
Outcomes of Modified Mayo Stage IIIa and IIIb Cardiac Light-Chain Amyloidosis: Real-World Experience in Clinical Characteristics and Treatment—67 Patients Multicenter Analysis

 , , , , , ,
, , , , , ,  ,
,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Patient Information
3.2. Methods and Effectiveness of First-Line Treatment
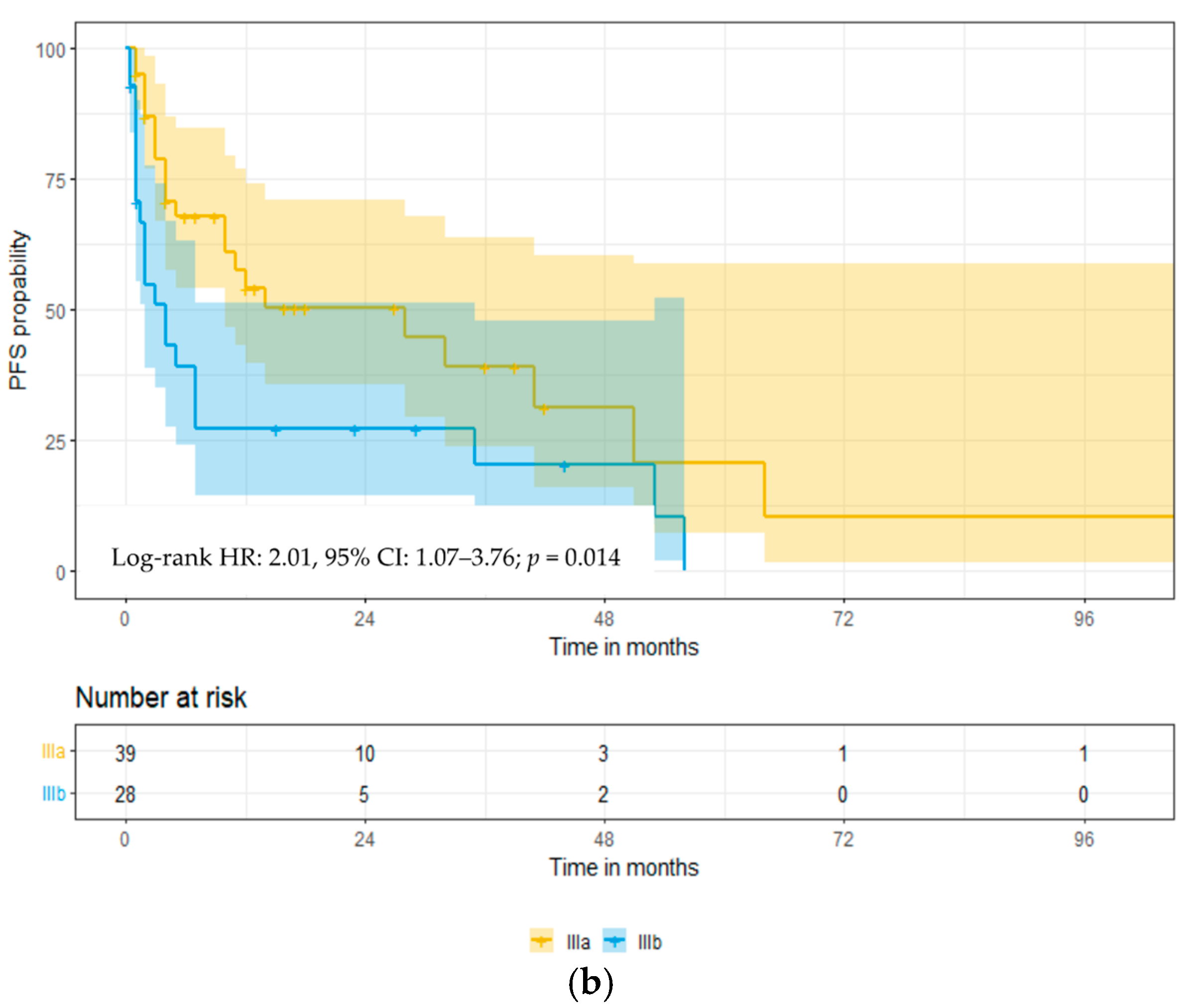
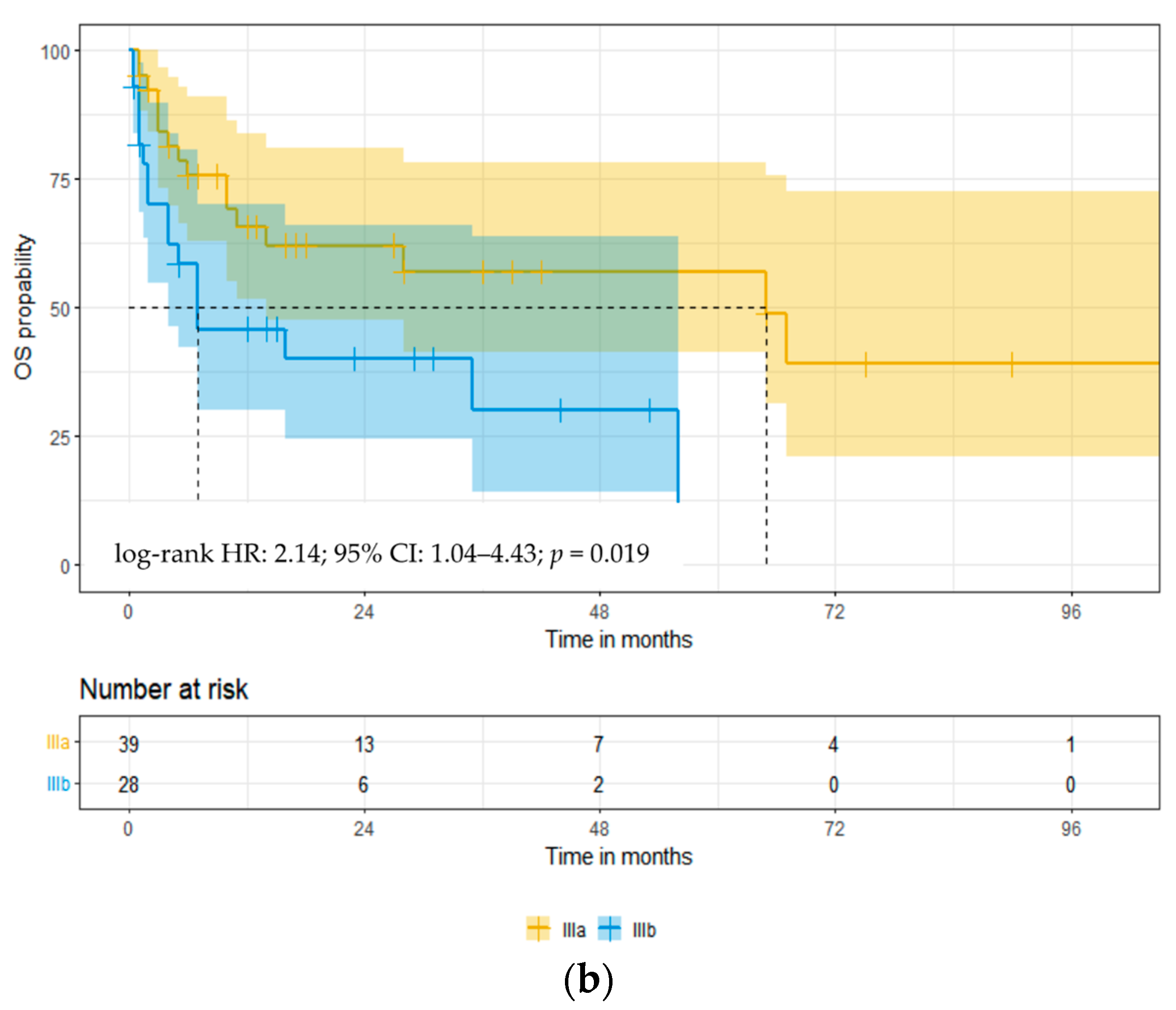
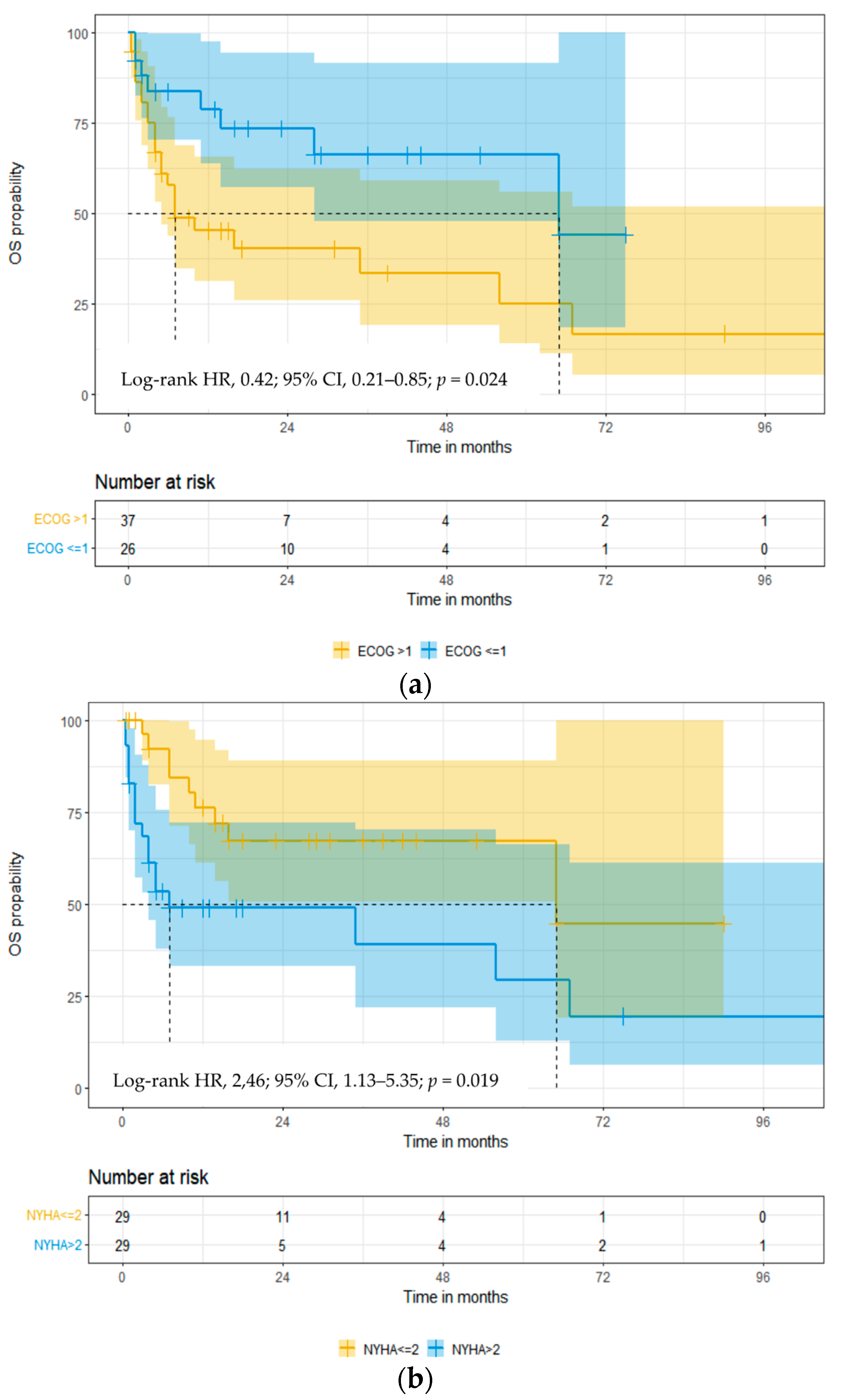
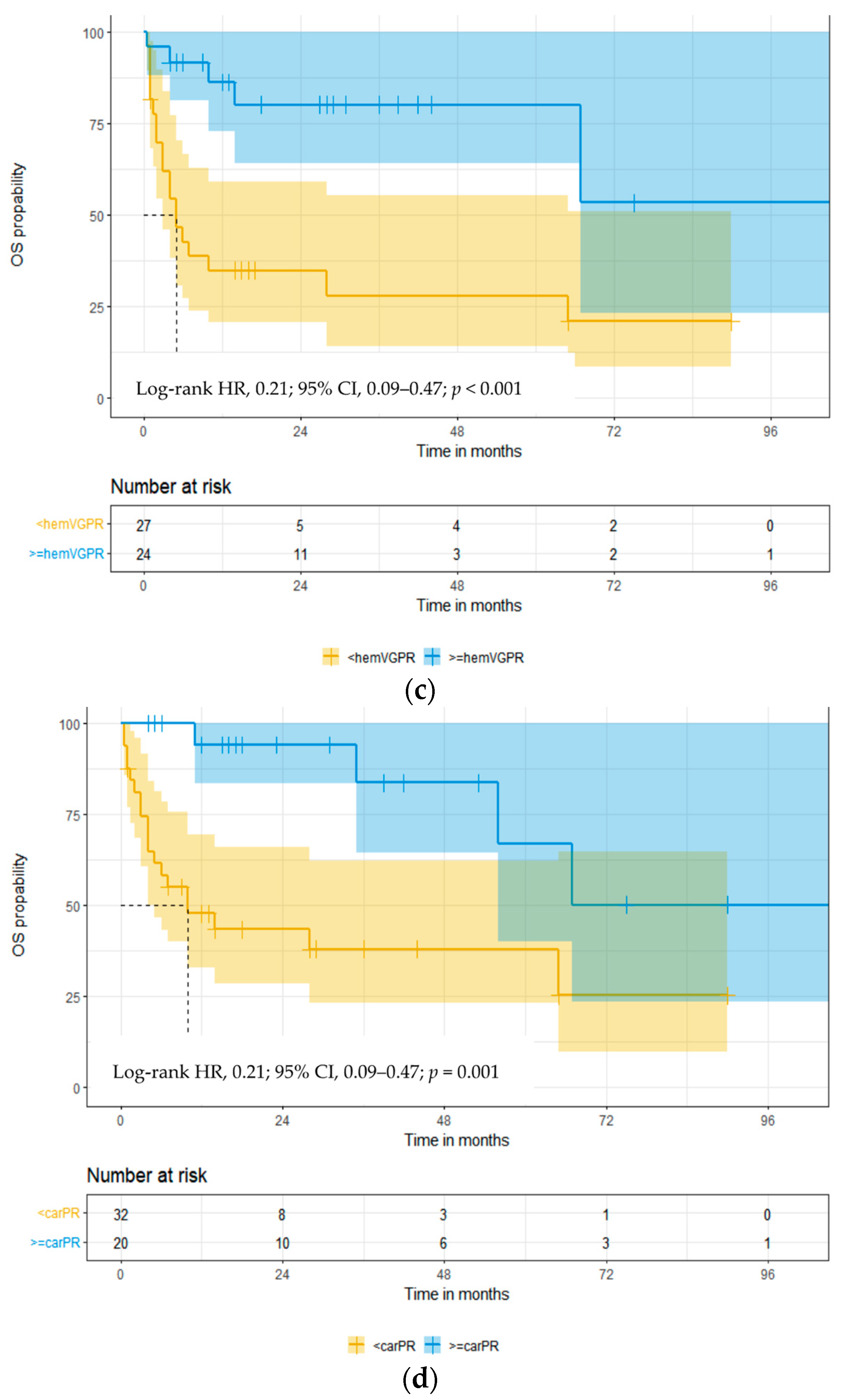
3.3. Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Germain, P.; Vardazaryan, A.; Padoy, N.; Labani, A.; Roy, C.; Schindler, T.H.; El Ghannudi, S. Deep Learning Supplements Visual Analysis by Experienced Operators for the Diagnosis of Cardiac Amyloidosis by Cine-CMR. Diagnostics 2021, 12, 69. [Google Scholar] [CrossRef]
- Merlini, G.; Seldin, D.C.; Gertz, M.A. Amyloidosis: Pathogenesis and new therapeutic options. J. Clin. Oncol. 2011, 29, 1924–1933. [Google Scholar] [CrossRef]
- Blank, M.; Campbell, M.; Clarke, J.O.; Comenzo, R.; Dember, L.M.; Dispenzieri, A.; Dorbala, S.; Dunnmon, P.; Faller, D.V.; Rodney, H.F.; et al. The amyloidosis forum: A public private partnership to advance drug development in AL amyloidosis. Orphanet. J. Rare Dis. 2020, 15, 268. [Google Scholar]
- Desport, E.; Bridoux, F.; Sirac, C.; Delbes, S.; Bender, S.; Fermandez, B.; Quellard, N.; Lacombe, C.; Goujon, J.M.; Lavergne, D.; et al. AL amyloidosis. Orphanet. J. Rare Dis. 2012, 7, 54. [Google Scholar] [CrossRef]
- Quock, T.P.; Yan, T.; Chang, E.; Guthrie, S.; Broder, M.S. Epidemiology of AL amyloidosis: A real-world study using US claims data. Blood Adv. 2018, 2, 1046–1053. [Google Scholar] [CrossRef]
- Vaxman, I.; Gertz, M. Recent advances in the diagnosis, risk stratification, and management of systemic light-chain amyloidosis. Acta Haematol. 2019, 141, 93–106. [Google Scholar] [CrossRef]
- Gertz, M.A.; Dispenzieri, A. Systemic amyloidosis recognition, prognosis, and therapy: A systematic review. JAMA 2020, 324, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Gillmore, J.D.; Hawkins, P.N. Pathophysiology and treatment of systemic amyloidosis. Nat. Rev. Nephrol. 2013, 9, 574–586. [Google Scholar] [CrossRef] [PubMed]
