
Local and Systemic Therapy of Recurrent Medulloblastomas in Children and Adolescents: Results of the P-HIT-REZ 2005 Study

 , , ,
, , ,  , , add
Show full author list
, , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Trial
2.1.1. Eligibility Criteria
2.1.2. Study Design
2.1.3. Treatment Arms and Local Therapy
2.1.4. Assessment of Therapy Response
2.1.5. Local Therapy
2.1.6. Safety Analysis
2.2. Statistical Analysis
2.3. Ethical Approval
3. Results
3.1. Clinical Characteristics
3.2. Treatment
3.3. Response to Chemotherapy
3.4. Survival Dependent on Patient and Relapse Characteristics
3.4.1. Survival in the Whole Cohort
3.4.2. Survival Dependent on Sex
3.4.3. Survival Dependent on Histological Entities
3.4.4. Survival Dependent on Molecular Subgroup
3.4.5. Survival Depending on Disease Stage at 1st Recurrence/Progression
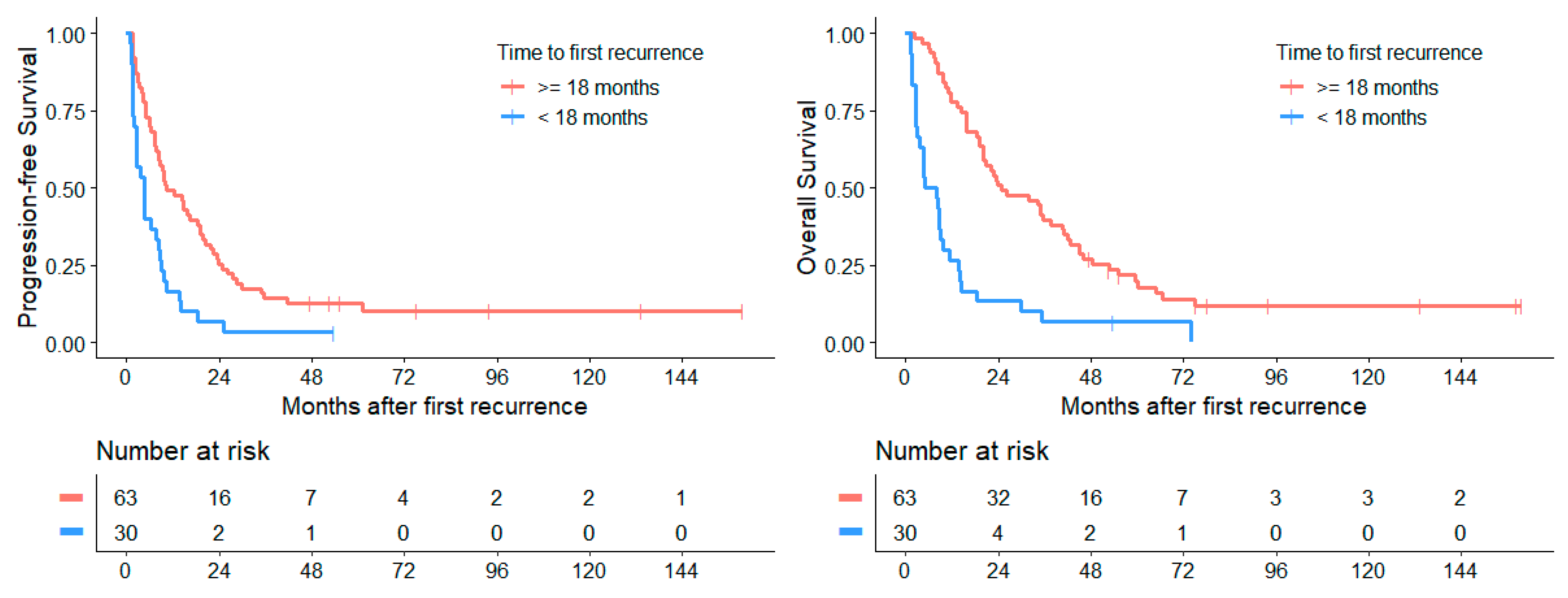
3.4.6. Survival Depending on Time to 1st Recurrence/Progression
3.5. Survival Dependent on Treatment Modalities
3.5.1. Chemotherapy
3.5.2. Surgery
3.5.3. Radiotherapy
3.6. Survival Rates
3.7. Cox Regression Analysis
3.8. Toxicity Analysis
3.8.1. Toxicity of Conventional Chemotherapy Arms
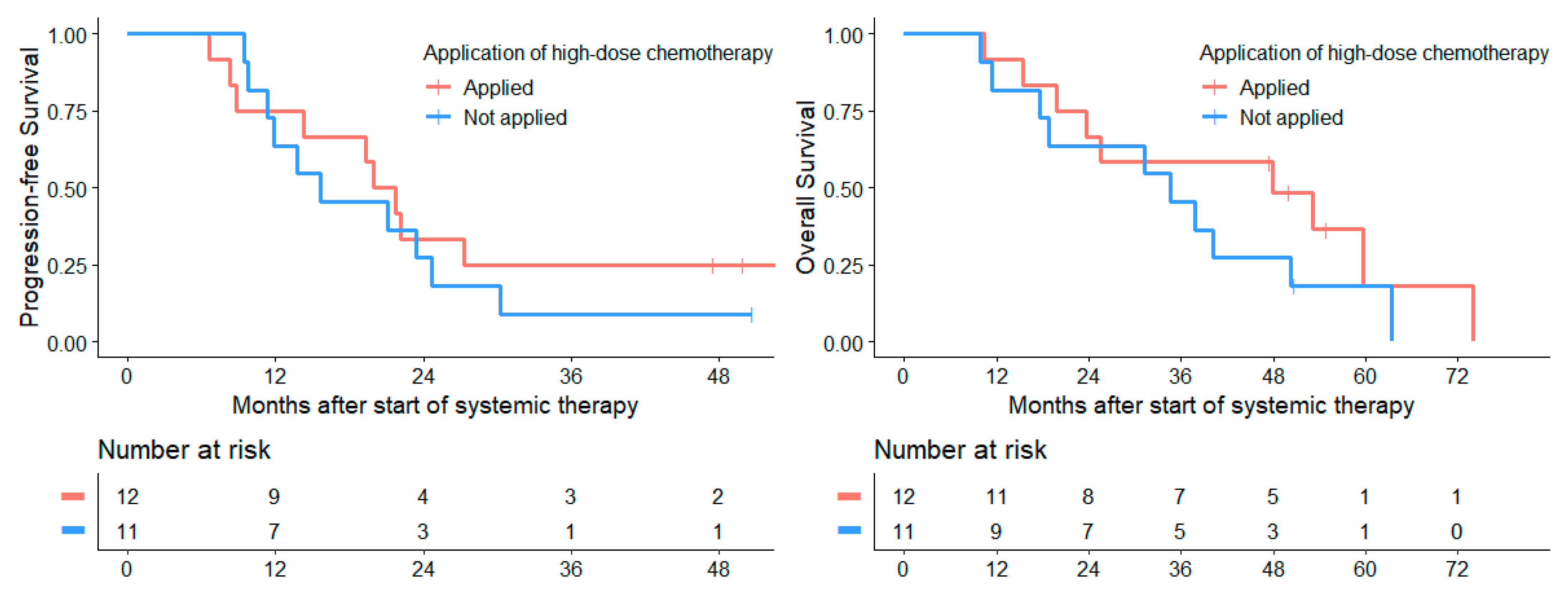
3.8.2. Toxicity of High-Dose Chemotherapy
3.8.3. Long-Term Toxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, R.M.; Richardson, S.; Schwalbe, E.C.; Hicks, D.; Lindsey, J.C.; Crosier, S.; Rafiee, G.; Grabovska, Y.; Wharton, S.B.; Jacques, T.S.; et al. Time, pattern, and outcome of medulloblastoma relapse and their association with tumour biology at diagnosis and therapy: A multicentre cohort study. Lancet Child Adolesc. Health 2020, 4, 865–874. [Google Scholar] [CrossRef]
- Kameda-Smith, M.M.; Wang, A.; Abdulhadi, N.; Voth, R.; Sergeant, A.; Maharaj, A.; Bakhshinyan, D.; Adile, A.A.; Pai, A.M.; Ajani, O.; et al. Salvage Therapy for Childhood Medulloblastoma: A Single Center Experience. Can. J. Neurol. Sci. 2019, 46, 403–414. [Google Scholar] [CrossRef]
- Levy, A.S.; Krailo, M.; Chi, S.; Villaluna, D.; Springer, L.; Williams-Hughes, C.; Fouladi, M.; Gajjar, A. Temozolomide with irinotecan versus temozolomide, irinotecan plus bevacizumab for recurrent medulloblastoma of childhood: Report of a COG randomized Phase II screening trial. Pediatr. Blood Cancer 2021, 68, e29031. [Google Scholar] [CrossRef]
- Gajjar, A.; Robinson, G.W.; Smith, K.S.; Lin, T.; Merchant, T.E.; Chintagumpala, M.; Mahajan, A.; Su, J.; Bouffet, E.; Bartels, U.; et al. Outcomes by Clinical and Molecular Features in Children With Medulloblastoma Treated With Risk-Adapted Therapy: Results of an International Phase III Trial (SJMB03). J. Clin. Oncol. 2021, 39, 822–835. [Google Scholar] [CrossRef]
- Juraschka, K.; Taylor, M.D. Medulloblastoma in the age of molecular subgroups: A review. J. Neurosurg. Pediatr. 2019, 24, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adile, A.A.; Kameda-Smith, M.M.; Bakhshinyan, D.; Banfield, L.; Salim, S.K.; Farrokhyar, F.; Fleming, A.J. Salvage therapy for progressive, treatment-refractory or recurrent pediatric medulloblastoma: A systematic review protocol. Syst. Rev. 2020, 9, 47. [Google Scholar] [CrossRef] [PubMed]
