
Seven-Month Analysis of Five SARS-CoV-2 Antibody Assay Results after ChAdOx1 nCoV-19 Vaccination: Significant Decrease in SARS-CoV-2 Antibody Titer

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Sample Collection
2.2. Measurement of SARS-CoV-2 Antibodies
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Participants and Samples
3.2. Qualitative Results of the SARS-CoV-2 Antibody Assays after Seven Months
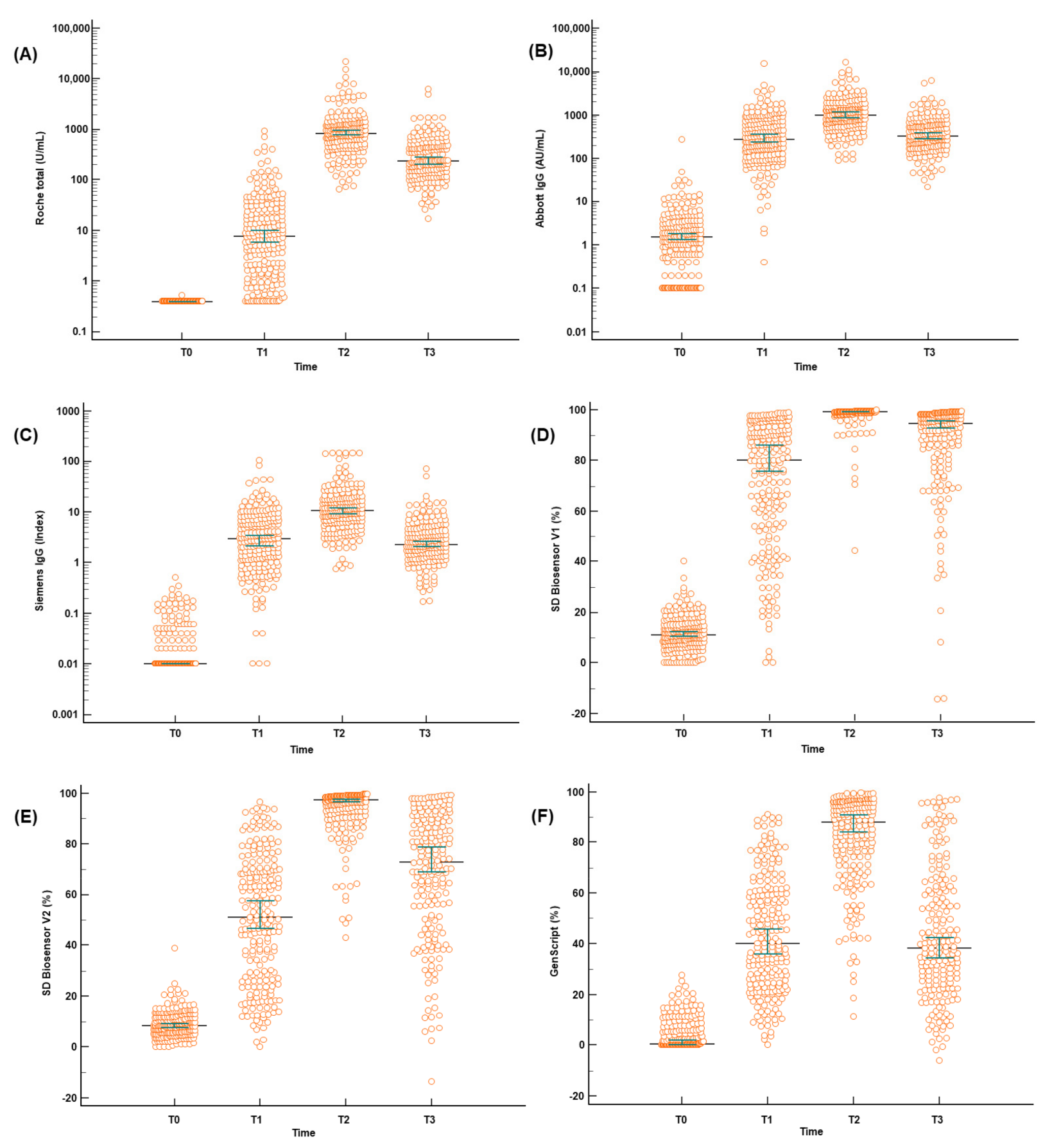
3.3. Quantitative Antibody Results of the SARS-CoV-2 Antibody Assays after Seven Months
3.4. Agreement and Correlation between the SARS-CoV-2 Assays
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pomara, C.; Sessa, F.; Ciaccio, M.; Dieli, F.; Esposito, M.; Giammanco, G.M.; Garozzo, S.F.; Giarratano, A.; Prati, D.; Rappa, F.; et al. COVID-19 Vaccine and Death: Causality Algorithm According to the WHO Eligibility Diagnosis. Diagnostics 2021, 11, 955. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Lee, N.; Lee, S.K.; Cho, E.J.; Hyun, J.; Park, M.J.; Song, W.; Jung, E.J.; Woo, H.; Seo, Y.B.; et al. Comparing Results of Five SARS-CoV-2 Antibody Assays Before and After the First Dose of ChAdOx1 nCoV-19 Vaccine among Health Care Workers. J. Clin. Microbiol. 2021, 59, e01105-21. [Google Scholar] [CrossRef]
- Jeong, S.; Lee, N.; Lee, S.K.; Cho, E.J.; Hyun, J.; Park, M.J.; Song, W.; Jung, E.J.; Woo, H.; Seo, Y.B.; et al. Comparison of the Results of Five SARS-CoV-2 Antibody Assays Before and After the First and Second ChAdOx1 nCoV-19 Vaccinations Among Health Care Workers: A Prospective Multicenter Study. J. Clin. Microbiol. 2021, 59, e01788-21. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Pang, Y.; Lyu, Z.; Wang, R.; Wu, X.; You, C.; Zhao, H.; Manickam, S.; Lester, E.; Wu, T.; et al. The COVID-19 Vaccines: Recent Development, Challenges and Prospects. Vaccines 2021, 9, 349. [Google Scholar] [CrossRef]
- Tsatsakis, A.; Vakonaki, E.; Tzatzarakis, M.; Flamourakis, M.; Nikolouzakis, T.K.; Poulas, K.; Papazoglou, G.; Hatzidaki, E.; Papanikolaou, N.C.; Drakoulis, N.; et al. Immune response (IgG) following full inoculation with BNT162b2 COVID19 mRNA among healthcare professionals. Int. J. Mol. Med. 2021, 48, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Erice, A.; Varillas-Delgado, D.; Caballero, C. Decline of antibody titres 3 months after two doses of BNT162b2 in non-immunocompromised adults. Clin. Microbiol. Infect. 2022, 28, 139.e1–139.e4. [Google Scholar] [CrossRef]
- Favresse, J.; Bayart, J.L.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Wieers, G.; Laurent, C.; Dogne, J.M.; et al. Antibody titres decline 3-month post-vaccination with BNT162b2. Emerg. Microbes Infect. 2021, 10, 1495–1498. [Google Scholar] [CrossRef]
