
A Hybrid Mechanism-Based Robot for End-Traction Lower Limb Rehabilitation: Design, Analysis and Experimental Evaluation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
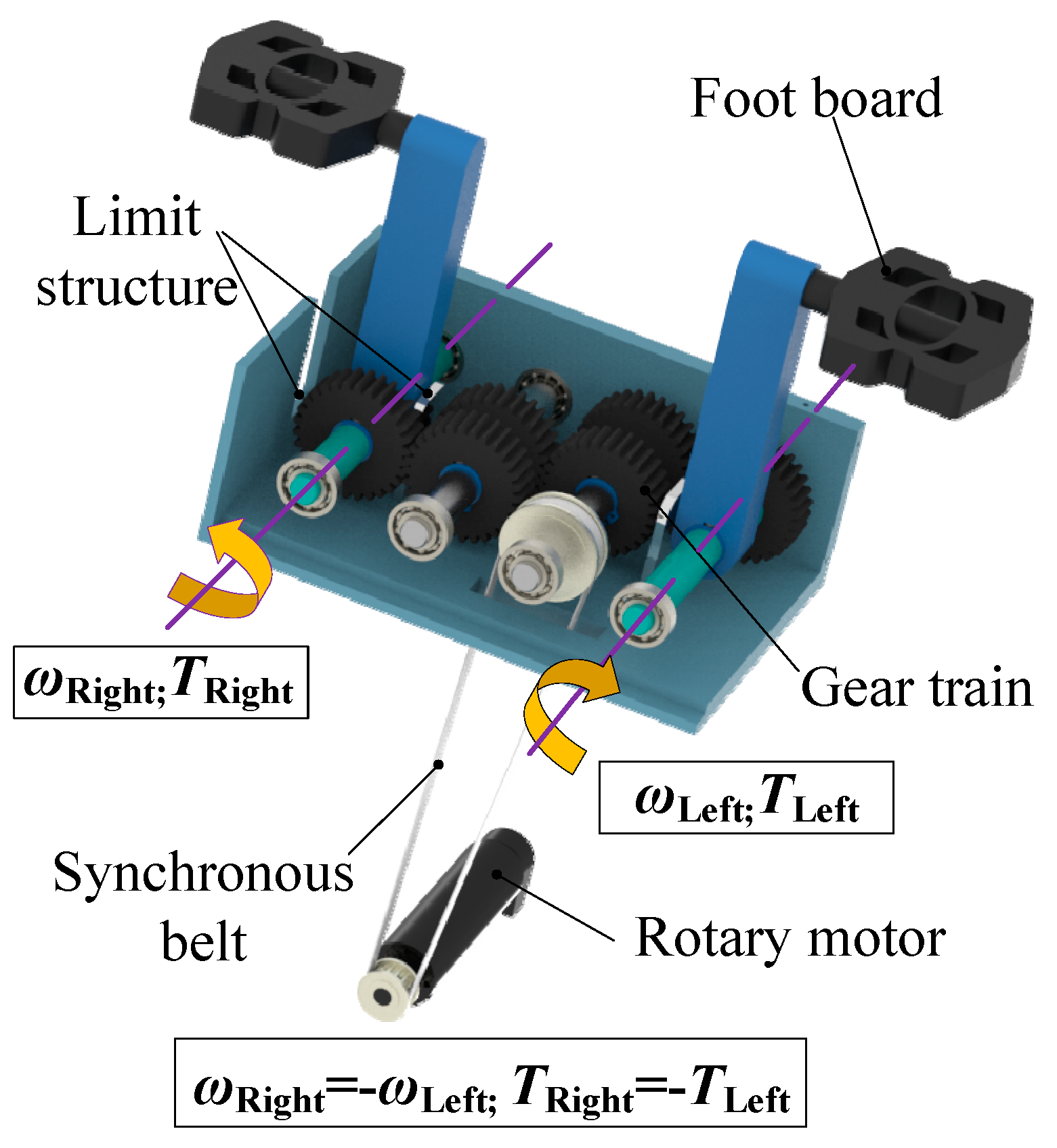
2.1. Configuration Design
2.2. Mobility Analysis
2.3. Inverse Kinematics
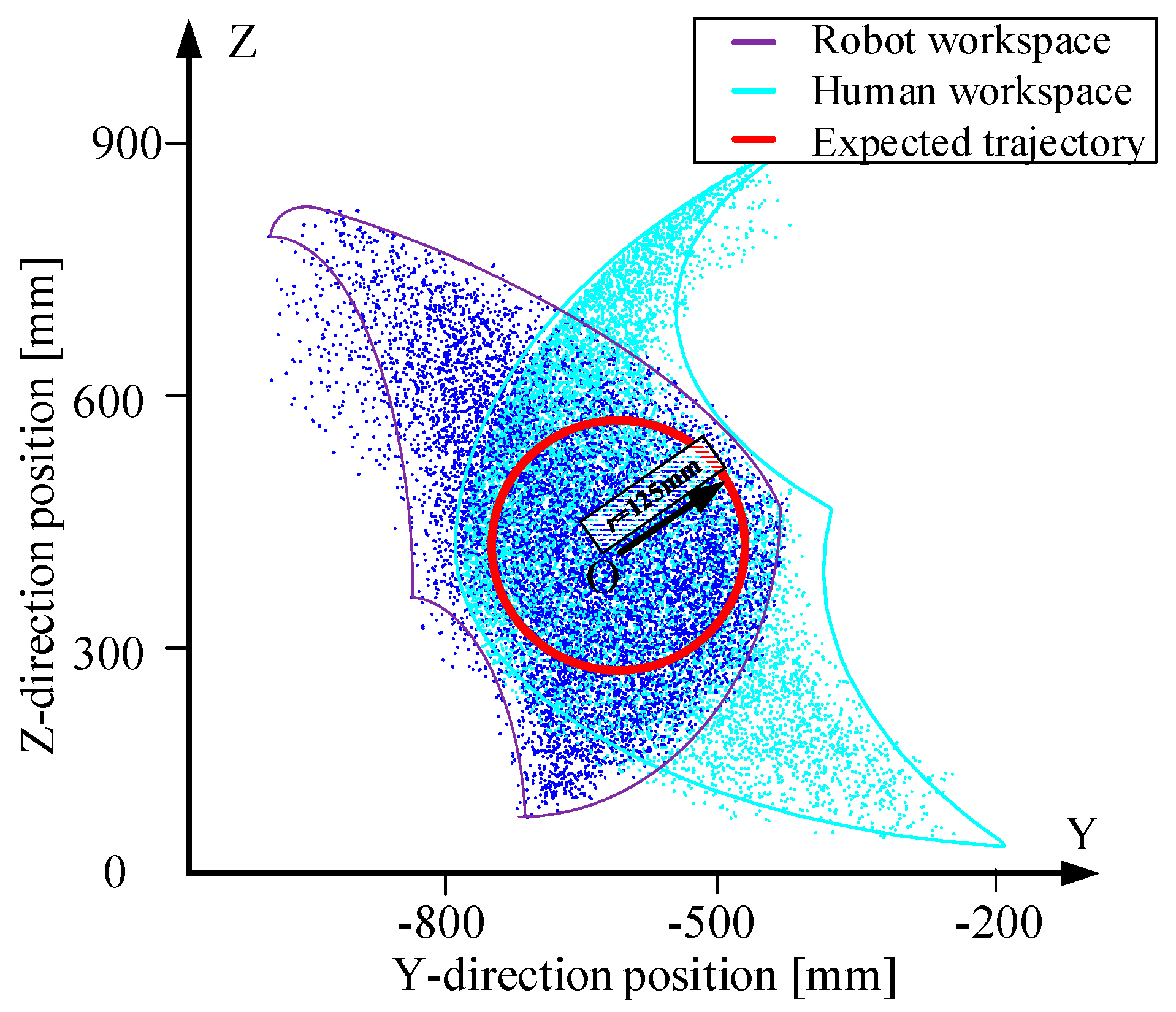
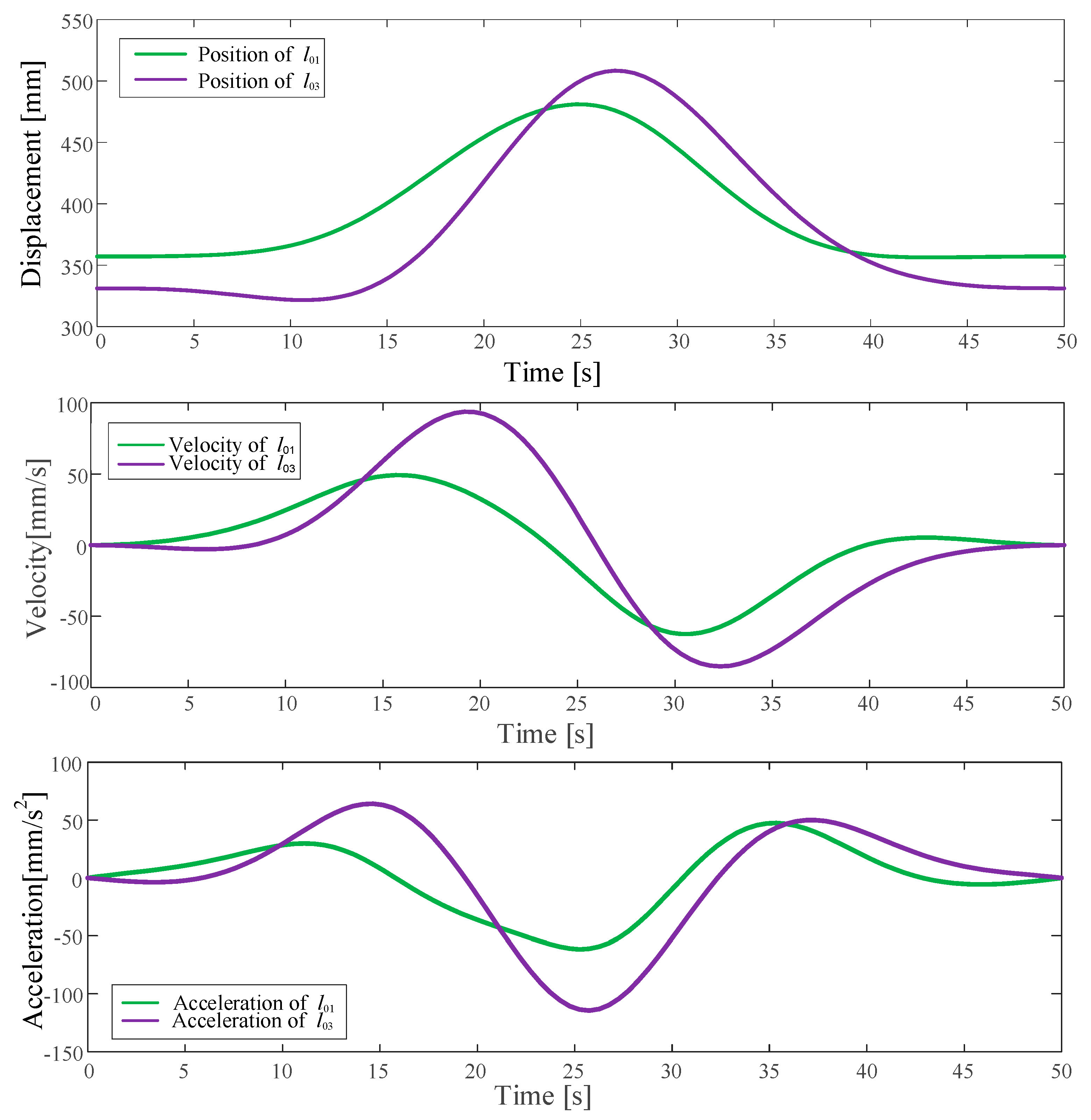
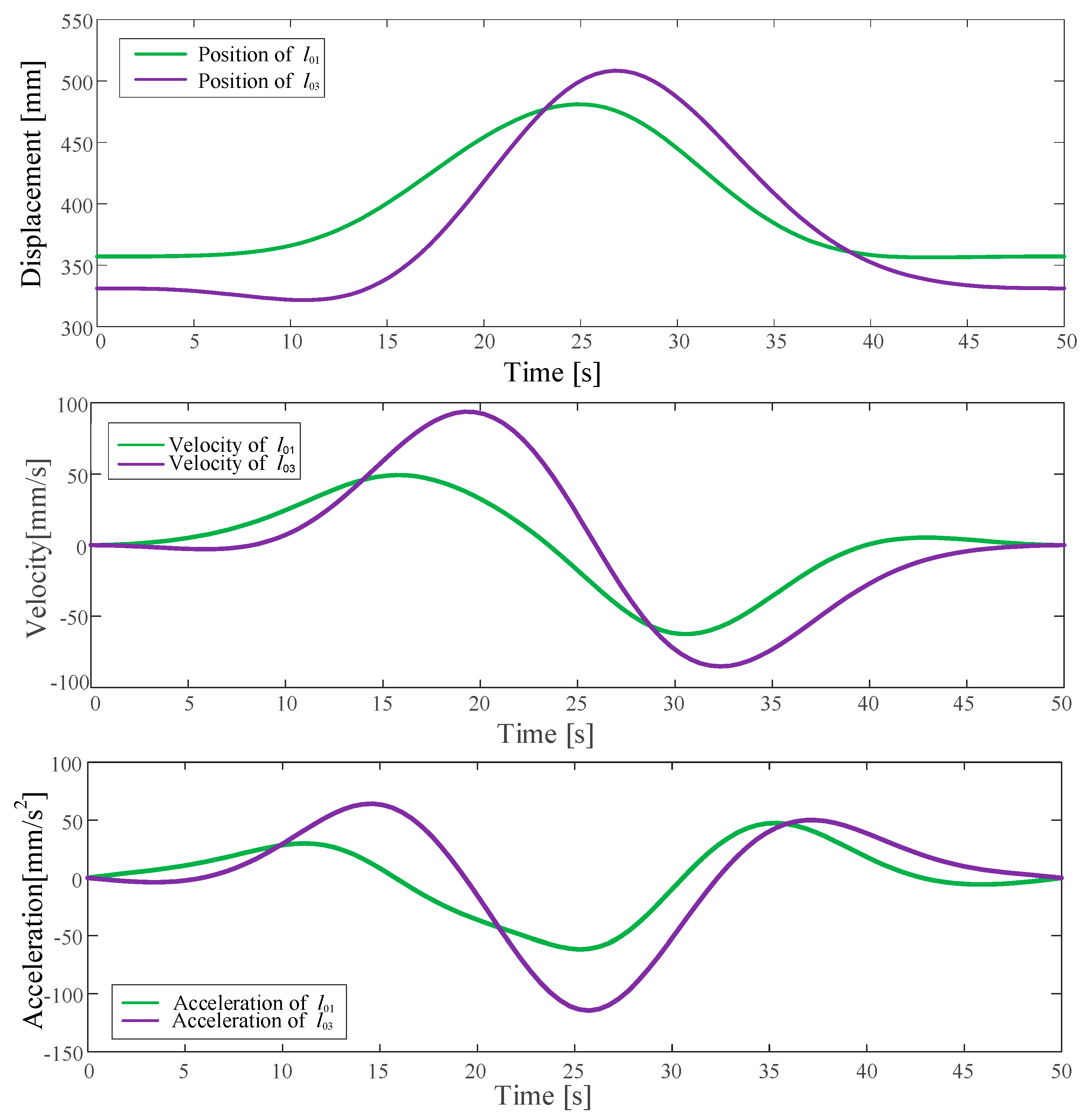
2.4. Trajectory Planning
3. Results
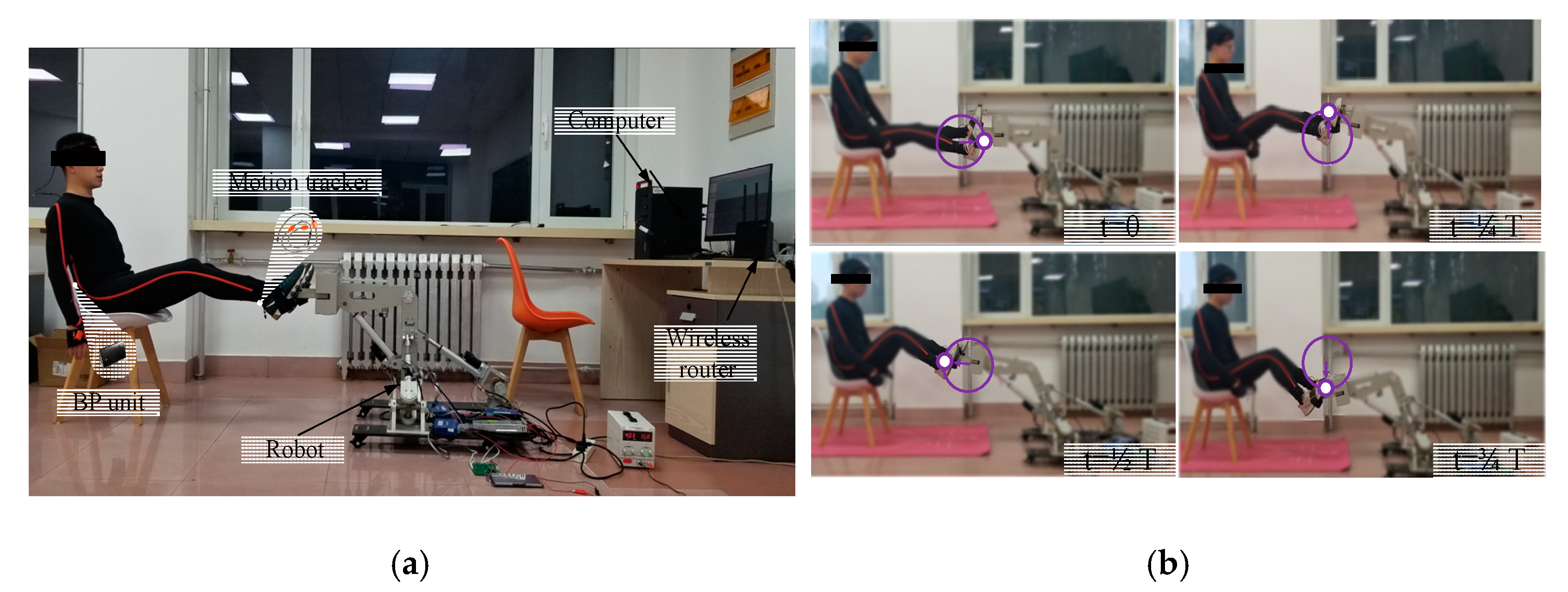
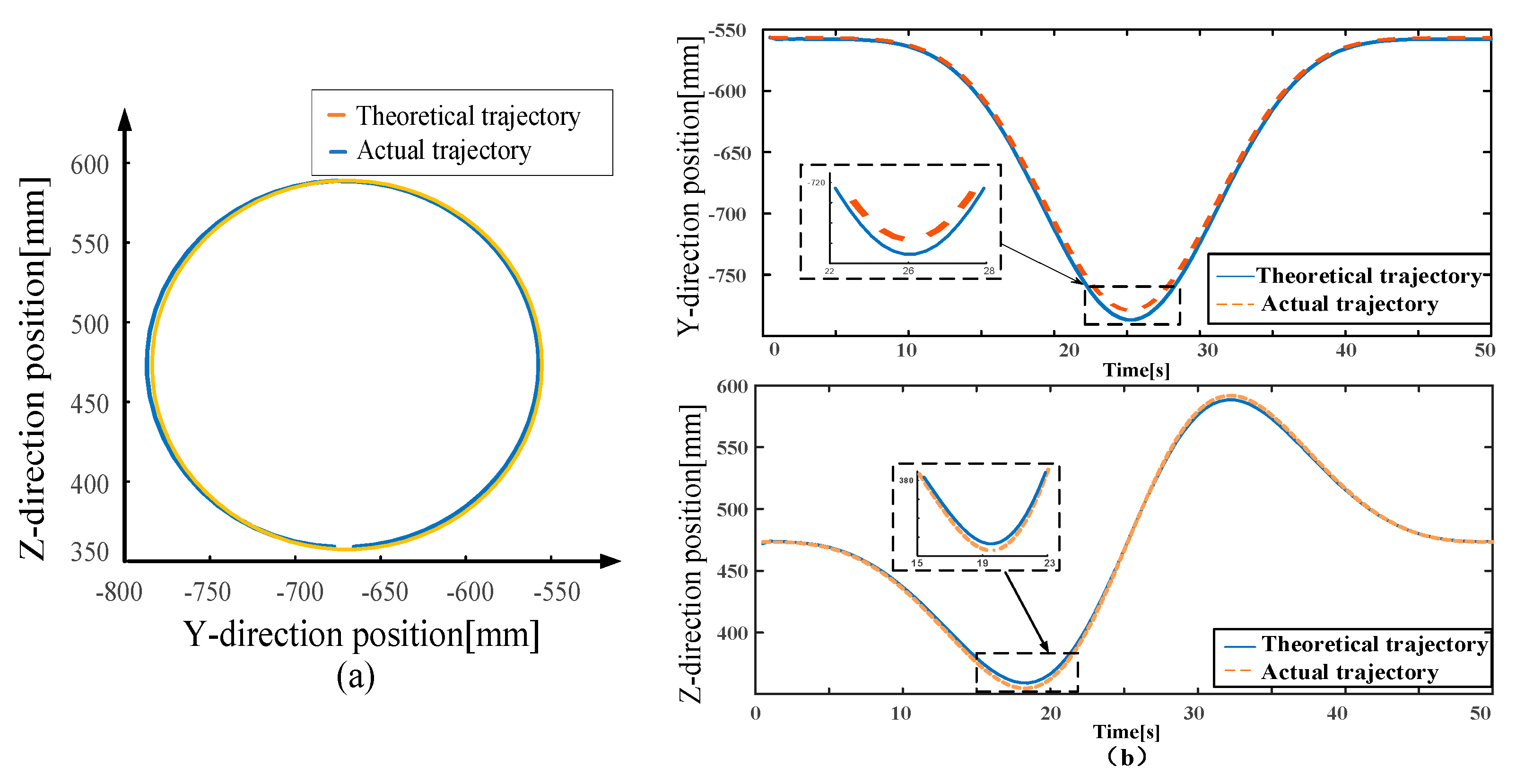
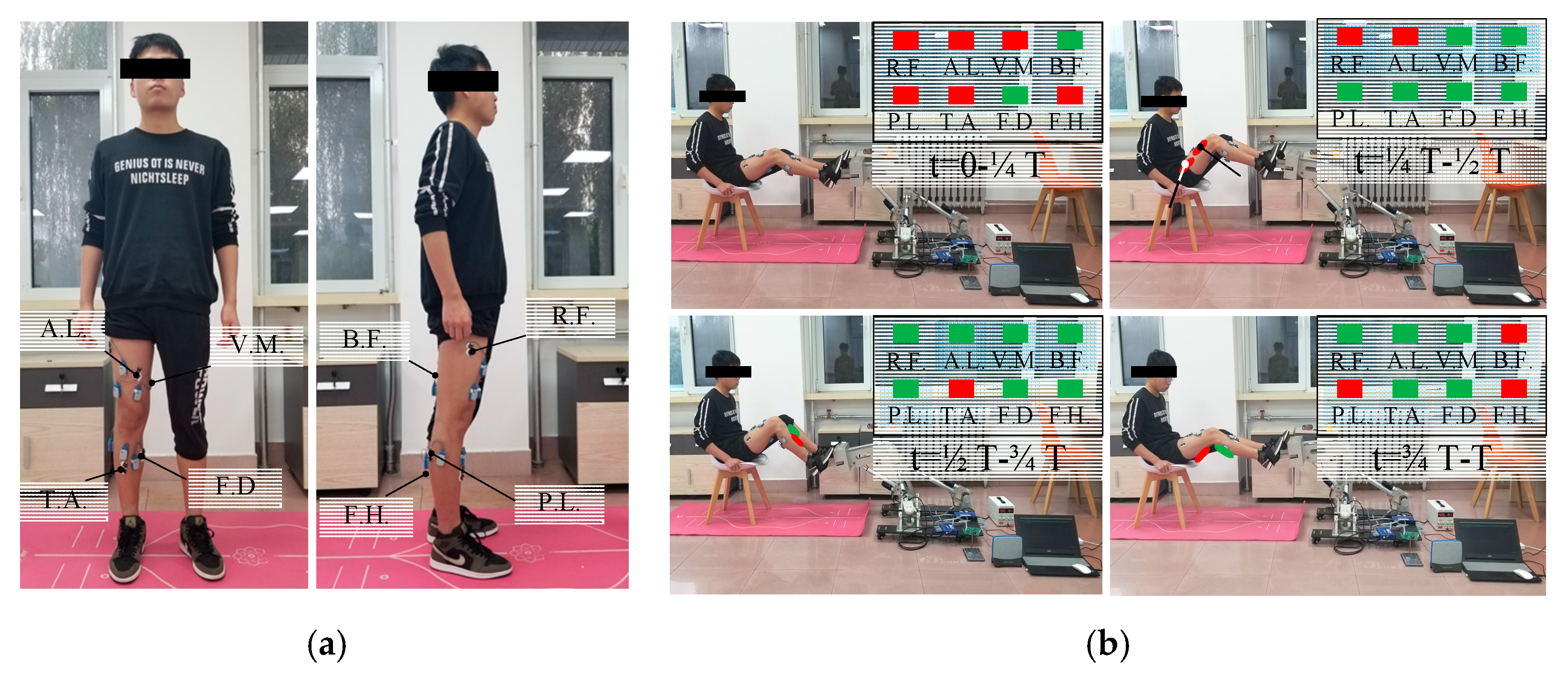
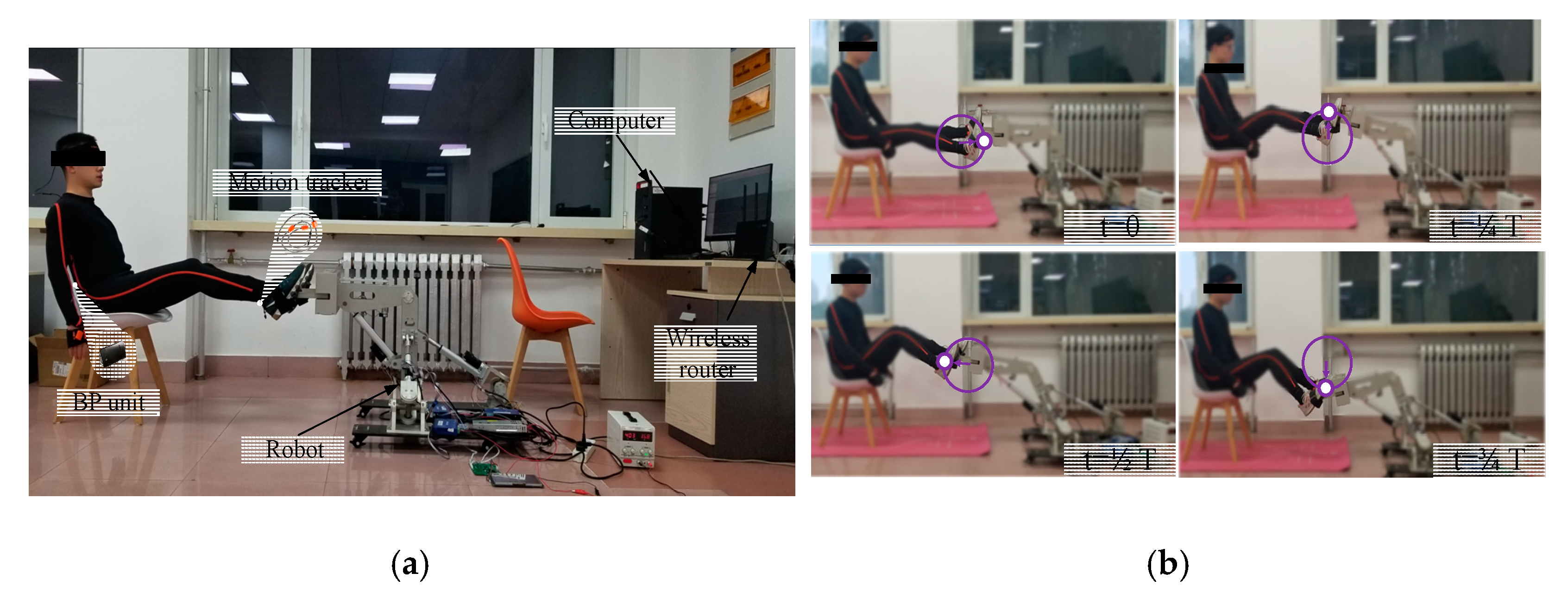
3.1. Motion Capture Experiment
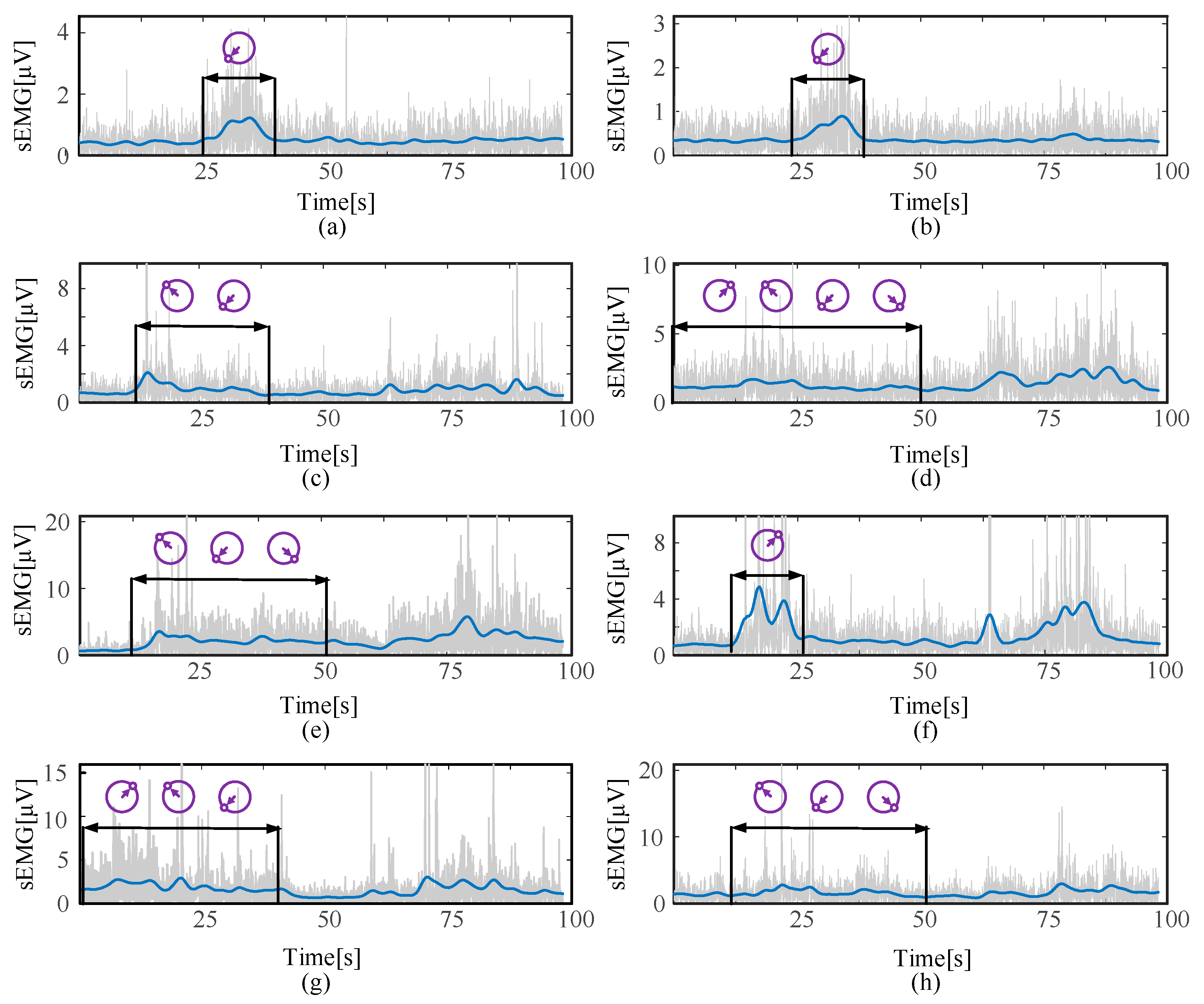
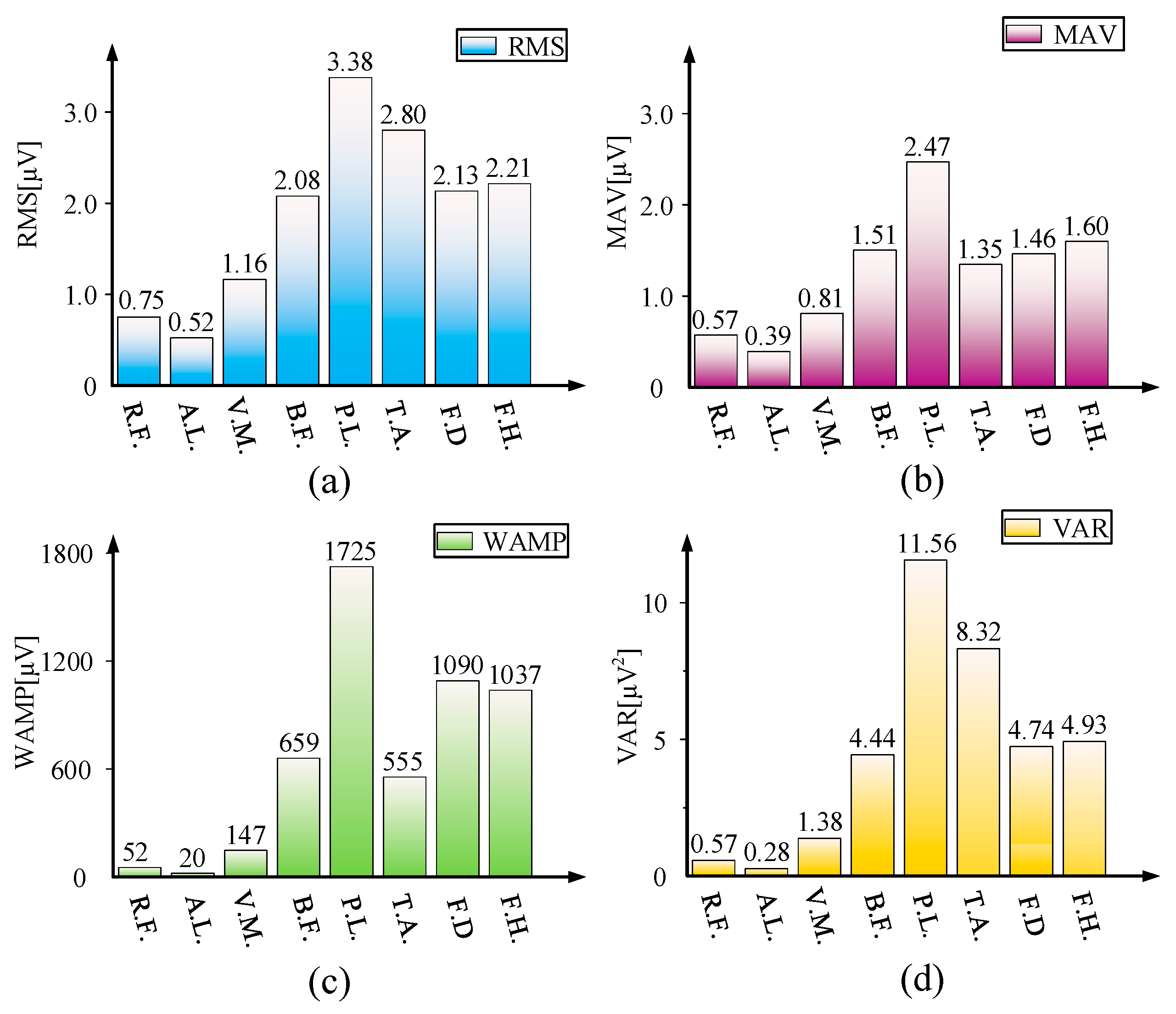
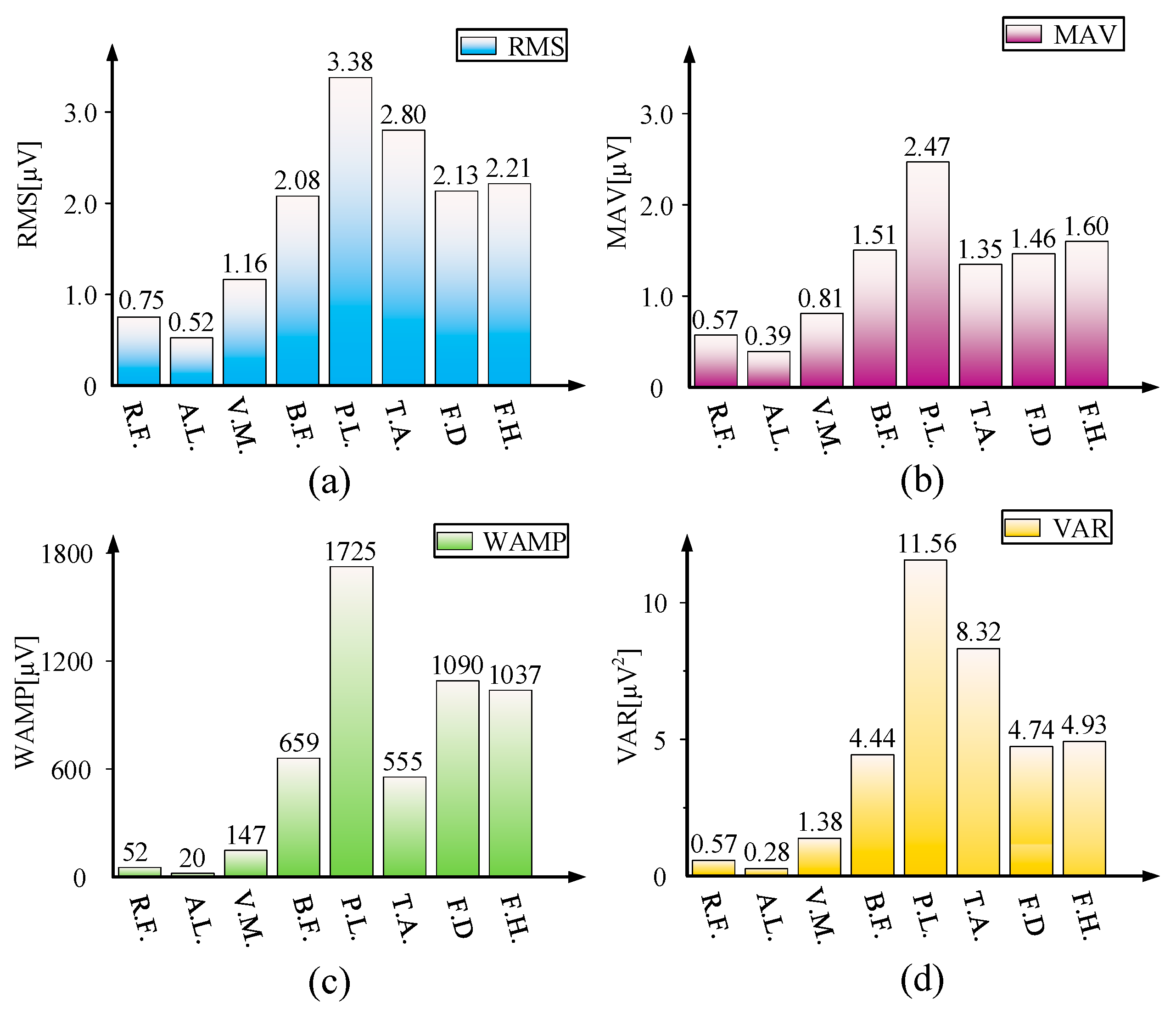
3.2. sEMG Signal Acquisition Experiment
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, J.; Li, Z.; Li, X.; Wang, X.; Song, R. Human–Robot Cooperation Control Based on Trajectory Deformation Algorithm for a Lower Limb Rehabilitation Robot. IEEE-ASME Trans. Mechatron. 2021, 26, 3128–3138. [Google Scholar] [CrossRef]
- Shi, X.; Wang, H.; Sun, L. Design and dynamic analysis of an exoskeletal lower limb rehabilitation robot. Chin. J. Mech. Eng. 2014, 50, 41–48. [Google Scholar] [CrossRef]
