
Synovial Fluid Interleukin Levels Cannot Distinguish between Prosthetic Joint Infection and Active Rheumatoid Arthritis after Hip or Knee Arthroplasty

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
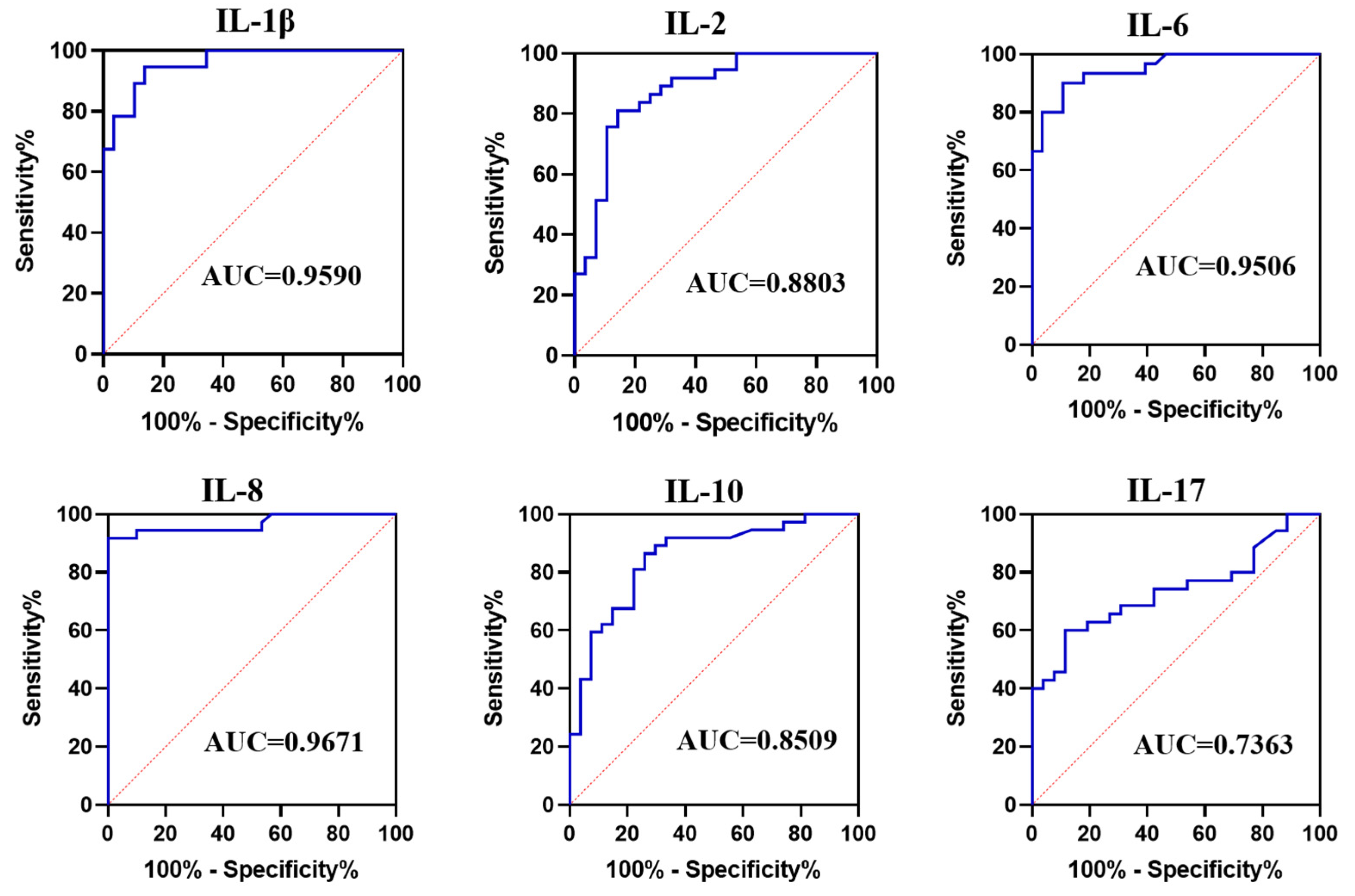
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Drain, N.P.; Bertolini, D.M.; Anthony, A.W.; Feroze, M.W.; Chao, R.; Onyekweli, T.; Longo, S.E.; Hersh, B.; Smith, C.; Rothenberger, S.D.; et al. High Mortality after Total Knee Arthroplasty Periprosthetic Joint Infection is Related to Preoperative Morbidity and the Disease Process but Not Treatment. J. Arthroplast. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, A.; Kolin, D.A.; Farley, K.X.; Wilson, J.M.; McLawhorn, A.S.; Cross, M.B.; Sculco, P.K. Projected Economic Burden of Periprosthetic Joint Infection of the Hip and Knee in the United States. J. Arthroplast. 2021, 36, 1484–1489.e3. [Google Scholar] [CrossRef] [PubMed]
- Keemu, H.; Vaura, F.; Maksimow, A.; Maksimow, M.; Jokela, A.; Hollmén, M.; Mäkelä, K. Novel Biomarkers for Diagnosing Periprosthetic Joint Infection from Synovial Fluid and Serum. JBJS Open Access 2021, 6, e20.00067. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Suh, D.H.; Jafari, S.M.; Mullan, A.; Purtill, J.J. Aseptic loosening of total hip arthroplasty: Infection always should be ruled out. Clin. Orthop. Relat. Res. 2011, 469, 1401–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheok, T.; Smith, T.; Siddiquee, S.; Jennings, M.P.; Jayasekera, N.; Jaarsma, R.L. Synovial fluid calprotectin performs better than synovial fluid polymerase chain reaction and interleukin-6 in the diagnosis of periprosthetic joint infection: A systematic review and meta-analysis. Bone Jt. J. 2022, 104, 311–320. [Google Scholar] [CrossRef]
- Deirmengian, C.; Hallab, N.; Tarabishy, A.; Della Valle, C.; Jacobs, J.J.; Lonner, J.; Booth, R.E., Jr. Synovial fluid biomarkers for periprosthetic infection. Clin. Orthop. Relat. Res. 2010, 468, 2017–2023. [Google Scholar] [CrossRef] [Green Version]
- Sharma, K.; Ivy, M.; Block, D.R.; Abdel, M.P.; Hanssen, A.D.; Beauchamp, C.; Perry, K.I.; Rosemark, C.L.; Greenwood-Quaintance, K.E.; Mandrekar, J.; et al. Comparative analysis of 23 synovial fluid biomarkers for hip and knee periprosthetic joint infection detection. J. Orthop. Res. 2020, 38, 2664–2674. [Google Scholar] [CrossRef]
- Blevins, J.L.; Chiu, Y.F.; Lyman, S.; Goodman, S.M.; Mandl, L.A.; Sculco, P.K.; Figgie, M.P.; McLawhorn, A.S. Comparison of Expectations and Outcomes in Rheumatoid Arthritis versus Osteoarthritis Patients Undergoing Total Knee Arthroplasty. J. Arthroplast. 2019, 34, 1946–1952.e2. [Google Scholar] [CrossRef]
