
The Repeatability and Agreement of Ocular Parameters Measured with the MYAH and Myopia Master Devices between Expert and Non-Expert Practitioners


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Devices
2.3. Measurement Procedure
2.4. Statistical Analyses
3. Results
3.1. Patient Demographics
3.2. Intraobserver Repeatability
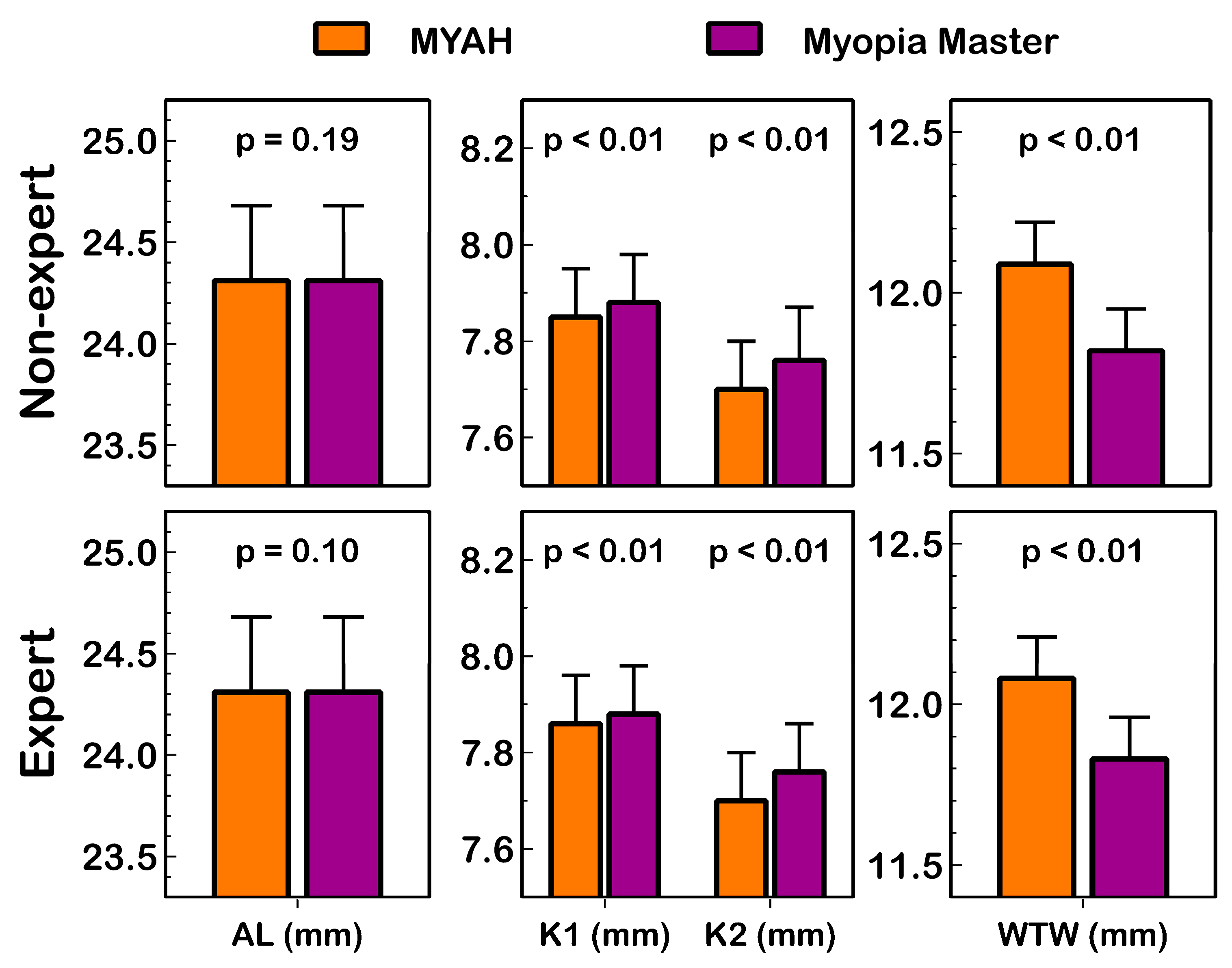
3.3. Interdevice Agreement (MYAH vs. Myopia Master)
3.4. Interobserver Agreement (between Expert and Non-Expert)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Sankaridurg, P.; Tahhan, N.; Kandel, H.; Naduvilath, T.; Zou, H.; Frick, K.D.; Marmamula, S.; Friedman, D.S.; Lamoureux, E.; Keeffe, J.; et al. IMI impact of myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 2. [Google Scholar] [CrossRef] [PubMed]
- Wildsoet, C.F.; Chia, A.; Cho, P.; Guggenheim, J.A.; Polling, J.R.; Read, S.; Sankaridurg, P.; Saw, S.-M.; Trier, K.; Walline, J.J.; et al. IMI—Interventions Myopia Institute: Interventions for controlling myopia onset and progression report. Investig. Ophthalmol. Vis. Sci. 2019, 60, M106–M131. [Google Scholar] [CrossRef]
- Ohno-Matsui, K.; Wu, P.-C.; Yamashiro, K.; Vutipongsatorn, K.; Fang, Y.; Cheung, C.M.G.; Lai, T.Y.Y.; Ikuno, Y.; Cohen, S.Y.; Gaudric, A.; et al. IMI pathologic myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 5. [Google Scholar] [CrossRef] [PubMed]
- Chia, A.; Chua, W.H.; Cheung, Y.B.; Wong, W.L.; Lingham, A.; Fong, A.; Tan, D. Atropine for the treatment of childhood myopia: Safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology 2012, 119, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, T. Myopia control with orthokeratology: A review. Eye Contact Lens 2022, 48, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Pomeda, A.; Villa-Collar, C. Slowing the progression of myopia in children with the MiSight contact lens: A narrative review of the evidence. Ophthalmol. Ther. 2020, 9, 783–795. [Google Scholar] [CrossRef]
- Lam, C.S.; Tang, W.C.; Lee, P.H.; Zhang, H.Y.; Qi, H.; Hasegawa, K.; To, C.H. Myopia control effect of defocus incorporated multiple segments (DIMS) spectacle lens in chinese children: Results of a 3-year follow-up study. Br. J. Ophthalmol. 2022, 106, 1110–1114. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Kollbaum, P.S.; Berntsen, D.A.; Atchison, D.A.; Benavente, A.; Bradley, A.; Buckhurst, H.; Collins, M.; Fujikado, T.; Hiraoka, T.; et al. IMI—Clinical myopia control trials and instrumentation report. Investig. Ophthalmol. Vis. Sci. 2019, 60, M132–M160. [Google Scholar] [CrossRef]