- Palladini, G.; Schonland, S.; Merlini, G.; Milani, P.; Jaccard, A.; Bridoux, F.; Dimopoulos, M.A.; Ravichandran, S.; Hegenbart, U.; Roeloffzen, W.; et al. The management of light chain (AL) amyloidosis in Europe: Clinical characteristics, treatment patterns, and efficacy outcomes between 2004 and 2018. Blood Cancer J. 2023, 13, 19. [Google Scholar] [CrossRef]
- Kumar, S.K.; Gertz, M.A.; Lacy, M.Q.; Dingli, D.; Hayman, S.R.; Buadi, F.K.; Short-Detweiler, K.; Zeldenrust, S.R.; Leung, N.; Greipp, P.R.; et al. Recent improvements in survival in primary systemic amyloidosis and the importance of an early mortality risk score. Mayo Clin. Proc. 2011, 86, 12–18. [Google Scholar] [CrossRef]
- Manwani, R.; Cohen, O.; Sharpley, F.; Mahmood, S.; Sachchithanantham, S.; Foard, D.; Lachmann, H.J.; Quarta, C.; Fontana, M.; Gillmore, J.D.; et al. A prospective observational study of 915 patients with systemic AL amyloidosis treated with upfront bortezomib. Blood 2019, 134, 2271–2280. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Dispenzieri, A.; Lacy, M.Q.; Hayman, S.R.; Buadi, F.K.; Colby, C.; Laumann, K.; Zeldenrust, S.R.; Leung, N.; Dingli, D.; et al. Revised prognostic staging system for light chain amyloidosis incorporating cardiac biomarkers and serum free light chain measurements. J. Clin. Oncol. 2012, 30, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Dispenzieri, A.; Gertz, M.A.; Kyle, R.A.; Lacy, M.Q.; Burritt, M.F.; Therneau, T.M.; Greipp, P.R.; Witzing, T.E.; Lust, J.A.; Rajkumar, S.V.; et al. Serum cardiac troponins and N-terminal pro-brain natriuretic peptide: A staging system for primary systemic amyloidosis. J. Clin. Oncol. 2004, 22, 3751–3757. [Google Scholar] [CrossRef] [PubMed]
- Wechalekar, A.D.; Schonland, S.O.; Kastritis, E.; Gillmore, J.D.; Dimopoulos, M.A.; Lane, T.; Foli, A.; Foard, D.; Milani, P.; Rannigan, L.; et al. A European collaborative study of treatment outcomes in 346 patients with cardiac stage III AL amyloidosis. Blood 2013, 121, 3420–3427. [Google Scholar] [CrossRef] [PubMed]
- Muchtar, E.; Gertz, M.A.; Kumar, S.K.; Lacy, M.Q.; Dingli, D.; Buadi, F.K.; Grogan, M.; Hayman, S.R.; Kapoor, P.; Leung, N.; et al. Improved outcomes for newly diagnosed AL amyloidosis between 2000 and 2014: Cracking the glass ceiling of early death. Blood 2017, 129, 2111–2119. [Google Scholar] [CrossRef] [PubMed]
- Wechalekar, A.D.; Gillmore, J.D.; Hawkins, P.N. Systemic amyloidosis. Lancet 2016, 387, 2641–2654. [Google Scholar] [CrossRef] [PubMed]
