
Analysis of Regional Medical Supply and Demand Network Characteristics Based on “Patient Flow Phenomenon”: A Case Study of the Core Area of the Wuhan Metropolitan Area


Abstract
1. Introduction
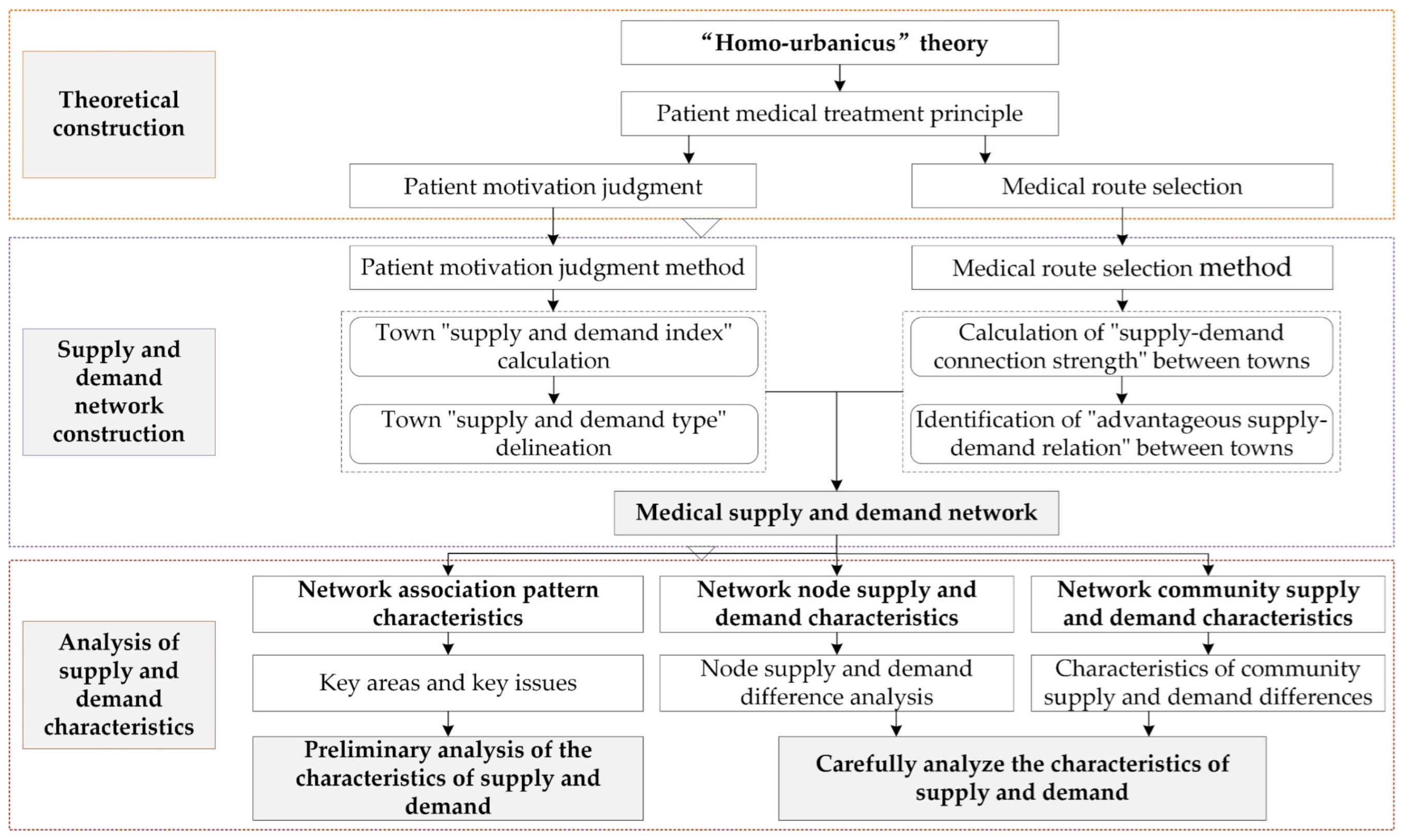
2. Theoretical Construction
2.1. Theoretical Basis
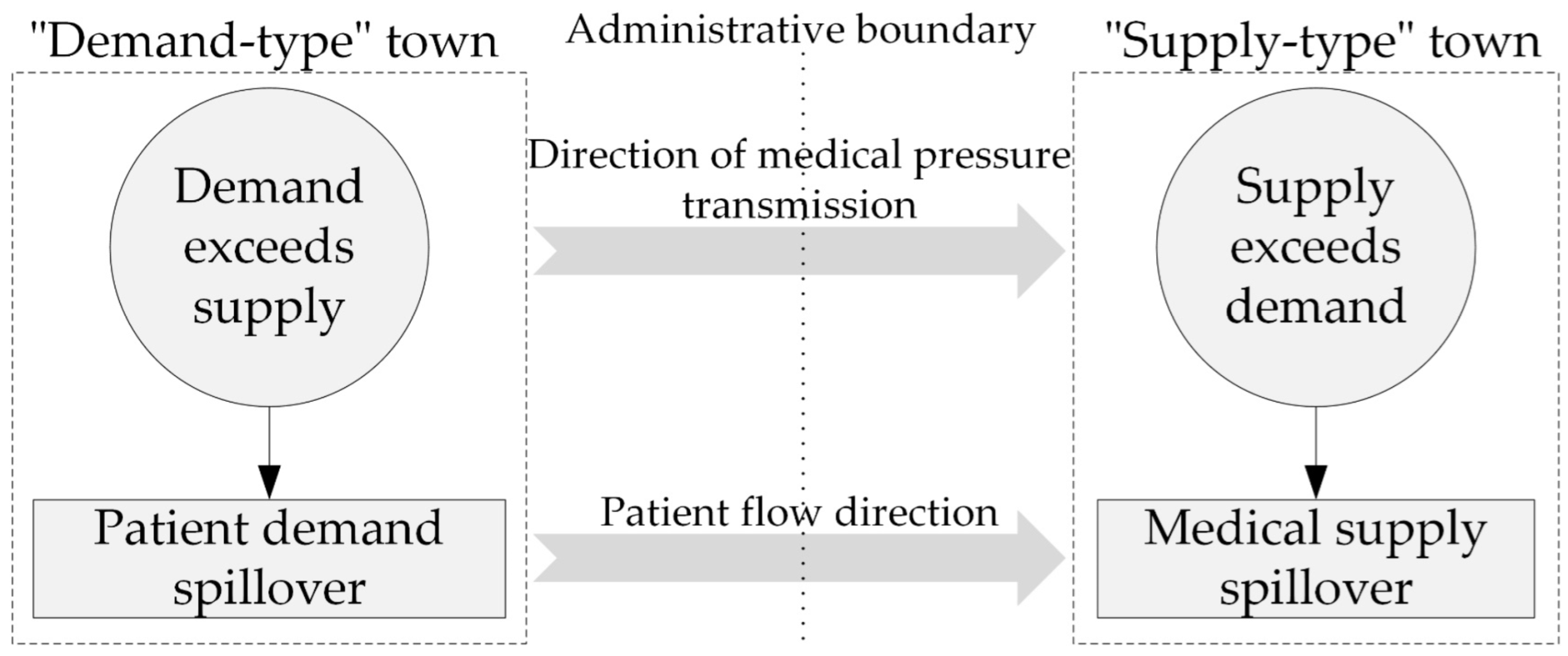
2.2. Patient Medical Treatment Principle
2.2.1. Patient Motivation Judgment
2.2.2. Medical Route Selection
- (1)
- Forming Potential Healthcare Connections:
- (2)
- Rationalizing Healthcare Connection Choices:
- (1)
- The demand ratio advantage criterion is focused on ‘self-existence’, where patients are inclined to opt for destinations within their existing healthcare connections that have a higher intensity. This reflects patients’ expectations of maximizing access to healthcare resources.
- (2)
- The supply ratio advantage criterion is centered on ‘coexistence,’ wherein patients prefer to avoid destinations that establish stronger connections with other ‘demand-type’ towns in the region, thus circumventing medical congestion. This reflects patients’ judgment of the overall competitive relationship in the region and their hope to maintain a reasonable competitive relationship with other patients.
3. Materials and Methods
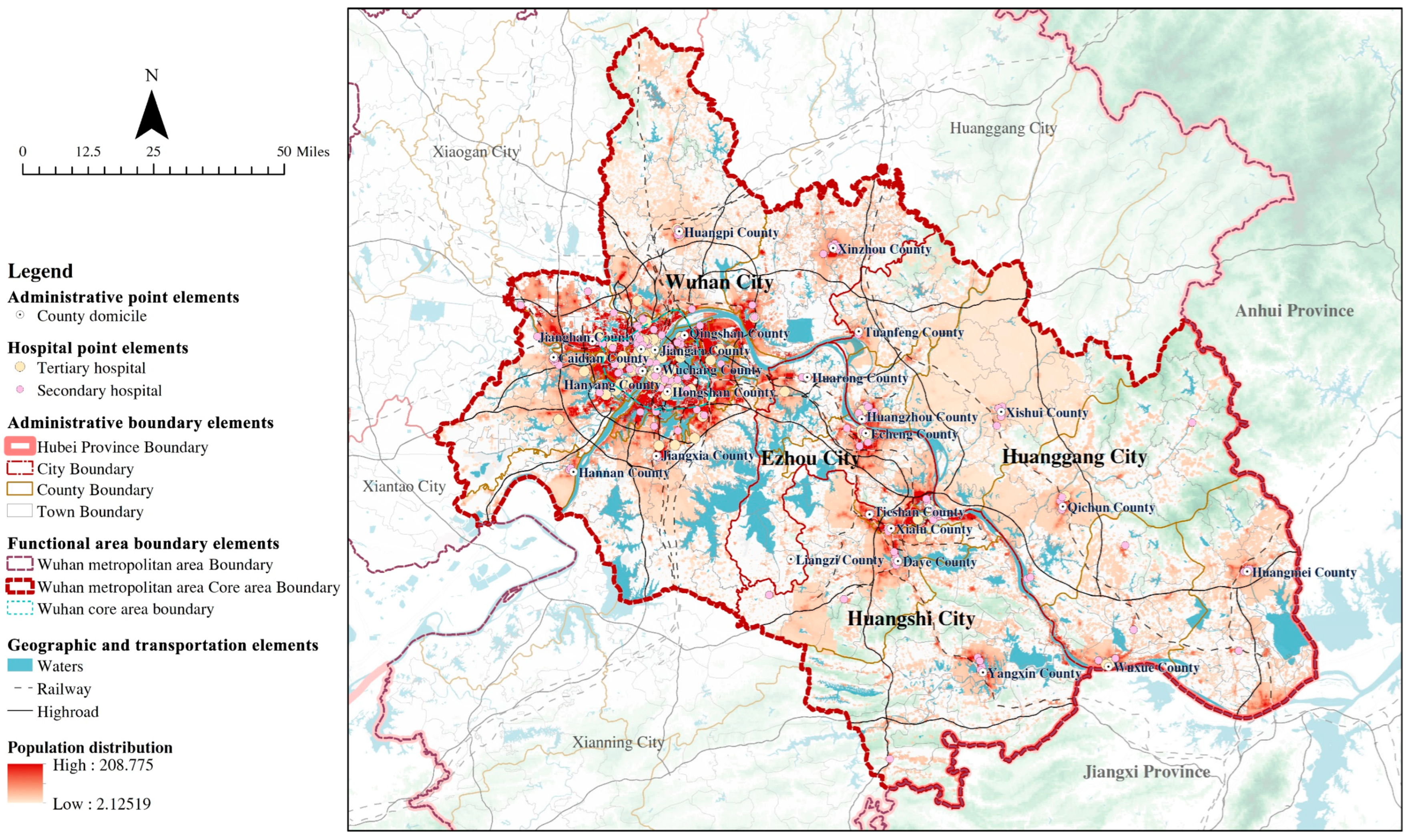
3.1. Study Area and Base Units
3.1.1. Study Area
3.1.2. Base Unit Determination
3.2. Data Source
- (1)
- Demand data:
- (2)
- Supply data:
- (3)
- Commuting data:
3.3. Methods
3.3.1. Supply and Demand Network Construction
- (1)
- Patient motivation judgment
- Fundamental analysis: Town “supply and demand index” calculation