- Klamroth-Marganska, V.; Blanco, J.; Campen, K.; Curt, A.; Dietz, V.; Ettlin, T.; Felder, M.; Fellinghauer, B.; Guidali, M.; Kollmar, A.J.T.L.N. Three-dimensional, task-specific robot therapy of the arm after stroke: A multicentre, parallel-group randomised trial. Lancet Neurol. 2014, 13, 159–166. [Google Scholar] [CrossRef]
- Major, Z.; Vaida, C.; Major, K.; Tucan, P.; Brusturean, E.; Gherman, B.; Birlescu, I.; Craciunaș, R.; Ulinici, I.; Simori, G.; et al. Comparative Assessment of Robotic versus Classical Physical Therapy Using Muscle Strength and Ranges of Motion Testing in Neurological Diseases. J. Pers. Med. 2021, 11, 953. [Google Scholar] [CrossRef]
- Seo, J.; Kim, H. Biomechanical Analysis in Five Bar Linkage Prototype Machine of Gait Training and Rehabilitation by IMU Sensor and Electromyography. Sensors 2021, 21, 1726. [Google Scholar] [CrossRef]
- Viekash, V.K.; Arun, P.; Manimozhi, S.; Nagotanekar, G.D.; Deenadayalan, E. Deep Learning Based Muscle Intent Classification in Continuous Passive Motion Machine for Knee Osteoarthritis Rehabilitation. In Proceedings of the IEEE Madras Section Conference, Chennai, India, 27–28 August 2021; pp. 1–8. [Google Scholar]