- Gertz, M.A.; Comenzo, R.; Falk, R.H.; Fermand, J.P.; Hazenberg, B.P.; Hawkins, P.N.; Merlini, G.; Moreau, P.; Ronco, P.; Sanchorawala, V.; et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): A consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18–22 April 2004. Am. J. Hematol. 2005, 79, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Palladini, G.; Dispenzieri, A.; Gertz, M.A.; Kumar, S.; Wechalekar, A.; Hawkins, P.N.; Schonland, S.; Hegenbart, U.; Comenzo, R.; Kastritis, E.; et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: Impact on survival outcomes. J. Clin. Oncol. 2012, 30, 4541–4549. [Google Scholar] [CrossRef] [PubMed]
- Muchtar, E.; Dispenzieri, A.; Wisniowski, B.; Palladini, G.; Milani, P.; Merlini, G.; Scholand, S.; Veelken, K.; Hegenbart, U.; Geyer, S.M.; et al. Graded cardiac response criteria for patients with systemic light chain amyloidosis. J. Clin. Oncol. 2023, 41, 1393–1403. [Google Scholar] [CrossRef]
- Kumar, S.K.; Mikhael, J.R.; Buadi, F.K.; Dingli, D.; Dispenzieri, A.; Fonseca, R.; Gertz, M.A.; Greipp, P.R.; Hayman, S.R.; Kyle, R.A.; et al. Management of Newly Diagnosed Symptomatic Multiple Myeloma: Updated Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) Consensus Guidelines. Mayo Clin. Proc. 2009, 84, 1095–1110. [Google Scholar] [CrossRef]
- Kaplan, E.; Meier, P. Non-parametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Kristen, A.V.; Brokbals, E.; Aus dem Siepen, F.; Bauer, R.; Hein, S.; Aurich, M.; Riffel, J.; Behrens, H.M.; Kruger, S.; Schirmacher, P.; et al. Cardiac amyloid load: A prognostic and predictive biomarker in patients with light-chain amyloidosis. J. Am. Coll. Cardiol. 2016, 68, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Lee, S.P.; Kim, Y.J.; Sohn, D.W. Incidence, diagnosis and prognosis of cardiac amyloidosis. Korean Circ. J. 2013, 43, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Reece, D.E.; Hegenbart, U.; Sanchorawala, V.; Merlini, G.; Palladini, G.; Blade, J.; Fermand, J.P.; Hassoun, H.; Heffner, L.; Vescio, R.A.; et al. Efficacy and safety of once-weekly and twice- weekly bortezomib in patients with relapsed systemic AL amyloidosis: Results of a phase 1/2 study. Blood 2011, 118, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Kastritis, E.; Wechalekar, A.D.; Dimopoulos, M.A.; Merlini, G.; Hawkins, P.N.; Perfetti, V.; Gillmore, J.D.; Palladini, G. Bortezomib with or without dexamethasone in primary systemic (light chain) amyloidosis. J. Clin. Oncol. 2010, 28, 1031–1037. [Google Scholar] [CrossRef]
