
Imiquimod Is Effective in Reducing Cervical Intraepithelial Neoplasia: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Literature Search and Eligibility Criteria
2.3. Selection Process and Data Collection
2.4. Risk of Bias and Quality Assessment of Included Articles
2.5. Synthesis Methods
3. Results
3.1. Search and Selection
3.2. Basic Characteristics of Included Studies
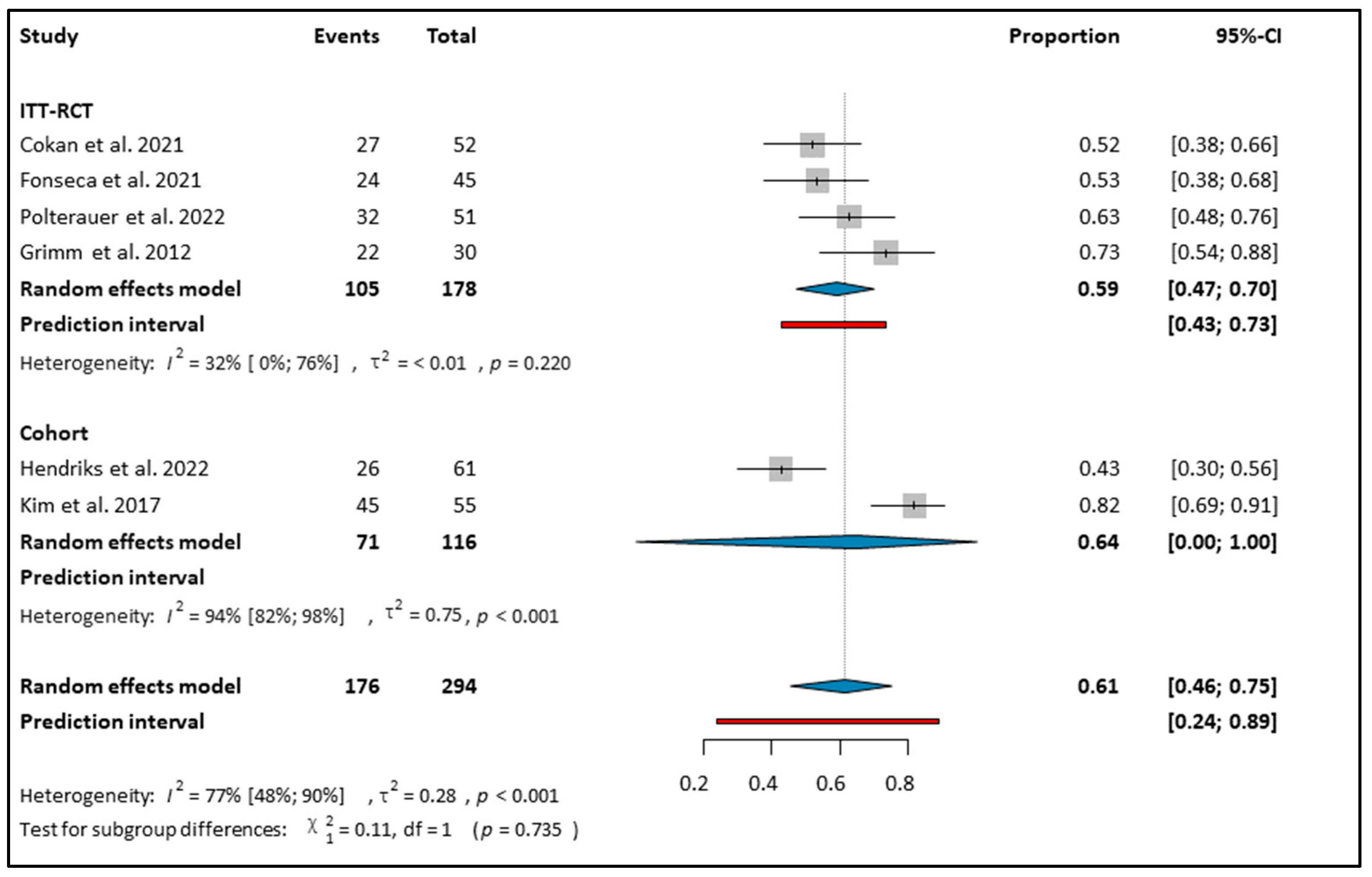
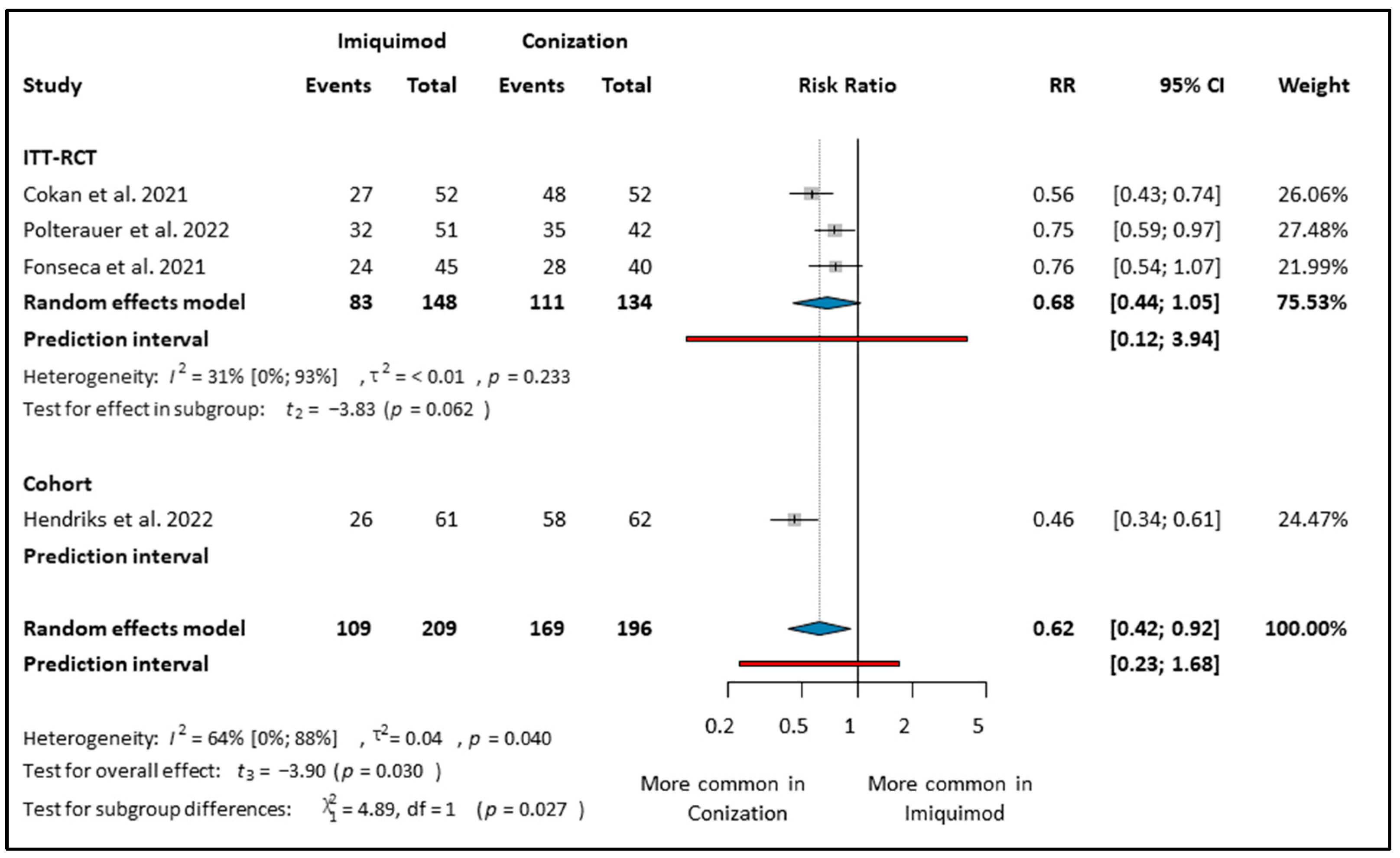
3.3. CIN 2–3 Regression
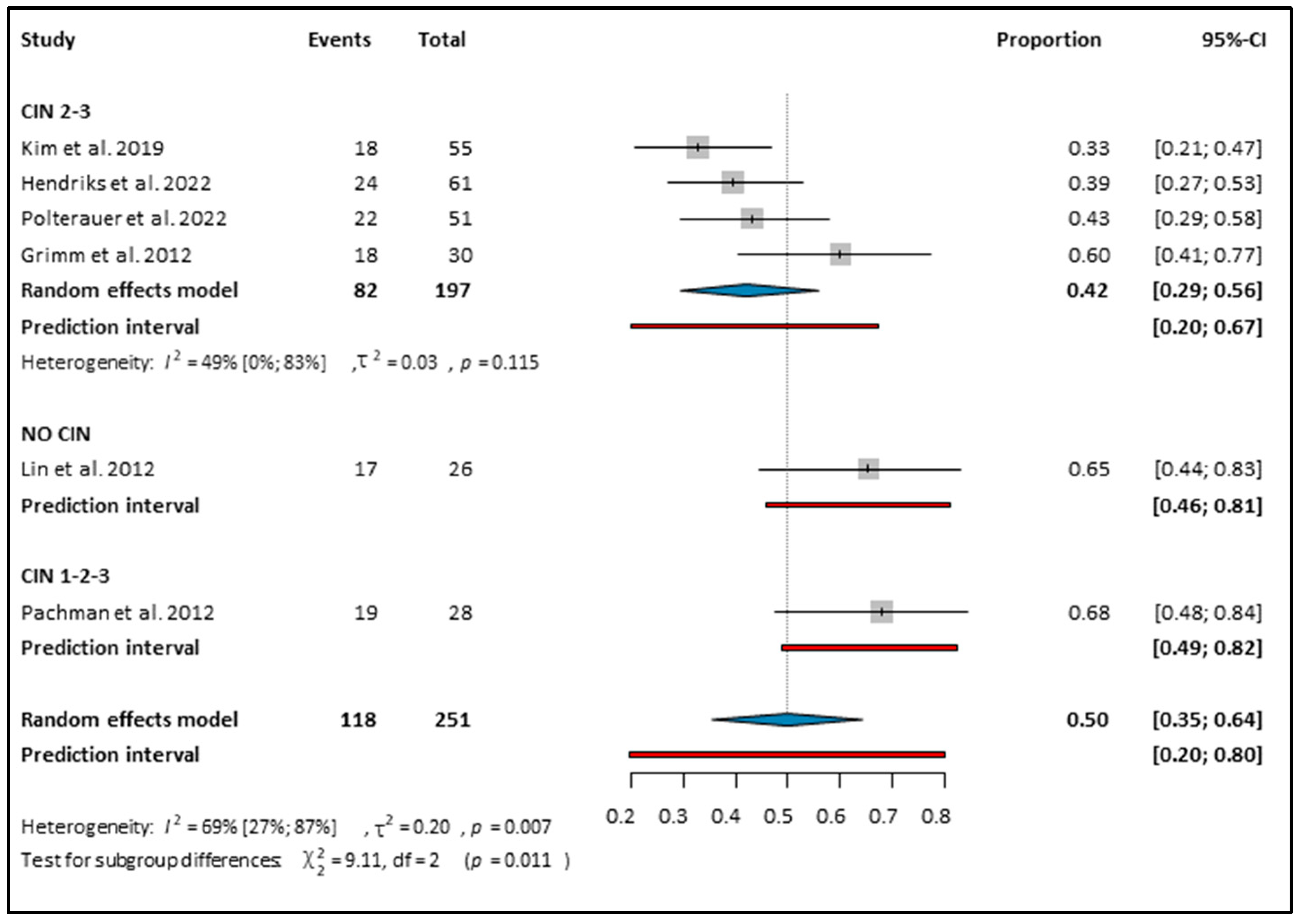
3.4. Imiquimod on HPV Clearance
3.5. Adverse Events
3.6. Risk of Bias Assessment and GRADE
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Practice and Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Okunade, K.S. Human papillomavirus and cervical cancer. J. Obstet. Gynaecol. 2020, 40, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Loopik, D.L.; Bentley, H.A.; Eijgenraam, M.N.; IntHout, J.; Bekkers, R.L.M.; Bentley, J.R. The Natural History of Cervical Intraepithelial Neoplasia Grades 1, 2, and 3: A Systematic Review and Meta-analysis. J. Low. Genit. Tract. Dis. 