- Wang, C.; Li, Y.; Xiong, Z.; Luo, Y.; Cao, Y. Lower Body Rehabilitation Dataset and Model Optimization. In Proceedings of the 2021 IEEE International Conference on Multimedia and Expo, Shenzhen, China, 5–9 July 2021; pp. 1–6. [Google Scholar]
- Shen, C.; Liu, F.; Yao, L.; Li, Z.; Qiu, L.; Fang, S. Effects of MOTOmed movement therapy on the mobility and activities of daily living of stroke patients with hemiplegia: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1569–1580. [Google Scholar] [CrossRef]
- Longde, W.; Jianmin, L.; Yi, Y.; Bin, P.; Yilong, W. The prevention and treatment of stroke in China still faces great challenges—Summary of the Report of Stroke Prevention and Treatment in China 2018. Chin. Circ. J. 2019, 34, 105–119. [Google Scholar]
- Sun, Z.; Li, F.; Lian, Y.; Liu, S.; Liu, K. An adaptive iterative learning control approach for lower limb rehabilitation robot in noisy environments. In Proceedings of the 2019 IEEE 9th Annual International Conference on CYBER Technology in Automation, Control, and Intelligent Systems (CYBER), IEEE, Suzhou, China, 29 July–2 August 2019; pp. 905–910. [Google Scholar]
- Shi, D.; Zhang, W.; Zhang, W. Human-centered adaptive control of lower limb rehabilitation robot based on human–robot interaction dynamic model. Mech. Mach. Theory 2021, 162, 104340. [Google Scholar] [CrossRef]