- Gururangan, S.; Krauser, J.; Watral, M.A.; Driscoll, T.; Larrier, N.; Reardon, D.A.; Rich, J.N.; Quinn, J.A.; Vredenburgh, J.J.; Desjardins, A.; et al. Efficacy of high-dose chemotherapy or standard salvage therapy in patients with recurrent medulloblastoma. Neuro-Oncol. 2008, 10, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Peyrl, A.; Chocholous, M.; Kieran, M.W.; Azizi, A.A.; Prucker, C.; Czech, T.; Dieckmann, K.; Schmook, M.T.; Haberler, C.; Leiss, U.; et al. Antiangiogenic metronomic therapy for children with recurrent embryonal brain tumors. Pediatr. Blood Cancer 2012, 59, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Balter-Seri, J.; Mor, C.; Shuper, A.; Zaizov, R.; Cohen, I.J. Cure of recurrent medulloblastoma: The contribution of surgical resection at relapse. Cancer 1997, 79, 1241–1247. [Google Scholar] [CrossRef] [Green Version]
- Gajjar, A.; Pizer, B. Role of high-dose chemotherapy for recurrent medulloblastoma and other CNS primitive neuroectodermal tumors. Pediatr. Blood Cancer 2010, 54, 649–651. [Google Scholar] [CrossRef] [PubMed]
- Bode, U.; Zimmermann, M.; Moser, O.; Rutkowski, S.; Warmuth-Metz, M.; Pietsch, T.; Kortmann, R.D.; Faldum, A.; Fleischhack, G. Treatment of recurrent primitive neuroectodermal tumors (PNET) in children and adolescents with high-dose chemotherapy (HDC) and stem cell support: Results of the HITREZ 97 multicentre trial. J. Neurooncol. 2014, 120, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Lefkowitz, I.B.; Packer, R.J.; Siegel, K.R.; Sutton, L.N.; Schut, L.; Evans, A.E. Results of treatment of children with recurrent medulloblastoma/primitive neuroectodermal tumors with lomustine, cisplatin, and vincristine. Cancer 1990, 65, 412–417. [Google Scholar] [CrossRef]
- Friedman, H.S.; Mahaley, M.S., Jr.; Schold, S.C., Jr.; Vick, N.A.; Falletta, J.M.; Bullard, D.E.; D’Souza, B.J.; Khandekar, J.D.; Lew, S.; Oakes, W.J.; et al. Efficacy of vincristine and cyclophosphamide in the therapy of recurrent medulloblastoma. Neurosurgery 1986, 18, 335–340. [Google Scholar] [CrossRef]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, D.R.; Cascino, T.L.; Schold, S.C., Jr.; Cairncross, J.G. Response criteria for phase II studies of supratentorial malignant glioma. J. Clin. Oncol. 1990, 8, 1277–1280. [Google Scholar] [CrossRef] [PubMed]
- Johnston, D.L.; Keene, D.; Strother, D.; Taneva, M.; Lafay-Cousin, L.; Fryer, C.; Scheinemann, K.; Carret, A.S.; Fleming, A.; Afzal, S.; et al. Survival Following Tumor Recurrence in Children With Medulloblastoma. J. Pediatr. Hematol. Oncol. 2018, 40, e159–e163. [Google Scholar] [CrossRef]
- Kumar, R.; Smith, K.S.; Deng, M.; Terhune, C.; Robinson, G.W.; Orr, B.A.; Liu, A.P.Y.; Lin, T.; Billups, C.A.; Chintagumpala, M.; et al. Clinical Outcomes and Patient-Matched Molecular Composition of Relapsed Medulloblastoma. J. Clin. Oncol. 2021, 39, 807–821. [Google Scholar] [CrossRef]
- Huybrechts, S.; Le Teuff, G.; Tauziède-Espariat, A.; Rossoni, C.; Chivet, A.; Indersie, É.; Varlet, P.; Puget, S.; Abbas, R.; Ayrault, O.; et al. Prognostic Clinical and Biologic Features for Overall Survival after Relapse in Childhood Medulloblastoma. Cancers 2020, 13, 53. [Google Scholar] [CrossRef]
- Sabel, M.; Fleischhack, G.; Tippelt, S.; Gustafsson, G.; Doz, F.; Kortmann, R.; Massimino, M.; Navajas, A.; von Hoff, K.; Rutkowski, S.; et al. Relapse patterns and outcome after relapse in standard risk medulloblastoma: A report from the HIT-SIOP-PNET4 study. J. Neuro-Oncol. 2016, 129, 515–524. [Google Scholar] [CrossRef] [Green Version]