- Müller-Ladner, U.; Ospelt, C.; Gay, S.; Distler, O.; Pap, T. Cells of the synovium in rheumatoid arthritis. Synovial fibroblasts. Arthritis Res. Ther. 2007, 9, 223. [Google Scholar] [CrossRef] [Green Version]
- Ren, Y.; Yang, Q.; Luo, T.; Lin, J.; Jin, J.; Qian, W.; Weng, X.; Feng, B. Better clinical outcome of total knee arthroplasty for rheumatoid arthritis with perioperative glucocorticoids and disease-modifying anti-rheumatic drugs after an average of 11.4-year follow-up. J. Orthop. Surg. Res. 2021, 16, 84. [Google Scholar] [CrossRef] [PubMed]
- Holdren, M.; Schieir, O.; Bartlett, S.J.; Bessette, L.; Boire, G.; Hazlewood, G.; Hitchon, C.A.; Keystone, E.; Tin, D.; Thorne, C.; et al. Improvements in Fatigue Lag behind Disease Remission in Early Rheumatoid Arthritis: Results from the Canadian Early Arthritis Cohort. Arthritis Rheumatol. 2021, 73, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Li, X.; Wang, J.; Gong, X.; Hu, N.; Huang, W. Improved diagnosis of chronic hip and knee prosthetic joint infection using combined serum and synovial IL-6 tests. Bone Jt. Res. 2020, 9, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Gehrke, T. Definition of periprosthetic joint infection. J. Arthroplast. 2014, 29, 1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mucke, J.; Krusche, M.; Burmester, G.R. A broad look into the future of rheumatoid arthritis. Ther. Adv. Musculoskelet Dis. 2022, 14, 1–8. [Google Scholar] [CrossRef]
- Goodman, S.M. Rheumatoid arthritis: Perioperative management of biologics and DMARDs. Semin. Arthritis Rheum. 2015, 44, 627–632. [Google Scholar] [CrossRef]
- Goodman, S.M.; Menon, I.; Christos, P.J.; Smethurst, R.; Bykerk, V.P. Management of perioperative tumour necrosis factor α inhibitors in rheumatoid arthritis patients undergoing arthroplasty: A systematic review and meta-analysis. Rheumatology 2016, 55, 573–582. [Google Scholar] [CrossRef] [Green Version]
- Bernatsky, S.; Hudson, M.; Suissa, S. Anti-rheumatic drug use and risk of serious infections in rheumatoid arthritis. Rheumatology 2007, 46, 1157–1160. [Google Scholar] [CrossRef] [Green Version]
- Vakharia, R.M.; Vakharia, A.M.; Ehiorobo, J.O.; Swiggett, S.J.; Mont, M.A.; Roche, M.W. Rheumatoid Arthritis Is Associated with Thromboembolic Complications following Primary Total Knee Arthroplasty. J. Arthroplast. 2020, 35, 1009–1013. [Google Scholar] [CrossRef]