- Almaghout, K.; Tarvirdizadeh, B.; Alipour, K.; Hadi, A. Part H: Design and control of a lower limb rehabilitation robot considering undesirable torques of the patient’s limb. J. Eng. Med. 2020, 234, 1457–1471. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, K.; Zhang, Z. Control strategy and experimental research of a cable-driven lower limb rehabilitation robot. IEEE Access 2020, 9, 79182–79195. [Google Scholar] [CrossRef]
- Ármannsdóttir, A.L.; Beckerle, P.; Moreno, J.C.; van Asseldonk, E.H.; Manrique-Sancho, M.-T.; Del-Ama, A.J.; Veneman, J.F.; Briem, K.J. Assessing the involvement of users during development of lower limb wearable robotic exoskeletons: A survey study. SAGE Choice 2020, 62, 351–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aurich, T.; Gut, A.; Labruyere, R. The FreeD module for the Lokomat facilitates a physiological movement pattern in healthy people—A proof of concept study. J. Neuroeng. Rehabil. 2019, 16, 1–13. [Google Scholar]
- Gandara, T.; Fernande, M.; Rodriguez, A. Robotic systems for gait re-education in cases of spinal cord injury: A systematic review. Rev. De Neurol. 2017, 64, 205–213. [Google Scholar]
- Koukolová, I. Overview of the robotic rehabilitation systems for lower limb rehabilitation. Transf. Inovácií 2015, 31, 107–111. [Google Scholar]
