Circulating Tumor Cells Detection and Counting in Uveal Melanomas by a Filtration-Based Method


 ,
,
Abstract
:1. Introduction
2. Results and Discussion
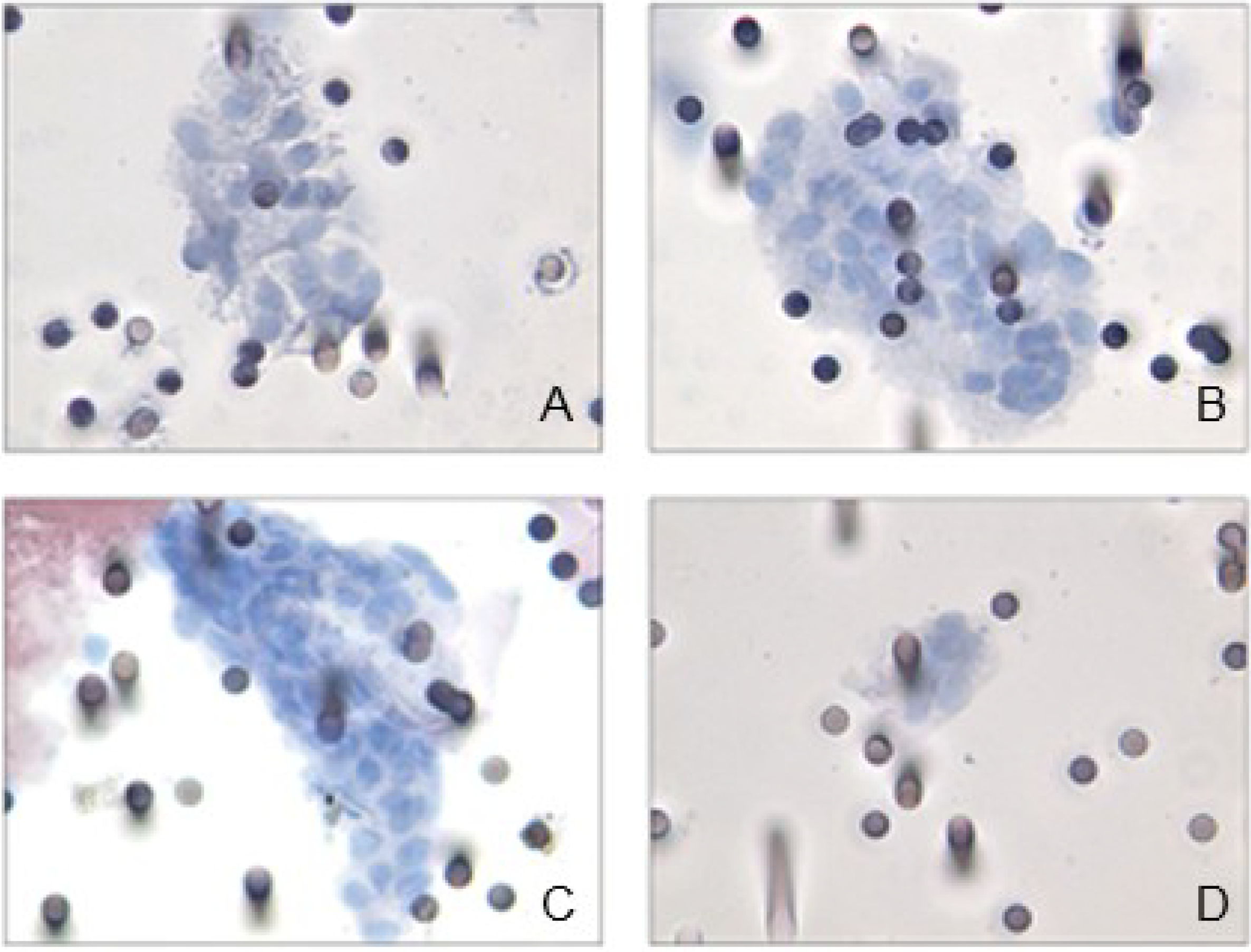
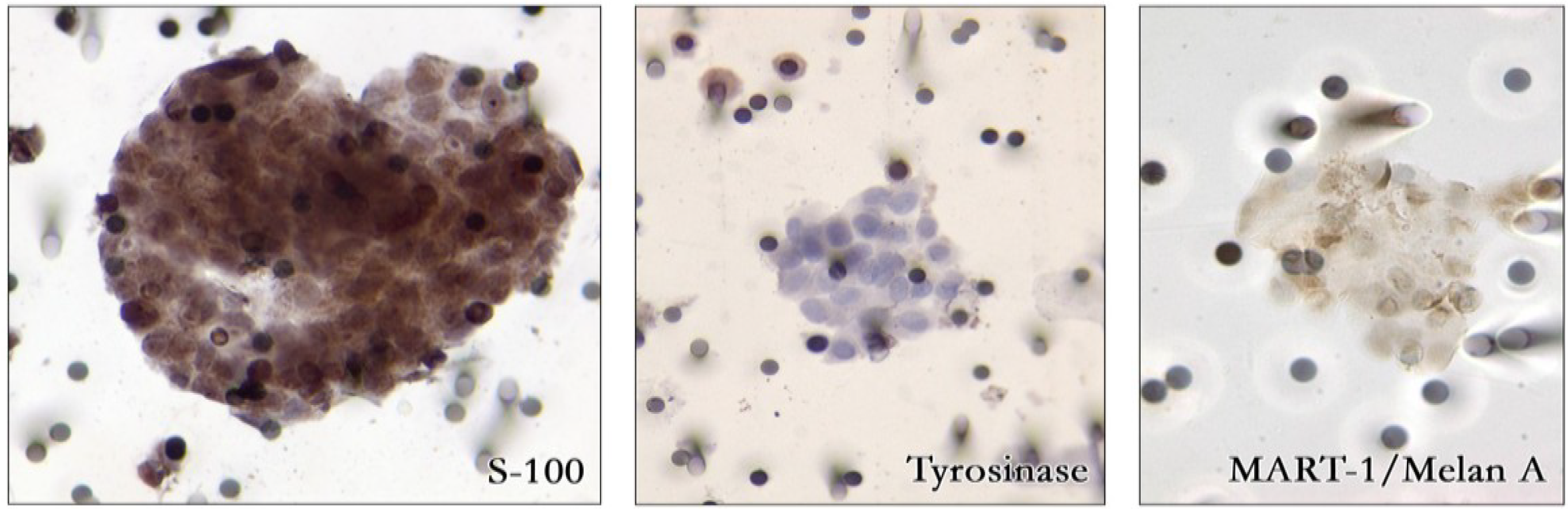
2.1. Detection of Circulating Uveal Melanoma Cells by ISET


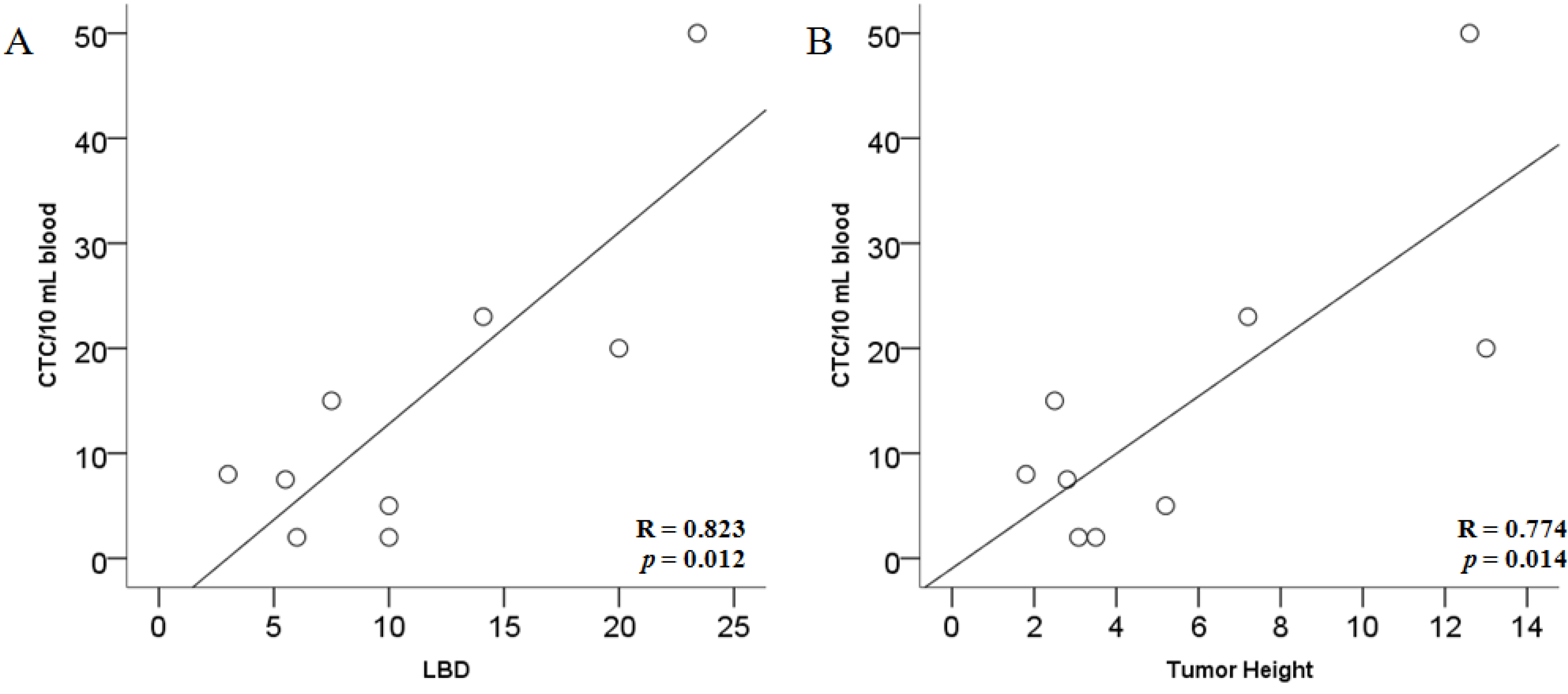
2.2. Correlation of CTC Number and CTM with Tumor Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | All patients (n = 31) | CTC Positive (n = 17) | CTC Negative (n = 14) | p value CTC+ vs. CTC− |
|---|---|---|---|---|
| Age (years) | ||||
| median | 72 | 72 | 74 | 0.564 a |
| min-max | 52–89 | 52–82 | 54–89 | |
| Sex | ||||
| Female | 14 | 7 | 7 | 0.725 b |
| Male | 17 | 10 | 7 | |
| LBD (mm) | ||||
| median | 10.0 | 9.8 | 9.7 | 0.691 a |
| min-max | 3.0–23.4 | 3.0–23.4 | 5.6–20.0 | |
| <14.0 mm | 24 | 12 | 12 | 0.412 b |
| >14.0 mm | 7 | 5 | 2 | |
| Tumor Height (mm) | ||||
| median | 4.2 | 3.5 | 4.35 | 0.796 a |
| min-max | 1.8–13.5 | 1.8–13.0 | 2.2–13.5 | |
| <7.0 mm | 23 | 12 | 11 | 0.698 b |
| >7.0 mm | 8 | 5 | 3 | |
| TNM | ||||
| T1N0M0 | 7 | 4 | 3 | 0.557 b |
| T2N0M0 | 17 | 8 | 9 | |
| T3N0M0 | 4 | 3 | 1 | |
| T4N0M0 | 1 | 0 | 1 | |
| T1N0M1 | 1 | 1 | 0 | |
| T4N0M1 | 1 | 1 | 0 | |
| LBD (mm) | <10 CTC/10 mL blood | >10 CTC/10 mL blood | CTM | Total |