- Motivation judgment: Town “supply and demand type” delineation
- (2)
- Medical route selection method
- Forming Potential Healthcare Connections: Calculation of “supply-demand connection strength” between towns
- Rationalizing Healthcare Connection Choices: Identification of “advantageous supply-demand relation” between towns
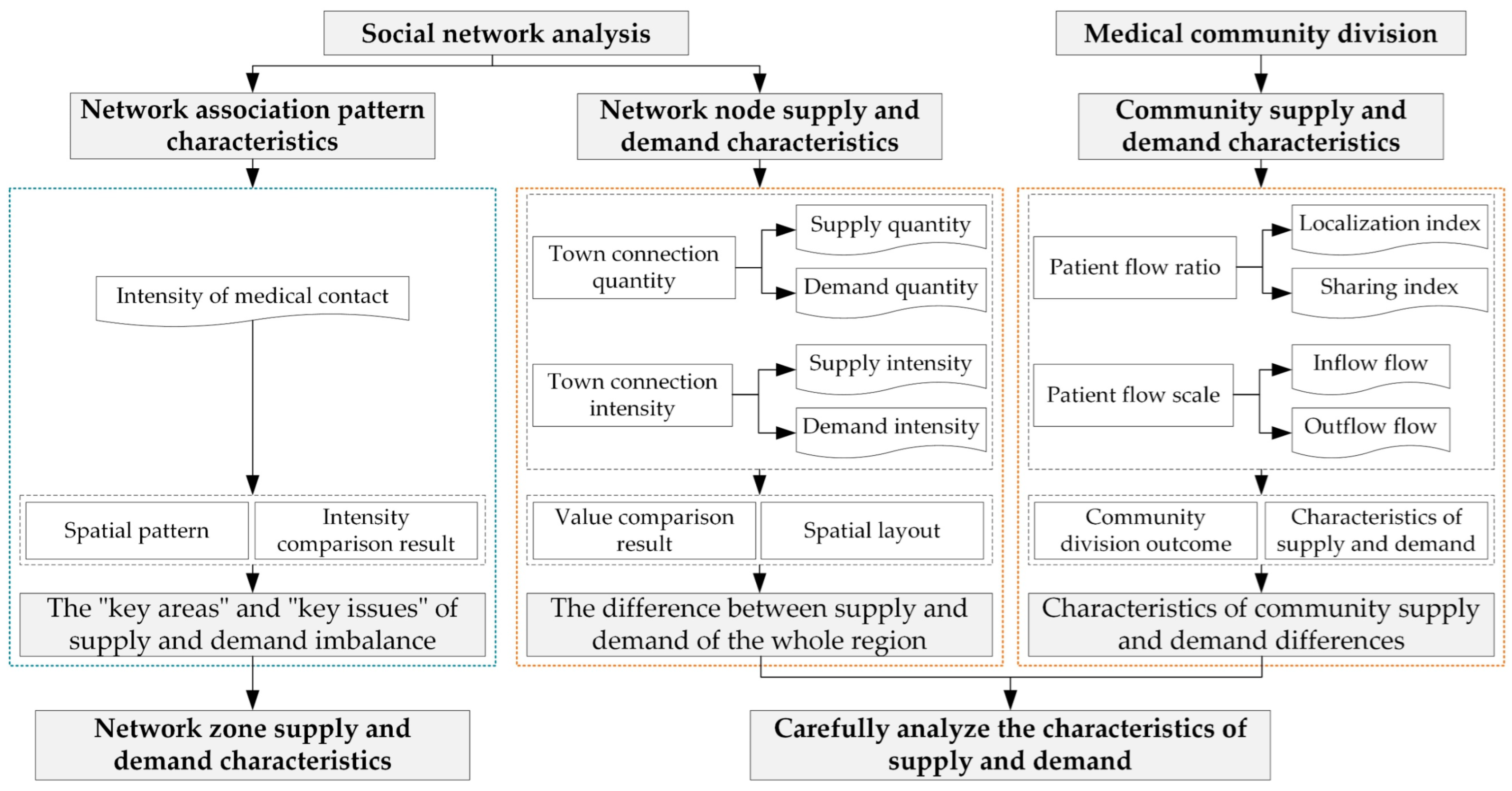
3.3.2. Analysis of Supply and Demand Characteristics
- (1)
- Social network analysis
- (2)
- Medical community division
4. Results
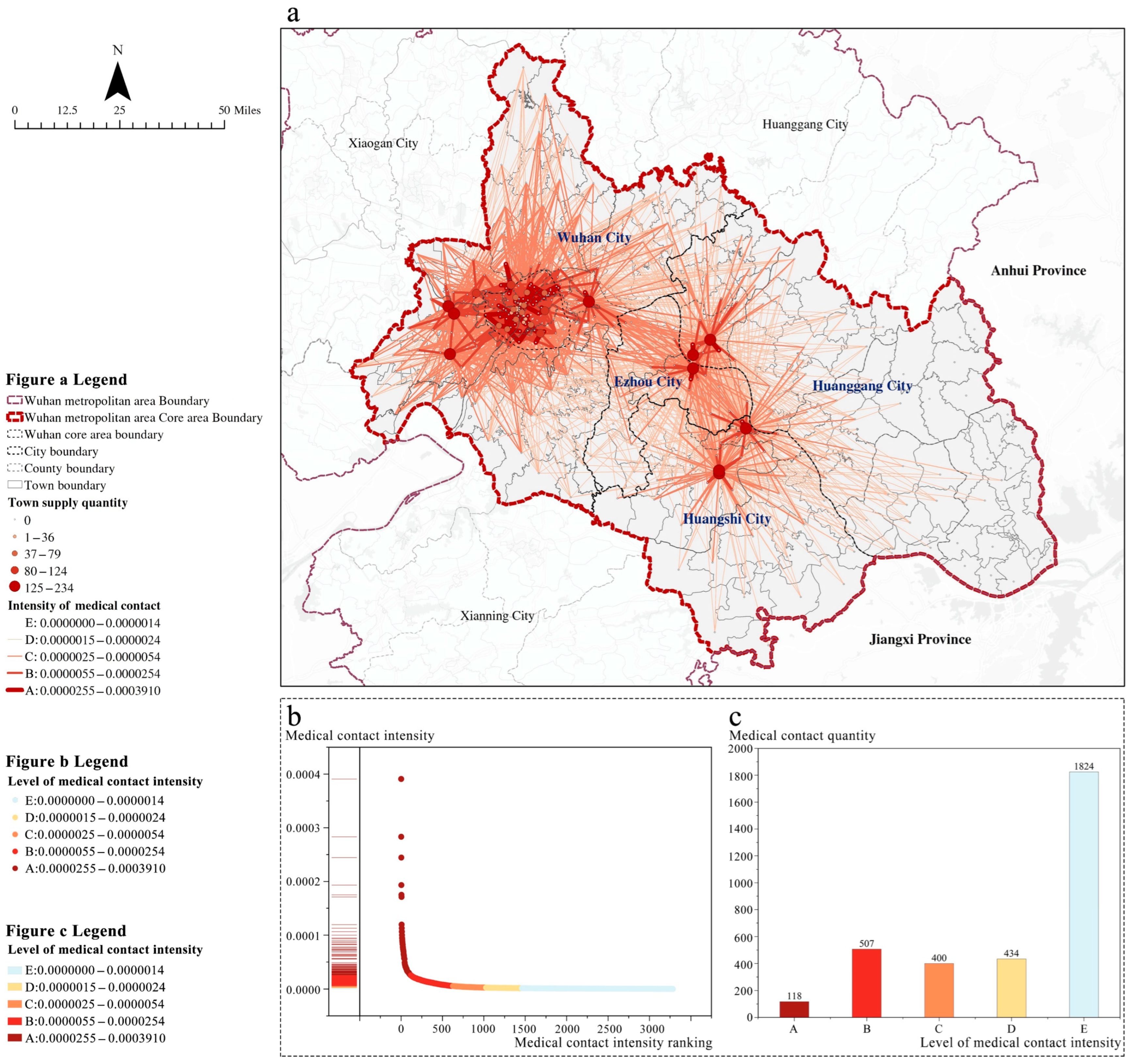
4.1. Network Association Pattern Characteristics
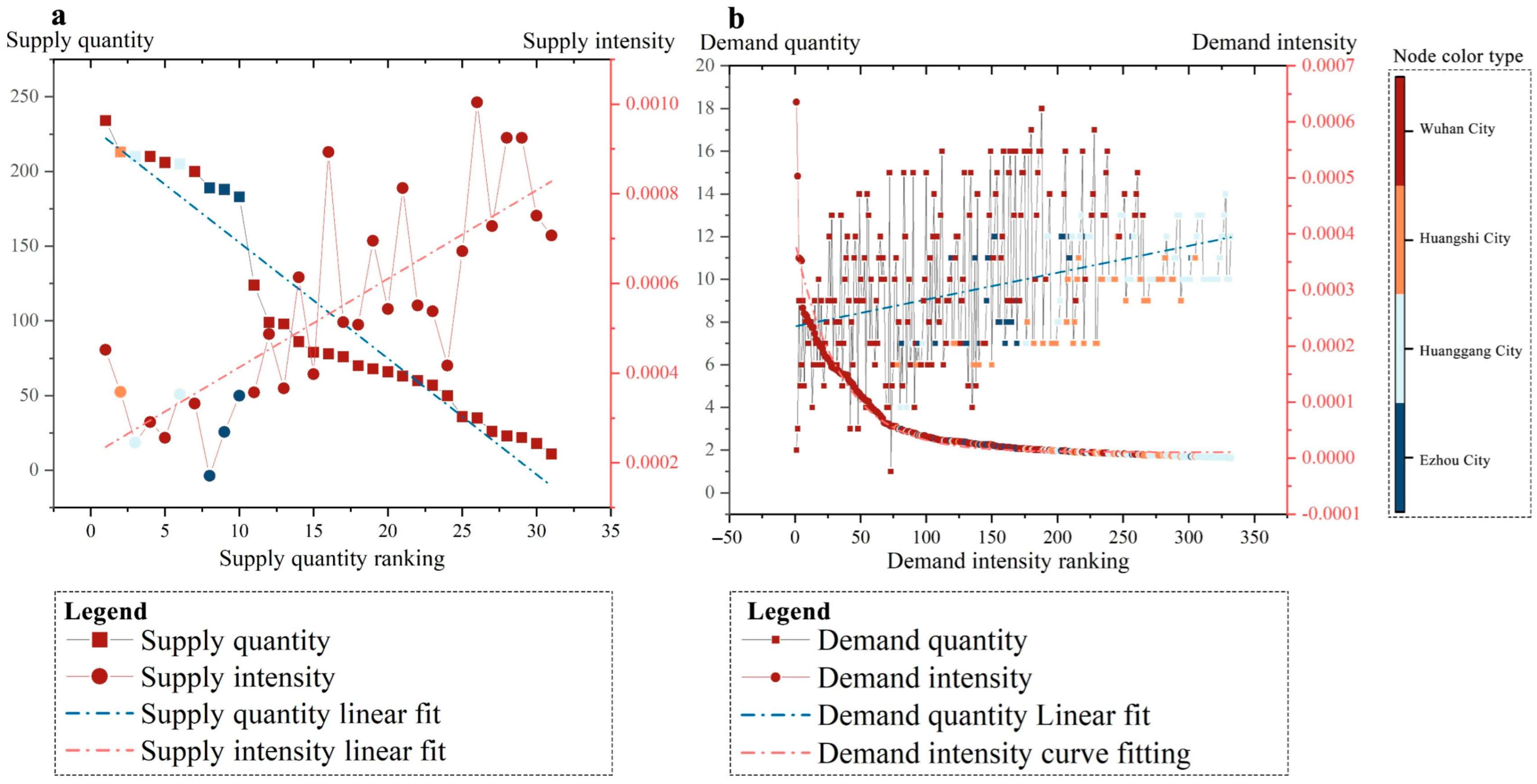
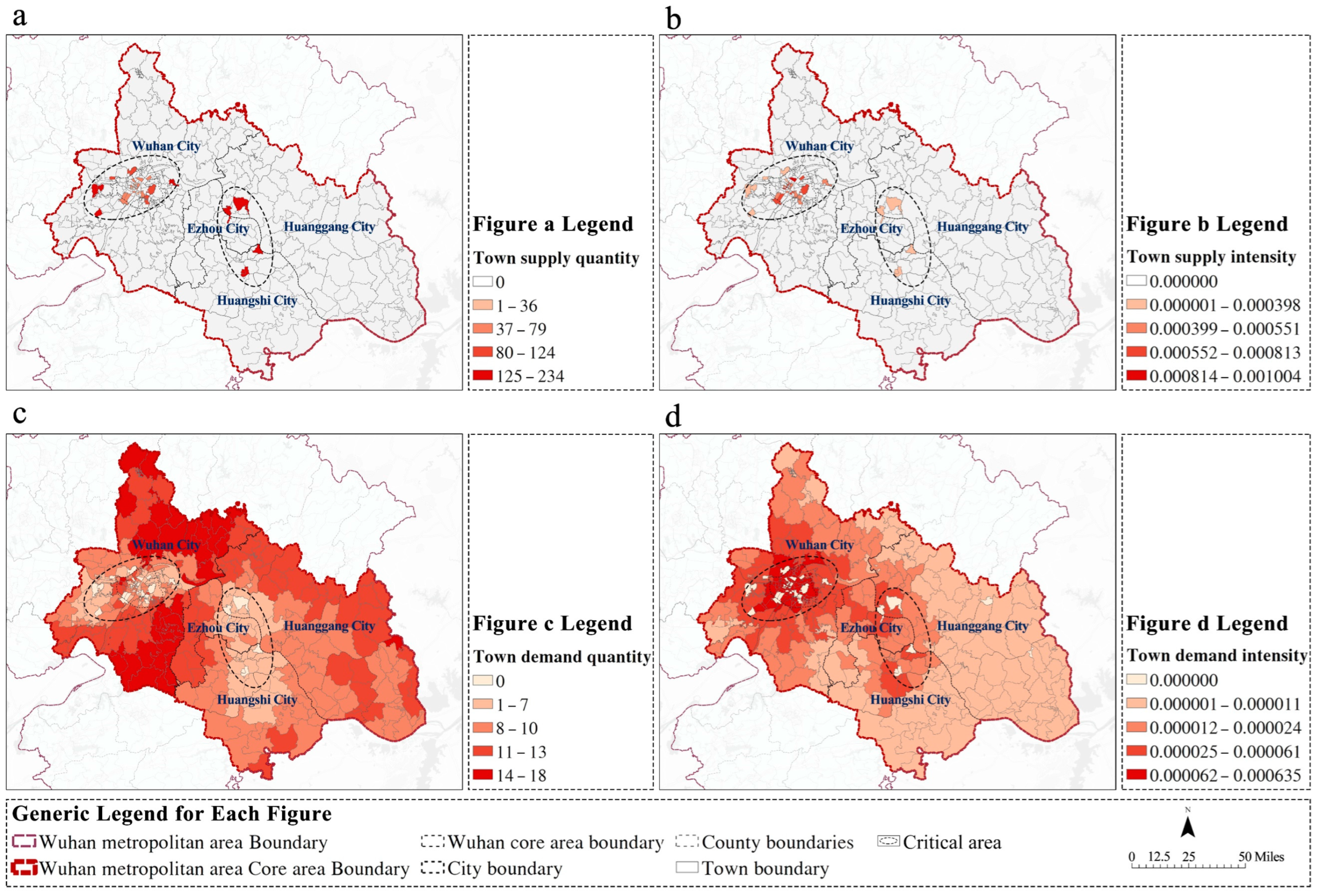
4.2. Network Node Supply and Demand Characteristics
4.3. Community Supply and Demand Characteristics
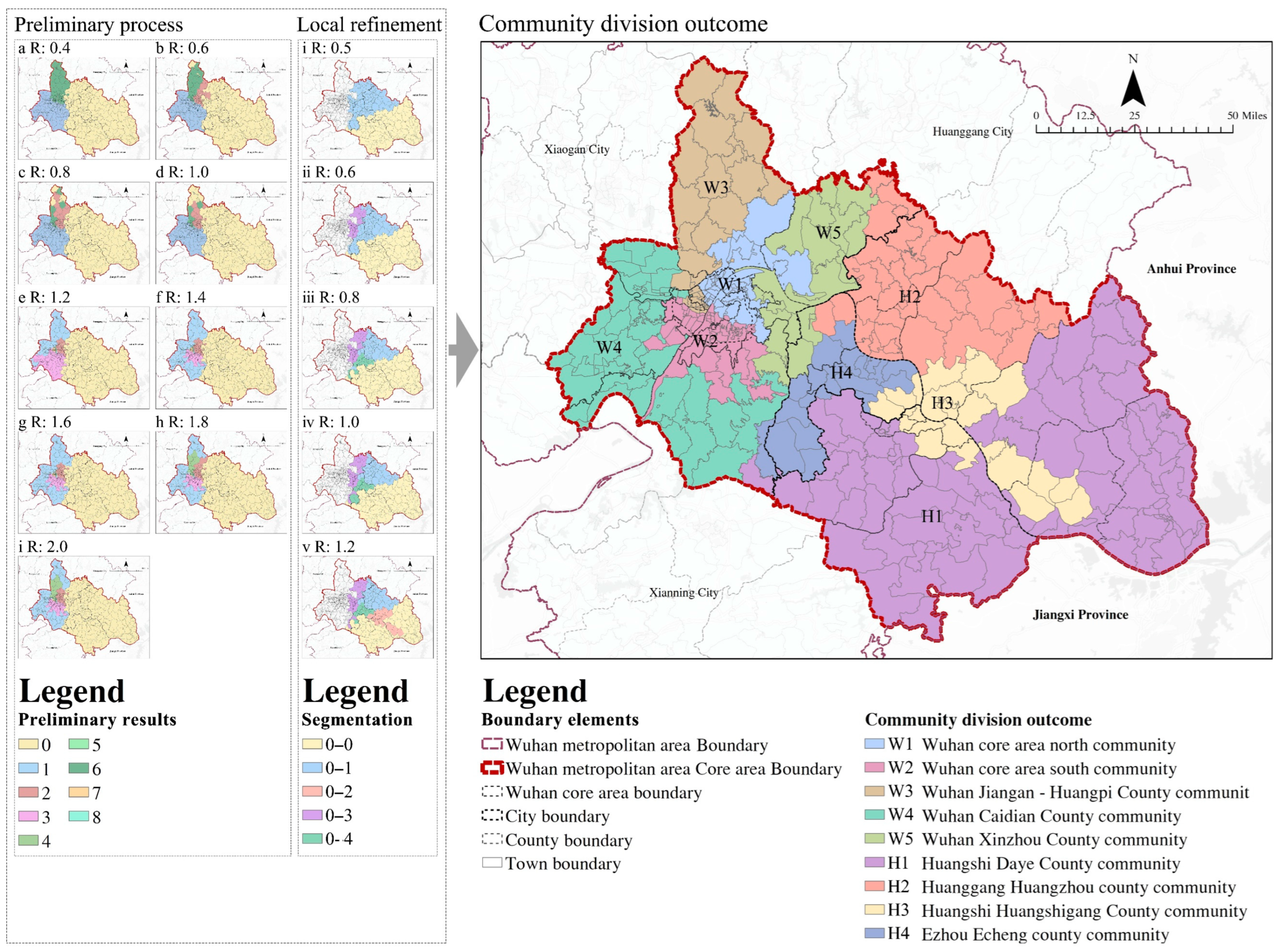
4.3.1. Division of Medical Service Communities
4.3.2. Supply and Demand Characteristics of Communities
5. Discussion
5.1. Advanced Construction of Medical Supply and Demand Network
5.2. Advanced Analysis of Community Supply and Demand Characteristics
5.3. Discussion Summary
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Yu, M.; He, S.; Wu, D.; Zhu, H.; Webster, C. Examining the Multi-Scalar Unevenness of High-Quality Healthcare Resources Distribution in China. Int. J. Environ. Res. Public Health 2019, 16, 2813. [Google Scholar] [CrossRef] [PubMed]