- Terpos, E.; Trougakos, I.P.; Karalis, V.; Ntanasis-Stathopoulos, I.; Gumeni, S.; Apostolakou, F.; Sklirou, A.D.; Gavriatopoulou, M.; Skourti, S.; Kastritis, E.; et al. Kinetics of Anti-SARS-CoV-2 Antibody Responses 3 Months Post Complete Vaccination with BNT162b2; A Prospective Study in 283 Health Workers. Cells 2021, 10, 1942. [Google Scholar] [CrossRef]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef]
- Tre-Hardy, M.; Cupaiolo, R.; Wilmet, A.; Antoine-Moussiaux, T.; Della Vecchia, A.; Horeanga, A.; Papleux, E.; Vekemans, M.; Beukinga, I.; Blairon, L. Six-month interim analysis of ongoing immunogenicity surveillance of the mRNA-1273 vaccine in healthcare workers: A third dose is expected. J. Infect. 2021, 83, 559–564. [Google Scholar] [CrossRef]
- Pegu, A.; O’Connell, S.E.; Schmidt, S.D.; O’Dell, S.; Talana, C.A.; Lai, L.; Albert, J.; Anderson, E.; Bennett, H.; Corbett, K.S.; et al. Durability of mRNA-1273 vaccine-induced antibodies against SARS-CoV-2 variants. Science 2021, 373, 1372–1377. [Google Scholar] [CrossRef]
- Widge, A.T.; Rouphael, N.G.; Jackson, L.A.; Anderson, E.J.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Durability of Responses after SARS-CoV-2 mRNA-1273 Vaccination. N. Engl. J. Med. 2021, 384, 80–82. [Google Scholar] [CrossRef]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef]
- Baraniuk, C. How long does covid-19 immunity last? BMJ 2021, 373, n1605. [Google Scholar] [CrossRef]
- Hung, I.F.N.; Poland, G.A. Single-dose Oxford-AstraZeneca COVID-19 vaccine followed by a 12-week booster. Lancet 2021, 397, 854–855. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-Spike Protein Assays to Determine SARS-CoV-2 Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. Microbiol. Spectr. 2021, 9, e00247-21. [Google Scholar] [CrossRef]
- Premkumar, L.; Segovia-Chumbez, B.; Jadi, R.; Martinez, D.R.; Raut, R.; Markmann, A.; Cornaby, C.; Bartelt, L.; Weiss, S.; Park, Y.; et al. The receptor binding domain of the viral spike protein is an immunodominant and highly specific target of antibodies in SARS-CoV-2 patients. Sci. Immunol. 2020, 5, eabc8413. [Google Scholar] [CrossRef]
- Dolscheid-Pommerich, R.; Bartok, E.; Renn, M.; Kummerer, B.M.; Schulte, B.; Schmithausen, R.M.; Stoffel-Wagner, B.; Streeck, H.; Saschenbrecker, S.; Steinhagen, K.; et al. Correlation between a quantitative anti-SARS-CoV-2 IgG ELISA and neutralization activity. J. Med. Virol. 