- Venner, C.P.; Lane, T.; Foard, D.; Rannigan, L.; Gibbs, S.D.J.; Pinney, J.H.; Whelan, C.J.; Lachmann, H.J.; Gilmore, J.D.; Hawkins, P.N.; et al. Cyclophosphamide, bortezomib, and dexamethasone therapy in AL amyloidosis is associated with high clonal response rates and prolonged progression-free survival. Blood 2012, 119, 4387–4390. [Google Scholar] [CrossRef] [PubMed]
- Jaccard, A.; Comenzo, R.L.; Hari, P.; Hawkins, P.N.; Roussel, M.; Morel, P.; Macro, M.; Pellegrin, J.L.; Lazaro, E.; Mohty, D.; et al. Efficacy of bortezomib, cyclophosphamide and dexamethasone in treatment-naive patients with high-risk cardiac AL amyloidosis (Mayo Clinic stage III). Haematologica 2014, 99, 1479–1485. [Google Scholar] [CrossRef] [PubMed]
- Sayago, I.; Krsnik, I.; Gomez-Bueno, M.; Garcia-Pavia, P.; Jaramillo, N.; Salas, C.; Mingo, S.; Oteo, J.F.; Alonso-Pulpon, L.; Segovia, J. Analysis of diagnostic and therapeutic strategies in advanced cardiac light-chain amyloidosis. J. Heart Lung Transplant. 2016, 35, 995–1002. [Google Scholar] [CrossRef]
- Palladini, G.; Kastritis, E.; Maurer, M.S.; Zonder, J.; Minnema, M.C.; Wechalekar, A.D.; Jaccard, A.; Lee, H.C.; Bumma, N.; Kaufman, J.L.; et al. Daratumumab plus CyBorD for patients with newly diagnosed AL amyloidosis: Safety run-in results of ANDROMEDA. Blood 2020, 136, 71–80. [Google Scholar] [CrossRef]
- Charliński, G.; Tyczyńska, A.; Małecki, B.; Fornagiel, S.; Barchnicka, A.; Kołkowska, A.; Kopińska, A.; Usnarska-Zubkiewicz, L.; Robak, P.; Waszczuk-Gajda, A.; et al. Risk factors and causes of early mortality in patients with newly diagnosed multiple myeloma in a “real-world” study: Experiences of the Polish Myeloma Group. Pol. Arch. Intern. Med. 2021, 131, 527–534. [Google Scholar] [CrossRef]
- Gertz, M.A.; Landau, H.; Comenzo, R.L.; Seldin, D.; Weiss, B.; Zonder, J.; Merlini, G.; Schonland, S.; Walling, J.; Kinney, G.G.; et al. First-in-human phase I/II study of NEOD001 in patients with light chain amyloidosis and persistent organ dysfunction. J. Clin. Oncol. 2016, 34, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Gertz, M.A.; Cohen, A.; Comenzo, R.; Kastritis, E.; Landau, H.; Libby, H.; Liedtke, M.; Sanchorawala, V.; Schonland, S.; Wechalekar, A.; et al. Survival benefit of birtamimab in Mayo Stage IV AL. Amyloidosis in phase 3 VITAL study was consistent across all key baseline variables. HemaSphere 2023, 7 (Suppl. S2), 41–42. [Google Scholar] [CrossRef]
