
Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia


1
Institute of Microbiology and Immunology, Faculty of Medicine, University of Ljubljana, Zaloška Cesta 4, SI-1000 Ljubljana, Slovenia
2
Department of Public Health, Faculty of Medicine, University of Ljubljana, Zaloška Cesta 4, SI-1000 Ljubljana, Slovenia
3
Sežana Hospital, Cankarjeva Ulica 4, SI-6210 Sežana, Slovenia
4
Karst Research Institute, Research Centre of the Slovenian Academy of Sciences and Arts, Titov Trg 2, SI-6230 Postojna, Slovenia
5
UNESCO Chair on Karst Education, University of Nova Gorica, SI-5271 Vipava, Slovenia
*
Author to whom correspondence should be addressed.
Atmosphere 2024, 15(5), 518; https://doi.org/10.3390/atmos15050518
Submission received: 22 March 2024
/
Revised: 18 April 2024
/
Accepted: 22 April 2024
/
Published: 24 April 2024
(This article belongs to the Special Issue Bioaerosol Exposure and Its Risk Assessment)
Abstract
:Speleotherapy is one of the non-pharmacological methods for the treatment and rehabilitation of patients with chronic respiratory diseases, especially those with chronic obstructive pulmonary disease (COPD) and asthma. On the one hand, one of the alleged main advantages of speleotherapeutic caves is the low microbial load in the air and the absence of other aeroallergens, but on the other hand, due to the lack of comprehensive air monitoring, there is little information on the pristine and human-influenced aerobiota in such environments. The aim of this study was to assess the anthropogenic effects of speleotherapy on the air microbiota and to investigate its potential impact on human health in Sežana Hospital Cave (Slovenia). From May 2020 to January 2023, air samples were collected in the cave before and after speleotherapeutic activities using two different volumetric air sampling methods—impaction and impingement—to isolate airborne microbiota. Along with sampling, environmental data were measured (CO2, humidity, wind, and temperature) to explore the anthropogenic effects on the aerobiota. While the presence of patients increased microbial concentrations by at least 83.3%, other parameters exhibited a lower impact or were attributed to seasonal changes. The structure and dynamics of the airborne microbiota are similar to those in show caves, indicating anthropization of the cave. Locally, concentrations of culturable microorganisms above 1000 CFU/m3 were detected, which could have negative or unpredictable effects on the autochthonous microbiota and possibly on human health. A mixture of bacteria and fungi typically associated with human microbiota was found in the air and identified by MALDI-TOF MS with a 90.9% identification success rate. Micrococcus luteus, Kocuria rosea, Staphylococcus hominis, and Staphylococcus capitis were identified as reliable indicators of cave anthropization.
1. Introduction
Chronic respiratory diseases are among the most common non-communicable diseases worldwide, largely due to widespread exposure to harmful environmental stimuli as well as genetic and lifestyle factors [1,2,3]. Among them, chronic obstructive pulmonary disease (COPD) and asthma are the most prevalent diseases affecting both children and adults, with a global prevalence of 3.9% and 3.6%, respectively. COPD and asthma are also the leading causes of death associated with chronic respiratory diseases worldwide. In the European Union, for example, there were 2,348,184 deaths attributable to COPD between 1994 and 2010 [1,4,5]. The treatment of COPD and asthma is quite complex as there is no cure. Therefore, the treatment of these diseases aims to control symptoms, prevent disease progression, restore patients’ daily activities, and minimize the impact of the disease on quality of life [2,4,6]. Traditionally, treatment is pharmacologic, but patients may also benefit from non-pharmacologic treatment approaches [2,6]. As COPD and asthma are strongly influenced by environmental factors such as tobacco smoke, pollen, molds, and other aeroallergens, it is logical that environmental modification could be beneficial [2,6,7,8]. The aggravation of COPD and asthma can be influenced by environmental factors, including bioaerosols. Bioaerosols, i.e., airborne particles of biological origin, include a wide range of organisms and substances, such as bacteria, fungi, viruses, pollen, and spores. These particles can cause respiratory diseases, inflammation, allergic reactions, and infections when inhaled [9,10,11]. Therefore, environmental measures that include reducing allergens in the home (e.g., house cleaning or dust mite control) and/or eliminating irritants (e.g., avoidance of secondhand smoke) are often recommended in the management of asthma [2,6,7]. More advanced environmental modification strategies have also been proposed, such as medical rehabilitation in spas, high-altitude climatotherapy, and speleotherapy [2,7,8,12]. The latter uses the climatic conditions of caves and salt mines for the rehabilitation treatment of chronic respiratory diseases, in particular COPD and asthma, as well as for some dermatological diseases, such as atopic dermatitis in children [12,13,14].
Speleotherapy began to gain attention after the Second World War, particularly in Eastern and Central Europe, and is associated with beneficial effects on patients with chronic and allergic respiratory diseases [8,12,15,16]. The reason for the clinical improvement of these diseases lies in the microclimatic characteristics of the caves that mitigate the inflammatory response—high relative humidity, constant air temperature, aerosolized minerals, little or no wind, short exposure to occasional natural elevated levels of radiation, and the absence of external pollutants, mites, pollen, and other particles that exacerbate chronic respiratory diseases [8,12,17,18]. Together, these factors facilitate expectoration, relax the respiratory muscles, stimulate the self-cleaning function of the lungs, and have an anesthetic effect [8,12]. Speleotherapy, therefore, helps asthmatics treat the disease themselves and minimize the use of medications [19,20,21]. The positive effect of speleotherapy is usually seen after 3–4 weeks of treatment with a daily stay in a cave for 3–6 h, depending on the temperature in the subterranean environment [19,21]. Low levels of air biocontamination are, therefore, considered an important factor in speleotherapy, but the data about microbiological air monitoring in speleotherapeutic caves are still scarce [20,22,23,24,25]. Monitoring of bioaerosols and climatic conditions in speleotherapeutic caves is important from the point of view of both the therapy and environmental protection [22,23,26]. Therefore, the question arises whether patients and medical staff can significantly alter the composition and concentration of microbes in the air to such an extent that the environment in the cave becomes less favorable for both patients with respiratory diseases and the indigenous microbiota of the cave itself.
Anthropogenic changes in aerobiota have already been described in show caves, which are accessible to the public for guided tours and equipped for tourist visits, with varying degrees of anthropization [25,26,27,28]. To complement these data, we studied the natural and human-influenced aerobiota in a karst cave that serves as a speleotherapeutic center in Slovenia. This underground facility has been an integral part of the Sežana Hospital since 1993 and is used for the treatment and rehabilitation of patients with chronic respiratory diseases [29]. The aim of this study was to assess the anthropogenic effect of speleotherapy on the air microbiota and consider its potential impact on human health in the Sežana Hospital Cave.
2. Materials and Methods
2.1. Sampling Sites
The air samples were taken in an artificial cave used for speleotherapy by Sežana Hospital in Sežana, Slovenia (pronounced [sɛˈʒaːna], 45°42′33.6672″ N, 13°52′25.7448″ E, 364 m a.s.l.). Sežana Hospital is a specialized hospital for the treatment and rehabilitation of patients with chronic lung diseases. Since 1993, a significant part of respiratory rehabilitation (speleotherapy) has taken place in a partly artificial karst cave directly behind the hospital. Karst caves are natural underground passages formed by the dissolution of soluble rocks such as limestone, dolomite, and gypsum and are characterized by features such as stalactites, stalagmites, and underground rivers. The cave was dug during the Second World War and is an approximately 207-meter-long tunnel-like passage with two entrances on each side and a smaller, elongated chamber in the middle, which was originally used for storage purposes (Figure 1). The central part of the cave, where most speleotherapeutic activities take place, has a volume of approximately 407 m3 (Telovadnica, Jedilnica), while the total volume of the cave is approximately 1321 m3. The sampling sites in Sežana Hospital Cave were selected on the basis of the speleotherapeutic activities taking place in the cave. The first sampling site was a small corridor that runs perpendicular to the main tunnel and is used for lunch breaks during therapy sessions (Jedilnica, dining room in Slovenian) (Figure 1). The second sampling site was located in the middle of the small chamber used for meditation and educational purposes (Spalnica, bedroom in Slovenian), and the third sampling site was located at the other end of the same chamber used for physical activities (Telovadnica, gym in Slovenian) (Figure 1). The rehabilitation program lasts five days a week for three weeks. On average, the cave is in operation for 40 weeks a year. The group consists of 15–18 patients who are referred to Sežana Hospital by their pulmonologists or general practitioners. Patients bring their medical records, which show that they meet the requirements for admission to the rehabilitation program. During the first few days, patients are examined in a doctor’s office and undergo physical fitness tests, pulmonary function tests, and basic laboratory tests. Over the next three weeks, patients learn how to manage their medication and learn breathing exercises, expectoration, and exercises to increase general physical fitness and muscle performance. Most of this rehabilitation therapy, around four hours a day, takes place in the cave.
2.2. Air Sampling and Measurement of Environmental Parameters
The air sampling began in the morning, starting with the sampling of the outdoor air 5 m in front of the main entrance of the cave. Then, a few hours before the cave was opened to patients, air samples were collected inside the cave to obtain a natural background. Atmospheric parameters were simultaneously measured. Immediately after the exit of the patient group, the second round of sampling began to observe a direct influence of the patients on the microclimate in the cave and the air microbiota. The measurements and aerosols were collected 1.0 m above the ground on a portable platform. Air sampling and measurements in the Sežana Hospital Cave were carried out in all sections: 29 May 2020, 7 July 2020, 27 November 2021, 2 June 2022, and 10 January 2023. Two different air samplers were used simultaneously to collect bioaerosols for comparison. Both air samplers were selected because they are ISO 14698 certified and were used in our previous study [27] and in our routine microbiological air monitoring of operating theaters. A VWR® SAS Super DUO 360 Air Sampler (VWR International, Radnor, PA, USA) with an airflow of 180 L/min was used to collect bioaerosols directly onto contact agar plates, while a Coriolis®µ Cyclonic Air Sampler (Bertin Technologies, Saint Quentin en Yvelines, France) with an airflow of 150 L/min was used to collect bioaerosols in saline solution. In the case of the impactor, 0.5 m3 of air was sampled simultaneously on two contact plates (Replicate Organism Detection and Counting, RODAC) with two different growth media (see Section 2.3). Airborne particles were collected from a total air volume of 4.5 m3 in 10 mL sterile saline solution (0.9% NaCl) using the Coriolis®µ Air Sampler. Prior to sampling, the flow tube and the surfaces of both air samplers were disinfected with 96% ethanol. After sampling in the cave, the RODAC plates were sealed with parafilm. The liquid was aseptically divided in a laboratory to perform individual microbiological analyses, culture-dependent biomass estimations, and microbial identifications.
Parallel to the microbiological sampling, environmental parameters were continuously measured at 30 s intervals before and after the speleotherapeutic activities in the cave. Temperature and relative humidity were measured with a portable Kestrel 4500 PocketWeather Tracker (Kestrel Instruments, Boothwyn, PA, USA). Atmospheric CO2 was measured with a Vaisala MI70 portable carbon dioxide meter (Vaisala, Helsinki, Finland). Wind speed and flow were measured with the VelociCalc Multi-Function Ventilation Meter 9565 (TSI Incorporated, Shoreview, MN, USA).
2.3. Microbial Cultivation
2.3.1. Microbial Cultivation after Sampling with the Impactor
For air sampling with the impactor, two different RODAC plates were used simultaneously on each of the two heads of the SAS Super DUO 360 Air Sampler: BDTM Columbia Agar with 5.0% sheep blood (BA) (Becton-Dickinson, Franklin Lakes, NJ, USA) and Sabouraud Dextrose Agar supplemented with chloramphenicol (SDA) (Oxoid Limited, Basingstoke, UK). BA and SDA were used to estimate and identify the culturable fraction of airborne bacteria and fungi, respectively. Both media were prepared according to the manufacturer’s instructions and poured into the RODAC Petri dishes. After solidification, the control strains Escherichia coli ATCC 25922 and Staphylococcus aureus ATCC 25923 were used as controls for BA, as suggested by the manufacturer. Aspergillus brasiliensis ATCC 16404 and Candida albicans ATCC 10231 were used as controls for SDA accordingly.