2022, 94, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.; Ryu, J.H.; Jang, J.H.; Bae, H.; Yoo, S.H.; Choi, A.R.; Jo, S.J.; Lim, J.; Lee, J.; Ryu, H.; et al. Comparison of SARS-CoV-2 Antibody Responses and Seroconversion in COVID-19 Patients Using Twelve Commercial Immunoassays. Ann. Lab. Med. 2021, 41, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Shin, S.; Nam, M.; Hong, Y.J.; Roh, E.Y.; Park, K.U.; Song, E.Y. Performance evaluation of three automated quantitative immunoassays and their correlation with a surrogate virus neutralization test in coronavirus disease 19 patients and pre-pandemic controls. J. Clin. Lab. Anal. 2021, 35, e23921. [Google Scholar] [CrossRef] [PubMed]
- Criscuolo, E.; Diotti, R.A.; Strollo, M.; Rolla, S.; Ambrosi, A.; Locatelli, M.; Burioni, R.; Mancini, N.; Clementi, M.; Clementi, N. Weak correlation between antibody titers and neutralizing activity in sera from SARS-CoV-2 infected subjects. J. Med. Virol. 2021, 93, 2160–2167. [Google Scholar] [CrossRef] [PubMed]
- Muench, P.; Jochum, S.; Wenderoth, V.; Ofenloch-Haehnle, B.; Hombach, M.; Strobl, M.; Sadlowski, H.; Sachse, C.; Torriani, G.; Eckerle, I.; et al. Development and Validation of the Elecsys Anti-SARS-CoV-2 Immunoassay as a Highly Specific Tool for Determining Past Exposure to SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e01694-20. [Google Scholar] [CrossRef] [PubMed]
- Riester, E.; Findeisen, P.; Hegel, J.K.; Kabesch, M.; Ambrosch, A.; Rank, C.M.; Langen, F.; Laengin, T.; Niederhauser, C. Performance evaluation of the Roche Elecsys Anti-SARS-CoV-2 S immunoassay. J. Virol. Methods 2021, 297, 114271. [Google Scholar] [CrossRef]
- Padoan, A.; Bonfante, F.; Pagliari, M.; Bortolami, A.; Negrini, D.; Zuin, S.; Bozzato, D.; Cosma, C.; Sciacovelli, L.; Plebani, M. Analytical and clinical performances of five immunoassays for the detection of SARS-CoV-2 antibodies in comparison with neutralization activity. EBioMedicine 2020, 62, 103101. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Roche Total (%) | Abbott IgG (%) | p-Value | Siemens IgG (%) | p-Value | SD Biosensor (%) | p-Value | GenScript (%) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Before vaccination (n = 228) | 0 (0.0) | 1 (0.4) | 0 (0.0) | 2 (0.9) | 0 (0.0) | ||||
| After the 1st vaccination (n = 228) | 193 (84.6) | 211 (92.5) | 172 (75.4) | 206 (90.7) | 151 (66.2) | ||||
| After the 2nd vaccination (n = 218) | 218 (100.0) | 218 (100.0) | 214 (98.2) | 218 (100.0) | 214 (98.2) | ||||
| After 7 months from the 1st vaccination (n = 200) | 200 (100.0) | 194 (97.0) | 172 (86.0) | 196 (98.0) | 132 (66.0) | ||||
| Sex | 0.240 | 0.232 | 0.378 | 0.123 | |||||
| Male (n = 32) | 32 (100.0) | 30 (93.8) | 30 (93.8) | 32 (100.0) | 25 (78.1) | ||||
| Female (n = 168) | 168 (100.0) | 164 (97.6) | 142 (86.1) | 164 (97.6) | 107 (64.1) | ||||