|---|---|---|---|---|
| <14.0 mm | 17 | 1 | 6 | 24 |
| >14.0 mm | 2 | 3 | 2 | 7 |
| Total | 19 | 4 | 8 | 31 |
| Tumor Height (mm) | <10 CTC/10 mL blood | >10 CTC/10 mL blood | CTM | Total- |
|---|---|---|---|---|
| <7.0 mm | 16 | 1 | 6 | 23 |
| >7.0 mm | 3 | 3 | 2 | 8 |
| Total | 19 | 4 | 8 | 31 |

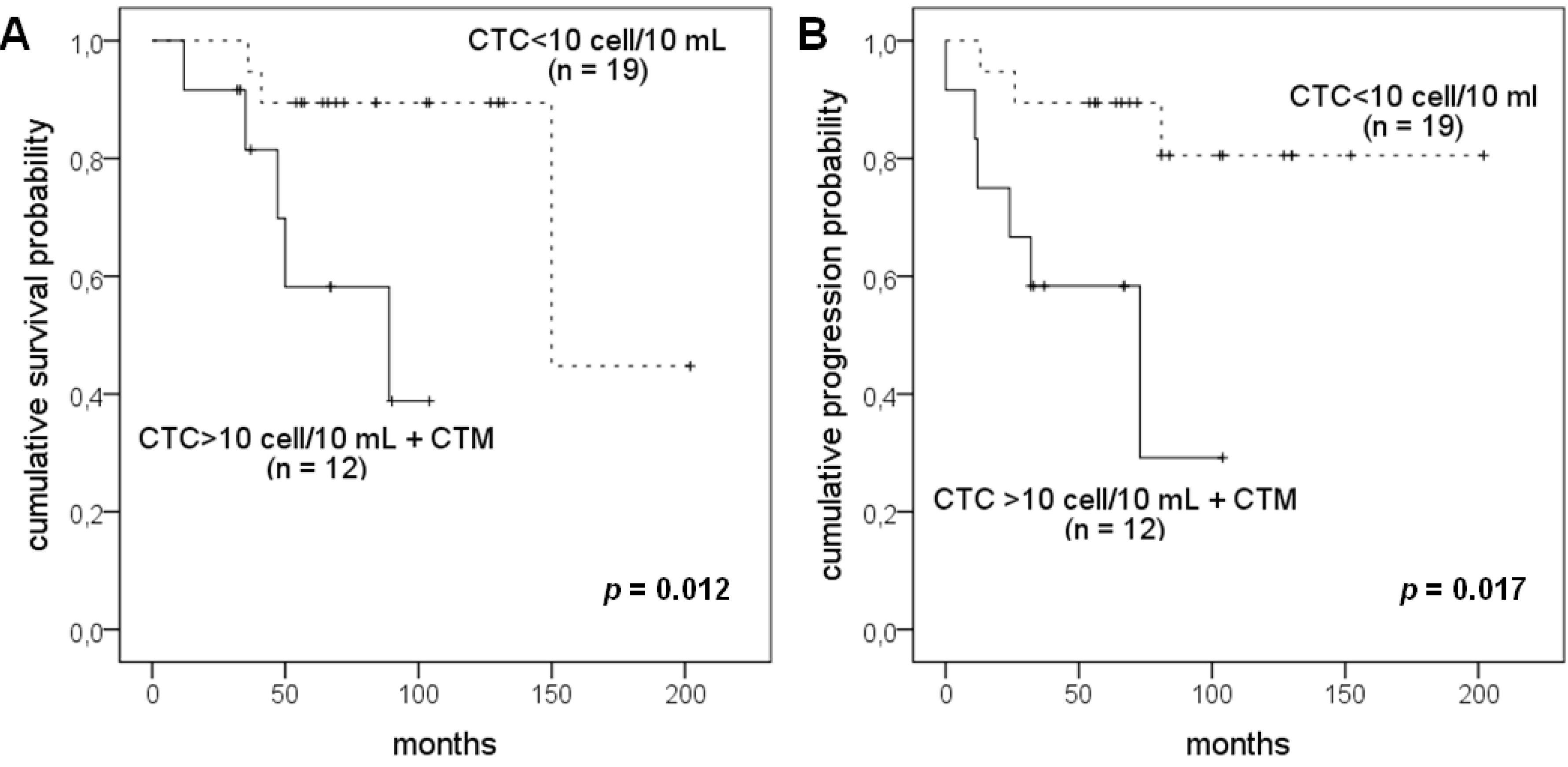
2.3. Correlation of CTC Number and CTM with Patients’ Survival

2.4. Discussion
3. Experimental
3.1. Patients and Sample Collection
3.2. Isolation by Size of Epithelial Tumor Cells (ISET)
3.3. Cell Staining and Immunostaining
3.4. Statistical Analysis
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Harbour, J.W. Clinical overwiev of uveal melanoma: Introduction to tumors of the eye. In Ocular Oncology; Albert, D.M., Polans, A., Eds.; Marcel Dekker: New York, NY, USA, 2003; pp. 1–18. [Google Scholar]
- McLaughlin, C.C.; Wu, X.C.; Jemal, A.; Martin, H.J.; Roche, L.M.; Chen, V.W. Incidence of non cutaneous melanomas in the U.S. Cancer 2005, 103, 1000–1007. [Google Scholar] [CrossRef]
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.V.; Wakade, O.A.; et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch. Ophthalmol. 2009, 127, 989–998. [Google Scholar] [CrossRef]
