
Pancreatic Cancer with Mutation in BRCA1/2, MLH1, and APC Genes: Phenotype Correlation and Detection of a Novel Germline BRCA2 Mutation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Mutational Analysis
2.3. Statistical Analysis
3. Results
3.1. HBOC Families
3.2. LS Families
3.3. FAP Families
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simoes, P.K.; Olson, S.H.; Saldia, A.; Kurtz, R.C. Epidemiology of pancreatic adenocarcinoma. Chin. Clin. Oncol. 2017, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.M.; Turk, T.; Al-Husseini, M.J.; Abdel-Rahman, O. Trends in pancreatic adenocarcinoma incidence and mortality in the United States in the last four decades; a SEER-based study. BMC Cancer 2018, 18, 688. [Google Scholar] [CrossRef] [PubMed]
- Collaborators GBDPC. The global, regional, and national burden of pancreatic cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2019, 4, 934–947. [Google Scholar] [CrossRef] [Green Version]
- Pilarski, R. The Role of BRCA Testing in Hereditary Pancreatic and Prostate Cancer Families. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Shimmura, H.; Kuramochi, H.; Jibiki, N.; Katagiri, S.; Nishino, T.; Araida, T. Dramatic response of FOLFIRINOX regimen in a collision pancreatic adenocarcinoma patient with a germline BRCA2 mutation: A case report. Jpn. J. Clin. Oncol. 2019, 49, 1049–1054. [Google Scholar] [CrossRef]
- Petersen, G.M. Familial pancreatic cancer. Semin. Oncol. 2016, 43, 548–553. [Google Scholar] [CrossRef] [Green Version]
- Vietri, M.T.; D’Elia, G.; Caliendo, G.; Casamassimi, A.; Resse, M.; Passariello, L.; Cioffi, M.; Molinari, A.M. Double mutation of APC and BRCA1 in an Italian family. Cancer Genet. 2020, 244, 32–35. [Google Scholar] [CrossRef]
- Vietri, M.T.; D’Elia, G.; Caliendo, G.; Casamassimi, A.; Federico, A.; Passariello, L.; Cioffi, M.; Molinari, A.M. Prevalence of mutations in BRCA and MMR genes in patients affected with hereditary endometrial cancer. Med. Oncol. 2021, 38, 13. [Google Scholar] [CrossRef]
- Vietri, M.T.; Molinari, A.M.; De Paola, M.; Cantile, F.; Fasano, M.; Cioffi, M. Identification of a novel in-frame deletion in BRCA2 and analysis of variants of BRCA1/2 in Italian patients affected with hereditary breast and ovarian cancer. Clin. Chem. Lab. Med. 2012, 50, 2171–2180. [Google Scholar] [CrossRef]
- Vietri, M.T.; D’Elia, G.; Benincasa, G.; Ferraro, G.; Caliendo, G.; Nicoletti, G.F.; Napoli, C. DNA methylation and breast cancer: A way forward (Review). Int. J. Oncol. 2021, 59, 98. [Google Scholar] [CrossRef]
- Lai, E.; Ziranu, P.; Spanu, D.; Dubois, M.; Pretta, A.; Tolu, S.; Camera, S.; Liscia, N.; Mariani, S.; Persano, M.; et al. BRCA-mutant pancreatic ductal adenocarcinoma. Br. J. Cancer 2021, 125, 1321–1332. [Google Scholar] [CrossRef]
- Benzel, J.; Fendrich, V. Familial Pancreatic Cancer. Oncol. Res. Treat. 2018, 41, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, E.M.; McKernin, S.E.; Brand, R.; Canto, M.; Goggins, M.; Moravek, C.; Nagarajan, A.; Petersen, G.M.; Simeone, D.M.; Yurgelun, M.; et al. Evaluating susceptibility to pancreatic cancer: ASCO Provisional Clinical Opinion. J. Clin. Oncol. 2019, 37, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Colao, A.; de Nigris, F.; Modica, R.; Napoli, C. Clinical Epigenetics of Neuroendocrine Tumors: The Road Ahead. Front. Endocrinol. 2020, 11, 604341. [Google Scholar] [CrossRef] [PubMed]
- de Nigris, F.; Ruosi, C.; Napoli, C. Clinical efficiency of epigenetic drugs therapy in bone malignancies. Bone 2021, 143, 115605. [Google Scholar] [CrossRef]