- Huang, J.; Wen, D.; Wang, Q.; McAlinden, C.; Flitcroft, I.; Chen, H.; Saw, S.M.; Chen, H.; Bao, F.; Zhao, Y.; et al. Efficacy comparison of 16 interventions for myopia control in children: A Network Meta-Analysis. Ophthalmology 2016, 123, 697–708. [Google Scholar] [CrossRef]
- Kojima, T.; Tamaoki, A.; Yoshida, N.; Kaga, T.; Suto, C.; Ichikawa, K. Evaluation of axial length measurement of the eye using partial coherence interferometry and ultrasound in cases of macular disease. Ophthalmology 2010, 117, 1750–1754. [Google Scholar] [CrossRef]
- Sabur, H.; Takes, O. Agreement of axial length and anterior segment parameters measured with the MYAH device compared to Pentacam AXL and IOLMaster 700 in myopic children. Int. Ophthalmol. 2023, 43, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Plaza, E.; Molina-Martín, A.; Arias-Puente, A.; Piñero, D.P. Clinical validation of a new optical biometer for myopia control in a healthy pediatric population. Children 2022, 9, 1713. [Google Scholar] [CrossRef]
- Garcia Ardoy, E.; Mateos, N.; Roda, L.; Torrado Sierra, O.; Baptista, A.M.; Serra, P.M. Repeatability and agreement of swept-source optical coherence tomography and partial coherence interferometry biometers in myopes. Clin. Exp. Optom. 2022, 106, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.A.P.; Azar, D.T.; Baudouin, C.; Bitton, E.; Chen, W.; Hafezi, F.; Hamrah, P.; Hogg, R.E.; Horwath-Winter, J.; Kontadakis, G.A.; et al. TFOS lifestyle: Impact of elective medications and procedures on the ocular surface. Ocul. Surf. 2023, 29, 331–385. [Google Scholar] [CrossRef] [PubMed]
- Efron, N. Contact Lens Complications, 3rd ed.; Elsevier Saunders: New York, NY, USA, 2012. [Google Scholar]
- Armstrong, R.A. Statistical guidelines for the analysis of data obtained from one or both eyes. Ophthalmic Physiol. Opt. 2013, 33, 7–14. [Google Scholar] [CrossRef]
- Ortiz-Toquero, S.; Rodriguez, G.; de Juan, V.; Martin, R. Repeatability of wavefront aberration measurements with a Placido-based topographer in normal and keratoconic eyes. J. Refract. Surg. 2016, 32, 338–344. [Google Scholar] [CrossRef]
