
The Use of Glucagon-like Peptide-1 Receptor Agonists in Patients with Type 2 Diabetes Mellitus Does Not Increase the Risk of Pancreatic Cancer: A U.S.-Based Cohort Study


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Outcomes
4. Discussion
4.1. Panceatic Cancer Incidence and Prevalanece
4.2. Risk Factors
4.2.1. Tobacco Use
4.2.2. Alcohol Use
4.2.3. Chronic Pancreatitis
4.2.4. Obesity
4.2.5. Diabetes Mellitus
4.2.6. Hereditary Factors
4.2.7. Pancreatic Cysts
4.3. GLP-1 RA Mechanism of Action
4.4. GLP-1 RA Safety Profile; Benefits and Side Effects
4.5. Association of GLP-1 RAs with Different Cancers
4.6. Association of GLP-1 RA with Pancreatic Cancer and Theories
4.7. Our Study and Current Evidence
4.8. Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FDA. Drug Safety Communication: FDA Investigating Reports of Possible Increased Risk of Pancreatitis and Pre-Cancerous Findings of the Pancreas from Incretin Mimetic Drugs for Type 2 Diabetes. FDA. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-investigating-reports-possible-increased-risk-pancreatitis-and-pre (accessed on 13 March 2024).
- Elashoff, M.; Matveyenko, A.V.; Gier, B.; Elashoff, R.; Butler, P.C. Pancreatitis, pancreatic, and thyroid cancer with glucagon-like peptide-1-based therapies. Gastroenterology 2011, 141, 150–156. Available online: https://pubmed.ncbi.nlm.nih.gov/21334333/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Ayoub, M.; Tomanguillo, J.; Faris, C.; Anwar, N.; Chela, H.; Daglilar, E. SARS-CoV-2 Infection Is an Independent Risk Factor for Decompensation in Cirrhosis Patients. Diseases 2024, 12, 46. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Key Statistics for Pancreatic Cancer. American Cancer Society. Available online: https://www.cancer.org/cancer/types/pancreatic-cancer/about/key-statistics.html (accessed on 12 March 2024).
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. Available online: https://pubmed.ncbi.nlm.nih.gov/24840647/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. Available online: https://pubmed.ncbi.nlm.nih.gov/33433946/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. Available online: https://pubmed.ncbi.nlm.nih.gov/30834048/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- US Preventive Services Task Force; Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Curry, S.J.; Doubeni, C.A.; Epling, J.W.; et al. Screening for Pancreatic Cancer: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA 2019, 322, 438–444. [Google Scholar] [PubMed]
- Capasso, M.; Franceschi, M.; Rodriguez-Castro, K.I.; Crafa, P.; Cambiè, G.; Miraglia, C.; Barchi, A.; Nouvenne, A.; Leandro, G.; Meschi, T.; et al. Epidemiology and risk factors of pancreatic cancer. Acta Biomed. Atenei Parm. 2018, 89 (Suppl. S9), 141. [Google Scholar] [PubMed Central]
- Park, W.; Chawla, A.; O’Reilly, E.M. Pancreatic Cancer: A Review. JAMA 2021, 326, 851. [Google Scholar] [CrossRef] [PubMed Central]
- Shindo, K.; Yu, J.; Suenaga, M.; Fesharakizadeh, S.; Cho, C.; Macgregor-Das, A.; Siddiqui, A.; Witmer, P.D.; Tamura, K.; Song, T.J.; et al. Deleterious Germline Mutations in Patients with Apparently Sporadic Pancreatic Adenocarcinoma. J. Clin. Oncol. 2017, 35, 3382–3390. Available online: https://pubmed.ncbi.nlm.nih.gov/28767289/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Golan, T.; Kindler, H.L.; Park, J.O.; Reni, M.; Macarulla, T.; Hammel, P.; van Cutsem, E.; Arnold, D.; Hochhauser, D.; McGuinness, D.; et al. Geographic and Ethnic Heterogeneity of Germline BRCA1 or BRCA2 Mutation Prevalence among Patients with Metastatic Pancreatic Cancer Screened for Entry into the POLO Trial. J. Clin. Oncol. 2020, 38, 1442–1454. Available online: https://pubmed.ncbi.nlm.nih.gov/32073954/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Iodice, S.; Gandini, S.; Maisonneuve, P.; Lowenfels, A.B. Tobacco and the risk of pancreatic cancer: A review and meta-analysis. Langenbeck’s Arch. Surg. 2008, 393, 535–545. Available online: https://pubmed.ncbi.nlm.nih.gov/18193270/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Tramacere, I.; Scotti, L.; Jenab, M.; Bagnardi, V.; Bellocco, R.; Rota, M.; Corrao, G.; Bravi, F.; Boffetta, P.; La Vecchia, C. Alcohol drinking and pancreatic cancer risk: A meta-analysis of the dose-risk relation. Int. J. Cancer 2010, 126, 1474–1486. Available online: https://pubmed.ncbi.nlm.nih.gov/19816941/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Gukovsky, I.; Li, N.; Todoric, J.; Gukovskaya, A.; Karin, M. Inflammation, autophagy, and obesity: Common features in the pathogenesis of pancreatitis and pancreatic cancer. Gastroenterology 2013, 144, 1199–1209.e4. Available online: https://pubmed.ncbi.nlm.nih.gov/23622129/ (accessed on 12 March 2024). [CrossRef]