- Scognamiglio, G.; De Chiara, A.; Parafioriti, A.; Armiraglio, E.; Fazioli, F.; Gallo, M.; Aversa, L.; Camerlingo, R.; Cacciatore, F.; Colella, G.; et al. Patient-derived organoids as a potential model to predict response to PD-1/PD-L1 checkpoint inhibitors. Br. J. Cancer 2019, 121, 979–982. [Google Scholar] [CrossRef] [Green Version]
- Ohmoto, A.; Yachida, S.; Morizane, C. Genomic Features and Clinical Management of Patients with Hereditary Pancreatic Cancer Syndromes and Familial Pancreatic Cancer. Int. J. Mol. Sci. 2019, 20, 561. [Google Scholar] [CrossRef] [Green Version]
- Sehdev, A.; Gbolahan, O.; Hancock, B.A.; Stanley, M.; Shahda, S.; Wan, J.; Wu, H.H.; Radovich, M.; O’Neil, B.H. Germline and Somatic DNA Damage Repair Gene Mutations and Overall Survival in Metastatic Pancreatic Adenocarcinoma Patients Treated with FOLFIRINOX. Clin. Cancer Res. 2018, 24, 6204–6211. [Google Scholar] [CrossRef] [Green Version]
- Williet, N.; Petrillo, A.; Roth, G.; Ghidini, M.; Petrova, M.; Forestier, J.; Lopez, A.; Thoor, A.; Weislinger, L.; De Vita, F.; et al. Gemcitabine/Nab-Paclitaxel versus FOLFIRINOX in Locally Advanced Pancreatic Cancer: A European Multicenter Study. Cancers 2021, 13, 2797. [Google Scholar] [CrossRef]
- Vietri, M.T.; Molinari, A.M.; Caliendo, G.; De Paola, M.L.; D’Elia, G.; Gambardella, A.L.; Petronella, P.; Cioffi, M. Double heterozygosity in the BRCA1 and BRCA2 genes in Italian family. Clin. Chem. Lab. Med. 2013, 51, 2319–2324. [Google Scholar] [CrossRef]
- Vietri, M.T.; Caliendo, G.; Schiano, C.; Casamassimi, A.; Molinari, A.M.; Napoli, C.; Cioffi, M. Analysis of PALB2 in a cohort of Italianbreastcancerpatients: Identification of a novel PALB2 truncatingmutation. Fam. Cancer 2015, 14, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Vietri, M.T.; Caliendo, G.; Casamassimi, A.; Cioffi, M.; De Paola, M.L.; Napoli, C.; Molinari, A.M. A novel PALB2 truncatingmutation in an Italian family with male breastcancer. Oncol. Rep. 2015, 33, 1243–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Xi, S.Y.; Hao, W.W.; Yang, X.H.; Deng, L.; Xu, Y.X.; Wu, X.Y.; Zeng, L.; Guo, K.H.; Wang, H.Y. Mutational landscape of primary pulmonary salivary gland-type tumors through targeted next-generation sequencing. Lung Cancer 2021, 160, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Peretti, U.; Cavaliere, A.; Niger, M.; Tortora, G.; Di Marco, M.C.; Rodriquenz, M.G.; Centonze, F.; Rapposelli, I.G.; Giordano, G.; De Vita, F.; et al. Germinal BRCA1-2 pathogenic variants (gBRCA1-2pv) and pancreatic cancer: Epidemiology of an Italian patient cohort. ESMO Open 2021, 6, 100032. [Google Scholar] [CrossRef]
- Matsubayashi, H.; Takaori, K.; Morizane, C.; Maguchi, H.; Mizuma, M.; Takahashi, H.; Wada, K.; Hosoi, H.; Yachida, S.; Suzuki, M.; et al. Familial pancreatic cancer: Concept, management and issues. World J. Gastroenterol. 2017, 23, 935–948. [Google Scholar] [CrossRef]
- Rosen, M.N.; Goodwin, R.A.; Vickers, M.M. BRCA mutated pancreatic cancer: A change is coming. World J. Gastroenterol. 2021, 27, 1943–1958. [Google Scholar] [CrossRef]
- Zhen, D.B.; Rabe, K.G.; Gallinger, S.; Syngal, S.; Schwartz, A.G.; Goggins, M.G.; Hruban, R.H.; Cote, M.L.; McWilliams, R.R.; Roberts, N.J.; et al. BRCA1, BRCA2, PALB2, and CDKN2A mutations in familial pancreatic cancer: A PACGENE study. Genet. Med. 2015, 17, 569–577. [Google Scholar] [CrossRef] [Green Version]