- McAlinden, C.; Khadka, J.; Pesudovs, K. Statistical methods for conducting agreement (comparison of clinical tests) and precision (repeatability or reproducibility) studies in optometry and ophthalmology. Ophthalmic Physiol. Opt. 2011, 31, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.A. Recommendations for analysis of repeated-measures designs: Testing and correcting for sphericity and use of manova and mixed model analysis. Ophthalmic Physiol. Opt. 2017, 37, 585–593. [Google Scholar] [CrossRef]
- Bland, J.M. An Introduction to Medical Statistics, 3rd ed.; Oxford University Press: Oxford, UK, 2000; pp. 137–155. [Google Scholar]
- McGraw, K.O.; Wong, S.P. Forming inferences about some intraclass correlation coefficients. Psychol. Methods 1996, 1, 30–46. [Google Scholar] [CrossRef]
- McAlinden, C.; Khadka, J.; Pesudovs, K. Precision (repeatability and reproducibility) studies and sample-size calculation. J. Cataract Refract. Surg. 2015, 41, 2598–2604. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Carkeet, A. Exact parametric confidence intervals for Bland-Altman limits of agreement. Optom. Vis. Sci. 2015, 92, 71–80. [Google Scholar] [CrossRef]
- Brennan, N.A.; Toubouti, Y.M.; Cheng, X.; Bullimore, M.A. Efficacy in Myopia Control. Prog. Retin. Eye Res. 2021, 83, 100923. [Google Scholar] [CrossRef]
- Srivannaboon, S.; Chirapapaisan, C.; Chonpimai, P.; Koodkaew, S. Comparison of ocular biometry and intraocular lens power using a new biometer and a standard biometer. J. Cataract Refract. Surg. 2014, 40, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Garza-Leon, M.; Fuentes-de la Fuente, H.A.; García-Treviño, A.V. Repeatability of ocular biometry with IOLMaster 700 in subjects with clear lens. Int. Ophthalmol. 2017, 37, 1133–1138. [Google Scholar] [CrossRef]
- Zhao, J.; Chen, Z.; Zhou, Z.; Ding, L.; Zhou, X. Evaluation of the repeatability of the Lenstar and comparison with two other non-contact biometric devices in myopes. Clin. Exp. Optom. 2013, 96, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Boyle, A.B.; Namkung, S.; Shew, W.; Gokul, A.; McGhee, C.N.J.; Ziaei, M. Repeatability and agreement of white-to-white measurements between slit-scanning tomography, infrared biometry, dual rotating Scheimpflug camera/Placido disc tomography, and swept source anterior segment optical coherence tomography. PLoS ONE 2021, 16, e0254832. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.S.; Buyse, M. Common pitfalls in statistical analysis: Clinical versus statistical significance. Perspect. Clin. Res. 2015, 6, 169–170. [Google Scholar] [CrossRef]