- Lowenfels, A.B.; Maisonneuve, P.; Cavallini, G.; Ammann, R.W.; Lankisch, P.G.; Andersen, J.R.; Dimagno, E.P.; Andren-Sandberg, A.; Domellof, L. Pancreatitis and the risk of pancreatic cancer. Int. Pancreat. Study Group. N. Engl. J. Med. 1993, 328, 1433–1437. Available online: https://pubmed.ncbi.nlm.nih.gov/8479461/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Raimondi, S.; Lowenfels, A.B.; Morselli-Labate, A.M.; Maisonneuve, P.; Pezzilli, R. Pancreatic cancer in chronic pancreatitis; aetiology, incidence, and early detection. Best Pract. Res. Clin. Gastroenterol. 2010, 24, 349–358. Available online: https://pubmed.ncbi.nlm.nih.gov/20510834/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Larsson, S.C.; Orsini, N.; Wolk, A. Body mass index and pancreatic cancer risk: A meta-analysis of prospective studies. Int. J. Cancer 2007, 120, 1993–1998. Available online: https://pubmed.ncbi.nlm.nih.gov/17266034/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Stocks, T.; Rapp, K.; Bjørge, T.; Manjer, J.; Ulmer, H.; Selmer, R.; Lukanova, A.; Johansen, D.; Concin, H.; Tretli, S.; et al. Blood glucose and risk of incident and fatal cancer in the metabolic syndrome and cancer project (me-can): Analysis of six prospective cohorts. PLoS Med. 2009, 6, e1000201. Available online: https://pubmed.ncbi.nlm.nih.gov/20027213/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Stolzenberg-Solomon, R.Z.; Newton, C.C.; Silverman, D.T.; Pollak, M.; Nogueira, L.M.; Weinstein, S.J.; Albanes, D.; Männistö, S.; Jacobs, E.J. Circulating Leptin and Risk of Pancreatic Cancer: A Pooled Analysis From 3 Cohorts. Am. J. Epidemiol. 2015, 182, 187–197. Available online: https://pubmed.ncbi.nlm.nih.gov/26085045/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Larsson, S.C.; Wolk, A. Red and processed meat consumption and risk of pancreatic cancer: Meta-analysis of prospective studies. Br. J. Cancer 2012, 106, 603–607. Available online: https://pubmed.ncbi.nlm.nih.gov/22240790/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Gullo, L.; Pezzilli, R.; Morselli-Labate, A.M. Diabetes and the risk of pancreatic cancer. N. Engl. J. Med. 1994, 331, 81–84. Available online: https://pubmed.ncbi.nlm.nih.gov/8208269/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Huxley, R.; Ansary-Moghaddam, A.; Berrington De González, A.; Barzi, F.; Woodward, M. Type-II diabetes and pancreatic cancer: A meta-analysis of 36 studies. Br. J. Cancer 2005, 92, 2076–2083. Available online: https://pubmed.ncbi.nlm.nih.gov/15886696/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Yang, J.; Waldron, R.T.; Su, H.Y.; Moro, A.; Chang, H.H.; Eibl, G.; Ferreri, K.; Kandeel, F.R.; Lugea, A.; Li, L.; et al. Insulin promotes proliferation and fibrosing responses in activated pancreatic stellate cells. Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 311, G675–G687. Available online: https://pubmed.ncbi.nlm.nih.gov/27609771/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Apte, M.V.; Wilson, J.S.; Lugea, A.; Pandol, S.J. A starring role for stellate cells in the pancreatic cancer microenvironment. Gastroenterology 2013, 144, 1210–1219. Available online: https://pubmed.ncbi.nlm.nih.gov/23622130/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Moran, A.; O’Hara, C.; Khan, S.; Shack, L.; Woodward, E.; Maher, E.R.; Lalloo, F.; Evans, D.G.R. Risk of cancer other than breast or ovarian in individuals with BRCA1 and BRCA2 mutations. Fam. Cancer 2012, 11, 235–242. Available online: https://pubmed.ncbi.nlm.nih.gov/22187320/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- De Snoo, F.A.; Bishop, D.T.; Bergman, W.; Van Leeuwen, I.; Van Der Drift, C.; Van Nieuwpoort, F.A.; Out-Luiting, C.J.; Vasen, H.F.; Ter Huurne, J.A.C.; Frants, R.R.; et al. Increased risk of cancer other than melanoma in CDKN2A founder mutation (p16-Leiden)-positive melanoma families. Clin. Cancer Res. 2008, 14, 7151–7157. Available online: https://pubmed.ncbi.nlm.nih.gov/18981015/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Biankin, A.V.; Waddell, N.; Kassahn, K.S.; Gingras, M.C.; Muthuswamy, L.B.; Johns, A.L.; Miller, D.K.; Wilson, P.J.; Patch, A.M.; Wu, J.; et al. Pancreatic cancer genomes reveal aberrations in axon guidance pathway genes. Nature 2012, 491, 399–405. Available online: https://pubmed.ncbi.nlm.nih.gov/23103869/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Bailey, P.; Chang, D.K.; Nones, K.; Johns, A.L.; Patch, A.M.; Gingras, M.C.; Miller, D.K.; Christ, A.N.; Bruxner, T.J.C.; Quinn, M.C.; et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature 2016, 531, 47–52. Available online: https://pubmed.ncbi.nlm.nih.gov/26909576/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Witkiewicz, A.K.; McMillan, E.A.; Balaji, U.; Baek, G.H.; Lin, W.C.; Mansour, J.; Mollaee, M.; Wagner, K.U.; Koduru, P.; Yopp, A.; et al. Whole-exome sequencing of pancreatic cancer defines genetic diversity and therapeutic targets. Nat. Commun. 2015, 6, 6744. Available online: https://pubmed.ncbi.nlm.nih.gov/25855536/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Sanchez-Vega, F.; Mina, M.; Armenia, J.; Chatila, W.K.; Luna, A.; La, K.C.; Dimitriadoy, S.; Liu, D.L.; Kantheti, H.S.; Saghafinia, S.; et al. Oncogenic Signaling Pathways in The Cancer Genome Atlas. Cell 2018, 173, 321–337.e10. Available online: https://pubmed.ncbi.nlm.nih.gov/29625050/ (accessed on 12 March 2024). [CrossRef]
- Luo, J. KRAS mutation in Pancreatic Cancer. Semin. Oncol. 2021, 48, 10. [Google Scholar] [CrossRef] [PubMed Central]
- Thakker, R.V. Multiple endocrine neoplasia type 1 (MEN1) and type 4 (MEN4). Mol. Cell Endocrinol. 2014, 386, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Pieterman, C.R.C.; Schreinemakers, J.M.J.; Koppeschaar, H.P.F.; Vriens, M.R.; Rinkes, I.H.M.B.; Zonnenberg, B.A.; Van Der Luijt, R.B.; Valk, G.D. Multiple endocrine neoplasia type 1 (MEN1): Its manifestations and effect of genetic screening on clinical outcome. Clin. Endocrinol. 2009, 70, 575–581. Available online: https://pubmed.ncbi.nlm.nih.gov/18616711/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Sadowski, S.M.; Triponez, F. Management of pancreatic neuroendocrine tumors in patients with MEN 1. Gland 2015, 4, 63. [Google Scholar] [PubMed Central]
- Thakker, R.V.; Newey, P.J.; Walls, G.V.; Bilezikian, J.; Dralle, H.; Ebeling, P.R.; Melmed, S.; Sakurai, A.; Tonelli, F.; Brandi, M.L. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1). J. Clin. Endocrinol. Metab. 2012, 97, 2990–3011. Available online: https://pubmed.ncbi.nlm.nih.gov/22723327/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Goudet, P.; Murat, A.; Binquet, C.; Cardot-Bauters, C.; Costa, A.; Ruszniewski, P.; Niccoli, P.; Ménégaux, F.; Chabrier, G.; Borson-Chazot, F.; et al. Risk factors and causes of death in MEN1 disease. A GTE (Groupe d’Etude des Tumeurs Endocrines) cohort study among 758 patients. World J. Surg. 2010, 34, 249–255. Available online: https://pubmed.ncbi.nlm.nih.gov/19949948/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Triponez, F.; Dosseh, D.; Goudet, P.; Cougard, P.; Bauters, C.; Murat, A.; Cadiot, G.; Niccoli-Sire, P.; Chayvialle, J.A.; Calender, A.; et al. Epidemiology data on 108 MEN 1 patients from the GTE with isolated nonfunctioning tumors of the pancreas. Ann. Surg. 2006, 243, 265–272. Available online: https://pubmed.ncbi.nlm.nih.gov/16432361/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Kastrinos, F.; Mukherjee, B.; Tayob, N.; Wang, F.; Sparr, J.; Raymond, V.M.; Bandipalliam, P.; Stoffel, E.M.; Gruber, S.B.; Syngal, S. Risk of pancreatic cancer in families with Lynch syndrome. JAMA 2009, 302, 1790–1795. Available online: https://pubmed.ncbi.nlm.nih.gov/19861671/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Hanlon, L.; Avila, J.L.; Demarest, R.M.; Troutman, S.; Allen, M.; Ratti, F.; Rustgi, A.K.; Stanger, B.Z.; Radtke, F.; Adsay, V.; et al. Notch1 functions as a tumor suppressor in a model of K-ras-induced pancreatic ductal adenocarcinoma. Cancer Res. 2010, 70, 4280–4286. Available online: https://pubmed.ncbi.nlm.nih.gov/20484026/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Thomas, M.M.; Zhang, Y.; Mathew, E.; Kane, K.T.; Maillard, I.; Di Magliano, M.P. Epithelial Notch signaling is a limiting step for pancreatic