- Catts, Z.A.; Baig, M.K.; Milewski, B.; Keywan, C.; Guarino, M.; Petrelli, N. Statewide Retrospective Review of Familial Pancreatic Cancer in Delaware, and Frequency of Genetic Mutations in Pancreatic Cancer Kindreds. Ann. Surg. Oncol. 2016, 23, 1729–1735. [Google Scholar] [CrossRef]
- Wong, W.; Raufi, A.G.; Safyan, R.A.; Bates, S.E.; Manji, G.A. BRCA Mutations in Pancreas Cancer: Spectrum, Current Management, Challenges and Future Prospects. Cancer Manag. Res. 2020, 12, 2731–2742. [Google Scholar] [CrossRef] [Green Version]
- Vietri, M.T.; D’Elia, G.; Caliendo, G.; Resse, M.; Casamassimi, A.; Passariello, L.; Albanese, L.; Cioffi, M.; Molinari, A.M. Hereditary Prostate Cancer: GenesRelated, Target Therapy and Prevention. Int. J. Mol. Sci. 2021, 22, 3753. [Google Scholar] [CrossRef]
- Moscatello, C.; Di Nicola, M.; Veschi, S.; Di Gregorio, P.; Cianchetti, E.; Stuppia, L.; Battista, P.; Cama, A.; Curia, M.C.; Aceto, G.M. Relationshipbetween MUTYH, OGG1 and BRCA1 mutations and mRNAexpression in breast and ovariancancerpredisposition. Mol. Clin. Oncol. 2021, 14, 15. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.; Das, S.; Brand, R.; Whitcomb, D.C. Inherited pancreatic cancer syndromes. Cancer J. 2012, 18, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, K.M.; Brune, K.A.; Griffin, C.; Sollenberger, J.E.; Petersen, G.M.; Bansal, R.; Hruban, R.H.; Kern, S.E. Evaluation of candidate genes MAP2K4, MADH4, ACVR1B, and BRCA2 in familial pancreatic cancer: Deleterious BRCA2 mutations in 17%. Cancer Res. 2002, 62, 3789–3793. [Google Scholar] [PubMed]
- Hahn, S.A.; Greenhalf, B.; Ellis, I.; Sina-Frey, M.; Rieder, H.; Korte, B.; Gerdes, B.; Kress, R.; Ziegler, A.; Raeburn, J.A.; et al. BRCA2 germline mutations in familial pancreatic carcinoma. J. Natl. Cancer Inst. 2003, 95, 214–221. [Google Scholar] [CrossRef]
- Bujanda, L.; Herreros-Villanueva, M. Pancreatic Cancer in Lynch Syndrome Patients. J. Cancer 2017, 8, 3667–3674. [Google Scholar] [CrossRef] [Green Version]
- Salo-Mullen, E.E.; O’Reilly, E.M.; Kelsen, D.P.; Ashraf, A.M.; Lowery, M.A.; Yu, K.H.; Reidy, D.L.; Epstein, A.S.; Lincoln, A.; Saldia, A.; et al. Identification of germline genetic mutations in patients with pancreatic cancer. Cancer 2015, 121, 4382–4388. [Google Scholar] [CrossRef]
- Vietri, M.T.; Caliendo, G.; D’Elia, G.; Resse, M.; Casamassimi, A.; Minucci, P.B.; Dello Ioio, C.; Cioffi, M.; Molinari, A.M. FiveItalian Families with TwoMutations in BRCA Genes. Genes 2020, 11, 1451. [Google Scholar] [CrossRef]
- Lowery, M.A.; Kelsen, D.P.; Stadler, Z.K.; Yu, K.H.; Janjigian, Y.Y.; Ludwig, E.; D’Adamo, D.R.; Salo-Mullen, E.; Robson, M.E.; Allen, P.J.; et al. An emerging entity: Pancreatic adenocarcinoma associated with a known BRCA mutation: Clinical descriptors, treatment implications, and future directions. Oncologist 2011, 16, 1397–1402. [Google Scholar] [CrossRef] [Green Version]
- Vietri, M.T.; Caliendo, G.; D’Elia, G.; Resse, M.; Casamassimi, A.; Minucci, P.B.; Cioffi, M.; Molinari, A.M. BRCA and PALB2 mutations ina cohort of male breastcancer with onebilateral case. Eur. J. Med. Genet. 2020, 63, 103883. [Google Scholar] [CrossRef]
- Scarpitta, R.; Zanna, I.; Aretini, P.; Gambino, G.; Scatena, C.; Mei, B.; Ghilli, M.; Rossetti, E.; Roncella, M.; Congregati, C.; et al. Germline investigation in male breast cancer of DNA repairgenes by next-generation sequencing. Breast Cancer Res. Treat. 2019, 178, 557–564. [Google Scholar] [CrossRef]
