1. Introduction
Lung cancer—ranking second among all cancers—remains the main cause of cancer deaths and is among the top five causes of death worldwide with NSCLC being the most common subtype of lung cancer [
1]. In 2020, more than two million people were diagnosed with lung cancer worldwide. While the 5-year survival rate for general NSCLC is currently 28% (33% in women and 23% in men), the 5-year survival rate of metastatic NSCLC is 9% with higher survival rates in those patients receiving targeted or immunotherapies [
1,
2].
Immune checkpoint blockade (ICB) as a type of immunotherapy aims to unleash the immune system of the body to identify and combat cancer cells. ICB has shown promising results in the treatment of various types of cancers, with NSCLC among them. It works through the targeting of cytotoxic T-lymphocyte antigen-4 (CTLA-4), programmed cell death protein 1 (PD-1), or programmed death-ligand 1 (PD-L1), known as immune checkpoints, which inhibit immune response [
3,
4] and can be employed by cancer cells to escape attacks from the immune system.
Recent advances in ICB research and development have significantly improved options and outcomes for NSCLC patients including (a) the approval of ICB as first-line combinational or monotherapy in stage IV NSCLC without driver alterations depending on PD-L1 expression [
5,
6,
7,
8] or as an adjuvant therapy in non-metastatic NSCLC for certain conditions [
9,
10]; (b) the enhanced biomarker development including tumour mutational burden and microsatellite instability [
11]; (c) ICB’s combination with other targeted, immuno-, chemo- or radiotherapy [
8]; (d) the exploration and development of novel immune checkpoint inhibitors, multispecific antibodies, and other immunomodulatory agents as well as the exploration of new immune regulation pathways [
12,
13]. To maximise the efficacy and minimise the toxicity of ICB or the development of resistance, ongoing research is being continued for the optimisation of immunotherapy approaches including personalised therapy strategies and research on immune evasion pathways, tumour microenvironment factors and host immune response [
2,
14,
15].
A number of immune checkpoint inhibitors have already received approval in Europe for first-line therapies in the field of advanced or metastasised NSCLCs [
16,
17,
18,
19,
20,
21]. Pembrolizumab is approved as (a) an adjuvant treatment after complete resection and platinum-based chemotherapy in NSCLC patients with a high recurrence prognosis; (b) a first-line therapy in metastatic high-PD-L1 (≥50% TPS) NSCLC without EGFR mutations or ALK translocations; (c) a first-line PD-L1 status-independent therapy combined with platinum-based chemotherapy in metastatic squamous NSCLC; (d) a first-line PD-L1 status-independent treatment in combination with platinum-based chemotherapy in metastatic non-squamous NSCLC with no EGFR or ALK aberrations; and (e) a second-line therapy of locally advanced or metastatic low-PD-L1 (≥1%)-expressing NSCLC following chemotherapy in patients with EGFR or ALK aberrations following targeted therapy [
16]. Nivolumab is approved as a first-line therapy in combination with ipilimumab and two cycles of platinum-based chemotherapy in metastatic NSCLC without EGFR or ALK aberrations [
18]. In addition, nivolumab can be given as a monotherapy in locally advanced or metastasised NSCLC after chemotherapy or in the neo-adjuvant setting in resectable, low-PD-L1 (≥1%) NSCLC [
18]. Cemiplimab is approved in Europe as a first-line therapy of locally advanced or metastatic low-(≥1%) or high-PD-L1 (≥50% TPS) NSCLC without EGFR, ALK, or ROS aberrations and only when not indicated for definitive radiochemotherapy [
19]. Atezolizumab is approved in Europe as a first-line therapy in metastatic NSCLC with no EGFR or ALK aberrations (a) in tumours with a high (≥50%) PD-L1 status or ≥10% tumour-infiltrating cells; (b) as a combinational therapy with nab paclitaxel and carboplatin in non-squamous tumours; or (c) as a combinational therapy with bevacizumab, paclitaxel, or carboplatin in non-squamous tumours. The utilisation of the latter combination is allowed as well in EGFR- or ALK-positive non-squamous NSCLC but only after the failure of targeted therapy [
20]. Lastly, durvalumab is approved in Europe as a first-line therapy combined with tremelimumab and platinum-based chemotherapy in stage IV NSCLC without EGFR or ALK aberrations. In addition, durvalumab can be applied in non-resectable advanced low-PD-L1 (≥1%) NSCLC without progression after platinum-based radiochemotherapy [
21]. Thus, the first-line application of anti-PD-1/PD-L1 treatments has developed broadly and has led to important improvements in the survival rates and health-related quality of life of the patients during the recent decade reflecting the grand efforts in finding a more effective therapy for this devastating disease.