carcinogenesis. BMC Cancer 2014, 14, 862. Available online: https://pubmed.ncbi.nlm.nih.gov/25416148/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Stanger, B.Z.; Stiles, B.; Lauwers, G.Y.; Bardeesy, N.; Mendoza, M.; Wang, Y.; Greenwood, A.; Cheng, K.H.; McLaughlin, M.; Brown, D.; et al. Pten constrains centroacinar cell expansion and malignant transformation in the pancreas. Cancer Cell 2005, 8, 185–195. Available online: https://pubmed.ncbi.nlm.nih.gov/16169464/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Di Magliano, M.P.; Sekine, S.; Ermilov, A.; Ferris, J.; Dlugosz, A.A.; Hebrok, M. Hedgehog/Ras interactions regulate early stages of pancreatic cancer. Genes. Dev. 2006, 20, 3161–3173. Available online: https://pubmed.ncbi.nlm.nih.gov/17114586/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Miyamoto, Y.; Maitra, A.; Ghosh, B.; Zechner, U.; Argani, P.; Iacobuzio-Donahue, C.A.; Sriuranpong, V.; Iso, T.; Meszoely, I.M.; Wolfe, M.S.; et al. Notch mediates TGFα-induced changes in epithelial differentiation during pancreatic tumorigenesis. Cancer Cell 2003, 3, 565–576. Available online: https://pubmed.ncbi.nlm.nih.gov/12842085/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Hingorani, S.R.; Petricoin, E.F.; Maitra, A.; Rajapakse, V.; King, C.; Jacobetz, M.A.; Ross, S.; Conrads, T.P.; Veenstra, T.D.; Hitt, B.A.; et al. Preinvasive and invasive ductal pancreatic cancer and its early detection in the mouse. Cancer Cell 2003, 4, 437–450. Available online: https://pubmed.ncbi.nlm.nih.gov/14706336/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Tremblay, I.; Paré, E.; Arsenault, D.; Douziech, M.; Boucher, M.J. The MEK/ERK pathway promotes NOTCH signalling in pancreatic cancer cells. PLoS ONE 2013, 8, e85502. Available online: https://pubmed.ncbi.nlm.nih.gov/24392017/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Ma, Y.C.; Shi, C.; Zhang, Y.N.; Wang, L.G.; Liu, H.; Jia, H.T.; Zhang, Y.X.; Sarkar, F.H.; Wang, Z.S. The tyrosine kinase c-Src directly mediates growth factor-induced Notch-1 and Furin interaction and Notch-1 activation in pancreatic cancer cells. PLoS ONE 2012, 7. Available online: https://pubmed.ncbi.nlm.nih.gov/22479394/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Gao, J.; Long, B.; Wang, Z. Role of Notch signaling pathway in pancreatic cancer. Am. J. Cancer Res. 2017, 7, 173. [Google Scholar] [PubMed] [PubMed Central]
- Jones, S.; Hruban, R.H.; Kamiyama, M.; Borges, M.; Zhang, X.; Parsons, D.W.; Lin, J.C.H.; Palmisano, E.; Brune, K.; Jaffee, E.M.; et al. Exomic sequencing identifies PALB2 as a pancreatic cancer susceptibility gene. Science 2009, 324, 217. Available online: https://pubmed.ncbi.nlm.nih.gov/19264984/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Principe, D.R. Precision Medicine for BRCA/PALB2-Mutated Pancreatic Cancer and Emerging Strategies to Improve Therapeutic Responses to PARP Inhibition. Cancers 2022, 14, 897. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Larusch, J.; Whitcomb, D.C. Genetics of pancreatitis. Curr. Opin. Gastroenterol. 2011, 27, 467–474. Available online: https://pubmed.ncbi.nlm.nih.gov/21844754/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Shi, C.; Hruban, R.H.; Klein, A.P. Familial pancreatic cancer. Arch. Pathol. Lab. Med. 2009, 133, 365–374. Available online: https://pubmed.ncbi.nlm.nih.gov/19260742/ (accessed on 12 March 2024). [CrossRef] [PubMed]
- Singh, R.R.; Gopakumar, H.; Sharma, N.R. Diagnosis and Management of Pancreatic Cysts: A Comprehensive Review of the Literature. Diagnostics 2023, 13, 550. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Munigala, S.; Gelrud, A.; Agarwal, B. Risk of pancreatic cancer in patients with pancreatic cyst. Gastrointest. Endosc. 2016, 84, 81–86. Available online: http://www.giejournal.org/article/S0016510715030461/fulltext (accessed on 13 March 2024). [CrossRef] [PubMed]