- Mattern, A.I.; Neller, K.; Devenijn, M.; Schwahn, H.; Langenbucher, A.; Seitz, B.; Kaymak, H. A comparison of optical biometers used in children for myopia control. Klin. Monbl. Augenheilkd. 2023, 240, 1306–1313. [Google Scholar] [CrossRef]
- Pedersen, H.R.; Svarverud, E.; Hagen, L.A.; Gilson, S.J.; Baraas, R.C. Comparing Ocular Biometry and Autorefraction Measurements from the Myopia Master with the IOLMaster 700 and the Huvitz HRK-8000A Autorefractor. Ophthalmic Physiol. Opt. 2023, 43, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Hessler, P.; Künzel, P.; Degle, S. Comparison of three different devices for the evaluation of axial length, refractive error, and keratometry. Optom. Vis. Sci. 2023, 100, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Zhao, Y.; Han, T.; Zhang, X.; Miao, H.; Qin, B.; Zhou, X. Accuracy of axial length, keratometry, and refractive measurement with Myopia Master in children with ametropia. BMC Ophthalmol. 2022, 22, 468. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD | Sw | P | r | CV (%) | ICC (95% CI) | p Value * | ||
|---|---|---|---|---|---|---|---|---|
| MYAH (TOPCON) | ||||||||
| Non-expert observer | AL (mm) | 24.31 ± 1.19 | 0.01 | 0.02 | 0.03 | 0.05 | 1.00 (1.00–1.00) | 0.52 |
| K1 (mm) | 7.85 ± 0.33 | 0.02 | 0.03 | 0.04 | 0.20 | 0.999 (0.998–0.999) | 0.70 | |
| K2 (mm) | 7.70 ± 0.33 | 0.02 | 0.03 | 0.04 | 0.20 | 0.999 (0.998–0.999) | 0.32 | |
| WTW (mm) | 12.09 ± 0.41 | 0.06 | 0.12 | 0.18 | 0.52 | 0.981 (0.968–0.989) | 0.93 | |
| Expert observer | AL (mm) | 24.31 ± 1.19 | 0.01 | 0.02 | 0.03 | 0.05 | 1.00 (1.00–1.00) | 0.11 |
| K1 (mm) | 7.86 ± 0.33 | 0.01 | 0.02 | 0.03 | 0.14 | 0.999 (0.999–1.00) | 0.54 | |
| K2 (mm) | 7.70 ± 0.33 | 0.01 | 0.03 | 0.04 | 0.19 | 0.999 (0.999–0.999) | 0.87 | |
| WTW (mm) | 12.08 ± 0.43 | 0.06 | 0.12 | 0.16 | 0.49 | 0.987 (0.978–0.992) | 0.67 | |
| MYOPIA MASTER (OCULUS) | ||||||||
| Non-expert observer | AL (mm) | 24.31 ± 1.19 | 0.01 | 0.03 | 0.04 | 0.06 | 1.00 (1.00–1.00) | 0.94 |
| K1 (mm) | 7.88 ± 0.33 | 0.01 | 0.02 | 0.03 | 0.12 | 1.00 (0.999–1.00) | 0.22 | |
| K2 (mm) | 7.76 ± 0.34 | 0.02 | 0.03 | 0.04 | 0.19 | 0.999 (0.998–0.999) | 0.19 | |
| WTW (mm) | 11.82 ± 0.42 | 0.05 | 0.11 | 0.15 | 0.46 | 0.984 (0.973–0.991) | 0.18 | |
| Expert observer | AL (mm) | 24.31 ± 1.19 | 0.01 | 0.03 | 0.04 | 0.06 | 1.00 (1.00–1.00) | 0.83 |
| K1 (mm) | 7.88 ± 0.33 | 0.01 | 0.02 | 0.03 | 0.12 | 1.00 (0.999–1.00) | 0.23 | |
| K2 (mm) | 7.76 ± 0.34 | 0.01 | 0.03 | 0.04 | 0.19 | 0.999 (0.998–0.999) | 0.18 | |
| WTW (mm) | 11.83 ± 0.43 | 0.05 | 0.10 | 0.14 | 0.43 | 0.991 (0.985–0.995) | 0.20 | |