| Age | 0.930 | 0.391 | 0.864 | 0.261 | |||||
| 21–30 (n = 80) | 80 (100.0) | 78 (97.5) | 67 (85.9) | 78 (97.5) | 48 (60.8) | ||||
| 31–40 (n = 46) | 46 (100.0) | 44 (95.7) | 42 (93.3) | 45 (97.8) | 36 (78.3) | ||||
| 41–50 (n = 44) | 44 (100.0) | 43 (97.7) | 36 (81.8) | 43 (97.7) | 29 (65.9) | ||||
| 51–60 (n = 30) | 30 (100.0) | 29 (96.7) | 27 (90.0) | 30 (100.0) | 19 (63.3) | ||||
| Occupation | 0.899 | 0.650 | 0.532 | 0.508 | |||||
| Doctor (n = 14) | 14 (100.0) | 14 (100.0) | 13 (92.9) | 14 (100.0) | 9 (64.3) | ||||
| Nurse (n = 130) | 3 (100.0) | 126 (96.9) | 109 (85.2) | 126 (96.9) | 82 (63.6) | ||||
| Laboratory technician (n = 54) | 54 (100.0) | 52 (96.3) | 49 (90.7) | 54 (100.0) | 39 (72.2) | ||||
| Others (n = 2) | 2 (100.0) | 2 (100.0) | 1 (100.0) | 2 (100.0) | 2 (100.0) |
| Assays | T0 (n = 228) | Difference between T0 and T1 (n = 228) | T1 (n = 228) | Difference between T1 and T2 (n = 218) | T2 (n = 218) | Difference between T2 and T3 (n = 200) | T3 (n = 200) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Roche total (U/mL) | <0.4 | 7.6 (1.3–26.3) | 8.0 (1.7–26.7) | 840.7 (470.0–1256.9) | 860.5 (485.3–1286.5) | 570.5 (314.0–902.8) | 232.0 (138.0–469.8) | <0.001 |
| Abbott IgG (AU/mL) | 1.5 (0.5–3.3) | 274.8 (113.1–723.7) | 278.4 (114.3–732.8) | 617.1 (168.1–1359.2) | 1041.5 (631.5–1681.9) | 658.9 (365.7–1103.6) | 325.5 (184.8–599.7) | <0.001 |
| Siemens IgG (index) | 0.01 (0.01–0.02) | 2.9 (1.0–7.1) | 3.0 (1.0–7.1) | 6.2 (1.8–14.0) | 10.9 (6.2–17.7) | 8.4 (4.4–14.0) | 2.3 (1.3–4.3) | <0.001 |
| SD Biosensor V1 (%) | 11.2 (7.5–15.4) | 69.1 (41.2–79.3) | 81.1 (55.0–91.9) | 15.9 (6.6-41.2) | 99.5 (98.9–99.6) | 4.8 (1.4–14.0) | 94.7 (85.2–98.2) | <0.001 |
| SD Biosensor V2 (%) | 8.3 (5.4–11.9) | 45.3 (16.4–62.3) | 52.0 (27.8–69.9) | 37.7 (20.6–64.6) | 97.4 (93.0–99.0) | 24.3 (9.3–39.3) | 72.8 (51.3-88.7) | <0.001 |
| GenScript (%) | 0.7 (0.1–7.5) | 37.7 (21.3–56.2) | 40.6 (24.4–59.5) | 37.5 (20.1–59.8) | 88.5 (74.2–95.4) | 40.5 (25.1–51.3) | 38.2 (24.0–61.4) | <0.001 |
| A/B | P/P (n) | P/N (n) | N/P (n) | N/N (n) | Positive Agreement of A to B (%) | Negative Agreement of A to B (%) | Positive Agreement of B to A (%) | Negative Agreement of B to A (%) | Total Agreement (%) | Kappa Value |
|---|---|---|---|---|---|---|---|---|---|---|
| Roche total/Abbott IgG | 602 | 9 | 22 | 239 | 96.5 (94.7–97.8) | 96.4 (93.2–98.3) | 98.5 (97.2–99.3) | 91.6 (87.5–94.6) | 96.4 (95.0–97.6) | 0.91 (0.88–0.94) |
| Roche total/Siemens IgG | 553 | 55 | 5 | 256 | 99.1 (97.9–99.7) | 82.3 (77.6–86.4) | 91.0 (88.4–93.1) | 98.1 (95.6–99.4) | 93.1 (91.2–94.7) | 0.84 (0.81–0.88) |
