Interobserver Variability in the Assessment of Tumor Budding in pT 3/4 Colon Cancer: Improvement by Supporting Immunohistochemistry?


Abstract
:1. Introduction
2. Material and Methods
Statistical Analysis
3. Results
3.1. Rating Results
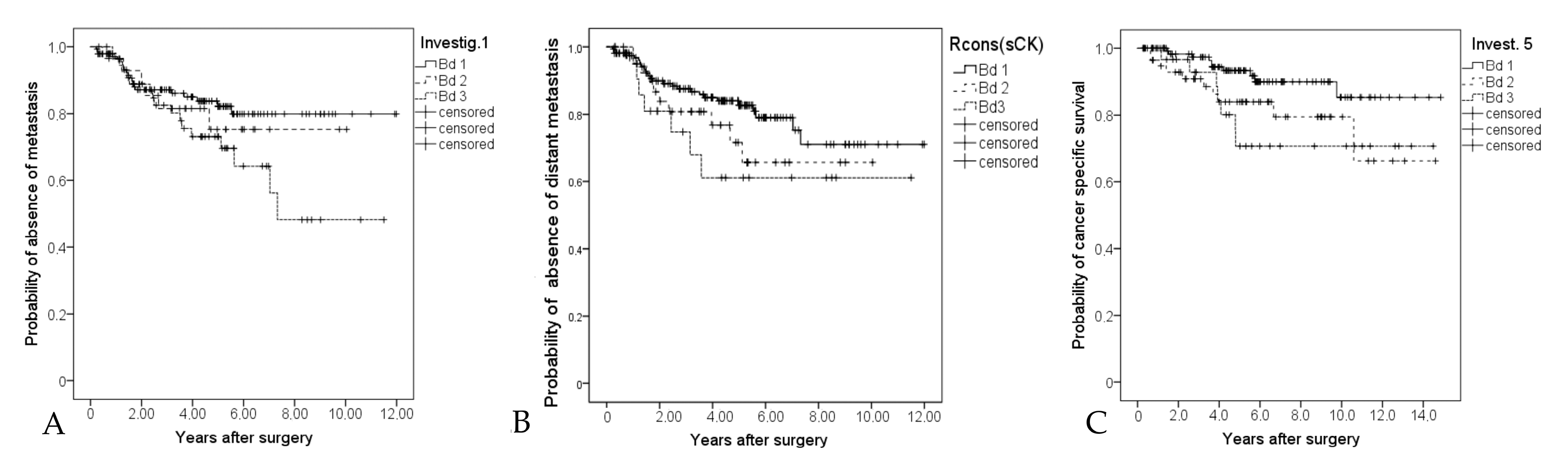
3.2. Prognostic Analyses
4. Discussion
5. Conclusions
Authors Contributions
Funding
Conflicts of Interest
References
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.-F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Dawson, H.; Assarzadegan, N.; Riddell, R.; Kirsch, R.; Blank, A.; Zlobec, I.; Lugli, A. Tumor budding is a strong predictor of disease-free survival in stage II colorectal cancer: Validation study based on the International Tumor Budding Consensus Conference (ITBCC) recommendations. J. Clin. Oncol. 2017, 35, 594. [Google Scholar] [CrossRef]
- Ueno, H.; Ishiguro, M.; Nakatani, E.; Ishikawa, T.; Uetake, H.; Matsuda, C.; Nakamoto, Y.; Kotake, M.; Kurachi, K.; Egawa, T.; et al. Prospective Multicenter Study on the Prognostic and Predictive Impact of Tumor Budding in Stage II Colon Cancer: Results From the SACURA Trial. J. Clin. Oncol. 2019, 37, 1886–1894. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-J.; Kakar, S. Tumor Budding in Colorectal Carcinoma: Translating a Morphologic Score into Clinically Meaningful Results. Arch. Pathol. Lab. Med. 2018, 142, 952–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, B.; Schäfer, E.; Jakubowicz, E.; Mayr, P.; Ihringer, R.; Anthuber, M.; Schenkirsch, G.; Schaller, T.; Märkl, B. Interobserver variability in the H&E-based assessment of tumor budding in pT3/4 colon cancer: Does it affect the prognostic relevance? Virchows Arch. 2018, 473, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Martin, B.; Schäfer, E.; Jakubowicz, E.; Mayr, P.; Ihringer, R.; Anthuber, M.; Schenkirsch, G.; Schaller, T.; Märkl, B. Level of interobserver variability estimation as a valuable tool: Assessment of tumour budding in colon cancer. Histopathology 2018, 73, 864–868. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kai, K.; Aishima, S.; Aoki, S.; Takase, Y.; Uchihashi, K.; Masuda, M.; Nishijima-Matsunobu, A.; Yamamoto, M.; Ide, K.; Nakayama, A.; et al. Cytokeratin immunohistochemistry improves interobserver variability between unskilled pathologists in the evaluation of tumor budding in T1 colorectal cancer. Pathol. Int. 2016, 66, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitrovic, B.; Schaeffer, D.F.; Riddell, R.H.; Kirsch, R. Tumor budding in colorectal carcinoma: Time to take notice. Mod. Pathol. 