- Horowitz, J.A.; Puvanesarajah, V.; Jain, A.; Li, X.J.; Shimer, A.L.; Shen, F.H.; Hassanzadeh, H. Rheumatoid Arthritis Is Associated with an Increased Risk of Postoperative Infection and Revision Surgery in Elderly Patients Undergoing Anterior Cervical Fusion. Spine 2018, 43, E1040–E1044. [Google Scholar] [CrossRef]
- Brocker, C.; Thompson, D.; Matsumoto, A.; Nebert, D.W.; Vasiliou, V. Evolutionary divergence and functions of the human interleukin (IL) gene family. Hum. Genom. 2010, 5, 30–55. [Google Scholar] [CrossRef] [PubMed]
- Elgeidi, A.; Elganainy, A.E.; Abou Elkhier, N.; Rakha, S. Interleukin-6 and other inflammatory markers in diagnosis of periprosthetic joint infection. Int. Orthop. 2014, 38, 2591–2595. [Google Scholar] [CrossRef] [PubMed]
- Kuo, F.C.; Lu, Y.D.; Wu, C.T.; You, H.L.; Lee, G.B.; Lee, M.S. Comparison of molecular diagnosis with serum markers and synovial fluid analysis in patients with prosthetic joint infection. Bone Jt. J. 2018, 100-B, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Gallo, J.; Svoboda, M.; Zapletalova, J.; Proskova, J.; Juranova, J. Serum IL-6 in combination with synovial IL-6/CRP shows excellent diagnostic power to detect hip and knee prosthetic joint infection. PLoS ONE 2018, 13, e0199226. [Google Scholar] [CrossRef]
- Randau, T.M.; Friedrich, M.J.; Wimmer, M.D.; Reichert, B.; Kuberra, D.; Stoffel-Wagner, B.; Limmer, A.; Wirtz, D.C.; Gravius, S. Interleukin-6 in serum and in synovial fluid enhances the differentiation between periprosthetic joint infection and aseptic loosening. PLoS ONE 2014, 9, e89045. [Google Scholar] [CrossRef]
- Cornet, E.; Behier, C.; Troussard, X. Guidance for storing blood samples in laboratories performing complete blood count with differential. Int. J. Lab. Hematol. 2012, 34, 655–660. [Google Scholar] [CrossRef]
- Hennø, L.T.; Storjord, E.; Christiansen, D.; Bergseth, G.; Ludviksen, J.K.; Fure, H.; Barene, S.; Nielsen, E.W.; Mollnes, T.E.; Brekke, O.L. Effect of the anticoagulant, storage time and temperature of blood samples on the concentrations of 27 multiplex assayed cytokines—Consequences for defining reference values in healthy humans. Cytokine 2017, 97, 86–95. [Google Scholar] [CrossRef] [Green Version]
- Bottini, N.; Firestein, G.S. Duality of fibroblast-like synoviocytes in RA: Passive responders and imprinted aggressors. Nat. Rev. Rheumatol. 2013, 9, 24–33. [Google Scholar] [CrossRef] [Green Version]