- Cardoso, F.C.; Goncalves, S.; Mele, P.G.; Liria, N.C.; Sganga, L.; Diaz Perez, I.; Podesta, E.J.; Solano, A.R. BRCA1 and BRCA2 mutations and clinical interpretation in 398 ovarian cancer patients: Comparison with breast cancer variants in a similar population. Hum. Genom. 2018, 12, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toss, A.; Venturelli, M.; Molinaro, E.; Pipitone, S.; Barbieri, E.; Marchi, I.; Tenedini, E.; Artuso, L.; Castellano, S.; Marino, M.; et al. Hereditary Pancreatic Cancer: A Retrospective Single-Center Study of 5143 Italian Families with History of BRCA-Related Malignancies. Cancers 2019, 11, 193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yurgelun, M.B.; Chittenden, A.B.; Morales-Oyarvide, V.; Rubinson, D.A.; Dunne, R.F.; Kozak, M.M.; Qian, Z.R.; Welch, M.W.; Brais, L.K.; Da Silva, A.; et al. Germline cancer susceptibility gene variants, somatic second hits, and survival outcomes inpatients with resected pancreatic cancer. Genet. Med. 2019, 21, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Møller, P.; Seppälä, T.T.; Bernstein, I.; Holinski-Feder, E.; Sala, P.; Gareth Evans, D.; Lindblom, A.; Macrae, F.; Blanco, I.; Sijmons, R.H.; et al. Cancer risk and survival in path_MMR carriers by gene and gender up to 75 years of age: A report from the Prospective Lynch Syndrome Database. Gut 2018, 67, 1306–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umar, A.; Boland, C.R.; Terdiman, J.P.; Syngal, S.; de la Chapelle, A.; Rüschoff, J.; Fishel, R.; Lindor, N.M.; Burgart, L.J.; Hamelin, R.; et al. Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J. Natl. Cancer Inst. 2004, 96, 261–268. [Google Scholar] [CrossRef] [PubMed]
- D’Elia, G.; Caliendo, G.; Casamassimi, A.; Cioffi, M.; Molinari, A.M.; Vietri, M.T. APC and MUTYH Analysis in FAP Patients: A Novel Mutation in APC Gene and Genotype-Phenotype Correlation. Genes 2018, 9, 322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goehringer, C.; Sutter, C.; Kloor, M.; Gebert, J.; Slater, E.P.; Keller, M.; Treiber, I.; Ganschow, P.; Kadmon, M.; Moog, U. Double germline mutations in APC and BRCA2 in an individual with a pancreatic tumor. Fam. Cancer 2017, 16, 303–309. [Google Scholar] [CrossRef]
- Giardiello, F.M.; Offerhaus, G.J.; Lee, D.H.; Krush, A.J.; Tersmette, A.C.; Booker, S.V.; Kelley, N.C.; Hamilton, S.R. Increased risk of thyroid and pancreatic carcinoma in familial adenomatous polyposis. Gut 1993, 34, 1394–1396. [Google Scholar] [CrossRef] [Green Version]
- Moussata, D.; Senouci, L.; Berger, F.; Scoazec, J.Y.; Pinson, S.; Walter, T.; Lombard-Bohas, C.; Saurin, J.C. Familial adenomatous polyposis and pancreatic cancer. Pancreas 2015, 44, 512–513. [Google Scholar] [CrossRef]
- Bellastella, G.; Maiorino, M.I.; De Bellis, A.; Vietri, M.T.; Mosca, C.; Scappaticcio, L.; Pasquali, D.; Esposito, K.; Giugliano, D. Serum but not salivary cortisol levels are influenced by daily glycemic oscillations in type 2 diabetes. Endocrine 2016, 53, 220–226. [Google Scholar] [CrossRef]
- Dinarvand, P.; Davaro, E.P.; Doan, J.V.; Ising, M.E.; Evans, N.R.; Phillips, N.J.; Lai, J.; Guzman, M.A. Familial Adenomatous Polyposis Syndrome: An Update and Review of Extraintestinal Manifestations. Arch. Pathol. Lab. Med. 2019, 143, 1382–1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canto, M.I.; Harinck, F.; Hruban, R.H.; Offerhaus, G.J.; Poley, J.; Kamel, I.; Nio, Y.; Schulick, R.S.; Bassi, C.; Kluijt, I.; et al. International Cancer of Pancreas Screening (CAPS) Consortium. International Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancer. Pract. Guidel. Gut 2013, 62, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Syngal, S.; Brand, R.E.; Church, J.M.; Giardiello, F.M.; Hampel, H.L.; Burt, R.W.; American College of Gastroenterology. ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am. J. Gastroenterol. 2015, 110, 223–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020. [Google Scholar] [CrossRef]