| Roche total/SD biosensor | 602 | 8 | 20 | 241 | 96.8 (95.1–98.0) | 96.8 (93.8–98.6) | 98.7 (97.4–99.4) | 92.3 (88.4-95.3) | 96.8 (95.4–97.9) | 0.92 (0.89–0.95) |
| Roche total/GenScript | 494 | 116 | 3 | 258 | 99.4 (98.2–99.9) | 69.0 (64.0–73.6) | 81.0 (77.6–84.0) | 98.9 (96.7–99.8) | 86.3 (83.9–88.6) | 0.71 (0.66–0.76) |
| Abbott IgG/Siemens IgG | 621 | 64 | 1 | 241 | 99.8 (99.1–100.0) | 79.0 (74.0–83.4) | 90.7 (88.2–92.7) | 99.6 (97.7–100.0) | 93.0 (91.2–94.5) | 0.83 (0.79–0.87) |
| Abbott IgG/SD biosensor | 623 | 8 | 7 | 241 | 98.9 (97.7–99.6) | 96.8 (93.8–98.6) | 98.7 (97.5–99.5) | 97.2 (94.3–98.9) | 98.3 (97.2–99.0) | 0.96 (0.94–0.98) |
| Abbott IgG/GenScript | 623 | 126 | 0 | 248 | 100.0 (99.4–100.0) | 66.3 (61.3–71.1) | 83.2 (80.3–85.8) | 100.0 (98.5–100.0) | 87.4 (85.1–89.4) | 0.69 (0.64–0.74) |
| Siemens IgG/SD biosensor | 556 | 1 | 63 | 248 | 89.8 (87.2–92.1) | 99.6 (97.8–100.0) | 99.8 (99.0–100.0) | 79.7 (74.8–84.1) | 92.6 (90.7–94.3) | 0.83 (0.79–0.87) |
| Siemens IgG/GenScript | 484 | 74 | 11 | 300 | 97.8 (96.1–98.9) | 80.2 (75.8–84.1) | 86.7 (83.6–89.4) | 96.5 (93.8–98.2) | 90.2 (88.0–92.1) | 0.80 (0.76–0.84) |
| SD biosensor/GenScript | 496 | 125 | 0 | 249 | 100.0 (99.3–100.0) | 66.6 (61.5–71.3) | 79.9 (76.5–83.0) | 100.0 (98.5–100.0) | 85.6 (83.1–87.9) | 0.69 (0.65–0.74) |
| Compared assays | After the First Vaccination (n = 228) | After the Second Vaccination (n = 218) | After 7 Months from the First Vaccination (n = 200) | Total | p-Value |
|---|---|---|---|---|---|
| Roche total/Abbott IgG | 0.808 | 0.919 | 0.907 | 0.884 | <0.001 |
| Roche total/Siemens IgG | 0.803 | 0.933 | 0.917 | 0.876 | <0.001 |
| Roche total/SD Biosensor V1 nAb | 0.781 | 0.568 | 0.857 | 0.928 | <0.001 |
| Roche total/GenScript nAb | 0.803 | 0.840 | 0.790 | 0.878 | <0.001 |
| Abbott IgG/Siemens IgG | 0.947 | 0.975 | 0.980 | 0.976 | <0.001 |
| Abbott IgG/GenScript nAb | 0.848 | 0.868 | 0.817 | 0.924 | <0.001 |
| Abbott IgG/SD Biosensor V1 nAb | 0.854 | 0.579 | 0.846 | 0.905 | <0.001 |
| Siemens IgG/SD Biosensor V1 nAb | 0.845 | 0.594 | 0.861 | 0.906 | <0.001 |
| Siemens IgG/GenScript nAb | 0.845 | 0.871 | 0.819 | 0.932 | <0.001 |
| SD Biosensor V1 nAb/GenScript nAb | 0.905 | 0.628 | 0.892 | 0.928 | <0.001 |
| Vaccine | Number of Participants | Sampling Time | Measurement | Results | Reference |
|---|---|---|---|---|---|
| ChAdOx1 nCoV-19 | 200 | 1, 4, and 7 months after the 1st dose | Roche total Abbott IgG Siemens IgG SD Biosensor nAb GenScript nAb | Roche (U/mL): 8.0→860.5→232.0 Abbott (AU/mL): 278.4→1041.5→325.5 Siemens (index): 3.0→10.9→2.3 SD Biosensor V1 (%): 81.1→99.5→94.7 GenScript (%): 40.6→88.5→38.2 | This study |
| BNT162b2 | 258 | 1.5 and 3 months after the 2nd dose | Architect IgG | Abbott (AU/mL): 9356→3952 | [6] |
