/10.3390/cancers12040998
APA StyleIndini, A., Petrelli, F., Tomasello, G., Rijavec, E., Facciorusso, A., Grossi, F., & Ghidini, M. (2020). Impact of Use of Gastric-Acid Suppressants and Oral Anti-Cancer Agents on Survival Outcomes: A Systematic Review and Meta-Analysis. Cancers, 12(4), 998. https://doi.org/10.3390/cancers12040998