- Gertz, M.A.; Tripuraneni, R.; Kinney, G.G. Birtamimab in patients with Mayo stage IV AL. Amyloidosis: Rationale for confirmatory Affirm-AL phase 3 study design. Blood 2021, 138 (Suppl. S1), 2754–2756. [Google Scholar] [CrossRef]
- Nuvolone, M.; Nevone, A.; Merlini, G. Targeting amyloid fibrils by passive immunotherapy in systemic amyloidosis. BioDrugs 2022, 36, 591–608. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.V.; Gould, J.; Langer, A.L.; Mapara, M.; Radhakrishnan, J.; Maurer, M.S.; Raza, S.; Mears, J.G.; Wall, J.; Solomon, A.; et al. Analysis of the phase 1a/b study of chimeric fibril-reactive monoclonal antibody 11-1f4 in patients with AL amyloidosis. Blood 2016, 128, 643. [Google Scholar] [CrossRef]
- Edwards, C.V.; Gould, J.; Langer, A.L.; Mapara, M.; Radhakrishnan, J.; Maurer, M.S.; Raza, S.; Mears, J.G.; Wall, J.; Solomon, A.; et al. Interim analysis of the phase 1a/b study of chimeric fibril-reactive monoclonal antibody 11-1f4 in patients with AL amyloidosis. Amyloid 2017, 24, 58–59. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.V.; Rao, N.; Bhutani, D.; Mapara, M.; Radhakrishnan, J.; Shames, S.; Maurer, M.S.; Leng, S.; Solomon, A.; Lentzsch, S.; et al. Phase 1a/b study of monoclonal antibody CAEL-101 (11-1f4) in patients with AL amyloidosis. Blood 2021, 138, 2632–2641. [Google Scholar] [CrossRef]
- Valent, J.; Liedtke, M.; Zonder, J.; Silowsky, J.; Kurman, M.; Daniel, E.; Jobes, J.; Harnet, M.; Bhattacharyya, A.; Quarta, C.C.; et al. Safety and tolerability of CAEL-101, an anti-amyloid monoclonal antibody, in combination with plasma cell dyscrasia therapy in patients with light-chain amyloidosis: Results from a phase 2 study. J. Am. Coll. Cardiol. 2022, 79 (Suppl. S9), 305. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | All Patients (n = 67) | Stage IIIa (n = 39; 58.2%) | Stage IIIb (n = 28, 41.8%) |
|---|---|---|---|
| n (%) or Median (Range) | n (%) or Median (Range) | n (%) or Median (Range) | |
| Male, n (%) | 36 (53.7) | 24 (61.5) | 12 (42.8) |
| Median age, years | 64 (41–83) | 63 (41–83) | 66 (41–83) |
| Distribution | |||
| <65 years | 36 (53.7) | 22 (56.4) | 14 (50.0) |
| ≥65 years | 31 (46.3) | 17 (43.6) | 14 (50.0) |
| ECOG PS, n = 63 | |||