- Yip, W.; Fu, H.; Chen, A.T.; Zhai, T.; Jian, W.; Xu, R.; Pan, J.; Hu, M.; Zhou, Z.; Chen, Q.; et al. 10 Years of Health-Care Reform in China: Progress and Gaps in Universal Health Coverage. Lancet 2019, 394, 1192–1204. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wu, J. The Effect of the Referral System on the Accessibility of Healthcare Services: A Case Study of the Wuhan Metropolitan Development Zone. Int. J. Environ. Res. Public Health 2022, 19, 10441. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lu, J.; Hu, S.; Cheng, K.; De Maeseneer, J.; Meng, Q.; Mossialos, E.; Xu, D.R.; Yip, W.; Zhang, H.; et al. The Primary Health-Care System in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Yang, C.; Wang, Y.; Li, P.; Wang, F.; Kang, Y.; Wang, H.; Liang, Z.; Zhang, J.; Han, P.; et al. Influential Factors of Intercity Patient Mobility and Its Network Structure in China. Cities 2023, 132, 103975. [Google Scholar] [CrossRef]
- Yan, X.; Shan, L.; He, S.; Zhang, J. Cross-City Patient Mobility and Healthcare Equity and Efficiency: Evidence from Hefei, China. Travel Behav. Soc. 2022, 28, 1–12. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhao, M. Spatial Delineation, Characteristics Analysis, and Classification of China’s Metropolitan Regions. Urban Plan. Forum 2023, 67, 67–76. [Google Scholar] [CrossRef]
- Fu, L.; Xu, K.; Liu, F.; Liang, L.; Wang, Z. Regional Disparity and Patients Mobility: Benefits and Spillover Effects of the Spatial Network Structure of the Health Services in China. Int. J. Environ. Res. Public Health 2021, 18, 1096. [Google Scholar] [CrossRef]
- Tao, Z.; Cheng, Y.; Bai, L.; Feng, L.; Wang, S. Planning Hierarchical Hospital Service Areas for Maternal Care Using a Network Optimization Approach: A Case Study in Hubei, China. J. Geogr. Sci. 2022, 32, 2577–2598. [Google Scholar] [CrossRef]