After air sampling, the RODAC plates were sealed with parafilm and transported to the Institute of Microbiology and Immunology, Faculty of Medicine, University of Ljubljana, Slovenia, where they were incubated at 37 °C for 48 h (BA) and at 20 °C for 7 days (SDA). The plates were checked daily for growth. The colony-forming units (CFU) counted were expressed per volume of air (CFU/m3) according to the equation provided by the manufacturer (VWR International, Radnor, PA, USA). In order to better compare the microbial concentration before and after the speleotherapeutic activities, the A/B index was calculated (after/before, A/B), which indicates how much higher or lower the concentration is after the therapy. Different morphotypes of bacterial colonies from all primary selection agar media were inoculated onto BA and incubated at 37 °C for 24 to 48 h to be subsequently identified by MALDI-TOF MS (Matrix-Assisted Laser Desorption/Ionization Time-Of-Flight Mass Spectrometry). Different fungal morphotypes from all primary selection agar media were inoculated onto Sabouraud dextrose agar supplemented with gentamicin and chloramphenicol (SGC2) (bioMérieux, Marcy-l’Étoile, France) and incubated at 37 °C or 30 °C (depending on their preliminary morphological identification) for 24 to 72 h to be subsequently identified by their morphological characteristics and MALDI-TOF MS.
2.3.2. Microbial Cultivation after Sampling with the Impinger
Cultivation of airborne microorganisms from samples obtained with the Coriolis®µ Cyclonic Air Sampler was performed as previously described [27], but with the addition of mycological media. Briefly, BA (Becton Dickinson, Franklin Lakes, NJ, USA) and SGC2 (bioMérieux, Marcy-l’Étoile, France) agar plates were used to estimate and identify the culturable fraction of airborne bacteria and fungi, respectively. A portion (200 µL) of the liquid samples was evenly distributed on the BA and SGC2 plates, and then the plates were incubated at 37 °C for 48 h and at 20 °C for 7 days, respectively. The colony-forming units (CFU) counted were expressed per volume of air (CFU/m3) according to the equation provided by the manufacturer (Bertin Technologies, Saint Quentin en Yvelines, France). In order to better compare the microbial concentration before and after the speleotherapeutic activities, the A/B index was calculated (after/before, A/B), which indicates how much higher or lower the concentration is after the therapy. Different morphotypes of bacterial colonies from all primary selection agar media were inoculated onto BA and incubated for 24 to 48 h at 37 °C for subsequent identification by MALDI-TOF MS. Different fungal morphotypes from all primary selection agar media were inoculated onto SGC2 and incubated at 37 °C or 30 °C (depending on preliminary morphological identification) for 24 to 72 h to be subsequently identified by their morphological characteristics and MALDI-TOF MS.
2.4. Microbial Identification
The pure microbial isolates on the BA and SGC2 plates were identified using MAL-DI-TOF MS and a formic acid on-spot extraction method, as previously described [27,30]. A 24- to 48-h-old colony was spread on the MALDI steel plate and overlaid with 1 µL of 98% formic acid. After drying, the sample was covered with 1 µL of photoabsorbent saturated α-cyano-4-hydroxycinnamic acid (HCCA) matrix solution in 50% acetonitrile–2.5% trifluoroacetic acid (Bruker Daltonik, Bremen, Germany) and allowed to dry before subsequent analysis with a linear-mode microflex LT/SH MALDI-TOF MS system (Bruker Daltonik). The spectra obtained were analyzed using the MALDI-TOF Biotyper® (MBT) Compact HT software with the Main Spectra Library BDAL v. 2023 for bacteria and yeasts and Filamentous Fungi v. 2023 for molds (Bruker Daltonik). The Bruker bacterial test standard was used for calibration according to the manufacturer’s instructions. The quality of the identification was evaluated using the score from 0 to 3 given by the manufacturer. A score of ≥2.00 indicates reliable identification at the species level; a score of 1.70 to 1.99 indicates reliable identification at the genus level; and a score of <1.70 was interpreted as no identification. In addition to MALDI-TOF MS identification, the filamentous fungi were identified on the basis of their growth and morphological characteristics [31,32].
2.5. Statistical Analysis
Descriptive statistics were used to present the distribution of absolute values of environmental parameters (temperature, relative humidity, wind, and CO2 concentration) and the quantification of airborne microorganisms in the observed cave before and after the speleotherapeutic session. Average values and standard deviations are given for temperature, relative humidity, wind, CO2, and microbial concentration. The influence of patients on the measured variables (microbial concentration and CO2) was determined using the Wilcoxon signed rank test adjusted by the Bonferroni correction. p-values of less than 0.05 were considered statistically significant. Statistical analyses were performed using IBM® SPSS® for Windows version 26 (SPSS Inc., IBM Company, Chicago, IL, USA) and Excel® for Windows® (Microsoft™, Redmond, WA, USA).
3. Results
3.1. Environmental Parameters
Table 1 shows the results for CO2 air concentrations, air temperature, airflow, and relative humidity (RH). The data for these environmental parameters are presented as minimum, maximum, and median values for each of the three sampling sites in the Sežana Hospital Cave. Wind speed (m/s) is presented in more detail in Table S1 along with other environmental parameters: a range between the minimum and maximum values and an arithmetic mean.
The average air temperature was stable during all measurements and ranged between 12.8 °C and 16.5 °C, with an average of 13.9 °C before and 13.8 °C after the speleotherapeutic activities (Table 1 and Table S1). The average CO2 concentrations ranged from 457.3 ppm to 6160.7 ppm and from 846.0 ppm to 2860.4 ppm before and after the speleotherapeutic activities (Table 1). There was always a certain level of airflow in the cave. The airflow can be partially controlled because one door (labeled “entrance/exit” in Figure 1) has an integrated hatch. The airflow in the Sežana Hospital Cave was the strongest on 7 July 2020 at the Telovadnica sampling site after the speleotherapeutic activities, with 0.64 L/s (Table 1 and Table S1). The hatch was partially open during the entire sampling period. In general, the airflow was stronger after speleotherapeutic activities in 66.7% (8/12) of samplings. The RH ranged from 77.4% to 100%, with an average of 90.9% before and 96.1% after the speleotherapeutic activities.
3.2. Quantification and Identification of Culturable Airborne Microorganisms
This study focuses on the cultivation of aerobiota and compares two aerobiological sampling methods, the impinger and the impactor, followed by identification using MALDI-TOF MS. Table 2 and Table 3 show the total concentrations of culturable bacteria and fungi in CFU/m3 and the number of species identified for both air sampling methods before and after the speleotherapeutic activities. In order to better compare the microbial concentration before and after the speleotherapeutic activities, the A/B index was calculated (after/before, A/B), which indicates how much higher or lower the concentration is after the therapy (Table 2 and Table 3).
The highest concentrations of culturable microorganisms were measured at the Telovadnica sampling site with both sampling methods before and after speleotherapeutic activities (Table 2). We detected higher microbial concentrations after the speleotherapeutic activities in 91.7% (11/12) of the cases with the SAS sampler and in 83.3% (10/12) of the cases with the Coriolis sampler (Table 2 and Table 3).
The influence of patients and medical staff on the measured variables (median concentration of microorganisms, CO2, and RH) is shown in Table 4. The differences in microbial concentrations measured with the SAS air sampler in Jedilnica and Spalnica show borderline results in terms of statistical significance (p = 0.068). The same applies to the microbial concentrations in Jedilnica, which were determined with the Coriolis air sampler (Table 4). In the other cases, the influence of cave visitors was not statistically significant (p > 0.05). For the environmental parameters, only the RH in Jedilnica showed borderline results in terms of statistical significance (p = 0.068). A comparison of the results obtained with the SAS and the Coriolis air sampler was not carried out due to technical differences between the two methods.
3.3. Identification of Culturable Airborne Microorganisms
A total of 74 bacterial species from 29 genera and 15 fungal species from seven genera were identified from air samples collected from May 2020 to January 2023 in three sampling sites in the Sežana Hospital Cave (Tables S2–S4). A relatively large number of isolates, 52.3% (1274/2672) from the “before patients” samples and 21.8% (2580/3300) from the “after patients” samples using the SAS air sampler, could not be identified due to low MALDI scores (<1.70) (Table 5). Using the Coriolis air sampler, we were unable to identify 26.2% (1923/7335) of the isolates from the “before patients” samples and 22.6% (3688/16350) from the “after patient” samples (Table 5).
The most common genera from the Firmicutes group (also known as Bacillota) were Bacillus and Staphylococcus, which accounted for up to 24.8% of the isolates per sampling site (Table S5). Genus Staphylococcus was present at all sampling sites (Table S5). In samples taken before speleotherapeutic activities, staphylococci represented 0.9–21.9% of isolates, and after speleotherapeutic activities, they represented 0.7–11.6% of isolates. Using MALDI-TOF MS, we were able to identify 12 different Staphylococcus sp. (Table S5). The highest percentage of Staphylococcus isolates, 21.9%, was detected in the Jedilnica sampling site on 10 January 2023 before the speleotherapeutic activities with the Coriolis air sampler (Table S2). Among the Actinobacteria (also known as Actinomycetota), Micrococcus, Dietzia, and Kocuria were the three most frequently isolated genera, accounting for up to 55.6% of isolates per sample (Table S5). Micrococcus luteus was one of the most abundant bacterial species in all samples, accounting for 31.3–55.6% in the “before patients” samples and 18.1–52.2% in the “after patients” samples (Table S5). Among the Proteobacteria (also known as Pseudomonadota), Acinetobacter, Serratia, and Pseudomonas were the three most frequently isolated genera, accounting for up to 16.3% of isolates per sample (Table S5). The kingdom Fungi was represented by 15 species from the Ascomycota and Basidiomycota (Table S5). We were able to identify 11 mold species and five yeast species. The most frequently encountered ascomycetous species were Penicillium spp., which accounted for up to 42.6% of all isolates per sample (Table S6). Among the opportunistic and allergenic filamentous fungi, Alternaria alternata reached the highest proportion of isolates—30.4%—in the Spalnica sampling site on 7 July 2020 with the Coriolis air sampler before speleotherapeutic activities (Table S3). Among the yeasts, Debaryomyces hansenii (formerly Candida famata) was detected most frequently, with 28.8% of isolates on 7 July 2020 in Telovadnica before the speleotherapeutic activities (Table S4).
3.4. Microbial Indicators of Cave Anthropization
Among the 89 identified bacterial and fungal species (Tables S5 and S6), we identified up to 22 species that are associated with the human microbiota and could serve as indicators of cave anthropization (Table 6). Half of these microorganisms (11/22) belong to the genus Staphylococcus, a known colonizer of human skin [33]. K. rosea, M. luteus, S. capitis, and S. hominis were isolated from all three sampling sites and are considered strong anthropogenic indicators. According to the American Biological Safety Association (https://my.absa.org/Riskgroups (accessed on 8 March 2024)), less than half (8/20) of the bacteria mentioned belong to risk group 2 as they have a limited pathogenic potential. Others (12/20) cause infections so rarely that they were not assigned to a risk group (Table 6). Among the fungi, the ascomycetous yeast Meyerozyma guilliermondii (formerly Candida guilliermondii) was also isolated at all three sampling sites. These yeasts are part of the human skin and gut microbiota but are also found in other environments such as soil, plants, insects, seawater, and processed foods [34]. A similar problem exists with some other bacteria, such as Acinetobacter spp., Enterococcus moraviensis, and Bacillus licheniformis (Table S5), as these bacteria are often associated with environments other than humans, e.g., soil, water, food, and various animals [33,35].
3.5. Outdoor Air
The results for the outdoor air, which were determined with the SAS air sampler, are listed in Table 7. We were able to detect four bacterial and seven fungal species. The most common isolates were Penicillium spp. and Cladosporium spp., with concentrations of up to 28 CFU/m3 per species. The highest microbial concentration was measured on 27 November 2021 with 122 CFU/m3. The identification success rate of isolates varied between 62.2% in May 2020 and 88.2% in January 2023.