- Le Teuff, G.; Castaneda-Heredia, A.; Dufour, C.; Jaspan, T.; Calmon, R.; Devos, A.; McHugh, K.; Leblond, P.; Frappaz, D.; Aerts, I.; et al. Phase II study of temozolomide and topotecan (TOTEM) in children with relapsed or refractory extracranial and central nervous system tumors including medulloblastoma with post hoc Bayesian analysis: A European ITCC study. Pediatr. Blood Cancer 2020, 67, e28032. [Google Scholar] [CrossRef]
- Ramaswamy, V.; Remke, M.; Bouffet, E.; Faria, C.C.; Perreault, S.; Cho, Y.J.; Shih, D.J.; Luu, B.; Dubuc, A.M.; Northcott, P.A.; et al. Recurrence patterns across medulloblastoma subgroups: An integrated clinical and molecular analysis. Lancet Oncol. 2013, 14, 1200–1207. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Dubuc, A.M.; Ramaswamy, V.; Mack, S.; Gendoo, D.M.; Remke, M.; Wu, X.; Garzia, L.; Luu, B.; Cavalli, F.; et al. Medulloblastoma subgroups remain stable across primary and metastatic compartments. Acta Neuropathol. 2015, 129, 449–457. [Google Scholar] [CrossRef] [Green Version]
- Cavalli, F.M.G.; Remke, M.; Rampasek, L.; Peacock, J.; Shih, D.J.H.; Luu, B.; Garzia, L.; Torchia, J.; Nor, C.; Morrissy, A.S.; et al. Intertumoral Heterogeneity within Medulloblastoma Subgroups. Cancer Cell 2017, 31, 737–754.e736. [Google Scholar] [CrossRef] [Green Version]
- Morrissy, A.S.; Cavalli, F.M.G.; Remke, M.; Ramaswamy, V.; Shih, D.J.H.; Holgado, B.L.; Farooq, H.; Donovan, L.K.; Garzia, L.; Agnihotri, S.; et al. Spatial heterogeneity in medulloblastoma. Nat. Genet. 2017, 49, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Morrissy, A.S.; Garzia, L.; Shih, D.J.; Zuyderduyn, S.; Huang, X.; Skowron, P.; Remke, M.; Cavalli, F.M.; Ramaswamy, V.; Lindsay, P.E.; et al. Divergent clonal selection dominates medulloblastoma at recurrence. Nature 2016, 529, 351–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Northcott, P.A.; Dubuc, A.; Dupuy, A.J.; Shih, D.J.; Witt, H.; Croul, S.; Bouffet, E.; Fults, D.W.; Eberhart, C.G.; et al. Clonal selection drives genetic divergence of metastatic medulloblastoma. Nature 2012, 482, 529–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramaswamy, V.; Taylor, M.D. Medulloblastoma: From Myth to Molecular. J. Clin. Oncol. 2017, 35, 2355–2363. [Google Scholar] [CrossRef]
- Weintraub, L.; Miller, T.; Friedman, I.; Abbott, R.; Levy, A.S. Misdiagnosing recurrent medulloblastoma: The danger of examination and imaging without histological confirmation. J. Neurosurg. Pediatr. 2014, 13, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Deng, M.Y.; Sturm, D.; Pfaff, E.; Sill, M.; Stichel, D.; Balasubramanian, G.P.; Tippelt, S.; Kramm, C.; Donson, A.M.; Green, A.L.; et al. Radiation-induced gliomas represent H3-/IDH-wild type pediatric gliomas with recurrent PDGFRA amplification and loss of CDKN2A/B. Nat. Commun. 2021, 12, 5530. [Google Scholar] [CrossRef]
- Müller, K.; Mynarek, M.; Zwiener, I.; Siegler, N.; Zimmermann, M.; Christiansen, H.; Budach, W.; Henke, G.; Warmuth-Metz, M.; Pietsch, T.; et al. Postponed is not canceled: Role of craniospinal radiation therapy in the management of recurrent infant medulloblastoma--an experience from the HIT-REZ 1997 & 2005 studies. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1019–1024. [Google Scholar] [CrossRef]