- Jia, P.; Xierali, I.M.; Fahui, W. Evaluating and Re-Demarcating the Hospital Service Areas in Florida. Appl. Geogr. 2015, 60, 248–253. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, F.; Xierali, I.M. Automated Delineation of Hospital Service Areas and Hospital Referral Regions by Modularity Optimization. Health Serv. Res. 2018, 53, 236–255. [Google Scholar] [CrossRef]
- Wang, F.; Wang, C.; Hu, Y.; Weiss, J.; Alford-Teaster, J.; Onega, T. Automated Delineation of Cancer Service Areas in Northeast Region of the United States: A Network Optimization Approach. Spat. Spatio-Temporal Epidemiol. 2020, 33, 100338. [Google Scholar] [CrossRef]
- Wang, C.; Wang, F.; Onega, T. Network Optimization Approach to Delineating Health Care Service Areas: Spatially Constrained Louvain and Leiden Algorithms. Trans. GIS 2021, 25, 1065–1081. [Google Scholar] [CrossRef] [PubMed]
- Haynes, A.G.; Wertli, M.M.; Aujesky, D. Automated Delineation of Hospital Service Areas as a New Tool for Health Care Planning. Health Serv. Res. 2020, 55, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Xing, J.; Ng, S.T. Analyzing Spatiotemporal Accessibility Patterns to Tertiary Healthcare Services by Integrating Total Travel Cost into an Improved E3SFCA Method in Changsha, China. Cities 2022, 122, 103541. [Google Scholar] [CrossRef]
- Krügel, F.; Mäs, S. A Web-Application for Measuring Spatial Accessibility in Health Planning. AGILE GIScience Ser. 2023, 4, 1–11. [Google Scholar] [CrossRef]
- Thompson, C.A.; Saxberg, K.; Lega, J.; Tong, D.; Brown, H.E. A Cumulative Gravity Model for Inter-Urban Spatial Interaction at Different Scales. J. Transp. Geogr. 2019, 79, 102461. [Google Scholar] [CrossRef]