2012, 25, 1315–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koelzer, V.H.; Zlobec, I.; Berger, M.D.; Cathomas, G.; Dawson, H.; Dirschmid, K.; Hädrich, M.; Inderbitzin, D.; Offner, F.; Puppa, G.; et al. Tumor budding in colorectal cancer revisited: Results of a multicenter interobserver study. Virchows Arch. 2015, 466, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuki, K.; Koyama, F.; Tamura, T.; Enomoto, Y.; Fujii, H.; Mukogawa, T.; Nakagawa, T.; Uchimoto, K.; Nakamura, S.; Nonomura, A.; et al. Prognostic value of immunohistochemical analysis of tumor budding in colorectal carcinoma. Anticancer Res. 2008, 28, 1831–1836. [Google Scholar] [PubMed]
- Okamura, T.; Shimada, Y.; Nogami, H.; Kameyama, H.; Kobayashi, T.; Kosugi, S.; Wakai, T.; Ajioka, Y. Tumor Budding Detection by Immunohistochemical Staining is Not Superior to Hematoxylin and Eosin Staining for Predicting Lymph Node Metastasis in pT1 Colorectal Cancer. Dis. Colon Rectum 2016, 59, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Yamadera, M.; Shinto, E.; Kajiwara, Y.; Mochizuki, S.; Okamoto, K.; Shimazaki, H.; Hase, K.; Ueno, H. Differential clinical impacts of tumour budding evaluated by the use of immunohistochemical and haematoxylin and eosin staining in stage II colorectal cancer. Histopathology 2019, 74, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Bokhorst, J.M.; Blank, A.; Lugli, A.; Zlobec, I.; Dawson, H.; Vieth, M.; Rijstenberg, L.L.; Brockmoeller, S.; Urbanowicz, M.; Flejou, J.F.; et al. Assessment of individual tumor buds using keratin immunohistochemistry: Moderate interobserver agreement suggests a role for machine learning. Mod. Pathol. 2020, 33, 825–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Ciarpaglini, C.; Fernandez-Sellers, C.; Tarazona, N.; Roselló, S.; Huerta, M.; Roda, D.; Mongort, C.; Ferrández, A.; Navarro, S.; Cervantes, A. Improving tumour budding evaluation in colon cancer by extending the assessment area in colectomy specimens. Histopathology 2019, 75, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Takamatsu, M.; Kawachi, H.; Yamamoto, N.; Kobayashi, M.; Toyama, Y.; Maekawa, T.; Chino, A.; Saito, S.; Ueno, M.; Takazawa, Y.; et al. Immunohistochemical evaluation of tumor budding for stratifying T1 colorectal cancer: Optimal cut-off value and a novel computer-assisted semiautomatic method. Mod. Pathol. 