| ≤1 | 26 (41.3) | 19 (52.8) | 7 (25.9) |
| >1 | 37 (58.7) | 17 (47.2) | 20 (74.1) |
| Comorbidities | |||
| 0/≥1 | 27 (40.3)/40 (59.7) | 18 (46.1)/21 (53.9) | 9 (32.1)/19 (67.9) |
| sFLC, n = 67 | |||
| lambda/kappa | 52 (77.6)/15 (22.4) | 32 (82.0)/7 (18.0) | 20 (71.4)/8 (28.6) |
| Heavy chain, n = 67 | |||
| IgG/IgA/IgM | 21 (31.3)/7 (10.4)/1 (1.5) | 14 (35.9)/5 (12.8)/0 (0.0) | 9 (32.1)/2 (7.1)/1 (3.6) |
| Other organ involvement | |||
| Kidneys, n = 66 | 42 (63.6) | 25 (64.1) | 17 (63.0) |
| Liver, n = 59 | 10 (16.9) | 5 (14.7) | 5 (20.0) |
| Peripheral neuropathy, n = 60 | 10 (16.7) | 6 (16.7) | 4 (16.7) |
| Autonomic neuropathy, n = 59 | 13 (22.0) | 6 (17.1) | 7 (29.2) |
| Gastrointestinal tract, n = 56 | 9 (16.1) | 5 (14.7) | 4 (18.2) |
| Cytogenetics | |||
| High-risk cytogenetics, n = 37 | 12 (32.4) | 8 (38.1) | 4 (25.0) |
| t(11;14) | 12 (32.4) | 7 (33.3) | 5 (31.2) |
| First-line chemotherapy | |||
| Bort-based | 64 (95.5) | 38 (97.4) | 26 (92.8) |
| Vd/VCd/Vd + IMiD | 28 (43.7)/25 (39.0)/11 (17.3) | 15 (39.5)/15 (39.5)/8 (21.0) | 13 (50.0)/10 (38.5)/3 (11.5) |
| IMiD-based (CTd, Rd) | 3 (4.5) | 1 (2.6) | 2 (7.2) |
| Daratumumab | 14 (20.9) | 8 (20.5) | 6 (21.4) |
| ASCT | 10 (14.9) | 9 (23.1) | 1 (3.6) |
| Laboratory parameters | |||
| CPBM > 10%, n = 67 | 20 (32.2) | 13 (33.3) | 7 (25.0) |
| Serum Hb (g/dL), n = 67 | 12.8 (7.7–17.5) | 12.7 (10.6–16.2) | 12.8 (7.7–17.5) |
| WBC count (×103/μL), n = 67 | 8.4 (3.8–17.1) | 8.2 (4.0–17.1) | 8.7 (3.8–16.4) |
| PLT count (×103/μL), n = 67 | 250.0 (114.0–624.0) | 260.0 (117.0–620.0) | 250.0 (114.0–624.0) |
| Serum albumin (mg/L), n = 67 | 3.2 (1.0–4.6) | 3.3 (1.0–4.6) | 3.2 (1.1–4.5) |
| Serum β2-microglobulin (mg/L), n = 49 | 4.0 (1.7–32.0) | 3.0 (1.7–18.0) | 5.5 (2.6–32.0) |
| sFLC lambda (mg/dL), n = 66 | 56.9 (0.7–7411.8) | 54.8 (0.7–1493.0) | 52.0 (0.9–7411.8) |
| sFLC kappa (mg/dL), n = 64 | 15.8 (0.2–3730.0) | 13.6 (0.5–588.0) | 16.0 (0.2–3730.0) |
| Serum LDH (IU/L), n = 49 | 267.0 (161.0–1021.0) | 250.0 (170.0–758.0) | 277.0 (161.0–1021.0) |
| Baseline echocardiography | 64 (95.5) | 39 (100.0) | 25 (89.3) |
| Baseline cardiac magnetic resonance | 31 (46.3) | 22 (56.4) | 9 (32.1) |
| Baseline endomyocardial biopsy | 15 (22.7) | 7 (17.9) | 8 (28.6) |
| Parameters | All Patients (n = 67) | Stage IIIa (n = 39; 58.2%) | Stage IIIb (n = 28; 41.8%) |
|---|---|---|---|