- Aggogeri, F.; Pellegrini, N.; Adamini, R. Functional design in rehabilitation: Modular mechanisms for ankle complex. Appl. Bionics Biomech. 2016, 21, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Aglia, J.; Tsagarakis, N.; Dai, J. Control strategies for patient-assisted training using the ankle rehabilitation robot (ARBOT). IEEE-ASME Trans. Mechatron. 2013, 18, 1799–1808. [Google Scholar]
- Abbasnejad, G.; Yoon, J.; Lee, H. Optimum kinematic design of a planar cable-driven parallel robot with wrench-closure gait trajectory. Mech. Mach. Theory 2016, 99, 1–18. [Google Scholar] [CrossRef]
- Marghi, Y.; Farjadian, A.; Yen, S. EEG-guided robotic mirror therapy system for lower limb rehabilitation In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). Jeju Island, Korea, 11–15 July 2017; pp. 1917–1921. [Google Scholar]
- Liu, W.; Yin, B.; Yan, B. A survey on the exoskeleton rehabilitation robot for the lower limbs. In Proceedings of the 2016 2nd International Conference on Control, Automation and Robotics (ICCAR), Hong Kong, China, 28–30 April 2016; pp. 90–94. [Google Scholar]
- Masengo, G. A Design of Lower Limb Rehabilitation Robot and its Control for Passive Training. In Proceedings of the 2020 10th Institute of Electrical and Electronics Engineers International Conference on Cyber Technology in Automation, Control, and Intelligent Systems, Xi’an, China, 10–14 October 2020; pp. 152–157. [Google Scholar]
- Liang, F.Y.; Zhong, C.H.; Zhao, X.; Castro, D.L.; Chen, B.; Gao, F.; Liao, W.H. Online Adaptive and LSTM-Based Trajectory Generation of Lower Limb Exoskeletons for Stroke Rehabilitation. In Proceedings of the 2018 IEEE International Conference on Robotics and Biomimetics (ROBIO), Kuala Lumpur, Malaysia, 12–15 December 2018; pp. 27–32. [Google Scholar]
- Dai, J.; Mechanisms, K. Geometrical Foundations and Screw Algebra for Mechanisms and Robotics; Higher Education Press: Beijing, China, 2014; pp. 225–235. [Google Scholar]
- Niu, J.; Wang, H.; Jiang, Z.; Chen, L.; Zhang, J.; Feng, Y.; Guo, S. Kinematic Analysis of a Serial-Parallel Hybrid Mechanism and Its Application to a Wheel-Legged Robot. IEEE Access 2020, 8, 111931–111944. [Google Scholar] [CrossRef]
- Niu, J.; Wang, H.; Shi, H.; Nicolae, P.; Li, D.; Li, S.; Wu, S. Study on Structural Modeling and Kinematics Analysis of a Novel Wheel-Legged Rescue Robot. Int. J. Adv. Robot. Syst. 2018, 15, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Lee, C.; Lin, R. Effect of biofeedback cycling training on