2021, 25, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.B.; Guido, R.S.; Castle, P.E.; Chelmow, D.; Einstein, M.H.; Garcia, F.; Huh, W.K.; Kim, J.J.; Moscicki, A.B.; Nayar, R.; et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J. Low. Genit. Tract. Dis. 2020, 24, 102–131. [Google Scholar] [CrossRef] [PubMed]
- Weinmann, S.; Naleway, A.; Swamy, G.; Krishnarajah, G.; Arondekar, B.; Fernandez, J.; Myers, E. Pregnancy Outcomes after Treatment for Cervical Cancer Precursor Lesions: An Observational Study. PLoS ONE 2017, 12, e0165276. [Google Scholar] [CrossRef] [PubMed]
- Lieb, J.A.; Mondal, A.; Lieb, L.; Fehm, T.N.; Hampl, M. Pregnancy outcome and risk of recurrence after tissue-preserving loop electrosurgical excision procedure (LEEP). Arch. Gynecol. Obstet. 2023, 307, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Di Donato, V.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Lopez, S.; Simoncini, T.; Plotti, F.; Casarin, J.; Serati, M.; et al. Recurrence rate after loop electrosurgical excision procedure (LEEP) and laser Conization: A 5-year follow-up study. Gynecol. Oncol. 2020, 159, 636–641. [Google Scholar] [CrossRef]