4. Discussion
4.1. Environmental Parameters
In the Sežana Hospital Cave, the air temperature ranged between 12.8 °C and 16.5 °C and did not change in the presence of patients and staff. It has already been proven that a stable air temperature is beneficial for patients with chronic respiratory diseases. Cold and hot temperatures have a negative effect and can lead to exacerbation of the disease, especially in COPD patients and children with asthma [36,37,38]. One of the therapeutic advantages of speleotherapeutic caves is precisely the stable low air temperature, which, in combination with high relative humidity, improves mucociliary clearance [15,39]. RH varied between 77.4% and 100%, with the lowest value measured at the Jedilnica sampling site. This is consistent with other studies in which lower RH near the entrance is typical, while RH inside the cave increases [40,41]. As already mentioned, high RH is also one of the positive climate factors in speleotherapy, as low RH is associated with an increase in emergency admissions in asthmatics, according to some studies [15,42]. Therefore, the deeper parts of the Sežana Hospital Cave, the Spalnica and Telovadnica sampling sites, are more suitable for speleotherapeutic activities, as the average RH is 93.3% and 96.9%, respectively [15,39]. At 82.4%, the Jedilnica sampling site has a lower RH than most low-temperature caves, which makes this part of the cave less favorable for speleotherapeutic activities [39,43]. Interestingly, the RH was influenced by the patients and the medical staff, as the RH was higher after the therapies, and the results were even in the statistical borderline range (p = 0.068). CO2 concentrations were also generally higher after speleotherapeutic activities, suggesting an anthropogenic influence on the cave microclimate, although these changes in concentrations were not as obvious as in some studies of show caves [44,45,46] and were also not statistically significant (p = 0.715). The largest increase in CO2 concentration after therapy was found on 27 November 2021 in the Jedilnica sampling site, when it increased threefold, but on the other hand, on 7 July 2020, we even found a decrease in CO2 after therapy at all sampling sites. One of the possible explanations for these differences is the increased artificial ventilation of the cave with a hatch at the alternative entrance. This hatch may serve to increase or decrease the ventilation of the cave. Nevertheless, we did not measure a higher wind speed or flow on 7 July 2020 than on the other sampling dates, so the behavior of the CO2 remains partially unexplained and can possibly be clarified by further investigations of the cave. The use of sensors to continuously monitor air parameters, including gas concentrations, could reduce uncertainty at this point. However, in agreement with other studies [44,45,47], CO2 concentrations indicate a seasonal distribution that is highest in the warmer months of the year.
4.2. Culturable Airborne Microorganisms and Speleotherapeutic Activities
The air in the Sežana Hospital Cave was not yet characterized microbiologically in detail. Similar to the show caves, higher concentrations of culturable airborne microorganisms were usually detected in the human presence. Just as tourist visits increase microbial concentrations in the show caves, speleotherapeutic activities in this therapeutic cave do the same in at least 83.3% (10/12) of the samples taken. Regardless of the method of air sampling, microbial concentrations increased 1.1- to 77.5-fold after speleotherapeutic activities, suggesting an anthropogenic influence, although there was no strong statistical association (p ≥ 0.068). The highest increase in concentration, namely 77.5 times, was measured in Jedilnica on 27 November 2021. On the same day, the highest microbial concentrations of over 3800 CFU/m3 were generally measured. This situation was due to the high concentrations of Acidovorax sp. In Spalnica and Telovadnica, we were able to identify it to genus level using MALDI-TOF MS (MALDI Score < 2.00)), and in Telovadnica, it even accounted for 59.3% of isolates after speleotherapeutic activities. Acidovorax sp. is also found in soil and plants [48] and could be part of the cave microbiota and aerosolized during physical activities. The other explanation lies in the fact that Acidovorax spp. is considered to be the core microbiota of human skin in some studies [49] and is, therefore, a strong anthropogenic indicator, although it has only been detected once with the Coriolis air sampler. As previously described [27], higher microbial concentrations were associated with speleotherapeutic treatments (10–19 people present) but not with the number of people present; e.g., 232 CFU/m3 were detected in Jedilnica on 27 November 2021, when only 10 people were present, and only 214 CFU/m3 in Jedilnica on 2 June 2022, when 19 people were present. A similar trend was previously observed in show caves in Slovenia and Romania, also with similar airborne microbial concentrations [26,27,50]. As we can see, Sežana Hospital Cave follows the pattern of show caves.
4.3. Comparison of Air Sampling Methods
Various methods of air sampling have been described so far, which are used in different environments [51,52]. We have opted for two active air sampling methods that are used both in the microbiological control of the hospital environment and in cave microbiology [26,27,53,54,55]. Speleotherapeutic caves are unique in this respect because they are caves and hospital environments at the same time. In hospitals and in the pharmaceutical industry, similar to cave microbiology, both active and passive air sampling methods are used, but unfortunately, they are not yet standardized [26,50,55,56]. They are roughly described in various national guidelines and in the EU GMP and formalized in ISO 14698-1:2003 [53,54,57]. The choice of method depends primarily on the type of room or the expected level of microbiological cleanliness. Since a low microbial load is expected in speleotherapeutic caves [21,25,58], we did not opt for the settle plate method, as it has a relatively low sensitivity compared to active methods [59,60]. Impingement and impaction air sampling methods are technically very different: they differ in the size and shape of the surface through which the air is pumped (circular for the impactor and square for the impinger), the impactor samples the air directly onto the solid culture medium, and the impinger samples into a physiological solution (or another type of liquid) with which the solid culture medium must be inoculated in the subsequent steps. The differences also lie in the sample volume and the airflow rate. A direct comparison is therefore not possible, although we were able to identify some differences. On average, we obtained higher microbial concentrations with the impinger air sampler than with the impactor sampler, which can possibly be explained by the nine times larger volume of air sampled (4.5 m3 compared to 0.5 m3). At the same time, we were able to detect more microbial species with the SAS air sampler than with the Coriolis sampler. It is possible that a larger air volume used with the SAS air sampler would lead to more comparable results. At this point, it must be emphasized that the two methods are difficult to compare and that air sampling is, to a certain extent, unpredictable and non-reproducible [59,61]. Further research will clarify the suitability of each sampling method for speleotherapeutic caves, but for now, we can only recommend the use of a single air sampling method in a cave for longitudinal studies to facilitate the comparison of results and to establish guidelines for microbiological monitoring of these “natural” parts of hospitals.
4.4. Cave Anthropization
It has been known for some time that human visitation can have a negative impact on the cave environment, for example, by increasing CO2 levels and introducing nutrients and allochthonous microorganisms [26,28,46,62,63,64]. Most research focuses on show caves, especially those exposed to mass tourism, such as Lascaux Cave (France), Nerja Cave (Spain), and Postojna Cave (Slovenia) [27,28,30,62,65]. There are relatively few datasets on the anthropogenic impact on speleotherapeutic caves [23,66]. Almost 13 years ago, Porca et al. made an important contribution to the standardization of the assessment of the anthropogenic impact on the cave ecosystem [67]. In 2018, Bercea et al. expanded and updated the criteria of Porca et al. and defined five categories of anthropogenic impact on caves according to the concentration of bacteria and fungi in the air [26,67]: Class 1: ≤ 50 CFU/m3 (no human impact); Class 2: 50–150 CFU/m3 (alarm signal—regular checks are recommended); Class 3: 150–500 CFU/m3 (regular checks and changes in cave management (e.g., visit schedules, ventilation, etc.) are recommended); Class 4: 500–1000 CFU/m3 (humans already have a strong influence on the cave ecosystem); and Class 5: ≥ 1000 CFU/m3 (irreversible ecological disturbance if high concentrations persist). If we apply this interpretation scheme to our data, we see that we never exceed the Class 5 limit when using the SAS air sampler before speleotherapeutic activities. A strong anthropogenic influence (Class 4) was only observed in Telovadnica on 10 January 2023, while the other results fall into Class 2, where regular monitoring is recommended, with the exception of Telovadnica on 2 June 2022, which falls into Class 3 with 152 CFU/m3. The presence of patients and medical staff leads to an increase in microbial concentrations and thus also to an increase in the class of anthropogenic disturbance: in all cases, after speleotherapeutic activities, we now have Class 3, which recommends regular microbiological monitoring and measures in terms of visiting times, arrangement of ventilation, etc. However, if we look at the results obtained with the Coriolis air sampler, the picture is somewhat different, as we generally found higher microbial concentrations than with the SAS air sampler. In this case, more than 1000 CFU/m3 were detected in Telovadnica on 27 November 2021 (2370 CFU/m3), even before speleotherapeutic activities. On 27 November 2021, after the speleotherapeutic activities, we found an increased microbial load (>1000 CFU/m3) at all sampling sites and, thus, the negative influence of humans on the cave ecosystem. Regardless of the air sampling method, increased microbial concentrations (Class 3) were found after speleotherapeutic activities, which may have a long-term negative impact on the cave ecosystem. However, Bercea et al. and Porca et al. [26,67] recommend regular microbiological monitoring and optimization of visits to the speleotherapeutic cave in terms of frequency, number of people in the group, etc. As the Sežana Hospital Cave is a relatively small cave with low ventilation, the microbial concentration could be reduced by increasing the artificial ventilation through the hatch at the side entrance shortly before and immediately after the speleotherapeutic activities.
4.5. MALDI-TOF MS Identification Success Rate
MALDI-TOF MS has found its place in medical microbiology laboratories, especially in bacteriology, while it is still underestimated in microbial ecology laboratories [68,69]. In recent years, MALDI-TOF MS has also gained visibility in cave microbiology as more and more authors use it for the characterization, especially the identification, of isolated cave microorganisms [27,30,70,71,72]. In general, we were able to identify more isolates in the samples after speleotherapeutic activities than in the samples before speleotherapeutic activities. We were able to identify a maximum of 79.3% of the isolates before the speleotherapeutic activities and 90.9% of the isolates after the speleotherapeutic activities, which is in line with some other studies [50,70]. As we have similarly found in Postojna Cave and Škocjan Caves, Slovenia [27,50], the samples collected after speleotherapeutic activities contain a greater proportion of typical human microbiota, particularly bacteria of the genus Micrococcus and Staphylococcus, which are well represented in the commercially available MALDI-Bruker library. Compared to the results from Postojna and Škocjan caves, where the air was also sampled with the Coriolis air sampler, we were able to identify a higher proportion of isolates: 29.8 percentage points more in the case of the natural background of the cave (73.8% vs. 44.0%) and 10.5 percentage points more after human activities (77.4% vs. 66.9%) [27]. On the one hand, this can be explained by the use of the newer MALDI-Bruker library, which has a broader spectrum of microbial species than in 2018, when we conducted the study in natural show caves [27]. The difference is also reflected in the number of species identified, as we identified 23 more bacterial species in the Sežana Hospital Cave than in the previous study (74 vs. 51) [27]. On the other hand, the better coverage of isolates in the MALDI-Bruker library could indicate a higher degree of anthropization of the Sežana Hospital Cave.
4.6. Culturable Microorganisms and Potential Indicators of Human Impact
Similar to other cave studies, bacteria from the phyla Actinomycetota (formerly Actinobacteria), Bacillota (formerly Firmicutes), and Pseudomonadota (formerly Proteobacteria) were frequently isolated from air samples [50,63,73,74,75,76]. We identified 74 different bacterial species from 29 genera, which is comparable to other culture-based studies [27,77,78]. On the one hand, we have succeeded in identifying more bacterial species than in other caves. Compared to Cueva de Ardales (Spain) and Lascaux Cave (France), we identified 33 and 40 more species in Sežana Hospital Cave, respectively (41 vs. 74 and 34 vs. 74), and in the aforementioned Postojna and Škocjan Caves (Slovenia), we identified 23 more species (74 vs. 51) [27,76,78]. On the other hand, we identified 1.8 times fewer bacterial species than in the Cueva del Tesoro (Spain) (74 vs. 130) [78]. As the different studies use different identification methods, a direct comparison may be difficult. If we lower the Bruker cut-off value for reliable species identification from 2.00 to 1.70, as we did in our earlier study for Postojna and Škocjan Caves [27], we obtain 97 different species, which compares favorably with the show caves Gruta de las Meravillas and Cueva del Tesoro (Spain) with 94 and 130 molecularly identified species, respectively, and with the Postojna and Škocjan Caves if we apply the same MALDI Score cut-off value—84 different species [27,78]. In terms of bacterial diversity, Sežana Hospital Cave is similar to other caves with varying degrees of anthropization [27,76,78].
Anthropogenic indicators have already been described in various studies [30,63,73,78,79]. Anthropogenic indicators are mostly bacterial and fungal species that are closely associated with humans as the typical microbiota of the skin, gastrointestinal tract, and upper respiratory tract [27,79]. In Sežana Hospital Cave, 22 potential indicators of anthropization of the cave were identified. Among the most reliable—part of the human core microbiota [30,33,80] and present at all sampling sites—are M. luteus, S. capitis, S. hominis, and K. rosea among the bacteria and M. guilliermondii among the fungi. According to other studies, S. epidermidis could also be among them [27,30,33]. In addition to the specific species mentioned, most coagulase-negative staphylococci are also important anthropogenic indicators [27,30,33]. Potential indicator microorganisms could also include Acinetobacter spp., Acidovorax spp., Enterococcus moraviensis, and Bacillus licheniformis, but these can also occur in other environments and are therefore not exclusively associated with the presence of humans [81,82,83]. Some of the anthropogenic indicators could also be found among the isolated molds. For example, Penicillium species are frequently found in human environments and nature, but it is hard to pick a particular species as a certain indicator due to their general ubiquity [84,85,86]. To obtain a more comprehensive view of the cave microbiota, we would also need data on microorganisms from cave surfaces that frequently come into contact with humans and those with which humans do not interact.