functional recovery and walking ability of lower extremity in patients with stroke. Kaohsiung J. Med. Sci. 2014, 30, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Skvortsova, V.; Ivanova, G.; Rumiantseva, N. Modern approach to gait restoration in patients in the acute period of cerebral stroke. Vserossiiskoe Obs. Psikhiatrov 2010, 110, 25–30. [Google Scholar]
- Wang, S.; Shi, X.; Li, H. DAPK1 Signaling Pathways in Stroke: From Mechanisms to Therapies. Mol. Neurobiol. 2017, 54, 4716–4722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, J.; Kim, G.; Hai, C. Reperfusion and Neurovascular Dysfunction in Stroke: From Basic Mechanisms to Potential Strategies for Neuroprotection. Mol. Neurobiol. 2010, 41, 172–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabinowitch, I. Inserting new synaptic connections into damaged neural circuits: Towards synapse therapy. Neural Regen. Res. 2022, 17, 2. [Google Scholar] [CrossRef] [PubMed]
- Kyeong, S.; Kim, J. Fatigue characteristics of surface electromyography during walking. In Proceedings of the 2018 18th International Conference on Control, Automation and Systems (ICCAS), PyeongChang, Korea, 17–20 October 2018; pp. 897–899. [Google Scholar]
- Kaur, M.; Mathur, S.; Bhatia, D.; Verma, S. EMG analysis for identifying walking patterns in healthy males. In Proceedings of the 2015 11th Conference on Ph. D. Research in Microelectronics and Electronics (PRIME), Glasgow, UK, 29 June 2015; pp. 65–68. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Age (Year) | Height (cm) | Thigh Length (cm) | Leg Length (cm) | Healthy Condition (Yes/No) |
|---|---|---|---|---|---|
| 1 | 29 | 170 | 47 | 40 | Yes |
| 2 | 21 | 175 | 48 | 40 | yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Tian, J.; Du, J.; Zheng, S.; Niu, J.; Zhang, Z.; Wu, J. A Hybrid Mechanism-Based Robot for End-Traction Lower Limb Rehabilitation: Design, Analysis and Experimental Evaluation. Machines 2022, 10, 99. https://doi.org/10.3390/machines10020099
Wang L, Tian J, Du J, Zheng S, Niu J, Zhang Z, Wu J. A Hybrid Mechanism-Based Robot for End-Traction Lower Limb Rehabilitation: Design, Analysis and Experimental Evaluation. Machines. 2022; 10(2):99. https://doi.org/10.3390/machines10020099
Chicago/Turabian StyleWang, Lipeng, Junjie Tian, Jiazheng Du, Siyuan Zheng, Jianye Niu, Zhengyan Zhang, and Jiang Wu. 2022. "A Hybrid Mechanism-Based Robot for End-Traction Lower Limb Rehabilitation: Design, Analysis and Experimental Evaluation" Machines 10, no. 2: 99. https://doi.org/10.3390/machines10020099