- Food and Drug Administration (FDA). Available online: https://www.fda.gov/drugs/drug-and-biologic-approval-and-ind-activity-reports/2021-first-generic-drug-approvals (accessed on 6 July 2023).
- Stary, G.; Bangert, C.; Tauber, M.; Strohal, R.; Kopp, T.; Stingl, G. Tumoricidal activity of TLR7/8-activated inflammatory dendritic cells. J. Exp. Med. 2007, 204, 1441–1451. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, B.O.; Possati-Resende, J.C.; Salcedo, M.P.; Schmeler, K.M.; Accorsi, G.S.; Fregnani, J.H.T.G.; Antoniazzi, M.; Pantano, N.P.; Santana, I.V.V.; Matsushita, G.M.; et al. Topical Imiquimod for the Treatment of High-Grade Squamous Intraepithelial Lesions of the Cervix: A Randomized Controlled Trial. Obstet. Gynecol. 2021, 137, 1043–1053. [Google Scholar] [CrossRef]
- Grimm, C.; Polterauer, S.; Natter, C.; Rahhal, J.; Hefler, L.; Tempfer, C.B.; Heinze, G.; Stary, G.; Reinthaller, A.; Speiser, P. Treatment of cervical intraepithelial neoplasia with topical imiquimod: A randomized controlled trial. Obstet. Gynecol. 2012, 120, 152–159. [Google Scholar] [CrossRef]
- Hendriks, N.; Koeneman, M.M.; Van De Sande, A.J.M.; Penders, C.G.J.; Piek, J.M.J.; Kooreman, L.F.S.; Van Kuijk, S.M.J.; Hoosemans, L.; Sep, S.J.S.; De Vos Van Steenwijk, P.J.; et al. Topical Imiquimod Treatment of High-grade Cervical Intraepithelial Neoplasia (TOPIC-3): A Nonrandomized Multicenter Study. J. Immunother. 2022, 45, 180–186. [Google Scholar] [CrossRef]
- Pachman, D.R.; Barton, D.L.; Clayton, A.C.; McGovern, R.M.; Jefferies, J.A.; Novotny, P.J.; Sloan, J.A.; Loprinzi, C.L.; Gostout, B.S. Randomized clinical trial of imiquimod: An adjunct to treating cervical dysplasia. Am. J. Obstet. Gynecol. 2012, 206, 42.e1–42.e7. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, Ed000142. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- National Cancer Institute (NIH). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 8 July 2023).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Joanna Briggs Institute (JBI). Critical Appraisal Checklist. 2017. Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Prevalence_Studies2017_0.pdf (accessed on 7 August 2023).