- Singh, A.D.; Topham, A. Survival rates with uveal melanoma in the United States: 1973–1997. Ophthalmology 2003, 110, 962–965. [Google Scholar] [CrossRef]
- Eskelin, S.; Pyrhonen, S.; Summanen, P.; Hahka-Kemppinen, M.; Kivela, T. Tumor doubling times in metastatic malignant melanoma of the uvea: Tumor progression before and after treatment. Ophthalmology 2000, 107, 1443–1449. [Google Scholar] [CrossRef]
- Suesskind, D.; Ulmer, A.; Schiebel, U.; Fierlbeck, G.; Spitzer, B.; Spitzer, M.S.; Bartz-Schmidt, K.U.; Grisanti, S. Circulating melanoma cells in peripheral blood of patients with uveal melanoma before and after different therapies and association with prognostic parameters: A pilot study. Acta Ophthalmol. 2011, 89, 17–24. [Google Scholar] [CrossRef]
- Harbour, J.W. Molecular prognostic testing and individualized patient care in uveal melanoma. Am. J. Ophthalmol. 2009, 148, 823–829. [Google Scholar]
- Pinzani, P.; Mazzini, C.; Salvianti, F.; Massi, D.; Grifoni, R.; Paoletti, C.; Ucci, F.; Molinara, E.; Orlando, C.; Pazzagli, M.; et al. Tyrosinase mRNA levels in the blood of uveal melanoma patients: Correlation with the number of circulating tumor cells and tumor progression. Melanoma Res. 2010, 20, 303–310. [Google Scholar] [CrossRef]