- Smith, D.; Timberlake, M. Conceptualizing and Mapping the Structure of the World Systems City System. Urban Stud. 1995, 32, 287–302. [Google Scholar] [CrossRef]
- Zhang, L.; Marzuki, A.; Liao, Z.; Zhao, K.; Huang, Z.; Chen, W. Spatial and Temporal Evolution of Guangdong Tourism Economic Network Structure from the Perspective of Social Networks. Heliyon 2023, 9, e18570. [Google Scholar] [CrossRef]
- Zhang, W.; Zhao, P.; Niu, C.; Thill, J.-C.; Zhu, J. City Networks and Clusters as Expressed in Chinese and Japanese Languages: A Multiscale Network Analysis with Language-Sensitive Webpage Big Data. Cities 2023, 141, 104502. [Google Scholar] [CrossRef]
- Sun, Y.; Shao, Y.; Chan, E.H.W. Co-Visitation Network in Tourism-Driven Peri-Urban Area Based on Social Media Analytics: A Case Study in Shenzhen, China. Landsc. Urban Plan. 2020, 204, 103934. [Google Scholar] [CrossRef]
- Huang, Y.; Hong, T.; Ma, T. Urban Network Externalities, Agglomeration Economies and Urban Economic Growth. Cities 2020, 107, 102882. [Google Scholar] [CrossRef]
- Yang, H.; Du, D.; Wang, J.; Wang, X.; Zhang, F. Reshaping China’s Urban Networks and Their Determinants: High-Speed Rail vs. Air Networks. Transp. Policy 2023, 143, 83–92. [Google Scholar] [CrossRef]
- Hong, M.; Wei, W.; Yin, L.; Xia, J. Exploring the Mechanism of the Impact of Basic Public Service Facilities on Residents’ Satisfaction: Based on the “Homo-Urbanicus” Theory. Hum. Geogr. 2023, 38, 107–117. [Google Scholar] [CrossRef]