- Golan, T.; Kanji, Z.S.; Epelbaum, R.; Devaud, N.; Dagan, E.; Holter, S.; Aderka, D.; Paluch-Shimon, S.; Kaufman, B.; Gershoni-Baruch, R.; et al. Overall survival and clinical characteristics of pancreatic cancer in BRCA mutation carriers. Br. J. Cancer 2014, 111, 1132–1138. [Google Scholar] [CrossRef]
- NCCN Guidelines Version 2. 2018 Pancreatic Adenocarcinoma. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx (accessed on 25 December 2018).
- Farmer, H.; McCabe, N.; Lord, C.J.; Tutt, A.N.; Johnson, D.A.; Richardson, T.B.; Santarosa, M.; Dillon, K.J.; Hickson, I.; Knights, C.; et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature 2005, 434, 917–921. [Google Scholar] [CrossRef]
- Bryant, H.E.; Schultz, N.; Thomas, H.D.; Parker, K.M.; Flower, D.; Lopez, E.; Kyle, S.; Meuth, M.; Curtin, N.J.; Helleday, T. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature 2005, 434, 913–991. [Google Scholar] [CrossRef]
- Czink, E.; Kloor, M.; Goeppert, B.; Fröhling, S.; Uhrig, S.; Weber, T.F.; Meinel, J.; Sutter, C.; Weiss, K.H.; Schirmacher, P.; et al. Successful immune checkpoint blockade in a patient with advanced stage microsatellite-unstable biliary tract cancer. Cold Spring Harb. Mol. Case Stud. 2017, 3, a001974. [Google Scholar] [CrossRef]
- Hu, Z.I.; Shia, J.; Stadler, Z.K.; Varghese, A.M.; Capanu, M.; Salo-Mullen, E.; Lowery, M.A.; Diaz, L.A., Jr.; Mandelker, D.; Yu, K.H.; et al. Evaluating mismatch repair deficiency in pancreatic adenocarcinoma: Challenges and recommendations. Clin. Cancer Res. 2018, 24, 1326–1336. [Google Scholar] [CrossRef] [Green Version]
- Albanese, L.; Caliendo, G.; D’Elia, G.; Passariello, L.; Molinari, A.M.; Napoli, C.; Vietri, M.T. Diagnostic utility of FGF-23 in mineral bone disorder during chronic kidney disease. J. Circ. Biomark. 2022, 11, 1–4. [Google Scholar] [CrossRef]
- Montisci, A.; Vietri, M.T.; Palmieri, V.; Sala, S.; Donatelli, F.; Napoli, C. Cardiac Toxicity Associated with Cancer Immunotherapy and Biological Drugs. Cancers 2021, 13, 4797. [Google Scholar] [CrossRef] [PubMed]
- Montisci, A.; Palmieri, V.; Liu, J.E.; Vietri, M.T.; Cirri, S.; Donatelli, F.; Napoli, C. Severe Cardiac Toxicity Induced by Cancer Therapies Requiring Intensive Care Unit Admission. Front. Cardiovasc. Med. 2021, 8, 713694. [Google Scholar] [CrossRef] [PubMed]
- Celešnik, H.; Potocnik, U. Peripheral Blood Transcriptome in Breast Cancer Patients as aSource of Less Invasive Immune Biomarkers for Personalized Medicine, and Implications for Triple Negative Breast Cancer. Cancers 2022, 14, 591. [Google Scholar] [CrossRef]
- Singh, J.; Sangwan, N.; Chauhan, A.; Sarma, P.; Prakash, A.; Medhi, B.; Avti, P.K. Screening and identification of phytochemical drug molecules against mutant BRCA1 receptor of breast cancer using computational approaches. Mol. Cell. Biochem. 2022. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Syndrome | N° of Families (Probands Total 69) | N° and Tumor Type of Probands | Mutation Rate | N° of PDAC Cases (Total 80) | Mean Age of PDAC Onset |
|---|---|---|---|---|---|
| HBOC | 56 | 13 pancreatic cancers; 34 breast cancers 5 ovarian cancers 3 breast and ovarian cancer 1 breast and colon cancer | (16/56) 28.6% | 64 | 66 years |