- Falconer, J.; Murphy, A.N.; Young, S.P.; Clark, A.R.; Tiziani, S.; Guma, M.; Buckley, C.D. Review: Synovial Cell Metabolism and Chronic Inflammation in Rheumatoid Arthritis. Arthritis Rheumatol. 2018, 70, 984–999. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Group A (N = 39) | Group B (N = 26) | Group C (N = 37) | P1-Value | P2-Value |
|---|---|---|---|---|---|
| Sex | 0.9999 * | 0.0003 * | |||
| Male | 17 (43.6%) | 3 (12.5%) | 16 (43.2%) | Male | |
| Female | 22 (56.4%) | 23 (88.5%) | 21 (56.8%) | ||
| Joint type | 0.2509 * | <0.0001 * | |||
| Knee | 16 (41.03%) | 26 (100%) | 21 (56.8%) | ||
| Hip | 23 (58.97%) | NA | 16 (43.2%) | ||
| Age, (yr) | 62.0 ± 8.386 | 55.8 ± 4.763 | 64.9 ± 6.817 | 0.1300 # | 0.0047 # |
| BMI, (kg/m2) | 24.04 ± 3.350 | 22.68 ± 2.278 | 23.65 ± 3.044 | 0.6041 # | 0.0998 # |
| Comorbidities (n) | |||||
| Hypertension | 15 | 7 | 21 | ||
| Diabetes | 8 | 5 | 17 | ||
| Cardiovascular disease | 2 | 0 | 4 |
| Markers | Cut-Off Value (pg/mL) | AUC (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|
| IL-1β | 71.03 | 0.9590 (0.9184 to 0.9995) | 94.59 (82.30% to 99.04%) | 86.21 (69.44% to 94.50%) |
| IL-2 | 6.50 | 0.8803 (0.7945 to 0.9661) | 81.08 (65.80% to 90.52%) | 85.71 (68.51% to 94.30%) |
| IL-6 | 1327 | 0.9506 (0.9009 to 1.000) | 90.00 (74.38% to 96.54%) | 89.29 (72.80% to 96.29%) |
| IL-8 | 1033 | 0.9616 (0.9172 to 1.000) | 86.11 (71.34% to 93.92%) | 100.0 (88.65% to 100.0%) |
| IL-10 | 1.48 | 0.8509 (0.7553 to 0.9464) | 86.49 (72.02% to 94.09%) | 74.07 (55.32% to 86.83%) |
| IL-17 | 2.95 | 0.7363 (0.6117 to 0.8609) | 60.00 (43.57% to 74.45%) | 88.46 (71.02% to 96.00%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, L.; Du, C.; Yang, J.; Wang, H.; Su, X.; Wei, L.; Zhao, C.; Chen, C.; Chen, H.; Hu, N.; et al. Synovial Fluid Interleukin Levels Cannot Distinguish between Prosthetic Joint Infection and Active Rheumatoid Arthritis after Hip or Knee Arthroplasty. Diagnostics 2022, 12, 1196. https://doi.org/10.3390/diagnostics12051196
Qin L, Du C, Yang J, Wang H, Su X, Wei L, Zhao C, Chen C, Chen H, Hu N, et al. Synovial Fluid Interleukin Levels Cannot Distinguish between Prosthetic Joint Infection and Active Rheumatoid Arthritis after Hip or Knee Arthroplasty. Diagnostics. 2022; 12(5):1196. https://doi.org/10.3390/diagnostics12051196
Chicago/Turabian StyleQin, Leilei, Chengcheng Du, Jianye Yang, Hai Wang, Xudong Su, Li Wei, Chen Zhao, Cheng Chen, Hong Chen, Ning Hu, and et al. 2022. "Synovial Fluid Interleukin Levels Cannot Distinguish between Prosthetic Joint Infection and Active Rheumatoid Arthritis after Hip or Knee Arthroplasty" Diagnostics 12, no. 5: 1196. https://doi.org/10.3390/diagnostics12051196