- Tsang, D.S.; Sarhan, N.; Ramaswamy, V.; Nobre, L.; Yee, R.; Taylor, M.D.; Hawkins, C.; Bartels, U.; Huang, A.; Tabori, U.; et al. Re-irradiation for children with recurrent medulloblastoma in Toronto, Canada: A 20-year experience. J. Neurooncol. 2019, 145, 107–114. [Google Scholar] [CrossRef]
- Dietzsch, S.; Braesigk, A.; Seidel, C.; Remmele, J.; Kitzing, R.; Schlender, T.; Mynarek, M.; Geismar, D.; Jablonska, K.; Schwarz, R.; et al. Pretreatment central quality control for craniospinal irradiation in non-metastatic medulloblastoma: First experiences of the German radiotherapy quality control panel in the SIOP PNET5 MB trial. Strahlenther. Und Onkol. 2021, 197, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Grill, J.; Geoerger, B.; Gesner, L.; Perek, D.; Leblond, P.; Canete, A.; Aerts, I.; Madero, L.; de Toledo Codina, J.S.; Verlooy, J.; et al. Phase II study of irinotecan in combination with temozolomide (TEMIRI) in children with recurrent or refractory medulloblastoma: A joint ITCC and SIOPE brain tumor study. Neuro-Oncol. 2013, 15, 1236–1243. [Google Scholar] [CrossRef] [Green Version]
- Blasberg, R.G.; Patlak, C.; Fenstermacher, J.D. Intrathecal chemotherapy: Brain tissue profiles after ventriculocisternal perfusion. J. Pharmacol. Exp. Ther. 1975, 195, 73–83. [Google Scholar]
- Levin, V.A.; Patlak, C.S.; Landahl, H.D. Heuristic modeling of drug delivery to malignant brain tumors. J. Pharmacokinet. Biopharm. 1980, 8, 257–296. [Google Scholar] [CrossRef]
- Fleischhack, G.; Jaehde, U.; Bode, U. Pharmacokinetics following intraventricular administration of chemotherapy in patients with neoplastic meningitis. Clin. Pharmacokinet. 2005, 44, 1–31. [Google Scholar] [CrossRef]
- Bass, J.K.; Huang, J.; Onar-Thomas, A.; Chang, K.W.; Bhagat, S.P.; Chintagumpala, M.; Bartels, U.; Gururangan, S.; Hassall, T.; Heath, J.A.; et al. Concordance between the chang and the International Society of Pediatric Oncology (SIOP) ototoxicity grading scales in patients treated with cisplatin for medulloblastoma. Pediatr. Blood Cancer 2014, 61, 601–605. [Google Scholar] [CrossRef] [Green Version]
- Massimino, M.; Gandola, L.; Spreafico, F.; Biassoni, V.; Luksch, R.; Collini, P.; Solero, C.N.; Simonetti, F.; Pignoli, E.; Cefalo, G.; et al. No salvage using high-dose chemotherapy plus/minus reirradiation for relapsing previously irradiated medulloblastoma. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1358–1363. [Google Scholar] [CrossRef]
- Ridola, V.; Grill, J.; Doz, F.; Gentet, J.C.; Frappaz, D.; Raquin, M.A.; Habrand, J.L.; Sainte-Rose, C.; Valteau-Couanet, D.; Kalifa, C. High-dose chemotherapy with autologous stem cell rescue followed by posterior fossa irradiation for local medulloblastoma recurrence or progression after conventional chemotherapy. Cancer 2007, 110, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Dunkel, I.J.; Gardner, S.L.; Garvin, J.H., Jr.; Goldman, S.; Shi, W.; Finlay, J.L. High-dose carboplatin, thiotepa, and etoposide with autologous stem cell rescue for patients with previously irradiated recurrent medulloblastoma. Neuro-Oncol. 2010, 12, 297–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Lesion | Non-Target Lesions and/or Nodular Meningeosis | New Lesions | CSF Cytology | Laminar Meningeosis | “Overall Response” |