| LS | 7 | 2 pancreatic cancer 4 colon cancer 1 ovarian cancer | (2/7) 28.6% | 8 | 58.6 years |
| FAP | 3 | 1 pancreatic cancer 2 colon cancer | (1/3) 33.3% | 5 | 48.8 years |
| FAMMM | 2 | 2 melanoma | - | 2 | 62 years |
| LFS | 1 | 1 sarcoma | - | 1 | 65 years |
| Number (77) | PDAC Patients of Non Mutated Families (55) | PDAC Patients of Mutated Families (22) | p-Value | |
|---|---|---|---|---|
| Gender | Females (30) | 22 (40%) | 8 (36%) | 0.77 |
| Males (47) | 33 (60%) | 14 (64%) | ||
| Mean age of PDAC onset (SD) | 64.5 (12.7) | 62.8 (11.7) | 0.59 | |
| Mean age of death (SD) | 66.8 (13.3) | 64.0 (11.7) | 0.41 |
| Type of Cancer | Cancer Number in Family | Non Mutated PDAC Patients | Mutated PDAC Patients | p-Value |
|---|---|---|---|---|
| BC | 0 | 2 (4%) | 2 (11%) | 0.27 |
| 1 | 15 (33%) | 2 (11%) | ||
| 2 | 13 (28%) | 4 (22%) | ||
| 3 | 10 (22%) | 5 (28%) | ||
| ≥4 | 6 (13%) | 5 (28%) | ||
| PDAC | 1 | 34 (74%) | 14 (78%) | 0.75 |
| 2 | 12 (26%) | 4 (22%) | ||
| OC | 0 | 33 (72%) | 8 (44%) | 0.042 |
| 1 | 11 (24%) | 6 (33%) | ||
| 2 | 2 (4%) | 4 (22%) | ||
| LC | 0 | 23 (50%) | 10 (56%) | 0.30 |
| 1 | 18 (39%) | 4 (22%) | ||
| 2 | 4 (9%) | 3 (17%) | ||
| 3 | 1 (2%) | 0 (0%) | ||
| 4 | 0 (0%) | 1 (6%) | ||
| LVC | 0 | 34 (74%) | 13 (72%) | 0.34 |
| 1 | 10 (22%) | 4 (22%) | ||
| 2 | 2 (4%) | 0 (0%) | ||
| 3 | 0 (0%) | 1 (6%) | ||
| GC | 0 | 27 (59%) | 11 (61%) | 0.93 |
| 1 | 15 (33%) | 6 (33%) | ||
| 2 | 3 (7%) | 1 (6%) | ||
| 4 | 1 (2%) | 0 (0%) | ||
| EC | 0 | 33 (72%) | 15 (83%) | 0.71 |
| 1 | 7 (15%) | 1 (6%) | ||
| 2 | 4 (9%) | 1 (6%) | ||
| 3 | 2 (4%) | 1 (6%) | ||
| CC | 0 | 34 (74%) | 14 (78%) | 0.78 |
| 1 | 6 (13%) | 3 (17%) | ||
| 2 | 4 (9%) | 1 (6%) | ||
| 3 | 2 (4%) | 0 (0%) | ||
| BLC | 0 | 37 (80%) | 15 (83%) | 0.35 |
| 1 | 8 (17%) | 2 (11%) | ||
| 2 | 0 (0%) | 1 (6%) | ||
| 3 | 1 (2%) | 0 (0%) | ||
| PC | 0 | 40 (87%) | 14 (78%) | 0.62 |
| 1 | 5 (11%) | 3 (17%) | ||
| 2 | 1 (2%) | 1 (6%) | ||
| LEU | 0 | 41 (89%) | 15 (83%) | 0.53 |
| 1 | 5 (11%) | 3 (17%) | ||
| bBC | 0 | 44 (96%) | 15 (83%) | 0.099 |
| 1 | 2 (4%) | 3 (17%) | ||
| LAC | 0 | 39 (85%) | 15 (83%) | 0.77 |
| 1 | 6 (13%) | 3 (17%) | ||
| 2 | 1 (2%) | 0 (0%) | ||
| MEL | 0 | 43 (93%) | 16 (89%) | 0.54 |
| 1 | 3 (7%) | 2 (11%) | ||
| KC | 0 | 43 (93%) | 17 (94%) | 0.89 |
| 1 | 3 (7%) | 1 (6%) | ||
| ESC | 0 | 45 (98%) | 16 (89%) | 0.13 |
| 1 | 1 (2%) | 2 (11%) | ||
| BRC | 0 | 43 (93%) | 17 (94%) | 0.81 |
| 1 | 2 (4%) | 1 (6%) | ||
| 2 | 1 (2%) | 0 (0%) | ||
| TC | 0 | 42 (91%) | 18 (100%) | 0.20 |
| 1 | 4 (9%) | 0 (0%) |
| Family | Gene | Mutation | Exon | Family Members (Diagnosis) | Age | Mutational Analysis |
|---|---|---|---|---|---|---|
| 1 | BRCA1 | c.181T>G (p.Cys61Gly) | 5 | Proband (Ovarian Cancer) | 72 | Mutated |
| Sister (Breast Cancer) | 64 | Mutated | ||||
| Daughter (Unaffected) | 48 | Wild Type | ||||
| 2 | BRCA1 | c.917delT (p.Leu306ArgfsTer27) | 11 | Proband (Breast/Ovarian Cancer) | 56 | Mutated |
| Son (Unaffected) | 28 | Mutated | ||||
| Brother (Unaffected) | 61 | Mutated | ||||
| Sister (Unaffected) | 65 | Wild Type | ||||
| 3 | BRCA1 | c.5123C>A (p.Ala1708Glu) | 18 | Proband (Pancreatic cancer) | 67 | Mutated |
| Sister (Ovarian cancer) | 63 | Mutated | ||||
| Nephew (Unaffected) | 38 | Wild Type | ||||
| Niece (Unaffected) | 40 | Mutated | ||||
| 4 | BRCA1 | c.5266dupC (p.Gln1756Profs) | 20 | Proband (Breast and Ovarian cancer) | 64 | Mutated |
| Daugheter (Unaffected) | 62 | Wild Type | ||||
| Son (Unaffected) | 38 | Mutated | ||||
| Brother (Unaffected) | 66 | Mutated | ||||