| Diff Mean ± SD | LoA 95% | ICC (95% CI) | p Value * | ||
|---|---|---|---|---|---|
| NON-EXPERT OBSERVER | |||||
| MYAH- Myopia Master | AL (mm) | 0.00 ± 0.02 | −0.04 to 0.05 | 1.00 (1.00–1.00) | 0.19 |
| K1 (mm) | −0.03 ± 0.02 | −0.07 to 0.01 | 0.999 (0.998–1.00) | <0.01 | |
| K2 (mm) | −0.06 ± 0.03 | −0.12 to 0.00 | 0.998 (0.997–0.999) | <0.01 | |
| WTW (mm) | 0.28 ± 0.13 | 0.02 to 0.54 | 0.974 (0.951–0.986) | <0.01 | |
| EXPERT OBSERVER | |||||
| MYAH- Myopia Master | AL (mm) | 0.00 ± 0.01 | −0.02 to 0.03 | 1.00 (1.00–1.00) | 0.10 |
| K1 (mm) | −0.03 ± 0.02 | −0.06 to 0.01 | 0.999 (0.999–1.00) | <0.01 | |
| K2 (mm) | −0.06 ± 0.03 | −0.11 to 0.00 | 0.998 (0.997–0.999) | <0.01 | |
| WTW (mm) | 0.25 ± 0.13 | −0.01 to 0.51 | 0.975 (0.954–0.987) | <0.01 | |
| Diff Mean ± SD | LoA 95% | ICC (95% CI) | p Value * | ||
|---|---|---|---|---|---|
| MYAH (TOPCON) | |||||
| Non-expert vs. Expert | AL (mm) | 0.00 ± 0.02 | −0.02 to 0.05 | 1.00 (1.00–1.00) | 0.67 |
| K1 (mm) | −0.01 ± 0.01 | −0.03 to 0.02 | 1.00 (0.999–1.00) | 0.12 | |
| K2 (mm) | 0.00 ± 0.02 | −0.03 to 0.03 | 0.999 (0.999–1.00) | 0.67 | |
| WTW (mm) | 0.01 ± 0.14 | −0.26 to 0.28 | 0.973 (0.950–0.985) | 0.60 | |
| MYOPIA MASTER (OCULUS) | |||||
| Non-expert vs. Expert | AL (mm) | 0.00 ± 0.02 | −0.05 to 0.05 | 1.00 (1.00–1.00) | 0.95 |
| K1 (mm) | 0.00 ± 0.01 | −0.03 to 0.03 | 1.00 (0.999–1.00) | 0.68 | |
| K2 (mm) | 0.00 ± 0.01 | −0.02 to 0.03 | 1.00 (0.999–1.00) | 0.13 | |
| WTW (mm) | −0.01 ± 0.08 | −0.18 to 0.15 | 0.991 (0.982–0.995) | 0.27 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz-Toquero, S.; Sanchez, I.; Gurrea, C.; Recio, A.; Balsa, D.; Martin, R. The Repeatability and Agreement of Ocular Parameters Measured with the MYAH and Myopia Master Devices between Expert and Non-Expert Practitioners. Life 2024, 14, 407. https://doi.org/10.3390/life14030407
Ortiz-Toquero S, Sanchez I, Gurrea C, Recio A, Balsa D, Martin R. The Repeatability and Agreement of Ocular Parameters Measured with the MYAH and Myopia Master Devices between Expert and Non-Expert Practitioners. Life. 2024; 14(3):407. https://doi.org/10.3390/life14030407
Chicago/Turabian StyleOrtiz-Toquero, Sara, Irene Sanchez, Carmen Gurrea, Alba Recio, David Balsa, and Raul Martin. 2024. "The Repeatability and Agreement of Ocular Parameters Measured with the MYAH and Myopia Master Devices between Expert and Non-Expert Practitioners" Life 14, no. 3: 407. https://doi.org/10.3390/life14030407