2019, 32, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Fauzi, M.F.A.; Chen, W.; Knight, D.; Hampel, H.; Frankel, W.L.; Gurcan, M.N. Tumor Budding Detection System in Whole Slide Pathology Images. J. Med. Syst. 2019, 44, 38. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, R.K.; Klarskov, L.L.; Lippert, M.F.; Novotny, G.W.; Hansen, T.P.; Christensen, I.J.; Høgdall, E.; Riis, L.B. Digital image analysis of pan-cytokeratin stained tumor slides for evaluation of tumor budding in pT1/pT2 colorectal cancer: Results of a feasibility study. Pathol. Res. Pract. 2018, 214, 1273–1281. [Google Scholar] [CrossRef] [PubMed]
- Nearchou, I.P.; Lillard, K.; Gavriel, C.G.; Ueno, H.; Harrison, D.J.; Caie, P.D. Automated Analysis of Lymphocytic Infiltration, Tumor Budding, and Their Spatial Relationship Improves Prognostic Accuracy in Colorectal Cancer. Cancer Immunol. Res. 2019, 7, 609–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Agreement | 6 of 6 | 5 of 6 | 4 of 6 | 3 of 6 | 2 of 6 | ||
|---|---|---|---|---|---|---|---|
| n | 85 | 34 | 60 | 42 | 8 | ||
| % | 37% | 15% | 26% | 18% | 4% | ||
| Kappa values | |||||||
| R1 | R2 | R3 | R5 | R6 | R7 | Rcons (sCK) | |
| I1 | x | 0.27 | 0.18 | 0.29 | 0.31 | 0.45 | 0.5 |
| I2 | 0.27 | x | 0.17 | 0.25 | 0.2 | 0.29 | 0.39 |
| I3 | 0.18 | 0.17 | x | 0.14 | 0.19 | 0.22 | 0.36 |
| I5 | 0.29 | 0.25 | 0.14 | x | 0.21 | 0.39 | 0.53 |
| I6 | 0.31 | 0.2 | 0.19 | 0.21 | x | 0.35 | 0.54 |
| I7 | 0.45 | 0.29 | 0.22 | 0.39 | 0.35 | x | 0.67 |
| Rcons (sCK) | 0.5 | 0.39 | 0.36 | 0.53 | 0.54 | 0.67 | x |
| Mean Bud Count | Bd1 1 | Bd2 1 | Bd3 1 | p | |||||
|---|---|---|---|---|---|---|---|---|---|
| H & E 1 | CK | ||||||||
| 0.785 mm2 | 0.785 mm2 | n | % | n | % | n | % | ||
| Rcons (sCK) | 164 | 43 | 22 | ||||||
| Death | 60 | 37% | 21 | 49% | 12 | 55% | 0.22 | ||
| Cancer-specific death | 17 | 10% | 5 | 12% | 5 | 23% | 0.26 | ||
| Distant metastasis | 27 | 16% | 10 | 23% | 7 | 32% | 0.15 | ||
| Investigator 1 | 4.9 ± 5.8 | 11.2 ± 13.5 | 144 | 29 | 56 | ||||
| Death | 56 | 39% | 13 | 45% | 24 | 43% | 0.72 | ||
| Cancer-specific death | 12 | 8% | 5 | 17% | 10 | 18% | 0.22 | ||
| Distant metastasis | 21 | 15% | 6 | 21% | 17 | 30% | 0.15/0.05 * | ||
| Investigator 2 | 2.9 ± 3.1 | 7.0 ± 5.7 | 154 | 52 | 23 | ||||
| Death | 64 | 42% | 17 | 33% | 12 | 52% | 0.20 | ||
| Cancer-specific death | 17 | 11% | 4 | 8% | 6 | 26% | 0.02 | ||
| Distant metastasis | 31 | 20% | 6 | 12% | 7 | 30% | 0.13/0.04 ° | ||
| Investigator 3 | 2.8 ± 3.4 | 6.6 ± 6.7 | 176 | 48 | 5 | ||||
| Death | 62 | 35% | 29 | 60% | 2 | 40% | 0.01 | ||