| Niece (Breast cancer) | 32 | Mutated | ||||
| Niece (Unaffected) | 41 | Mutated | ||||
| 5 | BRCA1 | c.5266dupC (p.Gln1756Profs) | 20 | Proband (Pancreatic Cancer) | 73 | Mutated |
| Sister (Breast Cancer) | 72 | Mutated | ||||
| 6 | BRCA1 | c.5397_5398del (p.Leu1800Trpfs*29) | 22 | Proband (Ovarian Cancer) | 63 | Mutated |
| Son (Unaffected) | 33 | Wild Type | ||||
| Daughter (Unaffected) | 41 | Wild Type | ||||
| 7 | BRCA2 | c.3545_3546del (p.Gln1181_Phe1182insTer) | 11 | Proband (Ovarian cancer) | 57 | Mutated |
| Daugheter (Unaffected) | 32 | Wild Type | ||||
| Daugheter (Unaffected) | 23 | Wild Type | ||||
| Son (Unaffected) | 28 | Wild Type | ||||
| Brother (Unaffected) | 58 | Wild Type | ||||
| Sister (Ovarian cancer) | 62 | Mutated | ||||
| Niece (Unaffected) | 34 | Mutated | ||||
| Nephew (Unaffected) | 30 | Mutated | ||||
| 8 | BRCA2 | c.4284dupT (p.Gln1429Serfs) | 11 | Proband (Breast cancer) | 85 | Mutated |
| Daugheter (Unaffected) | 57 | Wild Type | ||||
| Daugheter (Unaffected) | 56 | Mutated | ||||
| Son(Unaffected) | 52 | Wild Type | ||||
| Son(Unaffected) | 50 | Mutated | ||||
| Sister (Unaffected) | 83 | Mutated | ||||
| Niece (Unaffected) | 48 | Mutated | ||||
| Nephew (Unaffected) | 42 | Mutated | ||||
| Nephew (Unaffected) | 45 | Mutated | ||||
| Nephew (Unaffected) | 36 | Wild Type | ||||
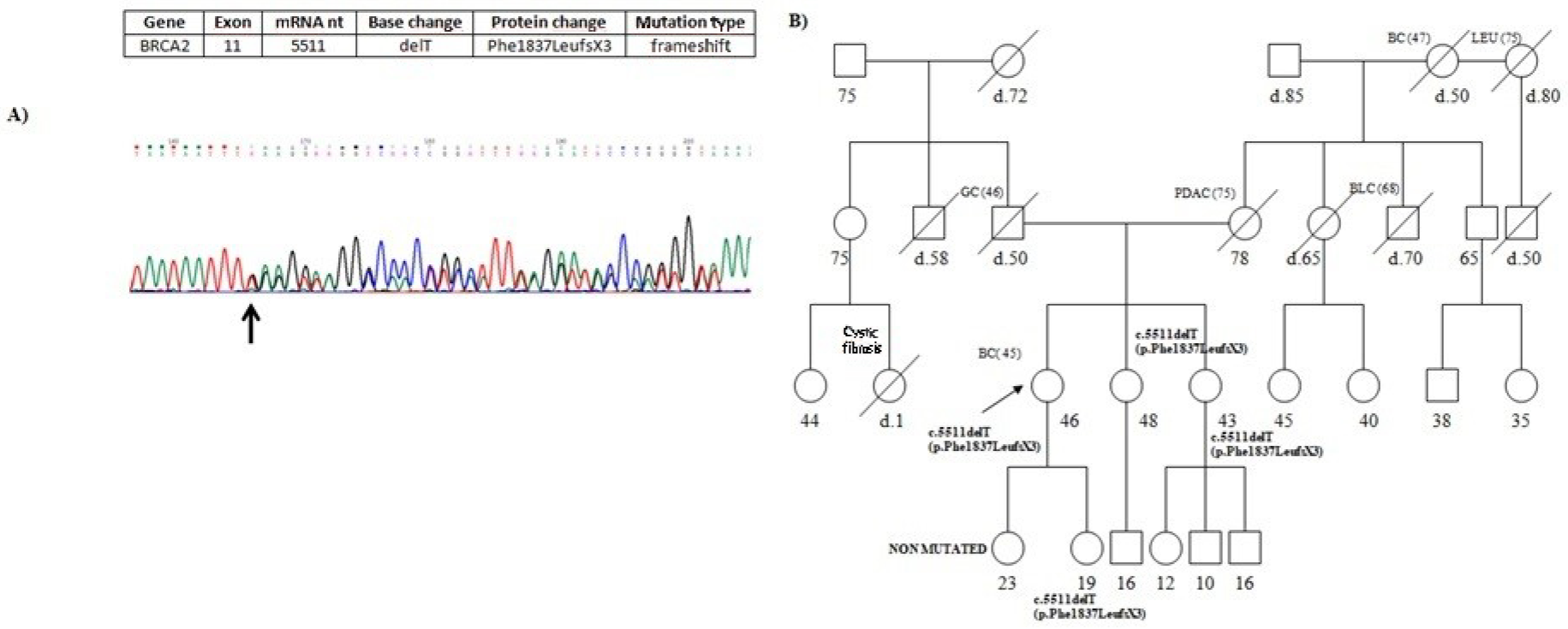
| 9 | BRCA2 | c.5511delT (p.Phe1837LeufsX3) | 11 | Proband (Breast cancer) | 46 | Mutated |
| Sister (Unaffected) | 48 | Mutated | ||||
| Sister (Unaffected) | 43 | Mutated | ||||
| Daughter (Unaffected) | 23 | Wild Type | ||||
| Daughter (Unaffected) | 19 | Mutated | ||||
| 10 | BRCA2 | c.5722_5723delCT (p.L1908RfsX2) | 11 | Proband (Breast cancer) | 62 | Mutated |
| Brother (Unaffected) | 61 | Wild Type | ||||
| 11 | BRCA2 | c.6037A>T (p.Lys2013Ter) | 11 | Proband (Ovarian cancer) | 52 | Mutated |
| Daugheter (Unaffected) | 25 | Mutated | ||||
| Son (Unaffected) | 21 | Wild type | ||||
| Sister (Unaffected) | 58 | Mutated | ||||
| Niece (Unaffected) | 32 | Wild type | ||||
| Niece (Unaffected) | 28 | Wild type | ||||
| 12 | BRCA2 | c.6450dup (p.Val2151fs) | 11 | Proband (Breast cancer) | 54 | Mutated |
| Son (Unaffected) | 24 | Wild Type | ||||
| Daughter (Unaffected) | 21 | Mutated | ||||
| 13 | BRCA2 | c.6468_6469delTC (p.Gln2157Ilefs) | 11 | Proband (Breast Cancer) | 47 | Mutated |
| Father (Unaffected) | 75 | Mutated | ||||
| Sister (Unaffected) | 46 | Mutated | ||||
| Sister (Unaffected) | 41 | Wild type | ||||
| 14 | BRCA2 | c.6468_6469delTC (p.Gln2157Ilefs) | 11 | Proband (Pancreatic Cancer) | 61 | Mutated |
| Sister (Breast and EndometrialCancer) | 62 | Mutated | ||||
| Sister (Ovarian Cancer) | 54 | Mutated | ||||
| Nephew (Unaffected) | 26 | Wild type | ||||
| 15 | BRCA2 | c.7857G>A (p.Trp2619Ter) | 17 | Proband (Breast Cancer) | 45 | Mutated |
| Sister (Unaffected) | 48 | Wild Type | ||||
| 16 | BRCA2 BRCA2 | c.631G>A (p.Val221Ile) c.7008-2A>T (IVS13-2A>T) | 7 14 | Proband (Breast Cancer) | 62 | Mutated |
| Daugheter (Unaffected) | 41 | Wild type | ||||
| Daugheter (Unaffected) | 35 | Mutated | ||||
| Brother (Unaffected) | 59 | Wild Type | ||||
| Sister (Bilateral Breast Cancer) | 56 | Mutated | ||||
| Niece (Unaffected) | 35 | Wild Type | ||||
| Niece (Unaffected) | 30 | Wild Type | ||||
| Niece (Breast cancer) | 33 † | Mutated | ||||
| Cousin (Breast cancer) | 70 | Mutated | ||||
| 1 | MLH1 | c.2181_2182delCA (p.Ile728Serfs) | 5 | Proband (Colon Cancer) | 25 | Mutated |
| Brother (Unaffected) | 29 | Wild Type | ||||