Viscum album L. (European white-berry mistletoe, VA) is approved in Germany for subcutaneous adjuvant and palliative treatment in malignant tumour diseases [
22,
23,
24,
25] and systematic reviews and meta-analyses reveal a significant medium-size effect in the improvement of health-related quality of life and fatigue [
26,
27,
28,
29,
30]. In addition, add-on VA has been associated in various studies and clinical studies with the improvement of survival [
31,
32,
33,
34,
35]. Hereby, the anti-proliferative [
36], pro-apoptotic [
37], immunomodulatory [
38,
39,
40,
41,
42], anti-nociceptive, and anti-depressant [
43] properties of the VA extracts seem to play a role. Two recent systematic reviews and meta-analyses revealed improved survival in oncological patients treated with add-on VA therapy—the reduction in hazard of death ranged from 19% (HR 0.81, 95% CI: 0.69–0.95,
p = 0.01) to 41% (HR 0.59, 95% CI: 0.53–0.65,
p < 0.0001) [
35,
44]. Furthermore, VA in addition to standard oncological chemotherapy revealed to be associated with improved overall survival in advanced or metastasised NSCLC patients [
31,
45,
46,
47]. So far, the association of combined PD-1/PD-L1 inhibitor plus add-on VA therapy with survival outcomes of advanced or metastasised NSCLC patients has not been studied systematically. First real-world evidence (RWE) results documented no enhanced adverse effects when VA was given in addition to PD-1/PD-L1 inhibitor therapy in patients with advanced or metastasised melanoma or lung cancer [
48,
49,
50,
51]. Furthermore, in another small RWE study with advanced or stage IV lung cancer patients, the PD-1 inhibitor-induced toxicity was almost halved when VA was added [
49].
The aim of our study was to investigate the overall survival of advanced or metastasised NSCLC patients receiving ICB as outlined above with or without VA.
4. Discussion
In the present study, we examined the efficacy of PD-1/PD-L1 inhibitor therapy in combination with add-on VA therapy in patients with advanced or metastatic NSCLC. Our findings indicate a significant association with survival benefits for these patients when treated with ICB in combination with VA therapy in comparison to ICB alone. Hereby, add-on VA reduced the adjusted hazard of death by 40%. Our findings comply with the results of two systematic reviews and meta-analyses stating a reduction in the general hazard of death in oncological patients after add-on VA therapy between 19% and 54% [
35,
44]. As to NSCLC patients, our findings mimic the effect of another RWD study in stage IV patients who were treated with standard chemotherapy and where add-on VA therapy reduced the hazard of death by 56% [