- GradePro. Available online: https://www.gradepro.org (accessed on 11 May 2023).
- Clopper, C.J.; Pearson, E.S. The Use of Confidence or Fiducial Limits Illustrated in the Case of the Binomial. Biometrika 1934, 26, 404–413. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. An Introduction to Meta-Analysis. In Introduction to Meta-Analysis; Wiley: Hoboken, NJ, USA, 2009; Volume 19. [Google Scholar]
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D. Doing Meta-Analysis with R: A Hands-On Guide; CRC Press: Boca Raton, FL, USA, 2021. [Google Scholar]
- Kim, J.H.; Kim, D.Y. Imiquimod as an alternative option for young women with high-grade cervical intraepithelial neoplasia. Eur. J. Gynaecol. Oncol. 2019, 40, 943–947. [Google Scholar]
- Cokan, A.; Pakiž, M.; Serdinšek, T.; Dovnik, A.; Kodrič, T.; Fokter, A.R.; Kavalar, R.; But, I. Comparison of conservative treatment of cervical intraepithelial lesions with imiquimod with standard excisional technique using lletz: A randomized controlled trial. J. Clin. Med. 2021, 10, 5777. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.T.; Qiu, J.T.; Wang, C.J.; Chang, S.D.; Tang, Y.H.; Wu, P.J.; Jung, S.M.; Huang, C.C.; Chou, H.H.; Jao, M.S.; et al. Topical imiquimod treatment for human papillomavirus infection in patients with and without cervical/vaginal intraepithelial neoplasia. Taiwan. J. Obstet. Gynecol. 2012, 51, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Polterauer, S.; Reich, O.; Widschwendter, A.; Hadjari, L.; Bogner, G.; Reinthaller, A.; Joura, E.; Trutnovsky, G.; Ciresa-Koenig, A.; Ganhoer-Schimboeck, J.; et al. Topical imiquimod compared with conization to treat cervical high-grade squamous intraepithelial lesions: Multicenter, randomized controlled trial. Gynecol. Oncol. 2022, 165, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.K.; Monk, B.J.; Brewer, C.; Keefe, K.A.; Osann, K.; McMeekin, S.; Rose, G.S.; Youssef, M.; Wilczynski, S.P.; Meyskens, F.L.; et al. HPV infection and number of lifetime sexual partners are strong predictors for ‘natural’ regression of CIN 2 and 3. Br. J. Cancer 2003, 89, 1062–1066. [Google Scholar] [CrossRef] [PubMed]
- Tainio, K.; Athanasiou, A.; Tikkinen, K.A.O.; Aaltonen, R.; Cárdenas, J.; Glazer-Livson, S.; Jakobsson, M.; Joronen, K.; Kiviharju, M.; Louvanto, K.; et al. Clinical course of untreated cervical intraepithelial neoplasia grade 2 under active surveillance: Systematic review and meta-analysis. BMJ 2018, 360, k499. [Google Scholar] [CrossRef] [PubMed]
- Kitchener, H.C.; Castle, P.E.; Cox, J.T. Chapter 7: Achievements and limitations of cervical cytology screening. Vaccine 2006, 24 (Suppl. S3), 63–70. [Google Scholar] [CrossRef] [PubMed]
- Terlou, A.; van Seters, M.; Ewing, P.C.; Aaronson, N.K.; Gundy, C.M.; Heijmans-Antonissen, C.; Quint, W.G.; Blok, L.J.; van Beurden, M.; Helmerhorst, T.J. Treatment of vulvar intraepithelial neoplasia with topical imiquimod: Seven years median follow-up of a randomized clinical trial. Gynecol. Oncol. 2011, 121, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Tranoulis, A.; Laios, A.; Mitsopoulos, V.; Lutchman-Singh, K.; Thomakos, N. Efficacy of 5% imiquimod for the treatment of Vaginal intraepithelial neoplasia-A systematic review of the literature and a meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 218, 129–136. [Google Scholar] [CrossRef]
- Committee Opinion No. 675 Summary: Management of Vulvar Intraepithelial Neoplasia. Obstet. Gynecol. 2016, 128, 937–938.