| BNT162b2 | 200 | 14, 28, 42, 56, and 90 days after the 1st dose | Roche total | Roche (U/mL): 38.2→2204→1863→1517→1262 | [7] |
| BNT162b2 | 283 | 8, 22, 36, 50 days after the 1st dose 111 days after the 2nd dose | Roche IgG GenScript nAb | Roche (U/mL): <20→2304→1504→761 GenScript nAb (%): 14.3→53.8→97.2→96.3→92.7 | [8] |
| BNT162b2 | 517 | 69 days after the 2nd dose | BIO-SHIELD IgG | BIO-SHIELD (ratio): 4.23 | [5] |
| mRNA-1273 | 33 | 209 days after the 1st dose | RBD ELISA Pseudovirus neutralization Live-virus neutralization | Maximum: 36 to 43 days ELISA (GMT): 92,451 Pseudovirus neutralization (ID50): 80 Live-virus neutralization (ID50): 406 | [9] |
| mRNA-1273 | 201 | 16, 42, 86, and 174 days after the 1st dose | LIAISON IgG | LIAISON (AU/mL): 90.8→>400→>400→221 | [10] |
| mRNA-1273 | 8 | 29, 43, 119, and 209 days after the 1st dose | Pseudovirus neutralization Live-virus neutralization ACE2 competition Cell-surface spike binding S-2P-binding assay RBD-binding assay | Maximum: 43 days (% of detectable antibodies) Pseudovirus neutralization: 25→100→100→88 Live-virus neutralization: 83→100→100→100 ACE2 competition: 100→100→100→100 Cell-surface spike binding: 100→100→100→100 S-2P-binding assay: 100→100→100→100 RBD-binding assay: 100→100→100→100 | [11] |
| mRNA-1273 | 34 | 119 days after the 1st dose | RBD ELISA Pseudovirus neutralization Live-virus neutralization | Maximum: 36 to 43 days ELISA (GMT): 235,228 Pseudovirus neutralization (ID50): 182 Live-virus neutralization (ID50): 775 | [12] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, S.; Lee, N.; Lee, S.-K.; Cho, E.-J.; Hyun, J.; Park, M.-J.; Song, W.; Jung, E.-J.; Woo, H.; Seo, Y.-B.; et al. Seven-Month Analysis of Five SARS-CoV-2 Antibody Assay Results after ChAdOx1 nCoV-19 Vaccination: Significant Decrease in SARS-CoV-2 Antibody Titer. Diagnostics 2022, 12, 85. https://doi.org/10.3390/diagnostics12010085
Jeong S, Lee N, Lee S-K, Cho E-J, Hyun J, Park M-J, Song W, Jung E-J, Woo H, Seo Y-B, et al. Seven-Month Analysis of Five SARS-CoV-2 Antibody Assay Results after ChAdOx1 nCoV-19 Vaccination: Significant Decrease in SARS-CoV-2 Antibody Titer. Diagnostics. 2022; 12(1):85. https://doi.org/10.3390/diagnostics12010085
Chicago/Turabian StyleJeong, Seri, Nuri Lee, Su-Kyung Lee, Eun-Jung Cho, Jungwon Hyun, Min-Jeong Park, Wonkeun Song, Eun-Ju Jung, Heungjeong Woo, Yu-Bin Seo, and et al. 2022. "Seven-Month Analysis of Five SARS-CoV-2 Antibody Assay Results after ChAdOx1 nCoV-19 Vaccination: Significant Decrease in SARS-CoV-2 Antibody Titer" Diagnostics 12, no. 1: 85. https://doi.org/10.3390/diagnostics12010085