|---|---|---|---|---|---|
| CR | CR | No | CR | CR | CR |
| CR | Non-CR | No | CR | CR | PR |
| PR | CR/Non-CR | No | CR | CR | PR |
| SD | CR/Non-CR | No | CR/NR | CR/NR | SD |
| CR/PR/SD | CR/Non-CR | No | NR | CR/NR | SD |
| CR/PR/SD | CR/Non-CR | No | CR/NR | NR | SD |
| PD | All | Yes or No | All | All | PD |
| All | PD | Yes or No | All | All | PD |
| All | All | Yes | All | All | PD |
| All | All | Yes or No | PD | All | PD |
| All | All | Yes or No | All | PD | PD |
| Clinical Characteristics | Subgroup/ Value | Number of Patients at 1st Recurrence (%) | Numbers of Patients at Study Relapse (%) |
|---|---|---|---|
| Sex | male | 67 (72.0) | 67 (72.0) |
| female | 26 (28.0) | 26 (28.0) | |
| Number of relapses | refractory | 20 (21.5) | 20 (21.5) |
| 1st | 73 (78.5) | 72 (77.4) | |
| 2nd | - | 1 (1.1) | |
| Age at diagnosis of 1st recurrence or at study relapse | median | 10.1 years | 10.1 years |
| range | 2.6–30.6 years | 2.6–30.6 years | |
| IQR | 6.9–16.1 years | 6.9–16.1 years | |
| <6 years | 19 (20.4) | 19 (20.4) | |
| >16 years | 23 (24.7) | 23 (24.7) | |
| Time to 1st recurrence after initial diagnosis | median | 23.6 months | 23.6 months |
| range | 1.3–220.2 months | 1.3–220.2 months | |
| IQR | 16.0–41.9 months | 16.0–41.9 months | |
| Chang stage at 1st recurrence or at study relapse | M0 | 10 (10.7) | 10 (10.7) |
| M1 | 1 (1.1) | 1 (1.1) | |
| M2 | 25 (26.9) | 25 (26.9) | |
| M3 | 55 (59.1) | 55 (59.1) | |
| M4 | 2 (2.2) | 2 (2.2) | |
| Extent of relapse | localized only | 10 (10.7) | 10 (10.7) |
| disseminated only | 61 (65.6) | 61 (65.6) | |
| combined | 22 (23.7) | 22 (23.7) | |
| Histological subgroups | classic | 76 (81.7) | 76 (81.7) |
| desmoplastic | 13 (14.0) | 13 (14.0) | |
| large cell/anaplastic | 4 (4.3) | 4 (4.3) | |
| Molecular subgroups | group 4 | 21 (22.6) | 21 (22.6) |
| group 3 | 16 (17.2) | 16 (17.2) | |
| SHH | 3 (3.2) | 3 (3.2) | |
| WNT | 2 (2.2) | 2 (2.2) | |
| no data | 51 (54.8) | 51 (54.8) |
| Treatment | Therapy Arms/ Therapy Characteristics | Therapy Subgroups | Number of Patients at First Relapse n = 93 (%) | Number of Patients at ≥2nd Relapse n = 51 (%) |
|---|---|---|---|---|
| Chemotherapy | all | yes | 93 (100) | 6 (11.8) |
| oCHT arm (temozolomide) | all | 46 (49.5) | 1 (2.0) | |
| with prior phase II window | 18 (19.3) | 1 (2.0) | ||
| with simultaneous ivc etoposide | 6 (6.4) | 1 (2.0) | ||
| with shift to oral | 6 (6.4) | 0 (0) | ||
| etoposide/trofosfamide | ||||
| with shift to ivCHT | 7 (7.5) | 0 (0) | ||
| ivCHT arm (carboplatin/ etoposide) | all | 28 (30.1) | 0 (0) | |
| with prior phase II window | 7 (7.5) | 0 (0) | ||
| with simultaneous ivc etoposide | 8 (8.6) | 0 (0) | ||
| with shift to oCHT | 5 (5.4) | 0 (0) | ||
| doc arm | all | 19 (20.4) | 5 (9.8) 1/37 (72.5) 2 | |
| systemic chemotherapy | 13 (14.0) | 5 (9.8) 1/37 (72.5) 2 | ||
| with prior phase II window | 6 (6.4) | 1 (2.0) 1/14 (27.5) 2 | ||
| Intra-ventricular chemotherapy | all | yes | 43 (46.2) | 9 (17.6) |
| agents | phase II window trial, etoposide | 32 (34.4) | 3 (5.9) | |
| simultaneous etoposide to | 18 (19.4) | 2 (3.9) | ||
| systemic chemotherapy | ||||
| liposomal cytarabine (doc arm) | 5 (5.4) | 5 (9.8) | ||
| methotrexate (doc arm) | 3 (3.2) | 1 (2.0) | ||
| High-dose chemotherapy | all | yes | 17 (18.3) | 1 (2.0) |