- O’Shea, A.S.; Stockdale, C.K. The impact of LEEP margin status on subsequent abnormal cervical cytology. Proc. Obstet. Gynecol. 2014, 4, 1–8. [Google Scholar] [CrossRef]
- Koeneman, M.M.; Essers, B.A.; Gerestein, C.G.; van de Sande, A.J.M.; Litjens, R.; Boskamp, D.; Goossens, M.F.J.; Beekhuizen, H.J.; Kruitwagen, R.; Kruse, A.J.; et al. Treatment of Cervical Intraepithelial Neoplasia: Patients Preferences for Surgery or Immunotherapy with Imiquimod. J. Immunother. 2017, 40, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Kyrgiou, M.; Athanasiou, A.; Kalliala, I.E.J.; Paraskevaidi, M.; Mitra, A.; Martin-Hirsch, P.P.; Arbyn, M.; Bennett, P.; Paraskevaidis, E. Obstetric outcomes after conservative treatment for cervical intraepithelial lesions and early invasive disease. Cochrane Database Syst. Rev. 2017, 11, Cd012847. [Google Scholar] [CrossRef] [PubMed]
- Abdulrahman, Z.; Hendriks, N.; Kruse, A.J.; Somarakis, A.; van de Sande, A.J.; van Beekhuizen, H.J.; Piek, J.M.; de Miranda, N.F.; Kooreman, L.F.; Slangen, B.F.; et al. Immune-based biomarker accurately predicts response to imiquimod immunotherapy in cervical high-grade squamous intraepithelial lesions. J. Immunother. Cancer 2022, 10, e005288. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.L.; da Silva Batista, Z.; Bastos, G.R.; Cunha, A.P.A.; Figueiredo, F.V.; de Castro, L.O.; Dos Anjos Pereira, L.; da Silva, M.; Vidal, F.C.B.; Barros, M.C.; et al. Role of HPV 16 variants among cervical carcinoma samples from Northeastern Brazil. BMC Women’s Health 2020, 20, 162. [Google Scholar] [CrossRef] [PubMed]
- Gravitt, P.E.; Winer, R.L. Natural History of HPV Infection across the Lifespan: Role of Viral Latency. Viruses 2017, 9, 267. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, R.D.; Snijders, P.J.; Heideman, D.A.; Meijer, C.J. Clinical implications of (epi)genetic changes in HPV-induced cervical precancerous lesions. Nat. Rev. Cancer 2014, 14, 395–405. [Google Scholar] [CrossRef]
- Rahangdale, L.; Lippmann, Q.K.; Garcia, K.; Budwit, D.; Smith, J.S.; van Le, L. Topical 5-fluorouracil for treatment of cervical intraepithelial neoplasia 2: A randomized controlled trial. Am. J. Obstet. Gynecol. 2014, 210, 314.e1–314.e8. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Years | Study Type | Region | Follow Up Time (Months) | Number of Patients in Intervention | Age (Mean) Intervention, SD | Number of Patients in Control | Age (Mean) Control, SD | CIN B | CIN2/CIN3 Ratio | HPV D Type | Dose of Imiquimod/Patient | Intervention of Control Group | Adverse Event Reporting | Dropout of Patients |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Grimm et al., 2012 [11] | RCT A | Austria | 5 | 30 | 29.2 ± 6.1 | 29 | 31.8 ± 7.8 | CIN 2–3 | 1.73 | HPV 16/18, other HR E HPV | 243.75 mg | observation | CTCAE F 3.0 | 6.70% |