4.7. Pathogenic Microorganisms in Cave Aerobiota
In most speleotherapeutic caves, aerosolized particles, especially minerals and ions, are studied, while bioaerosols are not given much attention [66,87,88,89,90]. There are limited data on air biocontamination and its impact on the health of patients with chronic and allergic respiratory diseases associated with speleotherapy [23,91]. Exposure to certain types of bacteria and fungi has been shown to be significantly associated with COPB and asthma exacerbations [9,92,93,94,95]. In addition to the infection, the dysbiosis of the lung microbiota is also important, affecting the local immune system, which determines the balance of inflammation and exacerbation of the disease [96,97]. Since exposure to pathogenic or even saprophytic microorganisms can aggravate the health status of patients with chronic respiratory diseases, the microbiological air quality is an important factor, especially in rooms where patients receive inhalation therapies [20,23,98]. The speleotherapeutic cave is part of the hospital and must, therefore, be maintained to ensure patient safety and protect them from healthcare-associated infections. Caves are particularly interesting in this case because their maintenance and cleaning/disinfection are particularly demanding. In this case, microbiological monitoring is extremely important to detect and control infection risks. In our study, commensals and opportunistic pathogens were identified among the microorganisms, but no primary pathogens were isolated from the air samples. Medically interesting isolates all belong either to risk group 2, as they have a limited pathogenic potential, or they do not belong to any risk group, as they do not normally cause infections in the immunocompetent host. Representatives of the genera Alternaria, Aspergillus, Cladosporium, and Penicillium were isolated in the Sežana Hospital Cave, the last two even at all three sampling locations. The above-mentioned molds are one of the most common causes of the development and exacerbation of asthma and rhinitis [99,100]. Aspergillus fumigatus, which we were only able to detect in low concentrations in Jedilnica, is the clinically most important fungal isolate as it can cause a broad spectrum of pathogenic interactions in patients with COPD and asthma, from allergic sensitization and allergic bronchopulmonary aspergillosis to invasive pulmonary aspergillosis [101,102,103]. Fortunately, high humidity near saturation is not favorable for the growth of Aspergillus spp. [86,104]. The absence of Aspergillus spp. in the deeper parts of the Sežana Hospital Cave is beneficial for patients, especially those who are sensitized to Aspergillus spp. In addition to Aspergillus spp., molds of the genera Penicillium and Cladosporium also have a considerable influence on the course of asthma and COPD but cannot cause infections, only hypersensitivity reactions [94,99]. In view of the fact that we isolated relatively high concentrations of Penicillium spp. (≤334 CFU/m3) in the Sežana Hospital Cave, which at times accounted for up to 42.6% of all isolates, we can conclude that a prolonged stay in the cave could have negative effects on the patients [73,105]. A similar species structure and concentration were also found in other speleotherapeutic caves and a spa center [25,91,106]. Here, increased ventilation of the cave and therapies with smaller groups could be recommended, as larger groups are partly responsible for the introduction of microorganisms into the cave [23,50]. Penicillium spp. are frequently found indoors, but for a healthy living environment, their concentration should be lower indoors than outdoors [107,108]. In the Sežana Hospital cave, the exact opposite was the case—we found lower concentrations and fewer species in the outdoor air than in the cave. Harmful mold concentrations in caves have not yet been defined [59]. The cut-off values for indoor areas proposed by the World Health Organization (WHO) and the European Commission’s report on biological particles in indoor environments (EC) may be helpful for interpretation. The WHO recommends <1000 CFU/m3 for indoor areas [109], while the EC recommends <500 CFU/m3 [110]. If we use the WHO recommendation, we see that the microbial concentrations exceed the cut-off value only on 27 November 2021 when sampling with a Coriolis air sampler. If we use the EC cut-off values, we obtain an excessively high microbial load only before the speleotherapeutic activities on 10 January 2023 in Telovadnica. If we take into account the isolated mold species and total concentrations, we find that the aerobiota in the Sežana Hospital Cave is similar to that in show caves and does not pose a risk to immunocompetent individuals [26,27]. One of the main characteristics of speleotherapeutic caves is the non-allergic atmosphere, which is somewhat compromised in the Sežana Hospital Cave by the mold species that can exacerbate COPD and asthma [95,110]. The microclimatic parameters (RH, T, and wind) are suitable for speleotherapy and probably compensate for the slightly poorer microbiological results [15,58]. Adequate artificial ventilation of the cave before and after speleotherapeutic activities, optimization of the number of patients, and time spent in the cave would probably also improve this parameter. Further research is needed to better understand the dynamics of aerobiota and its importance for the health of patients undergoing speleotherapy.
4.8. Limitations
This study originally had an ambitious plan to explore the aerobiota in more detail, but due to the COVID-19 pandemic (2020–2022) and the closure of the cave for speleotherapy during this period, air samples were taken less frequently. This limited our insight into the structure and dynamics of the aerobiota. Therefore, microbiological time-series analyses need to be performed to assess anthropization and ecological disturbance more accurately. Although reproducibility was not the aim of this study, the collection of only one sample per sampling site and air sampler limits the information on microbial concentrations. Three replicates for each sampling period and location and the use of sensors to continuously monitor air parameters, including gas concentrations, could provide us with more accurate results.
Another limitation of this study was the use of culture-based methods to analyze the cave aerobiota. The use of metagenomics-based approaches, such as advanced molecular genetic techniques and high-throughput sequencing technologies, would greatly increase our knowledge of the abundance and diversity of airborne microbes.
As far as the identification of microorganisms is concerned, MALDI-TOF MS alone is not an optimal identification method, especially in environmental microbiology [50,70,71]. A number of methods have been proposed for the optimal identification of microorganisms, each with its own advantages and limitations. In addition to MALDI-TOF MS and genome-based methods, other successful methods range from morphology and gas-liquid chromatography of cellular fatty acids to the use of optical methods for label-free detection of bacteria [68,111,112,113]. Overall, however, these studies emphasize the need for a multi-method approach to microbial identification that combines the strengths of individual methods to achieve optimal results. In addition to species identification, resistance profiles and phylogenetic comparisons could provide more precise information on the anthropogenic origin of the isolated microorganisms.
5. Conclusions
Speleotherapy is one of the non-pharmacological methods for the treatment and rehabilitation of patients with chronic respiratory diseases, especially COPD and asthma. The specific cave environment with constant temperature, high humidity, low ventilation, aerosolized minerals, and low concentrations of microorganisms and radioactivity benefits the rehabilitation of these patients. For successful and safe speleotherapeutic rehabilitation, it is necessary to control the microclimatic parameters, especially the concentration of aerosolized microorganisms, which can have a negative impact on patients. There are little data on microbiological air monitoring in speleotherapeutic caves. The optimal methods for air sampling have not yet been established internationally; due to the expected low microbial load, we recommend the use of volumetric methods. The methods are difficult to compare due to the technical diversity; therefore, we recommend that laboratories decide on one method and apply it consistently. There are no internationally recognized criteria for assessing the air quality in caves. We recommend using the WHO and EC criteria for indoor microbial concentration and the qualitative criteria from the published literature: absence or lowest possible concentrations of opportunistic and allergenic molds, mainly from the genera Aspergillus, Alternaria, Penicillium, and Cladosporium. Our data show that speleotherapeutic caves, similar to show caves, are also exposed to anthropization. By regulating the ventilation of the speleotherapeutic cave and optimizing the number of patients in the group, potentially excessive microbial concentrations are most likely to be successfully reduced. We recommend regular microbiological monitoring, optimization of ventilation, and reducing the number of patients in the groups.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/atmos15050518/s1, Table S1: Environmental parameters: CO2, temperature, wind velocity and flow, relative humidity, and radiation from May 2020 to January 2023 in Jedilnica, Spalnica, and Telovadnica sampling sites in Sežana Hospital Cave before and after speleotherapeutic activities; Table S2: Bacterial and fungal isolates (MALDI Score ≥ 2.00) from the Jedilnica sampling site in Sežana Hospital Cave; Table S3: Bacterial and fungal isolates (MALDI Score ≥ 2.00) from the Spalnica sampling site in Sežana Hospital Cave; Table S4: Bacterial and fungal isolates (MALDI Score ≥ 2.00) from the Telovadnica sampling site in Sežana Hospital Cave; Table S5: Bacterial isolates (MALDI Score ≥ 2.00) from the Jedilnica, Spalnica, and Telovadnica sampling sites in the Sežana Hospital Cave, their risk group assignment, and typical habitat; Table S6: Fungal isolates (MALDI Score ≥ 2.00) from the Jedilnica, Spalnica, and Telovadnica sampling sites in the Sežana Hospital Cave, their risk group assignment, and typical habitat.
Author Contributions
Conceptualization, R.T. and T.M.; methodology, R.T. and J.M.; software, J.M.; validation, R.T. and A.K.; formal analysis, R.T. and A.K.; investigation, R.T. and J.M.; resources, R.T., T.M. and V.Š.; data curation, R.T., J.M. and T.M.; writing—original draft preparation, R.T.; writing—review and editing, T.M., A.K., J.M. and V.Š.; visualization, R.T. and J.M.; supervision, T.M.; project administration, T.M. and V.Š.; funding acquisition, T.M. All authors have read and agreed to the published version of the manuscript.
Funding
The authors acknowledge the financial support from the Slovenian Research Agency (research core funding Nos. P6-0119 and P3-0083).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article or Supplementary Material.