| agents | thiotepa/carboplatin/etoposide | 13 (14.0) | 0 (0) | |
| temozolomide/thiotepa | 3 (3.2) | 0 (0) | ||
| other agents | 1 (1.1) | 1 (2.0) | ||
| Surgery | all | yes | 22 (23.7) | 11 (21.6) |
| extent of resection | GTR | 12 (12.9) | 4 (7.8) | |
| NTR | 7 (7.5) | 2 (3.9) | ||
| STR | 3 (3.2) | 0 (0) | ||
| unknown | 0 (0) | 5 (9.8) | ||
| Radiotherapy | all | yes | 20 (21.5) | 16 (31.4) |
| sequence | RT as 1st RT | 9 (9.7) | 1 (2.0) | |
| RT as 2nd RT | 11 (11.8) | 15 (29.4) | ||
| target volume | CSI only | 2 (2.2) | 0 (0) | |
| CSI with boost | 11 (11.8) | 2 (3.9) | ||
| local tumor bed only | 4 (4.3) | 9 (17.6) | ||
| unknown | 3 (3.2) | 5 (9.8) |
| Study Arm and Time Point | CR n (%) | PR n (%) | SD n (%) | PD n (%) | DOD n (%) | n. e. n | ORR % | p-Value |
|---|---|---|---|---|---|---|---|---|
| ivCHT after 2 cycles | 3 (11.1) | 11 (40.7) | 9 (33.3) | 4 (14.8) | 0 (0) | 1 | 51.8 | 0.015 |
| oCHT after 2 cycles | 2 (4.5) | 6 (13.6) | 15 (34.1) | 19 (43.2) | 2 (4.5) | 3 | 18.2 | |
| ivCHT after 4 cycles * | 6 (23.1) | 7 (26.9) | 6 (23.1) | 7 (26.9) | 0 (0) | 2 | 50.0 | 0.086 |
| oCHT after 4 cycles * | 2 (4.3) | 9 (19.6) | 12 (26.1) | 20 (43.5) | 3 (6.5) | 1 | 23.9 | |
| ivCHT Best overall response | 6 (22.2) | 12 (44.4) | 7 (25.9) | 2 (7.4) | 0 (0) | 1 | 66.7 | 0.023 |
| oCHT Best overall response | 3 (6.5) | 13 (28.3) | 14 (30.4) | 15 (32.6) | 2 (4.3) | 1 | 34.8 |
| Molecular Group | Number of Patients (%) | Metastases at 1st Recurrence (%) | Median PFS1stRD in Months (95%-CI) | Median OS1stRD in Months (95%-CI) |
|---|---|---|---|---|
| WNT | 2 (2.2) | 2 (100) | 4.1 (NA–NA) | 15.7 (NA–NA) |
| SHH | 3 (3.2) | 3 (100) | 2.4 (0–5.4) | 2.4 (0.4–4.4) |
| Group 3 1 | 16 (17.2) | 15 (93.8) | 4.9 (3.2–6.0) | 9.8 (8.2–11.3) |
| Group 4 1 | 21 (22.6) | 19 (90.5) | 7.2 (4.9–9.5) | 20.0 (15.1–24.9) |
| Characteristics | Subgroups | 2-Years PFS1stRD | 5-Year PFS1stRD | 10-Year PFS1stRD | 2-Year OS1stRD | 5-Year OS1stRD | 10-Year OS1stRD |
|---|---|---|---|---|---|---|---|
| Clinical Characteristics | |||||||
| Overall Cohort | 19.4 | 9.7 | 7.7 | 38.7 | 15.5 | 8.4 | |
| (12.8–29.3) | (5.2–18) | (3.6–16.6) | (30.0–50.0) | (9.5–25.2) | (4.1–17.4) | ||
| Sex | Male | 14.9 | 4.5 | 3.0 | 37.3 | 11.9 | 6.0 |
| (8.4–26.4) | (1.5–13.5) | (0.8–11.7) | (27.4–50.9) | (6.2–22.9) | (2.3–15.4) | ||
| Female | 30.8 | 23.1 | 23.1 | 42.3 | 24.6 | 16.4 | |
| (17.3–54.8) | (11.4–46.6) | (11.4–46.6) | (27.0–66.3) | (11.9–50.8) | (5.6–48.3) | ||
| Disease stage | Local | 40.0 | 20.0 | 20.0 | 80.0 | 40.0 | 20.0 |
| (18.7–85.5) | (5.8–69.1) | (5.8–69.1) | (58.7–100) | (18.7–85.5) | (5.8–69.1) | ||
| Metastatic | 16.9 | 8.4 | 5.6 | 33.7 | 12.6 | 7.2 | |
| (10.5–27.2) | (4.2–17.1) | (1.9–16.4) | (25.0–45.6) | (7.0–22.6) | (3.0–17.2) | ||
| Histological entity | Classical | 18.4 | 7.9 | 5.9 | 36.8 | 15.4 | 7.7 |
| (11.5–29.6) | (3.7–17.0) | (2.3–15.4) | (27.4–49.5) | (9.0–26.3) | (3.4–17.4) | ||
| Desmoplastic/nodular | 30.8 | 23.1 | 23.1 | 61.5 | 23.1 | 23.1 | |
| (13.6–69.5) | (8.6–62.3) | (8.6–62.3) | (40.0–94.6) | (8.6–62.3) | (8.6–62.3) | ||
| Large cell/anaplastic | 0 | 0 | 0 | 0 | 0 | 0 | |
| (NA-NA) | (NA-NA) | (NA-NA) | (NA-NA) | (NA-NA) | (NA-NA) | ||
| Time-point of 1st relapse | <18 months | 6.7 | 3.3 | 3.3 | 13.3 | 6.7 | 0 |
| (1.7–25.4) | (0.5–22.9) | (0.5–22.9) | (5.4–33.2) | (1.7–25.4) | (NA-NA) | ||