31]. However, neither the above-mentioned systematic reviews nor the RWD study included anti-PD-1, -PD-L1, or -CLT-4A treatments for the evaluation of the association with survival. Thus, our study is the first of its kind, giving the first insights into this research.
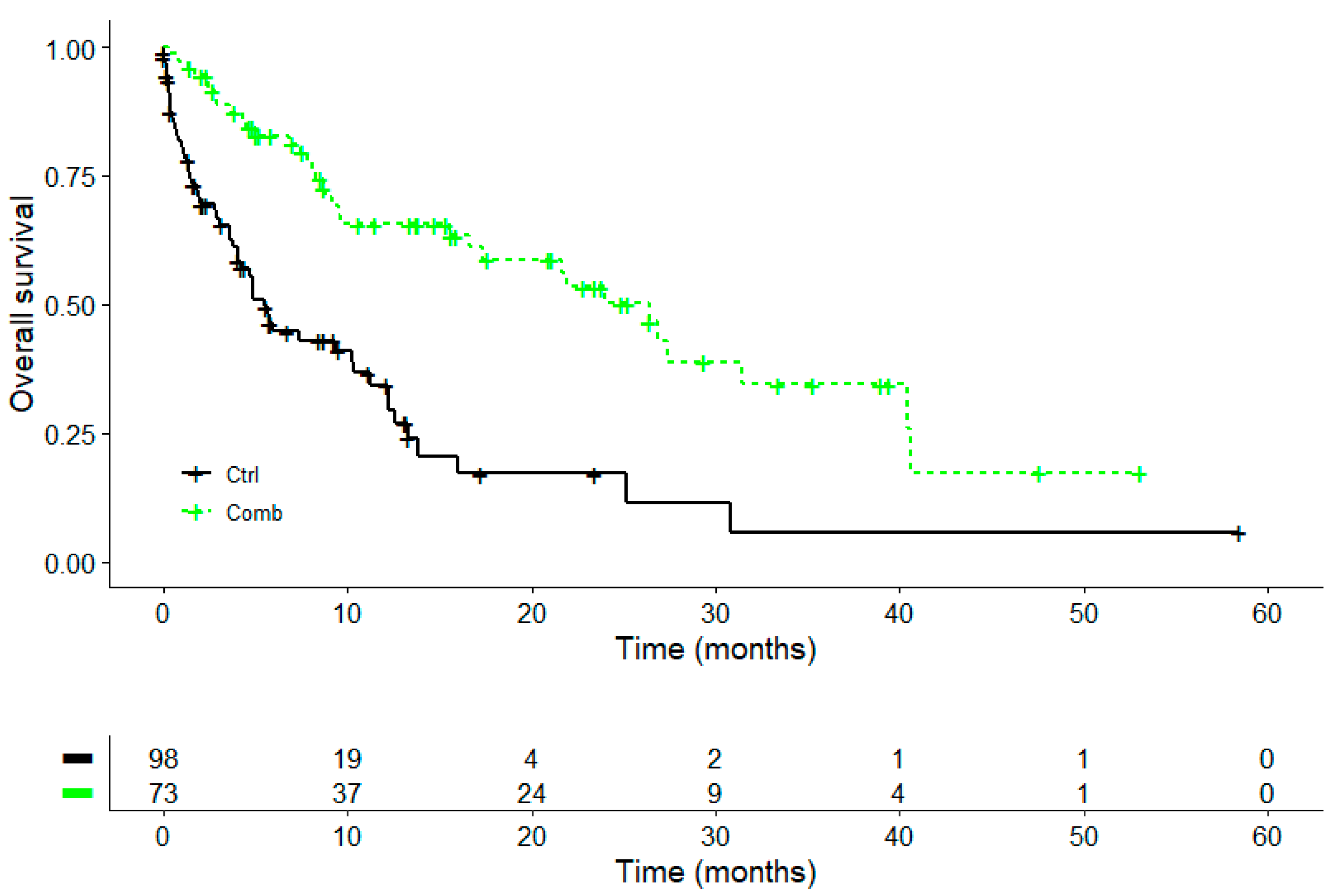
The overall survival in the present study was 13.8 months in the combination group (ICB + add-on VA) compared to 6.8 months in the control group (ICB), and the difference was significant. When comparing our findings with published RWD studies involving ICB treatment in general, we found comparable results. One study reported a median overall survival of stage I-IV NSCLC patients of 9.3 months (95% CI 8.5–10.5 months) after the start of immune checkpoint inhibitors with 4.4% fewer ECOG ≥ 2 patients compared to our study [
57]. Another RWD study observed an overall survival between 13.2 months (PD-L1 TPS < 1%) and 16.3 months (PD-L1 TPS 1–49%) in metastatic non-squamous NSCLC patients with an ECOG performance status from 0 to 1 who were treated with pembrolizumab plus pemetrexed–carboplatin [
58].
Due to different patient cohort characteristics, RWD findings are not directly comparable to survival parameters of current randomised controlled trials (RCTs). Thus, the one-year survival rate of 68.8% in ICB treatment of the Keynote-042 RCT is higher compared to the one-year survival rate in our cohort (34.4%). This could be driven by the fact that our cohort more closely mirrors a real-world NSCLC cohort with an older patient population (68 years) in line with the median age of NSCLC patients [
59] in the national cancer database (69 years) in comparison to the Keynote-042 trials (63 years) [
60]. Furthermore, the proportion of patients with a histological squamous cell cancer type in our study, 27.2%, mirrors the real-world situation of 28% [
59] better than the 55% recorded in the Keynote-042 China trial [
61]. Last but not least, our cohort included patients with all ECOG levels compared to the Keynote-042, where only patients with ECOG 0-1 were included [
60]. In one of the first head-to-head comparison studies between RCT and RWE studies, shorter OS has been observed in RWE studies for real-world first-line pembrolizumab therapy in stage IV NSCLC, partly due to a higher number of patients with performance status ≥ 2 in RWE studies [
62]. Therefore, the findings of our study may reveal a real-world situation for NSCLC patients and do not reflect eligibility procedures in RCTs using strict inclusion criteria. In addition, our RWE study included first- as well as second-line ICB treatment. All mentioned factors may, therefore, account for the poorer observed curves in our study in general.