| Aunt (Breast Cancer) | 58 | Wild Type | ||||
| Aunt (Unaffected) | 54 | Wild Type | ||||
| 2 | MLH1 | c.229T>C (p.Cys77Arg) | 3 | Proband (Colon Cancer) | 48 | Mutated |
| No family members | - | |||||
| 1 | APC | c.6709C>T (p.Arg2237Ter) | Proband (Pancreatic Cancer) | 52 † | Mutated | |
| Brother (Cerebral angiomas) | 65 | Mutated | ||||
| Sister (Pancreatic Cancer) | 48 † | Mutated | ||||
| Sister (Colon Cancer) | 55 | Mutated | ||||
| Sister (Colon Cancer) | 57 | Mutated | ||||
| Sister (Unaffected) | 67 | Wild Type | ||||
| Sister (Unaffected) | 66 | Wild Type |
| Study | Disease | Phase | ID |
|---|---|---|---|
| Niraparib in patients with germline or somatic DDRmutations | Locally advanced metastatic pancreatic cancer | Phase 2 | NCT03601923 |
| Rucaparib maintenance in patients with germline or somaticBRCA or PALB2 mutations | Locally advanced metastaticpancreatic cancer | Phase 2 | NCT03140670 |
| Olaparib in gBRCA Mutated Pancreatic Cancer Whose Disease Has Not Progressed on First Line Platinum-Based Chemotherapy | MetastaticPancreaticCancer | Phase 3 | NCT02184195 |
| Chlorambucil in Metastatic PDAC Patients Bearing a Germ Line DNA Defects Repair Mutations (SALE Trial) | MetastaticPancreaticCancer | Phase 2 | NCT04692740 |
| A Study of Maintenance Treatment withFluzoparib in gBRCA/PALB2 MutatedPancreatic Cancer Whose Disease Has Not Progressed on First Line Platinum-Based Chemotherapy | MetastaticPancreaticCancer | Phase 3 | NCT04300114 |
| Testing the Addition of Pembrolizumab, an Immunotherapy Cancer Drug to Olaparib Alone as Therapy for Patients WithPancreatic Cancer That Has Spread With Inherited BRCA Mutations | MetastaticPancreaticCancer | Phase 2 | NCT04548752 |
| Niraparib and Dostarlimab for the Treatment of Germline or Somatic BRCA1/2 and PALB2 Mutated Metastatic Pancreatic Cancer | PancreaticDuctal Adenocarcinoma | Phase 2 | NCT04493060 |
| A Randomized Study of Olaparib or Placebo in Patients With Surgically Removed Pancreatic Cancer Who Have a BRCA1, BRCA2, or PALB2 Mutation, The APOLLO Trial | P adenocarcinoma | Phase 2 | NCT04858334 |
| Niraparib and TSR-042 for the Treatment of BRCA-Mutated Unresectable or Metastatic Breast, Pancreas, Ovary, Fallopian Tube, or Primary Peritoneal Cancer | UnresectablePancreatic Carcinoma, MetastaticPancreaticCancer | Phase1 | NCT04673448 |
| Durvalumab and Olaparib for the treatment of Advanced PDAC, leiomyosarcoma or mismatch repair-proficient colorectal cancer | Advanced pancreaticcancer | Phase 2 | NCT03851614 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vietri, M.T.; D’Elia, G.; Caliendo, G.; Albanese, L.; Signoriello, G.; Napoli, C.; Molinari, A.M. Pancreatic Cancer with Mutation in BRCA1/2, MLH1, and APC Genes: Phenotype Correlation and Detection of a Novel Germline BRCA2 Mutation. Genes 2022, 13, 321. https://doi.org/10.3390/genes13020321
Vietri MT, D’Elia G, Caliendo G, Albanese L, Signoriello G, Napoli C, Molinari AM. Pancreatic Cancer with Mutation in BRCA1/2, MLH1, and APC Genes: Phenotype Correlation and Detection of a Novel Germline BRCA2 Mutation. Genes. 2022; 13(2):321. https://doi.org/10.3390/genes13020321
Chicago/Turabian StyleVietri, Maria Teresa, Giovanna D’Elia, Gemma Caliendo, Luisa Albanese, Giuseppe Signoriello, Claudio Napoli, and Anna Maria Molinari. 2022. "Pancreatic Cancer with Mutation in BRCA1/2, MLH1, and APC Genes: Phenotype Correlation and Detection of a Novel Germline BRCA2 Mutation" Genes 13, no. 2: 321. https://doi.org/10.3390/genes13020321