- Wei, W.; Tao, Y.; Yang, H. Satisfaction Improvement on Layout of Primary Schools in Central Area of Big City. Planners 2020, 36, 13–18. [Google Scholar] [CrossRef]
- Wei, W.; Ke, Z. Analysis of Supply and Demand Matching and Planning Methods of Community Logistics Points from the Perspective of “Homo Urbanicus”: A Case Study of Wuhan City. Mod. Urban Res. 2020, 38, 8–17. [Google Scholar] [CrossRef]
- Wan, Y.; Tan, X.; Shu, H. Finding and Evaluating Community Structures in Spatial Networks. ISPRS Int. J. Geo.-Inf. 2023, 12, 187. [Google Scholar] [CrossRef]
- Reyes, V.; Suárez, M. Firm Survival and Location Preference: Evidence from Mexico City. Heliyon 2022, 8, e09219. [Google Scholar] [CrossRef] [PubMed]
- Gan, C.; Voda, M.; Wang, K.; Chen, L.; Ye, J. Spatial Network Structure of the Tourism Economy in Urban Agglomeration: A Social Network Analysis. J. Hosp. Tour. Manag. 2021, 47, 124–133. [Google Scholar] [CrossRef]
- Han, M.; He, D.; Gao, P. Boundary Effect and Multi-Dimensional Mechanism of Inter-City Producer Services Network in Yangtze River Economic Belt. Econ. Geogr. 2021, 41, 126–135. [Google Scholar] [CrossRef]
- Klauss, G.; Staub, L.; Widmer, M.; Busato, A. Hospital Service Areas—A New Tool for Health Care Planning in Switzerland. BMC Health Serv. Res. 2005, 5, 33. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Tao, Z.; Cheng, Y.; Feng, L.; Wang, S. Delineating Hierarchical Obstetric Hospital Service Areas Using the Huff Model Based on Medical Records. Appl. Geogr. 2023, 153, 102903. [Google Scholar] [CrossRef]