- Lee, Y.S.; Jun, H.S. Anti-diabetic actions of glucagon-like peptide-1 on pancreatic beta-cells. Metabolism 2014, 63, 9–19. Available online: https://pubmed.ncbi.nlm.nih.gov/24140094/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Pyke, C.; Heller, R.S.; Kirk, R.K.; Ørskov, C.; Reedtz-Runge, S.; Kaastrup, P.; Hvelplund, A.; Bardram, L.; Calatayud, D.; Knudsen, L.B. GLP-1 receptor localization in monkey and human tissue: Novel distribution revealed with extensively validated monoclonal antibody. Endocrinology 2014, 155, 1280–1290. Available online: https://pubmed.ncbi.nlm.nih.gov/24467746/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Nauck, M.A.; Niedereichholz, U.; Ettler, R.; Holst, J.J.; Ørskov, C.; Ritzel, R.; Schmiegel, W.H. Glucagon-like peptide 1 inhibition of gastric emptying outweighs its insulinotropic effects in healthy humans. Am. J. Physiol. 1997, 273, E981–E988. Available online: https://pubmed.ncbi.nlm.nih.gov/9374685/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Koliaki, C.; Doupis, J. Incretin-based therapy: A powerful and promising weapon in the treatment of type 2 diabetes mellitus. Diabetes Ther. 2011, 2, 101–121. Available online: https://pubmed.ncbi.nlm.nih.gov/22127804/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Nauck, M.A.; Kleine, N.; Ørskov, C.; Holst, J.J.; Willms, B.; Creutzfeldt, W. Normalization of fasting hyperglycaemia by exogenous glucagon-like peptide 1 (7–36 amide) in type 2 (non-insulin-dependent) diabetic patients. Diabetologia 1993, 36, 741–744. Available online: https://pubmed.ncbi.nlm.nih.gov/8405741/ (accessed on 13 March 2024). [CrossRef]
- Vilsbøll, T.; Krarup, T.; Deacon, C.F.; Madsbad, S.; Holst, J.J. Reduced postprandial concentrations of intact biologically active glucagon-like peptide 1 in type 2 diabetic patients. Diabetes 2001, 50, 609–613. [Google Scholar] [CrossRef]
- Filippatos, T.D.; Panagiotopoulou, T.V.; Elisaf, M.S. Adverse Effects of GLP-1 Receptor Agonists. Rev. Diabet. Stud. 2014, 11, 202. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ratner, R.E.; Maggs, D.; Nielsen, L.L.; Stonehouse, A.H.; Poon, T.; Zhang, B.; Bicsak, T.A.; Brodows, R.G.; Kim, D.D. Long-term effects of exenatide therapy over 82 weeks on glycaemic control and weight in over-weight metformin-treated patients with type 2 diabetes mellitus. Diabetes Obes. Metab. 2006, 8, 419–428. Available online: https://pubmed.ncbi.nlm.nih.gov/16776749/ (accessed on 13 March 2024). [CrossRef]
- Ratner, R.; Han, J.; Nicewarner, D.; Yushmanova, I.; Hoogwerf, B.J.; Shen, L. Cardiovascular safety of exenatide BID: An integrated analysis from controlled clinical trials in participants with type 2 diabetes. Cardiovasc. Diabetol. 2011, 10, 22. Available online: https://pubmed.ncbi.nlm.nih.gov/21410975/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Schmidt, L.J.; Habacher, W.; Augustin, T.; Krahulec, E.; Semlitsch, T. A systematic review and meta-analysis of the efficacy of lixisenatide in the treatment of patients with type 2 diabetes. Diabetes Obes. Metab. 2014, 16, 769–779. Available online: https://pubmed.ncbi.nlm.nih.gov/24476092/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Robinson, L.E.; Holt, T.A.; Rees, K.; Randeva, H.S.; O’Hare, J.P. Effects of exenatide and liraglutide on heart rate, blood pressure and body weight: Systematic review and meta-analysis. BMJ Open 2013, 3, e001986. Available online: https://pubmed.ncbi.nlm.nih.gov/23355666/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Buse, J.B.; Garber, A.; Rosenstock, J.; Schmidt, W.E.; Brett, J.H.; Videbæk, N.; Holst, J.; Nauck, M. Liraglutide treatment is associated with a low frequency and magnitude of antibody formation with no apparent impact on glycemic response or increased frequency of adverse events: Results from the Liraglutide Effect and Action in Diabetes (LEAD) trials. J. Clin. Endocrinol. Metab. 2011, 96, 1695–1702. Available online: https://pubmed.ncbi.nlm.nih.gov/21450987/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Madsbad, S.; Kielgast, U.; Asmar, M.; Deacon, C.F.; Torekov, S.S.; Holst, J.J. An overview of once-weekly glucagon-like peptide-1 receptor agonists—Available efficacy and safety data and perspectives for the future. Diabetes Obes. Metab. 2011, 13, 394–407. Available online: https://pubmed.ncbi.nlm.nih.gov/21208359/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- De Heer, J.; Holst, J.J. Sulfonylurea compounds uncouple the glucose dependence of the insulinotropic effect of glucagon-like peptide 1. Diabetes 2007, 56, 438–443. Available online: https://pubmed.ncbi.nlm.nih.gov/17259389/ (accessed on 13 March 2024). [CrossRef]