Acknowledgments
We thank Manca Radež, Janja Svoljšak, Tatjana Marinko, and Franjo Drole for logistical and technical support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Labaki, W.W.; Han, M.K. Chronic Respiratory Diseases: A Global View. Lancet Respir. Med. 2020, 8, 531–533. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Mielgo-Ayuso, J.; Ramos-Campo, D.J.; Beltran-Velasco, A.I.; Martínez-Guardado, I.; Navarro Jimenez, E.; Redondo-Flórez, L.; Yáñez-Sepúlveda, R.; Tornero-Aguilera, J.F. Basis of Preventive and Non-Pharmacological Interventions in Asthma. Front. Public Health 2023, 11, 1172391. [Google Scholar] [CrossRef] [PubMed]
- Linneberg, A.; Dam Petersen, K.; Hahn-Pedersen, J.; Hammerby, E.; Serup-Hansen, N.; Boxall, N. Burden of Allergic Respiratory Disease: A Systematic Review. Clin. Mol. Allergy 2016, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Vogelmeier, C.; Roche, N.; Halpin, D.; Cardoso, J.; Chuchalin, A.G.; Kankaanranta, H.; Sandström, T.; Śliwiński, P.; Zatloukal, J. A Review of National Guidelines for Management of COPD in Europe. Eur. Respir. J. 2016, 47, 625–637. [Google Scholar] [CrossRef] [PubMed]
- López-Campos, J.L.; Ruiz-Ramos, M.; Soriano, J.B. Mortality Trends in Chronic Obstructive Pulmonary Disease in Europe, 1994–2010: A Joinpoint Regression Analysis. Lancet Respir. Med. 2014, 2, 54–62. [Google Scholar] [CrossRef] [PubMed]
- ur Rehman, A.; Hassali, M.A.A.; Abbas, S.; Ali, I.A.B.H.; Harun, S.N.; Muneswarao, J.; Hussain, R. Pharmacological and Non-Pharmacological Management of COPD; Limitations and Future Prospects: A Review of Current Literature. J. Public Health 2020, 28, 357–366. [Google Scholar] [CrossRef]
- Tong, S.; Yin, Y.; Bao, Y. Climatotherapy for Asthma: Research Progress and Prospect. Environ. Res. 2022, 214, 113988. [Google Scholar] [CrossRef] [PubMed]
- Lăzărescu, H.; Simionca, I.; Hoteteu, M.; Mirescu, L. Speleotherapy–Modern Bio-Medical Perspectives. J. Med. Life 2014, 7, 76. [Google Scholar]
- Kim, K.-H.; Kabir, E.; Jahan, S.A. Airborne Bioaerosols and Their Impact on Human Health. J. Environ. Sci. 2018, 67, 23–35. [Google Scholar] [CrossRef]
- GSJ, S.; Ramakodi, M.P.; TVBPS, R. Review of Bioaerosols from Different Sources and Their Health Impacts. Environ. Monit. Assess. 2023, 195, 1321. [Google Scholar]
- D’Amato, G.; Vitale, C.; Sanduzzi, A.; Molino, A.; Vatrella, A.; D’Amato, M. Allergenic Pollen and Pollen Allergy in Europe. In Allergy and Allergen Immunotherapy; Apple Academic Press: Palm Bay, FL, USA, 2017; pp. 287–306. [Google Scholar]
- Horvath, T. Speleotherapy: A Special Kind of Climatotherapy, Its Role in Respiratory Rehabilitation. Int. Rehabil. Med. 1986, 8, 90–92. [Google Scholar] [CrossRef]
- Puryshev, E.A. The Efficacy of Speleotherapy in Atopic Dermatitis in Children. Vopr. Kurortol. Fizioter. I Lech. Fiz. Kult. 1994, 4, 34–35. [Google Scholar]
- Munteanu, C.; Munteanu, D.; Simionca, I.; Hoteteu, M. Morphological and Electrophoretic Data about Heterogeneous Primary Skin Cells Cultures Obtained from Normal and Ovalbumin-Challenged Wistar Rats after Treatment by Speleotherapy in the Cacica and Dej Romanian Salt Mines. Balneo-Res. J. 2010, 1. Available online: https://bioclima.ro/J14.pdf (accessed on 8 March 2024). [CrossRef]
- Freidl, J.; Huber, D.; Braunschmid, H.; Romodow, C.; Pichler, C.; Weisböck-Erdheim, R.; Mayr, M.; Hartl, A. Winter Exercise and Speleotherapy for Allergy and Asthma: A Randomized Controlled Clinical Trial. J. Clin. Med. 2020, 9, 3311. [Google Scholar] [CrossRef] [PubMed]
- Munteanu, C. SPELEOTHERAPY-Scientific Relevance in the Last Five Years (2013–2017)–A Systematic Review. Balneo Res. J. 2017, 8, 252–254. [Google Scholar] [CrossRef]
- Eslaminejad, A.; Taghavi, K.; Zohal, M.; Kialashaki, M.; Fakharian, A. Speleotherapy as an Effective Treatment of Chronic Obstructive Pulmonary Disease. J. Respir. Med. Lung Dis. 2017, 2, 1029. [Google Scholar]
- Wasik, A.A.; Tuuminen, T. Salt Therapy as a Complementary Method for the Treatment of Respiratory Tract Diseases, With a Focus on Mold-Related Illness. Altern. Ther. Health Med. 2021, 27, 233. [Google Scholar]
- Beamon, S.P.; Falkenbach, A.; Fainburg, G.; Linde, K.; Group, C.A. Speleotherapy for Asthma. Cochrane Database Syst. Rev. 1996, 2019. [Google Scholar] [CrossRef]
- Hubelova, D.; Ulmann, V.; Mikuska, P.; Licbinsky, R.; Alexa, L.; Modra, H.; Gersl, M.; Babak, V.; Weston, R.T.; Pavlik, I. Nontuberculous Mycobacteria Prevalence in Aerosol and Spiders’ Webs in Karst Caves: Low Risk for Speleotherapy. Microorganisms 2021, 9, 2573. [Google Scholar] [CrossRef]
- Mętel, S.; Kostrzon, M.; Adamiak, J.; Gattner, H.; Kościelecka, D.; Sosulska, A.; Szczygieł, E.; Golec, J. The Influence of Speleotherapy Combined with Pulmonary Rehabilitation on Functional Fitness in Older Adults–Preliminary Report. Ther. Adv. Respir. Dis. 2020, 14, 1753466620926952. [Google Scholar] [CrossRef]
- Kertész, Z.; Borbély-Kiss, I.; Hunyadi, I. Study of Aerosols Collected in a Speleotherapeutic Cave Situated below Budapest, Hungary. Nucl. Instrum. Methods Phys. Res. Sect. B Beam Interact. Mater. At. 1999, 150, 384–391. [Google Scholar] [CrossRef]
- Cristofori, A.; Cristofolini, F.; Gottardini, E. Rare Occurrence of Airborne Bioparticles in a Speleotherapy Site: The Case Study of the Sant’Aloisio Disused Siderite Mine (Brescia, Italy). Aerobiologia 2020, 36, 125–130. [Google Scholar] [CrossRef]
- Iqbal, M.A.; Siddiqua, S.A.; Faruk, M.O.; Islam, A.R.M.T.; Salam, M.A. Systematic Review and Meta-Analysis of the Potential Threats to Respiratory Health from Microbial Bioaerosol Exposures. Environ. Pollut. 2023, 341, 122972. [Google Scholar] [CrossRef]
- Fraczek, K.; Górny, R.L. Microbial Air Quality at Szczawnica Sanatorium, Poland. Ann. Agric. Environ. Med. 2011, 18, 63–71. [Google Scholar]
- Bercea, S.; Năstase-Bucur, R.; Mirea, I.C.; Măntoiu, D.Ş.; Kenesz, M.; Petculescu, A.; Baricz, A.; Andrei, A.-Ş.; Banciu, H.L.; Papp, B. Novel Approach to Microbiological Air Monitoring in Show Caves. Aerobiologia 2018, 34, 445–468. [Google Scholar] [CrossRef]
- Tomazin, R.; Simčič, S.; Stopinšek, S.; Kopitar, A.N.; Kukec, A.; Matos, T.; Mulec, J. Effects of Anthropogenic Disturbance and Seasonal Variation on Aerobiota in Highly Visited Show Caves in Slovenia. Microorganisms 2023, 11, 2381. [Google Scholar] [CrossRef]
- Del Rosal, Y.; Liñán, C.; Hernández-Mariné, M. The Conservation of the Nerja Cave: Preserving Anthropogenic Impact in a Tourist Cave. In The Conservation of Subterranean Cultural Heritage; CRC Press/Balkema: Leide, Germany, 2014; pp. 193–206. [Google Scholar]
- Škerlj, A. Oblikovanje Speleoterapevtskega Parka Pri Bolnišnici Sežana/Designing a Speleotherapy Park by Sežana Hospital. Master’s Thesis, Biotechnical Faculty, University of Ljubljana, Ljubljana, Slovenia, 2015. [Google Scholar]
- Mulec, J.; Skok, S.; Tomazin, R.; Letić, J.; Pliberšek, T.; Stopinšek, S.; Simčič, S. Long-Term Monitoring of Bioaerosols in an Environment without UV and Desiccation Stress, an Example from the Cave Postojnska Jama, Slovenia. Microorganisms 2023, 11, 809. [Google Scholar] [CrossRef]
- Walsh, T.J.; Hayden, R.T.; Larone, D.H. Larone’s Medically Important Fungi: A Guide to Identification; John Wiley & Sons: Hoboken, NJ, USA, 2018; ISBN 1-68367-296-8. [Google Scholar]
- Hoog, G.S. Atlas of Clinical Fungi: The Ultimate Benchtool for Diagnostics; Foundation Atlas of Clinical Fungi: Hilversum, The Netherlands, 2020; ISBN 94-93226-12-3. [Google Scholar]
- Wilson, M. The Human Microbiota in Health and Disease: An Ecological and Community-Based Approach; Garland Science: New York, NY, USA, 2018. [Google Scholar]
- Savini, V.; Catavitello, C.; Onofrillo, D.; Masciarelli, G.; Astolfi, D.; Balbinot, A.; Febbo, F.; D’Amario, C.; D’Antonio, D. What Do We Know about Candida Guilliermondii? A Voyage throughout Past and Current Literature about This Emerging Yeast. Mycoses 2011, 54, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.R.; Rosenthal, K.S.; Pfaller, M.A. Medical Microbiology E-Book; Elsevier Health Sciences: London, UK, 2020; ISBN 0-323-67450-X. [Google Scholar]
- Hansel, N.N.; McCormack, M.C.; Kim, V. The Effects of Air Pollution and Temperature on COPD. COPD J. Chronic Obstr. Pulm. Dis. 2016, 13, 372–379. [Google Scholar] [CrossRef]
- Shoraka, H.R.; Soodejani, M.T.; Abobakri, O.; Khanjani, N. The Relation between Ambient Temperature and Asthma Exacerbation in Children: A Systematic Review. J. Lung Health Dis. 2019, 3, 1–9. [Google Scholar] [CrossRef]
- Hayes Jr, D.; Collins, P.B.; Khosravi, M.; Lin, R.-L.; Lee, L.-Y. Bronchoconstriction Triggered by Breathing Hot Humid Air in Patients with Asthma: Role of Cholinergic Reflex. Am. J. Respir. Crit. Care Med. 2012, 185, 1190–1196. [Google Scholar] [CrossRef] [PubMed]
- Internationales Symposium für Speläotherapie 9, 1987; Trimmel, H. Akten Des 9. Internationalen Symposiums Für Speläotherapie: Bad Bleiberg (Kärnten), September 1987, Verb. Österr. Höhlenforscher. 1992.
- Constantin, S.; Mirea, I.C.; Petculescu, A.; Arghir, R.A.; Măntoiu, D.Ș.; Kenesz, M.; Robu, M.; Moldovan, O.T. Monitoring Human Impact in Show Caves. A Study of Four Romanian Caves. Sustainability 2021, 13, 1619. [Google Scholar] [CrossRef]
- Forbes, J. Air Temperature and Relative Humidity Study: Torgac Cave, New Mexico. J. Caves Karst Stud. 1998, 60, 27–32. [Google Scholar]
- Bodaghkhani, E.; Mahdavian, M.; MacLellan, C.; Farrell, A.; Asghari, S. Effects of Meteorological Factors on Hospitalizations in Adult Patients with Asthma: A Systematic Review. Can. Respir. J. 2019, 2019, 3435103. [Google Scholar] [CrossRef] [PubMed]
- Lunghi, E.; Manenti, R.; Ficetola, G.F. Cave Features, Seasonality and Subterranean Distribution of Non-Obligate Cave Dwellers. PeerJ 2017, 5, e3169. [Google Scholar] [CrossRef] [PubMed]
- Smetanová, I.; Holý, K.; Luhová, Ľ.; Csicsay, K.; Haviarová, D.; Kunáková, L. Seasonal Variation of Radon and CO2 in the Važecká Cave, Slovakia. Nukleonika 2020, 65, 153–157. [Google Scholar] [CrossRef]
- Prelovšek, M.; Šebela, S.; Turk, J. Carbon Dioxide in Postojna Cave (Slovenia): Spatial Distribution, Seasonal Dynamics and Evaluation of Plausible Sources and Sinks. Environ. Earth Sci. 2018, 77, 289. [Google Scholar] [CrossRef]
- Lang, M.; Faimon, J.; Pracný, P.; Kejíková, S. A Show Cave Management: Anthropogenic CO2 in Atmosphere of Výpustek Cave (Moravian Karst, Czech Republic). J. Nat. Conserv. 2017, 35, 40–52. [Google Scholar] [CrossRef]
- Lang, M.; Faimon, J.; Godissart, J.; Ek, C. Carbon Dioxide Seasonality in Dynamically Ventilated Caves: The Role of Advective Fluxes. Theor. Appl. Climatol. 2017, 129, 1355–1372. [Google Scholar] [CrossRef]
- Siani, R.; Stabl, G.; Gutjahr, C.; Schloter, M.; Radl, V. Acidovorax Pan-Genome Reveals Specific Functional Traits for Plant Beneficial and Pathogenic Plant-Associations. Microb. Genom. 2021, 7, 000666. [Google Scholar] [CrossRef]
- Cosseau, C.; Romano-Bertrand, S.; Duplan, H.; Lucas, O.; Ingrassia, I.; Pigasse, C.; Roques, C.; Jumas-Bilak, E. Proteobacteria from the Human Skin Microbiota: Species-Level Diversity and Hypotheses. One Health 2016, 2, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Mulec, J.; Oarga-Mulec, A.; Šturm, S.; Tomazin, R.; Matos, T. Spacio-Temporal Distribution and Tourist Impact on Airborne Bacteria in a Cave (Škocjan Caves, Slovenia). Diversity 2017, 9, 28. [Google Scholar] [CrossRef]
- Lodge, J.P. Methods of Air Sampling and Analysis; Routledge: New York, NY, USA, 2017; ISBN 0-203-74740-2. [Google Scholar]
- Kabir, E.; Azzouz, A.; Raza, N.; Bhardwaj, S.K.; Kim, K.-H.; Tabatabaei, M.; Kukkar, D. Recent Advances in Monitoring, Sampling, and Sensing Techniques for Bioaerosols in the Atmosphere. ACS Sens. 2020, 5, 1254–1267. [Google Scholar] [CrossRef] [PubMed]
- IWC Authority. Linee Guida Sugli Standard Di Sicurezza e Di Igiene Del Lavoro Nel Reparto Operatorio; Istituto Superiore per la Prevenzione e la Sicurezza del Lavoro, Dipartimento Igiene del Lavoro (ISPESL): Rome, Italy, 2009. [Google Scholar]
- Sandle, T. EU GMP Annex 1: Manufacture of Sterile Medicinal Products; European Commission: Brussels, Belgium, 2022. [Google Scholar]
- Tomazin, R.; Matos, T. Mycological Methods for Routine Air Sampling and Interpretation of Results in Operating Theaters. Diagnostics 2024, 14, 288. [Google Scholar] [CrossRef]
- Pasquarella, C.; Vitali, P.; Saccani, E.; Manotti, P.; Boccuni, C.; Ugolotti, M.; Signorelli, C.; Mariotti, F.; Sansebastiano, G.E.; Albertini, R. Microbial Air Monitoring in Operating Theatres: Experience at the University Hospital of Parma. J. Hosp. Infect. 2012, 81, 50–57. [Google Scholar] [CrossRef] [PubMed]
- ISO 14698-1; Cleanrooms and Associated Controlled Environments–Biocontamination Control, Part 1: General Principles and Methods. ISO Standard. International Organization for Standardization: Geneva, Switzerland, 2003.