| n (%) or Median (Range) | n (%) or Median (Range) | n (%) or Median (Range) | |
| NYHA FC, grade, n = 58 | |||
| 1 | 3 (5.2) | 2 (6.3) | 1 (3.8) |
| 2 | 26 (44.8) | 14 (43.7) | 12 (46.2) |
| 3 | 24 (41.4) | 15 (46.9) | 9 (34.6) |
| 4 | 5 (8.6) | 1 (3.1) | 4 (15.4) |
| SBP (mmHg), n = 43 | 105 (32–152) | 105 (32–135) | 110 (70–152) |
| <100 mmHg | 16 (37.2) | 10 (37.0) | 6 (37.5) |
| LVEF (%), n = 60 | |||
| <50% | 14 (20.9) | 9 (25.0) | 5 (20.8) |
| ≥50% | 46 (68.7) | 27 (75.0) | 19 (79.2) |
| Cardiac Troponin T (μg/L), n = 24 | 54.5 (0.05–397.0) | 58.0 (0.07–242.0) | 97.8 (0.05–397.0) |
| ≥0.025 μg/L | 24 (100.0) | 15 (100.0) | 9 (100.0) |
| High sensitivity Troponin T (ng/L), n = 22 | 98.1 (45.0–566.0) | 68.5 (45.0–298.0) | 220.4 (57.0–566.0) |
| ≥40 ng/L | 22 (100.0) | 12 (100.0) | 10 (100.0) |
| Cardiac Troponin I (μg/L), n = 19 | 0.26 (0.02–4.7) | 0.23 (0.02–4.7) | 0.35 (0.04–0.36) |
| ≥0.1 μg/L | 15 (78.9) | 9 (75.0) | 6 (85.7) |
| NT-proBNP (ng/L), n = 67 | 6832.0 (655.0–70,000.0) | 4376.0 (655.0–8081.0) | 16,011.0 (8735.0–70,000.0) |
| ≥8500 μg/L | 28 (41.8) | 0 (0.0) | 28 (100.0) |
| Response | All Patients, n (%) | Stage IIIa, n (%) | Stage IIIb, n (%) |
|---|---|---|---|
| Hematological responses, n = 52 | |||
| Overall response rate | 37 (71.1) | 24 (75.0) | 13 (65.0) |
| Complete response | 15 (28.8) | 12 (37.6) | 3 (15.0) |
| Very good partial response | 9 (17.3) | 6 (18.7) | 3 (15.0) |
| Partial response | 13 (25.0) | 6 (18.7) | 7 (35.0) |
| No response | 15 (28.9) | 8 (25.0) | 7 (35.0) |
| Cardiac responses, n = 52 | |||
| Overall response rate | 20 (38.5) | 13 (40.6) | 7 (35.0) |
| Complete response | 3 (5.8) | 3 (9.4) | 0 (0.0) |
| Very good partial response | 2 (3.8) | 0 (0.0) | 2 (10.0) |
| Partial response | 15 (28.8) | 10 (31.2) | 5 (25.0) |
| No response | 32 (61.5) | 19 (59.4) | 13 (65.0) |
| Hematological and cardiac response, n = 50 | |||
| ≥hematological VGPR +≥cardiac PR | 13 (26.0) | 10 (33.3) | 3 (15.0) |
| Parameters | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age ≥ 65 years | 1.76 (0.88–3.53) | 0.104 | ||
| Male | 1.06 (0.53–2.11 | 0.867 | ||
| Comorbidities ≥ 1 | 1.39 (0.81–2.38) | 0.226 | ||
| ECOG PS > 1 | 0.41 (0.18–0.92) | 0.032 | 0.23 (0.06–0.84) | 0.026 |
| NYHA FC > 2 | 2.54 (1.12–5.79) | 0.025 | 4.33 (1.09–17.21) | 0.037 |
| Stage IIIb at diagnosis | 2.25 (1.10–4.60) | 0.025 | 1.65 (0.56–4.84) | 0.36 |