| ≥18 months | 25.4 | 12.7 | 10.2 | 50.8 | 19.8 | 11.9 | |
| (16.6–38.8) | (6.6–24.3) | (4.6–22.2) | (39.8–64.8) | (11.9–33) | (5.8–24.4) | ||
| Treatment Characteristics | |||||||
| Systemic treatment | ivCHT arm | 33.3 | 20.8 | 20.8 | 54.2 | 32.4 | 16.2 |
| (carboplatin/etoposide) | (18.9–58.7) | (9.6–45.4) | (9.6–45.4) | (37.5–78.3) | (18–58.4) | (6.0–43.7) | |
| oCHT arm | 9.4 | 0 | 0 | 25.0 | 3.1 | 0 | |
| (temozolomide) | (3.2–27.5) | (NA-NA) | (NA-NA) | (13.7–45.6) | (0.5–21.5) | (NA-NA) | |
| Response to systemic chemotherapy | Objective | 50.0 | 31.2 | 31.2 | 68.8 | 32.1 | 16.1 |
| (30.6–81.6) | (15.1–64.6) | (15.1–64.6) | (49.4–95.7) | (14.3–72.1) | (3.2–79.9) | ||
| No objective | 12.3 | 4.1 | 4.1 | 31.5 | 11.0 | 5.5 | |
| (6.7–22.7) | (1.3–12.3) | (1.3–12.3) | (22.5–44.2) | (5.7–21.1) | (2.1–14.2) | ||
| Local treatment | Surgery | 31.8 | 18.2 | 12.1 | 50.0 | 25.6 | 15.3 |
| (GTR, NTR, STR) | (17.3–58.7) | (7.5–44.1) | (3.7–40.0) | (32.9–75.9) | (12.3–53.3) | (5.5–42.8) | |
| No surgery/biopsy | 15.5 | 7.0 | 7.0 | 35.2 | 12.1 | 6.0 | |
| (9.0–26.7) | (3.0–16.4) | (3.0–16.4) | (25.7–48.3) | (6.3–23.1) | (2.2–16.9) | ||
| Radiotherapy | 50.0 | 30.0 | 22.5 | 55.0 | 33.3 | 26.7 | |
| (32.3–77.5) | (15.4–58.6) | (9.4–54.1) | (37.0–81.8) | (17.5–63.5) | (12.2–58.2) | ||
| No radiotherapy | 11.0 | 4.1 | 4.1 | 34.2 | 10.8 | 3.6 | |
| (5.7–21.1) | (1.4–12.4) | (1.4–12.4) | (24.9–47.1) | (5.5–21.0) | (1.0–13.4) | ||
| Treated in | 19.4 | 9.7 | 9.7 | 38.7 | 10.8 | 10.8 | |
| phase II window trial | (9.4–39.7) | (3.3–28.4) | (3.3–28.4) | (24.9–60.3) | (3.5–33.4) | (3.5–33.4) | |
| Variable | Survival Type | Univariate Cox-Regression | Multivariate Cox-Regression | ||||
|---|---|---|---|---|---|---|---|
| Statistical Value | HR | 95%-CI | p-Value | HR | 95%-CI | p-Value | |
| Female sex | PFS | 0.56 | 0.34–0.94 | 0.03 | 0.83 | 0.46–1.49 | 0.52 |
| OS | 0.70 | 0.42–1.15 | 0.16 | 1.01 | 0.46–1.59 | 0.62 | |
| Metastases at 1st recurrence | PFS | 1.62 | 0.78–3.38 | 0.20 | 0.73 | 0.30–1.82 | 0.50 |
| OS | 2.33 | 1.11–4.88 | 0.03 | 1.42 | 0.61–3.34 | 0.42 | |
| Desmoplastic histology | PFS | 0.69 | 0.36–1.34 | 0.27 | 0.51 | 0.22–1.17 | 0.11 |
| OS | 0.75 | 0.39–1.45 | 0.39 | 0.62 | 0.29–1.34 | 0.23 | |
| Objective response to chemotherapy at 1st recurrence | PFS | 0.32 | 0.17–0.61 | 0.0005 | 0.23 | 0.10–0.55 | 0.0009 |
| OS | 0.42 | 0.22–0.81 | 0.009 | 0.41 | 0.18–0.94 | 0.036 | |
| GTR/NTR/STR at 1st recurrence | PFS | 0.56 | 0.33–0.97 | 0.04 | 0.72 | 0.37–1.39 | 0.32 |
| OS | 0.60 | 0.35–1.04 | 0.07 | 0.91 | 0.48–1.73 | 0.78 | |
| First radiotherapy at 1st recurrence | PFS | 0.31 | 0.13–0.73 | 0.002 | 0.12 | 0.04–0.38 | 0.0003 |
| OS | 0.29 | 0.11–0.73 | 0.002 | 0.15 | 0.05–0.48 | 0.001 | |
| Time to 1st recurrence <18 months after initial diagnosis | PFS | 2.34 | 1.47–3.73 | 0.0003 | 2.90 | 1.57–5.33 | 0.0006 |
| OS | 3.26 | 2.04–5.20 | <0.0001 | 5.97 | 3.02–11.79 | <0.0001 | |
| Age < 6 years at 1st recurrence | PFS | 0.89 | 0.51–1.53 | 0.67 | 0.70 | 0.34–1.42 | 0.32 |
| OS | 1.10 | 0.64–1.91 | 0.72 | 0.46 | 0.22–0.99 | 0.047 | |
| Age > 16 years at 1st recurrence | PFS | 1.02 | 0.63–1.64 | 0.95 | 0.88 | 0.49–1.58 | 0.67 |
| OS | 0.70 | 0.42–1.15 | 0.16 | 0.67 | 0.36–1.22 | 0.19 | |
| Study Arm | ivCHT Arm | oCHT Arm | ||||||
|---|---|---|---|---|---|---|---|---|