- Calin, M.R.; Simionca, I.G.; Radulescu, I. Natural Therapeutic Factors Assessment for the Use in Speleotherapeutic Purposes of the Cacica Saline Mine, Romania. Rom. Rep. Phys. 2021, 73, 801. [Google Scholar]
- Chinn, R.Y.; Sehulster, L. Guidelines for Environmental Infection Control in Health-Care Facilities: Recommendations of CDC and Healthcare Infection Control Practices Advisory Committee (HICPAC). Morb. Mortal Wkly. Rep. 2003, 52. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5210a1.htm?fbclid=IwAR2fLaoYktAcxp7Mu9ngotP1FfdrJBBWE9Gtg5nGOjhTDrMIft46un3iQtU (accessed on 8 March 2024).
- Fleischer, M.; Bober-Gheek, B.; Bortkiewicz, O.; Rusiecka-Ziólkowskaa, J. Microbiological Control of Airborne Contamination in Hospitals. Indoor Built Environ. 2006, 15, 53–56. [Google Scholar] [CrossRef]
- Bhatia, L.; Vishwakarma, R. Hospital Indoor Airborne Microflora in Private and Government-Owned Hospitals in Sagar City, India. World J. Med. Sci. 2010, 5, 65–70. [Google Scholar]
- Alonso, L.; Pommier, T.; Kaufmann, B.; Dubost, A.; Chapulliot, D.; Doré, J.; Douady, C.J.; Moënne-Loccoz, Y. Anthropization Level of Lascaux Cave Microbiome Shown by Regional-scale Comparisons of Pristine and Anthropized Caves. Mol. Ecol. 2019, 28, 3383–3394. [Google Scholar] [CrossRef]
- Biagioli, F.; Coleine, C.; Piano, E.; Nicolosi, G.; Poli, A.; Prigione, V.; Zanellati, A.; Varese, C.; Isaia, M.; Selbmann, L. Microbial Diversity and Proxy Species for Human Impact in Italian Karst Caves. Sci. Rep. 2023, 13, 689. [Google Scholar] [CrossRef] [PubMed]
- Mulec, J. Human Impact on Underground Cultural and Natural Heritage Sites, Biological Parameters of Monitoring and Remediation Actions for Insensitive Surfaces: Case of Slovenian Show Caves. J. Nat. Conserv. 2014, 22, 132–141. [Google Scholar] [CrossRef]
- Bontemps, Z.; Alonso, L.; Pommier, T.; Hugoni, M.; Moënne-Loccoz, Y. Microbial Ecology of Tourist Paleolithic Caves. Sci. Total Environ. 2022, 816, 151492. [Google Scholar] [CrossRef] [PubMed]
- Licbinsky, R.; Faimon, J.; Tanda, S.; Hegrova, J.; Goessler, W.; Uberhuberova, J. Changes in the Elemental Composition of Particulate Matter in a Speleotherapeutic Cave. Atmos. Pollut. Res. 2020, 11, 1142–1154. [Google Scholar] [CrossRef]
- Porca, E.; Jurado, V.; Martin-Sanchez, P.M.; Hermosin, B.; Bastian, F.; Alabouvette, C.; Saiz-Jimenez, C. Aerobiology: An Ecological Indicator for Early Detection and Control of Fungal Outbreaks in Caves. Ecol. Indic. 2011, 11, 1594–1598. [Google Scholar] [CrossRef]
- Ashfaq, M.Y.; Da’na, D.A.; Al-Ghouti, M.A. Application of MALDI-TOF MS for Identification of Environmental Bacteria: A Review. J. Environ. Manag. 2022, 305, 114359. [Google Scholar] [CrossRef] [PubMed]
- Rychert, J. Benefits and Limitations of MALDI-TOF Mass Spectrometry for the Identification of Microorganisms. J. Infect. Epidemiol. 2019, 2. [Google Scholar] [CrossRef]
- Mudgil, D.; Paul, D.; Baskar, S.; Baskar, R.; Shouche, Y.S. Cultivable Microbial Diversity in Speleothems Using MALDI-TOF Spectrometry and DNA Sequencing from Krem Soitan, Krem Lawbah, Krem Mawpun, Khasi Hills, Meghalaya, India. Arch. Microbiol. 2022, 204, 495. [Google Scholar] [CrossRef] [PubMed]
- Bielen, A.; Babić, I.; Vuk Surjan, M.; Kazazić, S.; Šimatović, A.; Lajtner, J.; Udiković-Kolić, N.; Mesić, Z.; Hudina, S. Comparison of MALDI-TOF Mass Spectrometry and 16S RDNA Sequencing for Identification of Environmental Bacteria: A Case Study of Cave Mussel-Associated Culturable Microorganisms. Environ. Sci. Pollut. Res. 2024, 31, 21752–21764. [Google Scholar] [CrossRef] [PubMed]
- Kato, N.N.; Arini, G.S.; Silva, R.R.; Bichuette, M.E.; Bitencourt, J.A.P.; Lopes, N.P. The World of Cave Microbiomes: Biodiversity, Ecological Interactions, Chemistry, and the Multi-Omics Integration. J. Braz. Chem. Soc. 2024, 35, e-20230148. [Google Scholar] [CrossRef]
- Jurado, V.; Laiz, L.; Rodriguez-Nava, V.; Boiron, P.; Hermosin, B.; Sanchez-Moral, S.; Saiz-Jimenez, C. Pathogenic and Opportunistic Microorganisms in Caves. Int. J. Speleol. 2010, 39, 2. [Google Scholar] [CrossRef]
- Adetutu, E.M.; Thorpe, K.; Shahsavari, E.; Bourne, S.; Cao, X.; Mazaheri Nezhad Fard, R.; Kirby, G.; Ball, A.S. Bacterial Community Survey of Sediments at Naracoorte Caves, Australia. Int. J. Speleol. 2012, 41, 2. [Google Scholar] [CrossRef]
- Ikner, L.A.; Toomey, R.S.; Nolan, G.; Neilson, J.W.; Pryor, B.M.; Maier, R.M. Culturable Microbial Diversity and the Impact of Tourism in Kartchner Caverns, Arizona. Microb. Ecol. 2007, 53, 30–42. [Google Scholar] [CrossRef]
- Martin-Sanchez, P.M.; Jurado, V.; Porca, E.; Bastian, F.; Lacanette, D.; Alabouvette, C.; Saiz-Jimenez, C. Airborne Microorganisms in Lascaux Cave (France). Int. J. Speleol. 2014, 43, 295–303. [Google Scholar] [CrossRef]
- Yasir, M. Analysis of Bacterial Communities and Characterization of Antimicrobial Strains from Cave Microbiota. Braz. J. Microbiol. 2018, 49, 248–257. [Google Scholar] [CrossRef]
- Dominguez-Moñino, I.; Jurado, V.; Rogerio-Candelera, M.A.; Hermosin, B.; Saiz-Jimenez, C. Airborne Bacteria in Show Caves from Southern Spain. Microb. Cell 2021, 8, 247. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, K.H.; Northup, D.E. Bacteria as Indicators of Human Impact in Caves. In Proceedings of the 17th National Cave and Karst Management Symposium, Albany, NY, USA, 31 October–4 November 2005; The NCKMS Steering Committee: Albany, NY, USA, 2006; pp. 40–47. Available online: https://nckms.org/wp-content/uploads/2018/05/2005_lavoie-bacteria.pdf (accessed on 8 March 2024).
- Kloos, W.E.; Musselwhite, M.S. Distribution and Persistence of Staphylococcus and Micrococcus Species and Other Aerobic Bacteria on Human Skin. Appl. Microbiol. 1975, 30, 381–395. [Google Scholar] [CrossRef]
- Al Atrouni, A.; Joly-Guillou, M.-L.; Hamze, M.; Kempf, M. Reservoirs of Non-Baumannii Acinetobacter Species. Front. Microbiol. 2016, 7, 49. [Google Scholar] [CrossRef]
- Svec, P.; Devriese, L.A.; Sedlácek, I.; Baele, M.; Vancanneyt, M.; Haesebrouck, F.; Swings, J.; Doskar, J. Enterococcus Haemoperoxidus Sp. Nov. and Enterococcus Moraviensis Sp. Nov., Isolated from Water. Int. J. Syst. Evol. Microbiol. 2001, 51, 1567–1574. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.A.; To, E.; Fakhry, S.; Baccigalupi, L.; Ricca, E.; Cutting, S.M. Defining the Natural Habitat of Bacillus Spore-Formers. Res. Microbiol. 2009, 160, 375–379. [Google Scholar] [CrossRef]
- Ropars, J.; Didiot, E.; de La Vega, R.C.R.; Bennetot, B.; Coton, M.; Poirier, E.; Coton, E.; Snirc, A.; Le Prieur, S.; Giraud, T. Domestication of the Emblematic White Cheese-Making Fungus Penicillium Camemberti and Its Diversification into Two Varieties. Curr. Biol. 2020, 30, 4441–4453.e4. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.N.; Verma, P.; Kumar, V.; Sangwan, P.; Mishra, S.; Panjiar, N.; Gupta, V.K.; Saxena, A.K. Biodiversity of the Genus Penicillium in Different Habitats. In New and Future Developments in Microbial Biotechnology and Bioengineering; Elsevier: Amsterdam, The Netherlands, 2018; pp. 3–18. [Google Scholar]
- Poli, A.; Zanellati, A.; Piano, E.; Biagioli, F.; Coleine, C.; Nicolosi, G.; Selbmann, L.; Isaia, M.; Prigione, V.; Varese, G.C. Cultivable Fungal Diversity in Two Karstic Caves in Italy: Under-Investigated Habitats as Source of Putative Novel Taxa. Sci. Rep. 2024, 14, 4164. [Google Scholar] [CrossRef] [PubMed]
- Shah, P. A Review of Salt Therapy as a Complementary Treatment for Enhancing Respiratory Wellness and Skin Ailment. Indian Pract. 2019, 72, 28–32. [Google Scholar]
- Faimon, J.; Ličbinský, R.; Lang, M.; Überhuberová, J.; Hebelka, J. Cave Microclimatology: Diurnal Variations in Aerosol Particle Concentrations. Theor. Appl. Climatol. 2019, 137, 2841–2852. [Google Scholar] [CrossRef]