- Koylu, C.; Delil, S.; Guo, D.; Celik, R.N. Analysis of Big Patient Mobility Data for Identifying Medical Regions, Spatio-Temporal Characteristics and Care Demands of Patients on the Move. Int. J. Health Geogr. 2018, 17, 32. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index Name | ‘Supply-Type’ Town | ‘Demand-Type’ Town |
|---|---|---|
| Town connection quantity | The number of ‘demand-type’ towns radiated by medical services reflects the sharing scope of medical services in the town | The number of ‘supply-type’ towns providing medical services reflects the number of cross-border medical destinations in the town |
| Town connection intensity | The sum of the intensity of external medical services reflects the level of medical resource allocation in the town | The sum of the strength of the medical supply and demand connection established externally reflects the difficulty of the town’s patients in obtaining medical services |
| Intensity of medical contact | Intensity of supply and demand connection between two types of towns | |
| Index Name | Calculation Formula | Index Interpretation | Remark |
|---|---|---|---|
| Localization index | Proportion of patients in Community i who have cross-border medical treatment within the community | is the sum of the flow of patients in the community, that is, the sum of the supply and demand connection intensity among all towns in the community | |
| Sharing index | The proportion of non-local residents who go to Community i out of all people who go to community i for medical treatment | ||
| Inflow flow | The quantity of patients from the remaining communities who went to Community i for medical care | - | |
| Outflow flow | The quantity of patients within Community i who went to other communities for medical treatment |