The multivariable regression analysis in our study indicated that the additional VA therapy was associated with a significant reduction in the adjusted hazard of death in advanced or metastasised NSCLC patients treated with ICB. This effect was independent of age, gender, tumour stage, surgery, ECOG status, BMI, comorbidity status, smoking status, cranial irradiation, or PD-L1 TPS. However, when evaluating a subgroup where only NSCLC patients with PD-L1 TPS ≥ 1% and first-line ICB were included, the add-on VA was associated with a reduction in the adjusted hazard of death (56%) compared to the general cohort (40%) as well. Therefore, one might speculate that VA extracts may trigger or mediate a PD-L1-dependent or -mediated immune response in NSCLC patients. This hypothesis is supported by in vitro research where VA extracts downregulated PD-L1 expression in 3D spheroids of breast cancer cell lines T47D and HCC1937 [
63]. At the same time, no negative effect of VA therapy on the effect of atezolizumab or pembrolizumab was observed [
63]. These in vitro data suggest that VA extracts are involved in the mediation of PD-L1-regulated processes in cancer cells. However, these data need further confirmatory analyses [
63].
In vitro and in vivo studies revealed that the escape of potentially immunogenic tumours from the immune response of the host is mainly driven by the activation of the PD-1/PD-L1 signalling pathway [
64,
65,
66]. While PD-1 was already known in the early 1990s as being expressed in lieu of apoptosis induction [
66], it was later identified as a co-inhibitory molecule for T-cell activation, being involved in the negative regulation of apoptotic immunological reactions by binding to PD-L1 [
67]. While PD-L1 binding to PD-1 leads to impaired anti-tumour activity, it was shown for lung cancer that this involved the activation of the AKT/ß-catenin/WIP signalling pathway [
68]. Some studies suggest that VA extracts may also inhibit phosphoinositide 3-kinase (P13K), thereby affecting the downstream AKT signalling [
69,
70,
71,
72,
73]. The AKT pathway is involved in the regulation of apoptosis; thus, VA’s effects on this pathway could be attributed to its pro-apoptotic properties. Therefore, combining immune checkpoint inhibitors and VA could potentially synergistically target identical or multiple checkpoints and immune regulatory pathways, leading to a comprehensive and effective, i.e., stronger, inhibition of tumour growth. But beyond these hypotheses, the specific mode of action concerning how both treatment modalities act to increase survival of advanced or metastasised NSCLC patients still needs to be elucidated further.
We were unable to consider the association between EGFR mutations and overall survival in our study because only a small number of patients had EGFR mutations. However, our adjusted multivariable Cox regression analysis revealed a positive direction of the hazard of death, i.e., the probability of death is increased in the presence of common EGFR mutations. The efficacy of ICB can be influenced by the expression and activity of immune-related molecules which in turn are influenced by driver aberrations such as EGFR, ALK, KRAS, or others. It has been shown that, e.g., in EGFR-mutant lung cancer, the EGFR signalling pathway is activated, leading likely to an uninflamed tumour microenvironment [
74] due to the lowered activity of pro-inflammatory interleukins such as IL-6, IL-8, or TNF-α and due to the increased activity of immunosuppressive factors such as TGF-β, resulting in tumour escape or immunosuppression. Thus, these patients do not benefit from ICB therapy. TKI-treated NSCLCs with EGFR mutation often develop resistance which may limit therapy’s efficacy, mostly due to secondary mutations or compensatory pathways. The latter of the two adaptive mutability routes includes the activation of pharmacologically sensitive endogenous genes that enable continuous error-prone DNA replication in order to tolerate cancer therapy. Blocking involved genes or proteins may overcome these resistance mechanisms [
75,
76]. One of these proteins is the tyrosine kinase receptor Axl which activates intrinsic mutators and helps tumour cells evade tyrosine kinase inhibition [
76]. The treatment of NSCLC cell lines with EGFR TKI resulted in Axl overexpression, the viability of tumour cells, and the inhibition of apoptotic pathways. It was observed in in vitro, in vivo experiments, and patient samples that Axl-mediated TKI induction of error-prone DNA polymerases and the acceleration of common EGFR resulted in drug resistance. In patient-derived xenografts, this effect was reversed through anti-Axl therapy [
75]. The resistance to ICB is an emerging area in cancer therapy. Axl, which has been correlated to immune suppression, resistance to immunity, and lower response rates, was shown to be strongly associated with the PD-1 expression of the tumour. When treated with PD-1 inhibitors, tumours with high Axl expression revealed lower response rates and a trend toward shorter progression-free survival [
77]. In addition, the activation of TAM receptors including Axl negatively modified the immune response, leading to an immunosuppressive and pro-tumorigenic tumour microenvironment, suggesting the combination of TAM receptor inhibitors and checkpoint inhibitors as long-term clinical therapeutic strategies in NSCLC [
76,
78]. Thus, combinational ICB strategies will play a pivotal role in the future to effectively reduce tumour cell survival and metastatic potential.