- Collaborative Ocular Melanoma Study Group. Histopathologic characteristic of uveal melanomas in eyes enucleated: COMS Report No. 6. Am. J. Ophthalmol. 1998, 125, 745–766. [Google Scholar] [CrossRef]
- De Giorgi, V.; Pinzani, P.; Salvianti, F.; Panelos, J.; Paglierani, M.; Janowska, A.; Grazzini, M.; Wechsler, J.; Orlando, C.; Santucci, M.; et al. Application of a filtration- and isolation-by-size technique for the detection of circulating tumor cells in cutaneous melanoma. J. Invest. Dermatol. 2010, 130, 2440–2447. [Google Scholar] [CrossRef]
- Vona, G.; Sabile, A.; Louha, M.; Sitruk, V.; Romana, S.; Schütze, K.; Capron, F.; Franco, D.; Pazzagli, M.; Vekemans, M.; et al. Isolation by size of epithelial tumor cells: A new method for the immunomorphological and molecular characterization of circulatingtumor cells. Am. J. Pathol. 2000, 156, 57–63. [Google Scholar] [CrossRef]
- Pinzani, P.; Salvadori, B.; Simi, L.; Bianchi, S.; Distante, V.; Cataliotti, L.; Pazzagli, M.; Orlando, C. Isolation by size of epithelial tumor cells in peripheral blood of patients with breast cancer: correlation with real-time reverse transcriptase-polymerase chain reaction results and feasibility of molecular analysis by laser microdissection. Hum. Pathol. 2006, 37, 711–718. [Google Scholar] [CrossRef]