| Clonal plasma cells in bone marrow ≥ 10% | 0.88 (0.41–1.86) | 0.739 | ||
| High-risk cytogenetic abnormalities | 2.62 (0.96–7.17) | 0.061 | ||
| ASCT treatment | 3.05 (1.12–8.25) | 0.028 | 0.35 (0.04–2.79) | 0.33 |
| Hematologic response ≥ VGPR | 0.21 (0.08–0.56) | 0.002 | 0.26 (0.08–0.83) | 0.023 |
| Cardiac response ≥ PR | 0.19 (0.06–0.58) | 0.003 | 0.06 (0.01–0.34) | 0.001 |
| Hematologic response ≥ VGPR + Cardiac response ≥ PR | 3.89 (1.79–8.41) | <0.001 | 4.30 (1.97–9.38) | <0.001 |
| Renal involvement | 0.97 (0.48–1.99) | 0.945 | ||
| Liver involvement | 1.81 (0.68–4.82) | 0.236 | ||
| GI tract involvement | 2.44 (1.03–5.80) | 0.042 | not included | |
| PN involvement | 1.45 (0.62–3.40) | 0.393 | ||
| Organs involved > 2 at diagnosis | 0.53 (0.18–1.52) | 0.238 | ||
| Hb < 12 g/dL | 1.38 (0.67–2.83) | 0.383 | ||
| SBP < 100 mmHg | 0.52 (0.18–1.45) | 0.209 | ||
| Serum albumin < 3.5 g/dL | 1.46 (0.65–3.29) | 0.352 | ||
| Serum β2-microglobulin ≥ 5.5 mg/L | 1.46 (0.66–3.25) | 0.346 | ||
| LDH > ULN | 2.47 (0.81–7.49) | 0.108 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charliński, G.; Steinhardt, M.; Rasche, L.; Gonzalez-Calle, V.; Peña, C.; Parmar, H.; Wiśniewska-Piąty, K.; Dávila Valls, J.; Olszewska-Szopa, M.; Usnarska-Zubkiewicz, L.; et al. Outcomes of Modified Mayo Stage IIIa and IIIb Cardiac Light-Chain Amyloidosis: Real-World Experience in Clinical Characteristics and Treatment—67 Patients Multicenter Analysis. Cancers 2024, 16, 1592. https://doi.org/10.3390/cancers16081592
Charliński G, Steinhardt M, Rasche L, Gonzalez-Calle V, Peña C, Parmar H, Wiśniewska-Piąty K, Dávila Valls J, Olszewska-Szopa M, Usnarska-Zubkiewicz L, et al. Outcomes of Modified Mayo Stage IIIa and IIIb Cardiac Light-Chain Amyloidosis: Real-World Experience in Clinical Characteristics and Treatment—67 Patients Multicenter Analysis. Cancers. 2024; 16(8):1592. https://doi.org/10.3390/cancers16081592
Chicago/Turabian StyleCharliński, Grzegorz, Maximilian Steinhardt, Leo Rasche, Veronica Gonzalez-Calle, Camila Peña, Harsh Parmar, Katarzyna Wiśniewska-Piąty, Julio Dávila Valls, Magdalena Olszewska-Szopa, Lidia Usnarska-Zubkiewicz, and et al. 2024. "Outcomes of Modified Mayo Stage IIIa and IIIb Cardiac Light-Chain Amyloidosis: Real-World Experience in Clinical Characteristics and Treatment—67 Patients Multicenter Analysis" Cancers 16, no. 8: 1592. https://doi.org/10.3390/cancers16081592