| Cancer-specific death | 19 | 11% | 7 | 15% | 1 | 20% | 0.48 | ||
| Distant metastasis | 28 | 16% | 16 | 33% | 0 | 0% | 0.01 | ||
| Investigator 5 | 4.1 ± 4.4 | 11.1 ± 7.5 | 138 | 59 | 32 | ||||
| Death | 50 | 36% | 28 | 47% | 15 | 47% | 0.51 | ||
| Cancer-specific death | 10 | 7% | 10 | 17% | 7 | 22% | 0.05 | ||
| Distant metastasis | 21 | 15% | 11 | 19% | 12 | 38% | 0.01 | ||
| Investigator 6 | 2.7 ± 2.9 | 7.7 ± 5.8 | 167 | 48 | 14 | ||||
| Death | 68 | 41% | 19 | 40% | 6 | 43% | 0.94 | ||
| Cancer-specific death | 18 | 11% | 8 | 17% | 1 | 7% | 0.43 | ||
| Distant metastasis | 32 | 19% | 10 | 21% | 2 | 14% | 0.71 | ||
| Investigator 7 | 4.2 ± 9.5 | 10.1 ± 13.9 | 162 | 30 | 37 | ||||
| Death | 61 | 38% | 15 | 50% | 17 | 46% | 0.30 | ||
| Cancer-specific death | 16 | 10% | 6 | 20% | 5 | 14% | 0.18 | ||
| Distant metastasis | 28 | 17% | 9 | 30% | 7 | 19% | 0.19 | ||
| Range (Q1, Q3) of Bud Counts | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| H & E (0.785 mm2) | CK (0.785 mm2) | |||||||||
| Min | Q1 | Median | Q3 | Max | Min | Q1 | Median | Q3 | Max | |
| Investigator 1 | 0 | 0 | 2 | 9 | 33 | 0 | 2 | 7 | 17 | 76 |
| Investigator 2 | 0 | 0 | 3 | 4 | 12 | 0 | 3 | 6 | 10 | 20 |
| Investigator 3 | 0 | 0 | 2 | 4 | 17 | 0 | 0 | 5 | 10 | 25 |
| Investigator 5 | 0 | 1 | 2 | 6 | 22 | 0 | 5 | 10 | 17 | 26 |
| Investigator 6 | 0 | 0 | 2 | 4 | 12 | 0 | 4 | 6 | 12 | 33 |
| Investigator 7 | 0 | 0 | 0 | 5 | 83 | 0 | 0 | 4 | 17 | 83 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, B.; Mayr, P.; Ihringer, R.; Schäfer, E.-M.; Jakubowicz, E.; Anthuber, M.; Schenkirsch, G.; Schaller, T.; Märkl, B. Interobserver Variability in the Assessment of Tumor Budding in pT 3/4 Colon Cancer: Improvement by Supporting Immunohistochemistry? Diagnostics 2020, 10, 730. https://doi.org/10.3390/diagnostics10090730
Martin B, Mayr P, Ihringer R, Schäfer E-M, Jakubowicz E, Anthuber M, Schenkirsch G, Schaller T, Märkl B. Interobserver Variability in the Assessment of Tumor Budding in pT 3/4 Colon Cancer: Improvement by Supporting Immunohistochemistry? Diagnostics. 2020; 10(9):730. https://doi.org/10.3390/diagnostics10090730
Chicago/Turabian StyleMartin, Benedikt, Patrick Mayr, Regina Ihringer, Eva-Maria Schäfer, Elżbieta Jakubowicz, Matthias Anthuber, Gerhard Schenkirsch, Tina Schaller, and Bruno Märkl. 2020. "Interobserver Variability in the Assessment of Tumor Budding in pT 3/4 Colon Cancer: Improvement by Supporting Immunohistochemistry?" Diagnostics 10, no. 9: 730. https://doi.org/10.3390/diagnostics10090730