| Cycle | 1st | 2nd | 3rd | 4th | 1st | 2nd | 3rd | 4th |
| Toxicity rate (%) | ||||||||
| All Toxicities CTC° 3 and 4 | 86.4 | 76.1 | 80.9 | 78.9 | 14.3 | 22.6 | 23.1 | 20.8 |
| Hematological toxicity | ||||||||
| Anemia | 36.4 | 61.9 | 61.9 | 57.9 | 5.7 | 3.2 | 15.4 | 12.5 |
| Leukopenia | 68.2 | 61.9 | 80.9 | 68.4 | 2.9 | 9.7 | 15.4 | 16.7 |
| Granulocytopenia | 63.6 | 61.9 | 61.9 | 68.4 | 2.9 | 6.4 | 15.4 | 16.7 |
| Thrombocytopenia | 81.8 | 76.2 | 71.4 | 78.4 | 2.9 | 12.9 | 15.4 | 16.7 |
| Non-hematological toxicity | ||||||||
| Infection/febrile neutropenia | 50.0 | 33.3 | 38.1 | 26.3 | 2.9 | 6.4 | 11.5 | 0 |
| Oral mucositis | 4.5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Intestinal mucositis | 4.5 | 14.2 | 4.8 | 0 | 0 | 0 | 0 | 0 |
| Constipation | 0 | 0 | 0 | 0 | 2.9 | 0 | 0 | 0 |
| Skin toxicity | 0 | 0 | 0 | 0 | 2.9 | 3.2 | 3.8 | 0 |
| CNS neurotoxicity | 4.5 | 4.8 | 4.8 | 5.3 | 2.9 | 6.4 | 0 | 0 |
| Peripheral neurotoxicity | 0 | 0 | 0 | 0 | 0 | 3.2 | 0 | 0 |
| Nausea/Vomiting | 0 | 0 | 0 | 0 | 2.9 | 3.2 | 0 | 0 |
| Ototoxicity/hearing loss | 4.5 | 4.8 | 9.5 | 10.5 | 5.7 | 3.2 | 3.8 | 4.2 |
| Renal toxicity | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hepatotoxicity | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Pulmonal toxicity | 0 | 0 | 0 | 0 | 0 | 3.2 | 0 | 0 |
| Cardiotoxicity | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| CTC Grade | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Toxicity rate (%) | ||||
| Hematological toxicity | ||||
| Anemia | 0 | 0 | 64.3 | 35.7 |
| Leukopenia | 0 | 0 | 0 | 100 |
| Granulocytopenia | 0 | 0 | 0 | 100 |
| Thrombocytopenia | 0 | 0 | 0 | 100 |
| Non-hematological toxicity | ||||
| Infection | 6.7 | 13.3 | 66.7 | 6.7 |
| Febrile neutropenia | 0 | 13.3 | 40.0 | 46.7 |
| Oral mucositis | 0 | 35.7 | 50.0 | 7.1 |
| Intestinal mucositis | 20.0 | 20.0 | 46.7 | 13.3 |
| Skin toxicity | 30.7 | 23.1 | 7.7 | 0 |
| CNS neurotoxicity | 11.1 | 11.1 | 0 | 22.2 |
| Peripheral neurotoxicity | 0 | 0 | 0 | 0 |
| Nausea/Vomiting | 6.7 | 40.0 | 53.3 | 0 |
| Ototoxicity/hearing loss | 0 | 20.0 | 80.0 | 0 |
| Renal toxicity | 20.0 | 0 | 0 | 10.0 |
| Hepatotoxicity | 41.7 | 25.0 | 33.3 | 0 |
| Pulmonary toxicity | 0 | 20.0 | 30.0 | 0 |
| Cardiotoxicity | 0 | 30.0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaab, C.; Adolph, J.E.; Tippelt, S.; Mikasch, R.; Obrecht, D.; Mynarek, M.; Rutkowski, S.; Pfister, S.M.; Milde, T.; Witt, O.; et al. Local and Systemic Therapy of Recurrent Medulloblastomas in Children and Adolescents: Results of the P-HIT-REZ 2005 Study. Cancers 2022, 14, 471. https://doi.org/10.3390/cancers14030471
Gaab C, Adolph JE, Tippelt S, Mikasch R, Obrecht D, Mynarek M, Rutkowski S, Pfister SM, Milde T, Witt O, et al. Local and Systemic Therapy of Recurrent Medulloblastomas in Children and Adolescents: Results of the P-HIT-REZ 2005 Study. Cancers. 2022; 14(3):471. https://doi.org/10.3390/cancers14030471
Chicago/Turabian StyleGaab, Christine, Jonas E. Adolph, Stephan Tippelt, Ruth Mikasch, Denise Obrecht, Martin Mynarek, Stefan Rutkowski, Stefan M. Pfister, Till Milde, Olaf Witt, and et al. 2022. "Local and Systemic Therapy of Recurrent Medulloblastomas in Children and Adolescents: Results of the P-HIT-REZ 2005 Study" Cancers 14, no. 3: 471. https://doi.org/10.3390/cancers14030471