| Hendriks et al., 2022 [12] | Non-randomized interventional | The Netherlands | 6 | 61 | 33.3 ± 9.1 | 62 | 35.2 ± 7 | CIN 2–3 | 0.69 | HPV 16/18, other HR HPV | 300 mg | conization | VAS G | 22.90% |
| Cokan et al., 2021 [28] | RCT | Slovenia | 6 | 52 | 28.3 ± 4.2 | 52 | 26 ± 4.6 | CIN 2–3 | 0.79 | NA | 600 mg | conization | CTCAE 5.0 | 17.30% |
| Lin et al., 2012 [29] | Retrospective cohort analysis | Taiwan | 33.4 | 72 | 51.75 B | 20 | 50 B | NA C | NA | persistent HR-HPV | 150 mg | observation | NA | NA |
| Fonseca et al., 2021 [10] | RCT | Brazil | 24 | 45 | 32 B | 45 | 36 B | CIN 2–3 | 0.4 | NA | 150 mg | observation | CTCAE 4.0 | 15.60% |
| Pachman et al., 2012 [13] | RCT | USA | 37.2 | 28 | 30 ± 8.9 | 28 | 29 ± 9.7 | CIN 1–2–3 | 1.42 | HR-HPV | 12.5 mg | conization, laser, cryotherapy | CTCH H 2.0 | 7.14% |
| Polterauer et al., 2022 [30] | RCT | Austria | 24 | 51 | 31.4 B | 42 | 30.1 B | CIN 2–3 | 0.28 | HPV 16/18, other HR HPV | 243.75 mg | conization | CTCAE 3.0 | 9.80% |
| Kim et al., 2019 [27] | retrospective cohort analysis | Republic of Korea | 13.4 | 55 | 30 B | NA | NA | CIN 2–3 | 0.74 | HPV 16/18, other HR HPV | 100 mg | NA | NA | 1.80% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamar, B.; Teutsch, B.; Hoffmann, E.; Hegyi, P.; Harnos, A.; Nyirády, P.; Hunka, Z.; Ács, N.; Bánhidy, F.; Melczer, Z. Imiquimod Is Effective in Reducing Cervical Intraepithelial Neoplasia: A Systematic Review and Meta-Analysis. Cancers 2024, 16, 1610. https://doi.org/10.3390/cancers16081610
Hamar B, Teutsch B, Hoffmann E, Hegyi P, Harnos A, Nyirády P, Hunka Z, Ács N, Bánhidy F, Melczer Z. Imiquimod Is Effective in Reducing Cervical Intraepithelial Neoplasia: A Systematic Review and Meta-Analysis. Cancers. 2024; 16(8):1610. https://doi.org/10.3390/cancers16081610
Chicago/Turabian StyleHamar, Balázs, Brigitta Teutsch, Eszter Hoffmann, Péter Hegyi, Andrea Harnos, Péter Nyirády, Zsombor Hunka, Nándor Ács, Ferenc Bánhidy, and Zsolt Melczer. 2024. "Imiquimod Is Effective in Reducing Cervical Intraepithelial Neoplasia: A Systematic Review and Meta-Analysis" Cancers 16, no. 8: 1610. https://doi.org/10.3390/cancers16081610