- Filippatos, T.D.; Elisaf, M.S. Effects of glucagon-like peptide-1 receptor agonists on renal function. World J. Diabetes 2013, 4, 190. Available online: https://pubmed.ncbi.nlm.nih.gov/24147203/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Michos, E.D.; Bakris, G.L.; Rodbard, H.W.; Tuttle, K.R. Glucagon-like peptide-1 receptor agonists in diabetic kidney disease: A review of their kidney and heart protection. Am. J. Prev. Cardiol. 2023, 14, 100502. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sattar, N.; Lee, M.M.Y.; Kristensen, S.L.; Branch, K.R.H.; Del Prato, S.; Khurmi, N.S.; Lam, C.S.P.; Lopes, R.D.; McMurray, J.J.V.; Pratley, R.E.; et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021, 9, 653–662. Available online: https://pubmed.ncbi.nlm.nih.gov/34425083/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Iorga, R.A.; Bacalbasa, N.; Carsote, M.; Bratu, O.G.; Stanescu, A.M.A.; Bungau, S.; Pantis, C.; Diaconu, C.C. Metabolic and cardiovascular benefits of GLP-1 agonists, besides the hypoglycemic effect (Review). Exp. Ther. Med. 2020, 20, 2396. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marx, N.; Husain, M.; Lehrke, M.; Verma, S.; Sattar, N. GLP-1 Receptor Agonists for the Reduction of Atherosclerotic Cardiovascular Risk in Patients with Type 2 Diabetes. Circulation 2022, 146, 1882–1894. Available online: https://www.ahajournals.org/doi/abs/10.1161/CIRCULATIONAHA.122.059595 (accessed on 13 March 2024). [CrossRef] [PubMed]
- Das, S.R.; Everett, B.M.; Birtcher, K.K.; Brown, J.M.; Januzzi, J.L.; Kalyani, R.R.; Kosiborod, M.; Magwire, M.; Morris, P.B.; Neumiller, J.J.; et al. 2020 Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients with Type 2 Diabetes: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2020, 76, 1117–1145. Available online: https://pubmed.ncbi.nlm.nih.gov/32771263/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. S1), S144–S174. Available online: https://pubmed.ncbi.nlm.nih.gov/34964815/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Knudsen, L.B.; Madsen, L.W.; Andersen, S.; Almholt, K.; De Boer, A.S.; Drucker, D.J.; Gotfredsen, C.; Egerod, F.L.; Hegelund, A.C.; Jacobsen, H.; et al. Glucagon-like Peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010, 151, 1473–1486. Available online: https://pubmed.ncbi.nlm.nih.gov/20203154/ (accessed on 20 February 2024). [CrossRef] [PubMed]
- Lisco, G.; De Tullio, A.; Disoteo, O.; Piazzolla, G.; Guastamacchia, E.; Sabbà, C.; De Geronimo, V.; Papini, E.; Triggiani, V. Glucagon-like peptide 1 receptor agonists and thyroid cancer: Is it the time to be concerned? Endocr. Connect 2023, 12. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bezin, J.; Gouverneur, A.; Penichon, M.; Mathieu, C.; Garrel, R.; Hillaire-Buys, D.; Pariente, A.; Faillie, J.L. GLP-1 Receptor Agonists and the Risk of Thyroid Cancer. Diabetes Care 2023, 46, 384–390. Available online: https://pubmed.ncbi.nlm.nih.gov/36356111/ (accessed on 24 March 2024). [CrossRef] [PubMed]
- Wang, L.; Wang, W.; Kaelber, D.C.; Xu, R.; Berger, N.A. GLP-1 Receptor Agonists and Colorectal Cancer Risk in Drug-Naive Patients with Type 2 Diabetes, with and without Overweight/Obesity. JAMA Oncol. 2024, 10, 256. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Skriver, C.; Friis, S.; Knudsen, L.B.; Catarig, A.M.; Clark, A.J.; Dehlendorff, C.; Mørch, L.S. Potential preventive properties of GLP-1 receptor agonists against prostate cancer: A nationwide cohort study. Diabetologia 2023, 66, 2007–2016. Available online: https://link.springer.com/article/10.1007/s00125-023-05972-x (accessed on 24 March 2024). [CrossRef] [PubMed]
- Arvanitakis, K.; Koufakis, T.; Kotsa, K.; Germanidis, G. How Far beyond Diabetes Can the Benefits of Glucagon-like Peptide-1 Receptor Agonists Go? A Review of the Evidence on Their Effects on Hepatocellular Carcinoma. Cancers 2022, 14, 4651. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Singh, S.; Chang, H.Y.; Richards, T.M.; Weiner, J.P.; Clark, J.M.; Segal, J.B. Glucagonlike peptide 1-based therapies and risk of hospitalization for acute pancreatitis in type 2 diabetes mellitus: A population-based matched case-control study. JAMA Intern. Med. 2013, 173, 534–539. Available online: https://pubmed.ncbi.nlm.nih.gov/23440284/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- FDA Approves First Oral GLP-1 Treatment for TYPE 2 Diabetes. FDA. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-oral-glp-1-treatment-type-2-diabetes (accessed on 19 April 2024).