- Pinzani, P.; Scatena, C.; Salvianti, F.; Corsini, E.; Canu, L.; Poli, G.; Paglierani, M.; Piccini, V.; Pazzagli, M.; Nesi, G.; et al. Detection of circulating tumor cells in patients with adrenocortical carcinoma: A monocentric preliminary study. J. Clin. Endocrinol. Metab. 2013, 98, 3731–3738. [Google Scholar] [CrossRef]
- Hou, J.M.; Krebs, M.G.; Lancashire, L.; Sloane, R.; Backen, A.; Swain, R.K.; Priest, L.J.; Greystoke, A.; Zhou, C.; Morris, K.; et al. Clinical significance and molecular characteristics of circulating tumor cells and circulating tumor microemboli in patients with small-cell lung cancer. J. Clin. Oncol. 2012, 30, 525–532. [Google Scholar] [CrossRef]
- Paterlini-Brechot, P.; Benali, N.L. Circulating tumor cells (CTC) detection: Clinical impact and future directions. Cancer Lett. 2007, 253, 180–204. [Google Scholar] [CrossRef]
- Ulmer, A.; Beutel, J.; Süsskind, D.; Hilgers, R.D.; Ziemssen, F.; Lüke, M.; Röcken, M.; Rohrbach, M.; Fierlbeck, G.; Bartz-Schmidt, K.U.; et al. Visualization of circulating melanoma cells in peripheral blood of patients with primary uveal melanoma. Clin. Cancer Res. 2008, 14, 4469–4474. [Google Scholar] [CrossRef]