Lastly, in our study, we observed that an increased ECOG level was associated with an increased adjusted hazard of death while the occurrence of a co-morbidity at baseline was associated with a reduced adjusted hazard. The first association observed is in line with a systematic review and meta-analysis of real-world data covering data from 19 studies and 3600 NSCLC patients, showing that patients with a performance score ≥ 2 had a worse outcome in terms of OS, progression-free survival, and overall response rate [
79]. The latter association in our study that the occurrence of a comorbidity is associated with a better survival outcome does not seem plausible at first sight. However, a recent real-world data study on 431 advanced cancer patients treated with PD-1/PD-L1 inhibitors revealed that (a) ≥grade 3/4 immune-related adverse events (irAEs) are affected by comorbidities including diabetes mellitus and others and that (b) patients with these ≥grade 3/4 irAEs revealed an improved progression-free survival (PFS) compared to patients without any adverse events [
80]. This is in accordance with a recent systematic review and meta-analysis of 24 studies which showed that developing irAEs during PD-1/PD-L1 therapy was significantly associated with a 26% and 45% reduced hazard for OS and PFS, respectively, with endocrine, skin, gastrointestinal, and low-grade irAEs showing the best outcomes [
81].
In the combinational setting of the present study, ICB with add-on VA was started in the first-line setting a median of 24 days after NSCLC diagnosis. Until now, no systematic research on the combinational ICB plus VA therapy and timing exists in the literature, with our data providing the first data on this topic so far. For other combinations including chemotherapy and add-on VA, findings of an RCT reported an application start of the combination 1 week after surgery with a duration of 23 weeks in patients with gastric cancer [
82]. Another study, a real-world data study, revealed an effective application duration of add-on VA at a minimum of four weeks alongside chemotherapy in advanced or metastasised NSCLC patients, and the adjusted hazard was further reduced when add-on VA duration was prolonged to greater than sixteen weeks [
31]. Add-on VA can be applied directly following a tumour diagnosis in an adjuvant setting during chemo- and/or radiochemotherapy, helping to improve patient health-related quality of life by reducing the adverse effects of standard oncological therapies [
30,
83,
84].
Several systematic reviews and meta-analyses, clinical as well as real-world data studies, point towards the positive impact of VA extracts on survival [
31,
32,
33,
34,
35,
44,
46,
47], indicating that clinical findings with survival-improving effects of add-on VA in cancer patients are accumulating. Besides being effectively used in combination with radio-/and or chemotherapy [
30,
31,
83], VA in combination with targeted therapy is associated with (i) a well-documented safety profile [
48,
49,
50,
51]; (ii) a significant reduction in adverse effects in cancer patients treated with monoclonal antibodies [
85]; (iii) a reduction by approximately 50% in adverse event rates in patients with advanced or metastasised lung cancer treated with anti-PD-1 agents [
49]; and (iv) improved ability to continue standard cancer therapy in patients treated with targeted therapies [
51]. Thus, the synergistic association between combinatory PD-1/PD-L1 inhibitors and VA therapy in patients with advanced or metastasised NSCLC as observed in the present study joins the ranks of previous achievements.
Limitations
The non-randomised nature of the present real-world data study limits our results. However, the confounding bias was reduced by applying adjusted multivariable logistic regression methods addressing potential confounders. It is worth noting that our findings suggest a correlation between add-on VA application and improved survival in advanced NSCLC patients receiving PD-1/PD-L1 inhibitors but do not establish causation. However, our data study mirrors the real-world application situation of PD-1/PD-L1 inhibitor therapy in NSCLC patients in standard clinical practice and is the first of its kind showing a positive survival association between combinatory PD-1/PD-L1 inhibitor and VA therapy. Owing to the real-world nature of our study, the occurrence of comorbidity (not distinguished between specific comorbidity variables) was documented. In the future, it will be necessary to detect further comorbidity conditions influencing combinational treatment response. Lastly, evaluated molecular markers in our cohort may not represent the current molecular marker panel as the RWE study started in 2015 and has been developed since. Further markers such as AXL, HER2, HER3, MERTK, VIM, and RAD18 or error-prone polymerases could be examined in further clinical trials evaluating resistance or compensatory pathways and how they are affected by the combinational PD-1/PD-L1 and add-on VA therapy in advanced or metastasised NSCLC patients. Prospective and randomised controlled trials are warranted to validate these findings and better understand the specific impact of combinatory PD-1/PD-L1 inhibitor plus VA therapy in lung cancer treatment.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}