- FDA. Approves First Treatment to Reduce Risk of Serious Heart Problems Specifically in Adults with Obesity or Overweight. FDA. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-reduce-risk-serious-heart-problems-specifically-adults-obesity-or (accessed on 19 April 2024).
- Suryadevara, V.; Roy, A.; Sahoo, J.; Kamalanathan, S.; Naik, D.; Mohan, P.; Kalayarasan, R. Incretin based therapy and pancreatic cancer: Realising the reality. World J. Gastroenterol. 2022, 28, 2881. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Perfetti, R.; Zhou, J.I.E.; Doyle, M.E.; Egan, J.M. Glucagon-like peptide-1 induces cell proliferation and pancreatic-duodenum homeobox-1 expression and increases endocrine cell mass in the pancreas of old, glucose-intolerant rats. Endocrinology 2000, 141, 4600–4605. Available online: https://pubmed.ncbi.nlm.nih.gov/11108273/ (accessed on 13 March 2024). [CrossRef] [PubMed]
- Dankner, R.; Murad, H.; Agay, N.; Olmer, L.; Freedman, L.S. Glucagon-Like Peptide-1 Receptor Agonists and Pancreatic Cancer Risk in Patients with Type 2 Diabetes. JAMA Netw. Open 2024, 7, e2350408. Available online: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2813598 (accessed on 13 March 2024). [CrossRef]
- Nreu, B.; Dicembrini, I.; Tinti, F.; Mannucci, E.; Monami, M. Pancreatitis and pancreatic cancer in patients with type 2 diabetes treated with glucagon-like peptide-1 receptor agonists: An updated meta-analysis of randomized controlled trials. Minerva Endocrinol. 2023, 48, 206–213. Available online: https://pubmed.ncbi.nlm.nih.gov/32720500/ (accessed on 13 March 2024). [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Before PSM | After PSM | |||||
|---|---|---|---|---|---|---|
| Characteristic | GLP-1 RA | No GLP-1 RA | p-Value | GLP-1 RA | No GLP-1 RA | p-Value |
| Demographics | ||||||
| Age | 54.4 ± 12.8 | 60.9 ± 15.3 | <0.001 | 54.4 ± 12.8 | 54.4 ± 12.9 | 0.46 |
| White | 61.7% | 57.8% | <0.001 | 61.7% | 61.7% | 0.44 |
| Black or African American | 17.9% | 16.5% | <0.001 | 17.9% | 18% | 0.28 |
| Asian | 3% | 4.4% | <0.001 | 3% | 3.3% | 0.41 |
| Unknown race | 12.3% | 16% | <0.001 | 12.3% | 12.3% | 0.88 |
| Female | 52.6% | 47.3% | <0.001 | 52.6% | 52.7% | 0.75 |
| Diagnosis | ||||||
| Tobacco use | 2.1% | 1.9% | <0.001 | 2.1% | 2% | 0.12 |
| Alcohol use | 0.2% | 0.5% | <0.001 | 0.2% | 0.2% | 0.09 |