- Bidard, F.C.; Madic, J.; Mariani, P.; Piperno-Neumann, S.; Rampanou, A.; Servois, V.; Cassoux, N.; Desjardins, L.; Milder, M.; Vaucher, I.; et al. Detection rate and prognostic value of circulating tumor cells and circulating tumor DNA in metastatic uveal melanoma. Int. J. Cancer 2013. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Mazzini, C.; Pinzani, P.; Salvianti, F.; Scatena, C.; Paglierani, M.; Ucci, F.; Pazzagli, M.; Massi, D. Circulating Tumor Cells Detection and Counting in Uveal Melanomas by a Filtration-Based Method. Cancers 2014, 6, 323-332. https://doi.org/10.3390/cancers6010323
Mazzini C, Pinzani P, Salvianti F, Scatena C, Paglierani M, Ucci F, Pazzagli M, Massi D. Circulating Tumor Cells Detection and Counting in Uveal Melanomas by a Filtration-Based Method. Cancers. 2014; 6(1):323-332. https://doi.org/10.3390/cancers6010323
Chicago/Turabian StyleMazzini, Cinzia, Pamela Pinzani, Francesca Salvianti, Cristian Scatena, Milena Paglierani, Francesca Ucci, Mario Pazzagli, and Daniela Massi. 2014. "Circulating Tumor Cells Detection and Counting in Uveal Melanomas by a Filtration-Based Method" Cancers 6, no. 1: 323-332. https://doi.org/10.3390/cancers6010323
APA StyleMazzini, C., Pinzani, P., Salvianti, F., Scatena, C., Paglierani, M., Ucci, F., Pazzagli, M., & Massi, D. (2014). Circulating Tumor Cells Detection and Counting in Uveal Melanomas by a Filtration-Based Method. Cancers, 6(1), 323-332. https://doi.org/10.3390/cancers6010323