| Community Code | LI | SI | IF | OF |
|---|---|---|---|---|
| W1 | 0.810 | 0.792 | 0.939 | 0.841 |
| W2 | 0.789 | 0.761 | 1.013 | 0.864 |
| W3 | 0.695 | 0.709 | 1.250 | 1.331 |
| W4 | 0.568 | 0.597 | 0.498 | 0.561 |
| W5 | 0.376 | 0.381 | 0.280 | 0.285 |
| H1 | 0.446 | 0.586 | 0.182 | 0.320 |
| H2 | 0.592 | 0.535 | 0.278 | 0.221 |
| H3 | 0.494 | 0.469 | 0.186 | 0.168 |
| H4 | 0.411 | 0.450 | 0.197 | 0.231 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, F.; Wei, W.; Xiang, B.; Hong, M. Analysis of Regional Medical Supply and Demand Network Characteristics Based on “Patient Flow Phenomenon”: A Case Study of the Core Area of the Wuhan Metropolitan Area. Land 2024, 13, 142. https://doi.org/10.3390/land13020142
Guo F, Wei W, Xiang B, Hong M. Analysis of Regional Medical Supply and Demand Network Characteristics Based on “Patient Flow Phenomenon”: A Case Study of the Core Area of the Wuhan Metropolitan Area. Land. 2024; 13(2):142. https://doi.org/10.3390/land13020142
Chicago/Turabian StyleGuo, Fang, Wei Wei, Bowen Xiang, and Mengyao Hong. 2024. "Analysis of Regional Medical Supply and Demand Network Characteristics Based on “Patient Flow Phenomenon”: A Case Study of the Core Area of the Wuhan Metropolitan Area" Land 13, no. 2: 142. https://doi.org/10.3390/land13020142
APA StyleGuo, F., Wei, W., Xiang, B., & Hong, M. (2024). Analysis of Regional Medical Supply and Demand Network Characteristics Based on “Patient Flow Phenomenon”: A Case Study of the Core Area of the Wuhan Metropolitan Area. Land, 13(2), 142. https://doi.org/10.3390/land13020142