| Acute pancreatitis | 0.5% | 0.9% | <0.001 | 0.5% | 0.5% | 0.06 |
| Chronic pancreatitis | 0.1% | 0.4% | <0.001 | 0.1 | 0.1 | 0.08 |
| Medication | ||||||
| Metformin | 39.5% | 19.8% | <0.001 | 39.5% | 39.5% | 0.85 |
| Insulin | 24.1% | 20.3% | <0.001 | 24.1% | 24% | 0.39 |
| DPP-4 inhibitors | 7% | 3.1% | <0.001 | 7% | 6.9% | 0.32 |
| Laboratory Results | ||||||
| Hemoglobin A1c | 7.9 ± 2.2 | 7.3 ± 2.1 | <0.001 | 7.9 ± 2.2 | 7.5 ± 2.2 | 0.062 |
| Body weight | 228.5 ± 59.6 | 200 ± 55.4 | <0.001 | 228.1 ± 59.6 | 210 ± 58.2 | 0.078 |
|
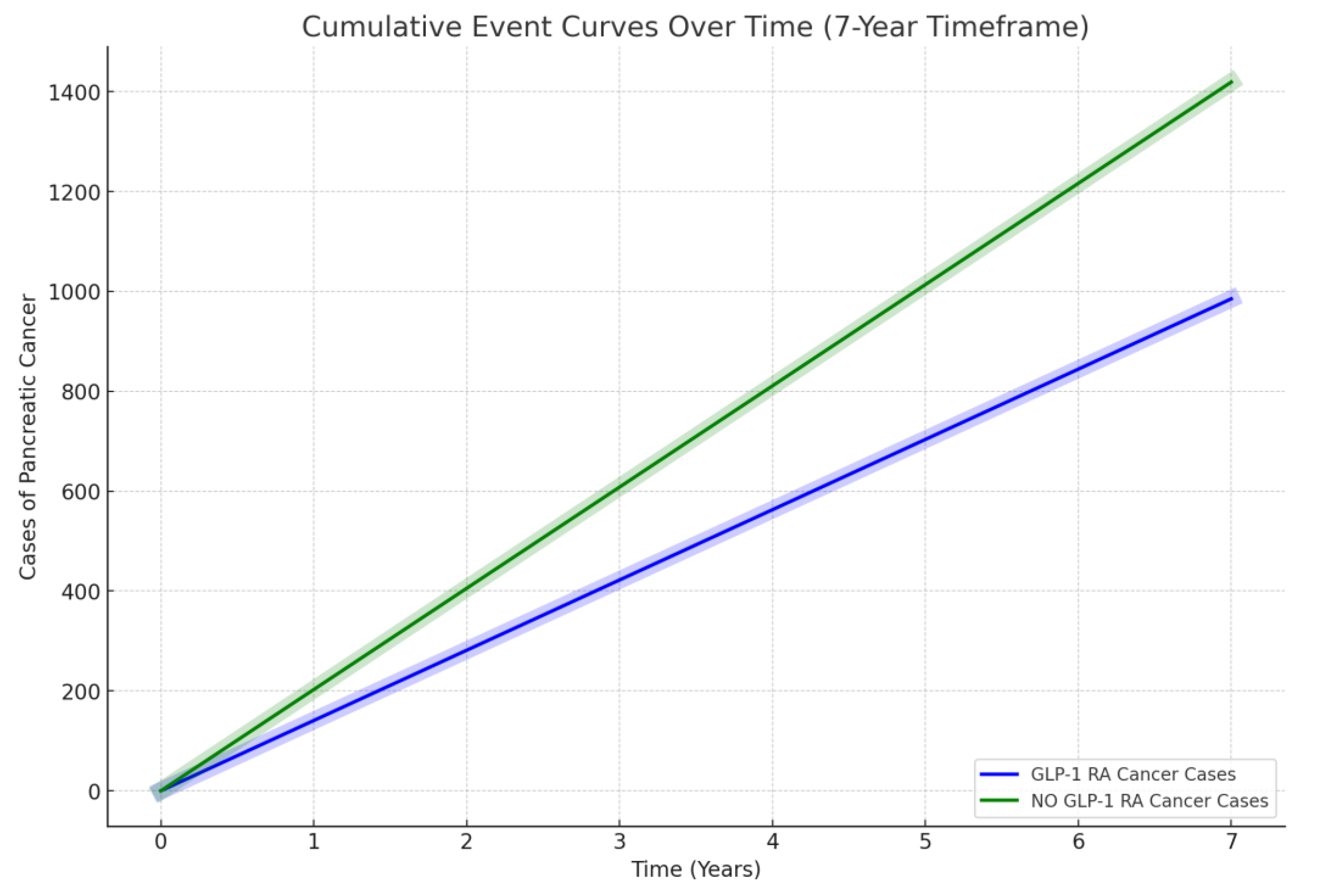
GLP-1 RA (n = 720,678) |
NO GLP-1 RA (n = 720,678) | p -Value | |||
|---|---|---|---|---|---|
| Outcome Pancreatic cancer | 0.14% (n = 985) | 0.2% (n = 1419) | <0.0001 | ||
| Log-rank test | X2 | df | p | ||
| 250.681 | 1 | 0.000 | |||
| Hazard ratio and proportionality | HR | 95% CI | X2 | df | p |
| 0.524 | (0.483–0.568) | 41.010 | 1 | 0.000 | |
| Generic Name | Brand Name(s) | Dosing Schedule |
|---|---|---|
| Exenatide | Byetta, Bydureon | Byetta: twice daily; Bydureon: once weekly |
| Liraglutide | Victoza, Saxenda | Once daily |
| Dulaglutide | Trulicity | Once weekly |
| Semaglutide | Ozempic, Rybelsus, Wegovy | Ozempic: once weekly; Rybelsus: once daily; Wegovy: once weekly |
| Albiglutide | Tanzeum | Once weekly |
| Lixisenatide | Adlyxin, Lyxumia | Once daily |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayoub, M.; Faris, C.; Juranovic, T.; Chela, H.; Daglilar, E. The Use of Glucagon-like Peptide-1 Receptor Agonists in Patients with Type 2 Diabetes Mellitus Does Not Increase the Risk of Pancreatic Cancer: A U.S.-Based Cohort Study. Cancers 2024, 16, 1625. https://doi.org/10.3390/cancers16091625
Ayoub M, Faris C, Juranovic T, Chela H, Daglilar E. The Use of Glucagon-like Peptide-1 Receptor Agonists in Patients with Type 2 Diabetes Mellitus Does Not Increase the Risk of Pancreatic Cancer: A U.S.-Based Cohort Study. Cancers. 2024; 16(9):1625. https://doi.org/10.3390/cancers16091625
Chicago/Turabian StyleAyoub, Mark, Carol Faris, Tajana Juranovic, Harleen Chela, and Ebubekir Daglilar. 2024. "The Use of Glucagon-like Peptide-1 Receptor Agonists in Patients with Type 2 Diabetes Mellitus Does Not Increase the Risk of Pancreatic Cancer: A U.S.-Based Cohort Study" Cancers 16, no. 9: 1625. https://doi.org/10.3390/cancers16091625