- LEMKO, O.; LEMKO, I. Haloaerosoltherapy: Mechanisms of Curative Effect and Place in the Respiratory Rehabilitation. Balneo PRM Res. J. 2021, 12, 365–375. [Google Scholar] [CrossRef]
- Tanda, S.; Ličbinský, R.; Hegrová, J.; Faimon, J.; Goessler, W. Arsenic Speciation in Aerosols of a Respiratory Therapeutic Cave: A First Approach to Study Arsenicals in Ultrafine Particles. Sci. Total Environ. 2019, 651, 1839–1848. [Google Scholar] [CrossRef]
- Myszkowska, D.; Kostrzon, M.; Dyga, W.; Kędzierska, J.; Namysł, M.; Stanisz, A.; Zagórska, M.; Ziemianin, M.; Obtułowicz, K.; Czarnobilska, E. Bioaerosol of Salt Chambers in the ‘Wieliczka’Salt Mine, Poland. Aerobiologia 2019, 35, 297–311. [Google Scholar] [CrossRef]
- Ferri, S.; Crimi, C.; Campisi, R.; Cacopardo, G.; Paoletti, G.; Puggioni, F.; Crimi, N.; Heffler, E. Impact of Asthma on Bronchiectasis Severity and Risk of Exacerbations. J. Asthma 2022, 59, 469–475. [Google Scholar] [CrossRef]
- Viniol, C.; Vogelmeier, C.F. Exacerbations of COPD. Eur. Respir. Rev. 2018, 27, 170103. [Google Scholar] [CrossRef]
- Tiew, P.Y.; San Ko, F.W.; Pang, S.L.; Matta, S.A.; Sio, Y.Y.; Poh, M.E.; Lau, K.J.; Mac Aogáin, M.; Jaggi, T.K.; Ivan, F.X. Environmental Fungal Sensitisation Associates with Poorer Clinical Outcomes in COPD. Eur. Respir. J. 2020, 56, 2000418. [Google Scholar] [CrossRef]
- Tiwary, M.; Samarasinghe, A.E. Initiation and Pathogenesis of Severe Asthma with Fungal Sensitization. Cells 2021, 10, 913. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.D.; Genco, C.A. Microbiota, Immune Subversion, and Chronic Inflammation. Front. Immunol. 2017, 8, 255. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Ran, Z.; Wang, F.; Xin, C.; Xiong, B.; Song, Z. Role of Pulmonary Microorganisms in the Development of Chronic Obstructive Pulmonary Disease. Crit. Rev. Microbiol. 2021, 47, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Górny, R.L.; Frączek, K.; Ropek, D.R. Size Distribution of Microbial Aerosols in Overground and Subterranean Treatment Chambers at Health Resorts. J. Environ. Health Sci. Eng. 2020, 18, 1437–1450. [Google Scholar] [CrossRef] [PubMed]
- Murrison, L.B.; Brandt, E.B.; Myers, J.B.; Hershey, G.K.K. Environmental Exposures and Mechanisms in Allergy and Asthma Development. J. Clin. Investig. 2019, 129, 1504–1515. [Google Scholar] [CrossRef] [PubMed]
- Jusufovic, E. Molds as a Cause of Asthma and Exacerbations. J. Lung Pulm. Respir. Res. 2022, 9, 94–98. [Google Scholar] [CrossRef]
- Hammond, E.E.; McDonald, C.S.; Vestbo, J.; Denning, D.W. The Global Impact of Aspergillus Infection on COPD. BMC Pulm. Med. 2020, 20, 241. [Google Scholar] [CrossRef]
- Knutsen, A.P. Allergic Bronchopulmonary Aspergillosis in Asthma. Expert Rev. Clin. Immunol. 2017, 13, 11–14. [Google Scholar] [CrossRef]
- Knutsen, A.P. Allergic Aspects of Aspergillosis. Curr. Fungal Infect. Rep. 2013, 7, 334–344. [Google Scholar] [CrossRef]
- Kozlova, E.V.; Mazina, S.E. Biodiversity of Fungi in the Photic and Aphotic Zones of Montenegro Caves. Aerobiologia 2020, 36, 589–604. [Google Scholar] [CrossRef]
- Dominguez-Moñino, I.; Jurado, V.; Rogerio-Candelera, M.A.; Hermosin, B.; Saiz-Jimenez, C. Airborne Fungi in Show Caves from Southern Spain. Appl. Sci. 2021, 11, 5027. [Google Scholar] [CrossRef]
- Frączek, K.; Górny, R.L.; Ropek, D. Bioaerosols of Subterraneotherapy Chambers at Salt Mine Health Resort. Aerobiologia 2013, 29, 481–493. [Google Scholar] [CrossRef]
- Reboux, G.; Rocchi, S.; Vacheyrou, M.; Millon, L. Identifying Indoor Air Penicillium Species: A Challenge for Allergic Patients. J. Med. Microbiol. 2019, 68, 812–821. [Google Scholar] [CrossRef]
- Méheust, D.; Le Cann, P.; Reboux, G.; Millon, L.; Gangneux, J.-P. Indoor Fungal Contamination: Health Risks and Measurement Methods in Hospitals, Homes and Workplaces. Crit. Rev. Microbiol. 2014, 40, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Hänninen, O.O. WHO Guidelines for Indoor Air Quality: Dampness and Mold. In Fundamentals of Mold Growth in Indoor Environments and Strategies for Healthy Living; Wageningen Academic: Wageningen, The Netherlands, 2011; pp. 277–302. [Google Scholar]
- Wanner, H.; Verhoeff, A.; Colombi, A.; Flannigan, B.; Gravesen, S.; Mouilleseaux, A.; Nevalainen, A.; Papadakis, J.; Seidel, K. Indoor Air Quality and Its Impact on Man: Report No. 12: Biological Particles in Indoor Environments; Brussels-Luxembourg: ECSC-EEC-EAEC; Publications Office of the European Union: Luxembourg, 1993. [Google Scholar]
- Wilkendorf, L.S.; Bowles, E.; Buil, J.B.; van der Lee, H.A.; Posteraro, B.; Sanguinetti, M.; Verweij, P.E. Update on Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry Identification of Filamentous Fungi. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Sun, H.; Yang, W.; Fang, Y. Optical Methods for Label-Free Detection of Bacteria. Biosensors 2022, 12, 1171. [Google Scholar] [CrossRef] [PubMed]
- Eerola, E.; Lehtonen, O.-P. Optimal Data Processing Procedure for Automatic Bacterial Identification by Gas-Liquid Chromatography of Cellular Fatty Acids. J. Clin. Microbiol. 1988, 26, 1745–1753. [Google Scholar] [CrossRef]
Figure 1.
Sampling sites are in Sežana Hospital Cave. The floor plan is adapted from the register of the Karst Research Institute, the Research Center of the Slovenian Academy of Sciences and Arts.
Figure 1.
Sampling sites are in Sežana Hospital Cave. The floor plan is adapted from the register of the Karst Research Institute, the Research Center of the Slovenian Academy of Sciences and Arts.


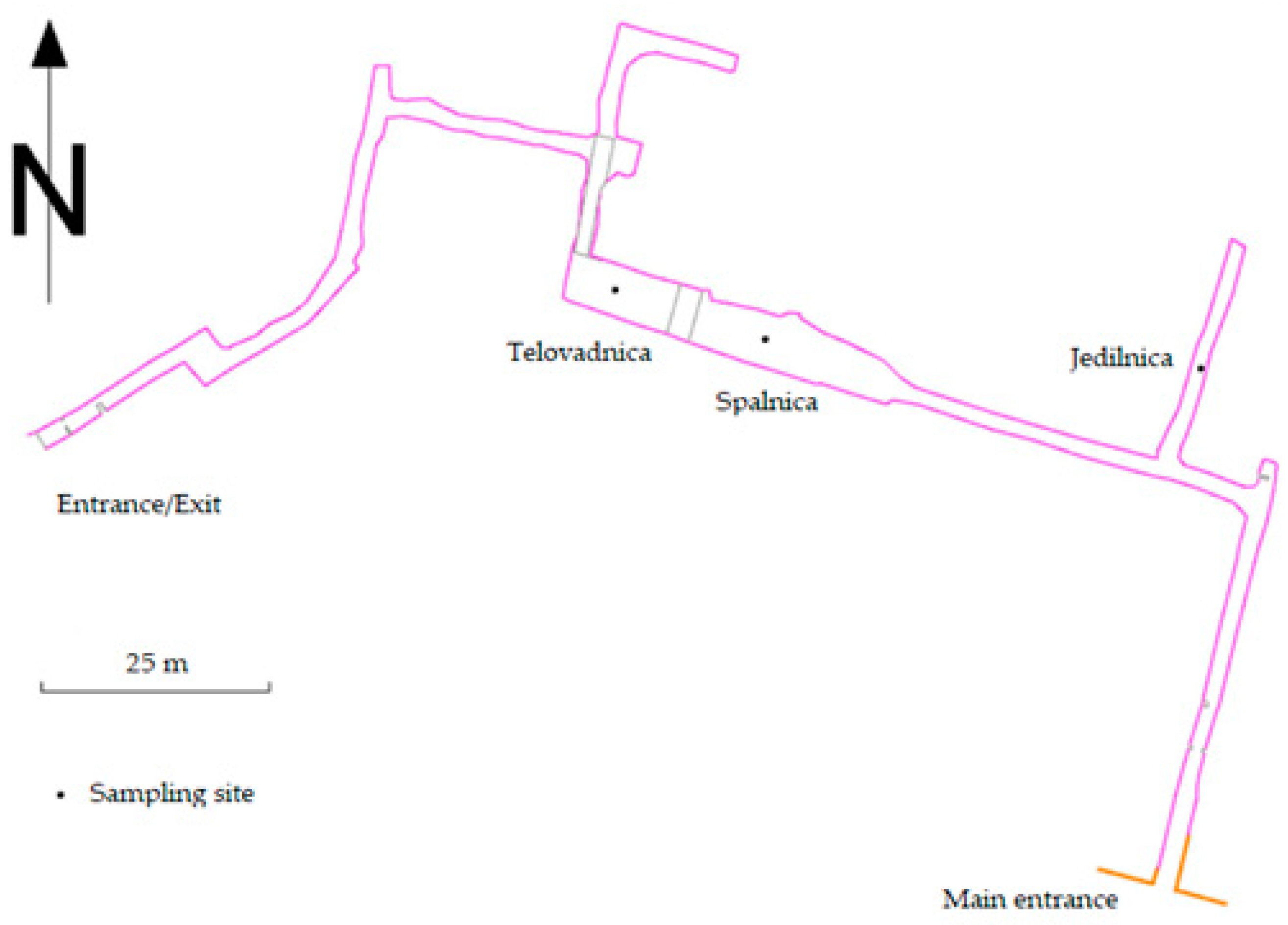{kind=link}
Table 1.
Environmental parameters: Air CO2 concentration, temperature, airflow, and relative humidity from May 2020 to January 2023 at the Jedilnica, Spalnica, and Telovadnica sampling sites in the Sežana Hospital Cave before and after speleotherapeutic activities.
Table 1.
Environmental parameters: Air CO2 concentration, temperature, airflow, and relative humidity from May 2020 to January 2023 at the Jedilnica, Spalnica, and Telovadnica sampling sites in the Sežana Hospital Cave before and after speleotherapeutic activities.
| Location | Before Therapeutic Activities | After Therapeutic Activities | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T (°C) | CO2 (ppm) | RH (%) | Airflow (L/s) | T (°C) | CO2 (ppm) | RH (%) | Airflow (L/s) | ||
| Jedilnica | Mean | 15.0 | 1694.6 | 82.4 | 0.14 | 14.1 | 1528.3 | 93.7 | 0.20 |
| Minimum | 14.2 | 489.0 | 77.4 | 0.07 | 13.2 | 846.0 | 78.8 | 0.09 | |
| Maximum | 16.5 | 4757.9 | 84.6 | 0.21 | 16.2 | 2687.8 | 100.0 | 0.34 | |
| Standard deviation | 1.0 | 2048.4 | 3.4 | 0.06 | 1.4 | 810.1 | 10.1 | 0.10 | |
| Spalnica | Mean | 13.4 | 2112.8 | 93.3 | 0.17 | 13.8 | 1480.1 | 95.1 | 0.22 |
| Minimum | 13.0 | 457.3 | 90.6 | 0.09 | 13.1 | 939.0 | 88.7 | 0.00 | |
| Maximum | 14.1 | 6092.6 | 95.6 | 0.24 | 14.9 | 2121.6 | 100.0 | 0.52 | |
| Standard deviation | 0.5 | 2680.9 | 2.1 | 0.06 | 0.8 | 486.7 | 5.0 | 0.22 | |
| Telovadnica | Mean | 13.2 | 2219.8 | 96.9 | 0.16 | 13.4 | 1886.8 | 99.4 | 0.37 |
| Minimum | 12.8 | 508.0 | 93.4 | 0.01 | 13.0 | 1003.8 | 97.8 | 0.22 | |
| Maximum | 13.7 | 6160.7 | 99.4 | 0.41 | 13.9 | 2860.4 | 100.0 | 0.64 | |
| Standard deviation | 0.4 | 2673.7 | 2.5 | 0.18 | 0.4 | 792.6 | 1.1 | 0.19 | |
Table 2.
Microbial concentrations (CFU/m3) and number of identified species before and after speleotherapeutic activities in the air samples collected by impactors from the Jedilnica, Spalnica, and Telovadnica sampling sites in the Sežana Hospital Cave from May 2020 to January 2023. The A/B index (after/before speleotherapeutic activities, A/B) shows the changes in concentration and number of species between samples taken after and before speleotherapeutic activities.
Table 2.
Microbial concentrations (CFU/m3) and number of identified species before and after speleotherapeutic activities in the air samples collected by impactors from the Jedilnica, Spalnica, and Telovadnica sampling sites in the Sežana Hospital Cave from May 2020 to January 2023. The A/B index (after/before speleotherapeutic activities, A/B) shows the changes in concentration and number of species between samples taken after and before speleotherapeutic activities.
| SAS Duo Air Sampler | ||||||||
|---|---|---|---|---|---|---|---|---|
| Location | Date | Microbes—Before Patients (CFU/m3) | Microbes—After Patients (CFU/m3) | A/B Index—Microbial Load | No. of Microbial Species—Before Patients | No. of Microbial Species—After Patients | A/B Index—Species | No. of Patients and Staff |
| Jedilnica | 7 July 2020 | 102 | 354 | 3.5 | 10 | 10 | 1.1 | 15 |
| 27 November 2021 | 112 | 232 | 2.1 | 5 | 5 | 1.0 | 10 | |
| 2 June 2022 | 106 | 214 | 2.0 | 9 | 9 | 1.1 | 19 | |
| 10 January 2023 | 88 | 610 | 6.9 | 10 | 10 | 1.1 | 15 | |
| 10.2 * | 182.6 * | |||||||
| Spalnica | 7 July 2020 | 144 | 163 | 1.1 | 7 | 7 | 0.8 | 15 |
| 27 November 2021 | 143 | 185 | 1.3 | 4 | 4 | 1.3 | 10 | |
| 2 June 2022 | 64 | 218 | 3.4 | 7 | 7 | 0.6 | 19 | |
| 10 January 2023 | 54 | 138 | 2.6 | 8 | 8 | 1.1 | 15 | |
| 48.9 * | 33.9 * | |||||||
| Telovadnica | 7 July 2020 | 169 | 198 | 1.2 | 8 | 8 | 0.8 | 15 |
| 27 November 2021 | 202 | 148 | 0.7 | 3 | 3 | 0.6 | 10 | |
| 2 June 2022 | 152 | 190 | 1.3 | 11 | 11 | 1.4 | 19 | |
| 10 January 2023 | 96 | 650 | 6.8 | 7 | 7 | 0.9 | 15 | |
| 44.3 * | 236.7 * | |||||||
* Standard deviation.
Table 3.
Microbial concentrations (CFU/m3) and number of identified species before and after speleotherapeutic activities in the air samples collected by impinger from the Jedilnica. Spalnica and Telovadnica sampling sites in the Sežana Hospital Cave from May 2020 to January 2023. The A/B index (after/before speleotherapeutic activities, A/B) shows the changes in concentration and number of species between samples taken after and before speleotherapeutic activities.
Table 3.
Microbial concentrations (CFU/m3) and number of identified species before and after speleotherapeutic activities in the air samples collected by impinger from the Jedilnica. Spalnica and Telovadnica sampling sites in the Sežana Hospital Cave from May 2020 to January 2023. The A/B index (after/before speleotherapeutic activities, A/B) shows the changes in concentration and number of species between samples taken after and before speleotherapeutic activities.
| Coriolis Air Sampler | ||||||||
|---|---|---|---|---|---|---|---|---|
| Microbes—Before Patients (CFU/m3) | Microbes—After Patients (CFU/m3) | A/B Index—Microbial Load | No. of Microbial Species—Before Patients | No. of Microbial Species—After Patients | A/B Index—Species | No. of Patients and Staff | ||
| Jedilnica | 7 July 2020 | 134 | 757 | 5.6 | 4 | 7 | 1.8 | 15 |
| 27 November 2021 | 50 | 3873 | 77.5 | 1 | 4 | 4.0 | 10 | |
| 2 June 2022 | 653 | 886 | 1.4 | 5 | 9 | 1.8 | 19 | |
| 10 January 2023 | 151 | 784 | 5.2 | 4 | 10 | 2.5 | 15 | |
| 274.2 * | 1533.0 * | |||||||
| Spalnica | 7 July 2020 | 217 | 518 | 2.4 | 5 | 3 | 0.6 | 15 |
| 27 November 2021 | 185 | 1820 | 9.8 | 3 | 4 | 1.3 | 10 | |
| 2 June 2022 | 818 | 435 | 0.5 | 8 | 7 | 0.9 | 19 | |
| 10 January 2023 | 304 | 951 | 3.1 | 8 | 5 | 0.6 | 15 | |
| 295.6 * | 634.4 * | |||||||
| Telovadnica | 7 July 2020 | 117 | 469 | 4.0 | 2 | 7 | 3.5 | 15 |
| 27 November 2021 | 2370 | 4558 | 1.9 | 2 | 4 | 2.0 | 10 | |
| 2 June 2022 | 501 | 301 | 0.6 | 5 | 5 | 1.0 | 19 | |
| 10 January 2023 | 317 | 934 | 2.9 | 5 | 6 | 1.2 | 15 | |
| 1041.0 * | 2012.9 * | |||||||
* Standard deviation.
Table 4.
The influence of patients and hospital staff on measured variables (median concentration of microorganisms, CO2, and percentage of relative humidity, RH) in air samples from 2020 to 2023 in Jedilnica, Spalnica, and Telovadnica sampling sites in the Sežana Hospital Cave. Air was sampled simultaneously by the impactor and impinge methods.
Table 4.
The influence of patients and hospital staff on measured variables (median concentration of microorganisms, CO2, and percentage of relative humidity, RH) in air samples from 2020 to 2023 in Jedilnica, Spalnica, and Telovadnica sampling sites in the Sežana Hospital Cave. Air was sampled simultaneously by the impactor and impinge methods.
| Location | SAS Impactor (CFU/m3) | p | Coriolis Impinger (CFU/m3) | p | CO2 (ppm) | p | RH (%) | p | |
|---|---|---|---|---|---|---|---|---|---|
| Jedilnica | Before therapeutic activities | 104.0 | 0.068 | 142.5 | 0.068 | 765.8 | 0.715 | 83.8 | 0.068 |
| After therapeutic activities | 293.0 | 835.0 | 1289.7 | 97.9 | |||||
| Spalnica | Before therapaeutic activities | 103.5 | 0.068 | 260.5 | 0.273 | 950.60 | 0.715 | 93.5 | 0.465 |
| After therapeutic activities | 174.0 | 734.5 | 1429.9 | 95.9 | |||||
| Telovadnica | Before therapeutic activities | 160.5 | 0.465 | 409.0 | 0.144 | 1105.3 | 0.715 | 97.3 | 0.066 |
Table 5.
Number and percentage of microbial isolates identified (MALDI score ≥ 1.70, genus level identification) per sampling site (Jedilnica, Spalnica, and Telovadnica) and comparison between different sampling methods.
Table 5.
Number and percentage of microbial isolates identified (MALDI score ≥ 1.70, genus level identification) per sampling site (Jedilnica, Spalnica, and Telovadnica) and comparison between different sampling methods.
| Jedilnica | Spalnica | Telovadnica | Locations Combined | ||||||
|---|---|---|---|---|---|---|---|---|---|
| SAS | Coriolis | SAS | Coriolis | SAS | Coriolis | SAS | Coriolis | ||
| Non-identified microorganisms (CFU/m3) | Before patients | 412 | 550 | 514 | 622 | 472 | 751 | 1398 | 1923 |
| After patients | 288 | 2621 | 217 | 500 | 215 | 567 | 720 | 3688 | |
| All isolated microorganisms (CFU/m3) | Before patients | 850 | 1672 | 869 | 2041 | 953 | 3622 | 2672 | 7335 |
| After patients | 1410 | 6300 | 704 | 3743 | 1186 | 6262 | 3300 | 16,305 | |
| % of identified microorganisms | Before patients | 51.5 | 67.1 | 40.9 | 69.5 | 50.5 | 79.3 | 47.7 | 73.8 |
| After patients | 79.6 | 58.4 | 69.2 | 86.6 | 81.9 | 90.9 | 78.2 | 77.4 | |
SAS—VWR® SAS Super DUO 360 Air Sampler (VWR International, Radnor, PA, USA); Coriolis—Coriolis®µ Cyclonic Air Sampler (Bertin Technologies, Saint Quentin en Yvelines, France).
Table 6.
Potential microbial indicators of cave anthropization (MALDI-TOF MS score value > 2.00, species level identification).
Table 6.
Potential microbial indicators of cave anthropization (MALDI-TOF MS score value > 2.00, species level identification).
| Microorganisms | Sampling Sites * | Risk Group (Country) | Human Microbiota |
|---|---|---|---|
| Bacteria | |||
| Aerococcus viridans | 1, 2 | 2 (BE, CH, DE) | skin, urinary tract |
| Corynebacterium amycolatum | 1 | 2 (CH, DE) | skin |
| Corynebacterium aurimucosum | 1, 3 | - | skin, vaginal mucosa |
| Kocuria marina | 1, 2 | - | skin |
| Kocuria palustris | 1, 2 | - | skin |
| Kocuria rhizophila | 2 | - | skin |
| Kocuria rosea | 1, 2, 3 | - | skin |
| Micrococcus luteus | 1, 2, 3 | 2 (BE, CH, DE, NIH) | skin |
| Rothia dentocariosa | 1 | - | oral mucosa |
| Staphylococcus capitis | 1, 2, 3 | - | skin, scalp |
| Staphylococcus cohnii | 1, 3 | - | skin |
| Staphylococcus epidermidis | 1, 2 | 2 (BE, CH, DE) | skin, nasopharynx |
| Staphylococcus haemolyticus | 2, 3 | 2 (CH, DE) | skin |
| Staphylococcus hominis | 1, 2, 3 | - | skin |
| Staphylococcus lugdunensis | 1, 2 | 2 (BE, CH, DE) | skin |
| Staphylococcus pettenkoferi | 1 | - | skin, urinary tract |
| Staphylococcus petrasii | 1 | - | skin |
| Staphylococcus saprophyticus | 2 | 2 (BE, CA, CH, DE) | skin |
| Staphylococcus schleiferi | 1 | 2 (BE, CH, DE) | skin |
| Staphylococcus warneri | 1, 2 | - | skin |
| Fungi | |||
| Cutaneotrichosporon dermatis | 2, 3 | - | skin |
| Meyerozyma guilliermondii | 1, 2, 3 | 2 (EU, UK) | skin, intestinal tract |
BE—Belgium; CA—Canada; CH—Switzerland; DE—Germany; EU—European Union; UK—United Kingdom. * 1: Jedilnica sampling site; 2: Spalnica sampling site; 3: Telovadnica sampling site.
Table 7.
Bacterial and fungal isolates (MALDI Score ≥ 2) were obtained from the outdoor air samples from May 2020 to January 2023.
Table 7.
Bacterial and fungal isolates (MALDI Score ≥ 2) were obtained from the outdoor air samples from May 2020 to January 2023.
| Microbial Concentration (CFU/m3) | |||||
|---|---|---|---|---|---|
| Bacteria | 29 May 2020 | 7 July 2020 | 27 November 2021 | 2 June 2022 | 10 January 2023 |
| Arthrobacter parietis | NP | NP | 4 | NP | 2 |
| Bacillus pumilus | NP | NP | 4 | NP | 6 |
| Pantoea eucrina | NP | 2 | NP | NP | 4 |
| Paenarthrobacter ilicis | NP | NP | 4 | NP | NP |
| Fungi | NP | NP | NP | NP | NP |
| Aspergillus fumigatus * | 4 | 2 | 4 | 2 | 4 |
| Aspergillus flavus * | NP | 2 | NP | 2 | 4 |
| Aspergillus glaucus * | NP | NP | 8 | NP | 12 |
| Cladosporium * sp. | 20 | 20 | 28 | 26 | 24 |
| Penicillium brevicompactum * | 2 | 4 | 6 | 4 | 8 |
| Penicillium italicum * | 4 | 2 | 8 | 4 | 8 |
| Penicillium * sp. | 16 | 20 | 22 | 20 | 18 |
| Total microorganisms | 74 | 72 | 122 | 88 | 102 |
| Non-identified microorganisms | 28 | 20 | 26 | 30 | 12 |
| % of identified microorganisms | 62.2 | 72.2 | 78.7 | 65.9 | 88.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tomazin, R.; Kukec, A.; Švigelj, V.; Mulec, J.; Matos, T. Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia. Atmosphere 2024, 15, 518. https://doi.org/10.3390/atmos15050518
AMA Style
Tomazin R, Kukec A, Švigelj V, Mulec J, Matos T. Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia. Atmosphere. 2024; 15(5):518. https://doi.org/10.3390/atmos15050518
Chicago/Turabian StyleTomazin, Rok, Andreja Kukec, Viktor Švigelj, Janez Mulec, and Tadeja Matos. 2024. "Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia" Atmosphere 15, no. 5: 518. https://doi.org/10.3390/atmos15050518
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.