
Recent Advances in the Diagnosis of Enamel Cracks: A Narrative Review


Restorative Dentistry Department, King Abdulaziz University, P.O. Box 80209, Jeddah 21589, Saudi Arabia
Diagnostics 2022, 12(8), 2027; https://doi.org/10.3390/diagnostics12082027
Submission received: 31 May 2022
/
Revised: 8 August 2022
/
Accepted: 13 August 2022
/
Published: 22 August 2022
(This article belongs to the Special Issue Current Concepts and Prospects of Diagnostics in Oral Diseases)
Abstract
:Cracked teeth can pose a diagnostic dilemma for a clinician as they can mimic several other conditions. The constant physiological stress along with any pathological strain like trauma or iatrogenic causes can lead to the development of microcracks in the teeth. Constant exposure to immense stress can cause the progression of these often-undiagnosed tooth cracks to cause tooth fractures. This review aims to outline the etiology of tooth cracks, their classification, and recent advances in the diagnosis of enamel cracks. Diagnosing a cracked tooth can be an arduous task as symptoms differ according to the location and extension of the incomplete fracture. Early detection is critical because restorative treatment can prevent fracture propagation, microleakage, pulpal or periodontal tissue involvement, and catastrophic cusp failure. Older methods of crack detection are not sensitive or specific. They include clinical examination, visual inspection, exploratory excavation, and percussion test. The dye test used blue or gentian violet stains to highlight fracture lines. Modern methods include transillumination, optical coherence tomography Swept-Source Optical Coherence Tomography (SSOCT), near-infrared imaging, ultrasonic system, infrared thermography, and near-infrared laser. These methods appear to be more efficacious than traditional clinical dental imaging techniques in detecting longitudinal tooth cracks. Clinically distinguishing between the various types of cracks can be difficult with patient-reported signs and symptoms varying according to the location and extension of the incomplete fracture. Cracks are more common in restored teeth. Technological advances such as transillumination allow for early detection and enhanced prognosis.
1. Introduction
A cracked tooth refers to a partial enamel rupture in a living tooth with dentinal and even pulpal involvement [1]. The causative factors of a tooth crack vary. A masticatory function is the most common factor related to vertical tooth fracture [2]. Depending on the crack’s extension depth and subsequent bacterial infections, cracked teeth can cause several clinical symptoms [3]. Typical symptoms include acute pain on chewing or unexplained pain as a result of exposure to a cold stimulus [4]. An incidence rate of 34–74% has been reported in adults between the ages of 30–50 [5], with a female predisposition [6,7]. The probability of a cracked tooth is higher in an aging population with a greater number of retained teeth [8]. There is an increase in the mineral density of enamel with aging. This is concurrent with a decrease in the volume of the protein matrix [9]. Cosmetic procedures such as bleaching can accelerate this deterioration in fracture toughness and mechanical properties of the enamel [10,11].
The mandibular molars are more susceptible to enamel fractures. Fractured enamel is more prevalent in the upper and lower bicuspids as well as the upper molar teeth [7]. The mesiopalatal cusp of the upper first grinder is quite protuberant. This creates wedging on the first mandibular grinders, which might also contribute to tooth cracks [12]. As a consequence, these teeth are more liable to fracture. Diagnosing a cracked tooth can be an arduous task for a clinician as its symptoms can be variable and bizarre [13]. The cracks will continue to spread if prompt treatment is not given. This can eventually lead to pulpitis or a complete tooth fracture [14]. The primary objective of its diagnosis is early detection. Visual inspection [15], periodontal probing, bite diagnosis, pulp vitality test [16], staining [17], transillumination [18], and computed tomography (CT) [19] were the most common clinical diagnosis methods. Surface crack detection methods such as optical coherence tomography (OCT) have recently attracted a lot of attention [20,21]. Cone-beam computed tomography (CBCT) and Micro-CT appeared to be more efficacious than traditional clinical dental imaging techniques in detecting longitudinal tooth cracks [22,23]. This paper aims to outline the cracked tooth syndrome, diagnostic methods used over the years, and the recent advances in diagnosis.
2. Clinical Features
The clinical symptoms differ according to the location and extension of the incomplete fracture [12,24,25]. It is possible to elicit a history of months of discomfort and acute pain while chewing or consuming cold beverages. “Rebound pain” or pain that occurs when pressure is released after eating fibrous foods is frequently observed. Patients may not be able to identify the tooth where the pain is felt. They may report a negative response to heat stimuli.
Microleakage of bacterial byproducts and toxins can cause chronic pulpitis without causing clinical symptoms. Pulpal and periodontal symptoms may develop from cracks with pulpal involvement [26,27].
The physiological basis of chewing pain as proposed by Brannstrom and Astrom [28] states that the independent movement of the fractured tooth part with each other could cause a sudden transition in the fluids within the dentinal tubules. Subsequently, the A-type fibers get activated in the dental pulp leading to immediate pain. The toxic irritants may leak via the cracks producing hypersensitivity to cold. The release of neuropeptides as a result of the toxic irritant leakage within the dental pulp leads to a decreased pain threshold. These symptoms occur because of alternate compression and stretching of the odontoblast processes inside the crack.
Asymptomatic enamel cracks can have multiple pathogenic consequences. Teeth with enamel cracks may be further damaged by ultrasonic instrumentation such as scaling and root planing [29].
3. Difference between a Fractured Cusp or a Split Tooth and a Cracked Tooth
A cracked tooth can be differentiated from a split tooth by checking the movements of the segment by wedging. A cracked tooth demonstrates no movement with wedging pressures. Under light pressure, a split tooth may break off, leaving patients with no further mobility. Under wedging stresses, a fractured cusp will display mobility and the mobile part will extend deep beyond the cementoenamel junction. Postoperative sensitivity as a result of broken restoration, areas of hyper occlusion due to dental restoration, microleakage from newly filled composite resin restorations, orofacial pain, and bruxism pain, can all be considered as a cracked tooth [30].
4. Causes of Enamel Cracks and Identification
The sources and causes of enamel cracks are multifactorial. They can develop glacially over a long time period. Enamel cracks can exist independent of dentin cracks. The pain from a cracked tooth can be difficult to distinguish from other conditions such as ear pain, atypical orofacial pain, migraine, sinusitis, or temporomandibular joint disorders. As a consequence, diagnosis may be clinically challenging and delayed. Early detection is critical because restorative treatment can prevent fracture propagation, microleakage, pulpal or periodontal tissue involvement, and catastrophic cusp failure [31].
The ease at which a fracture can be diagnosed varies depending on its location and extent. An extensive intracoronal repair is usually present on the tooth. Humans uniquely consume both hot and cold food, leading to repeated thermal changes that can cause expansion and contraction [32]. This is particularly relevant in the case of teeth restored with ceramics where thermal expansion and cyclic loading can lead to crack formation and propagation. Microscopic cracks at the edges of a restoration can indicate structural weakness [18]. Cracks at the margins of composite restorations may be due to polymerization contraction stress. It can present as a whitish margin [33]. Well-defined discoloration of a cusp can be a sign of a lack of structural integrity [18]. Pain can arise after dental procedures, such as the cementation of an inlay, and is often misdiagnosed to be due to the high spots on the recent restoration. The presence of underlying cracks could be indicated by regularly debonding the cemented intracoronal restorations like inlays.
5. Classification/Definitions of Tooth Fracture
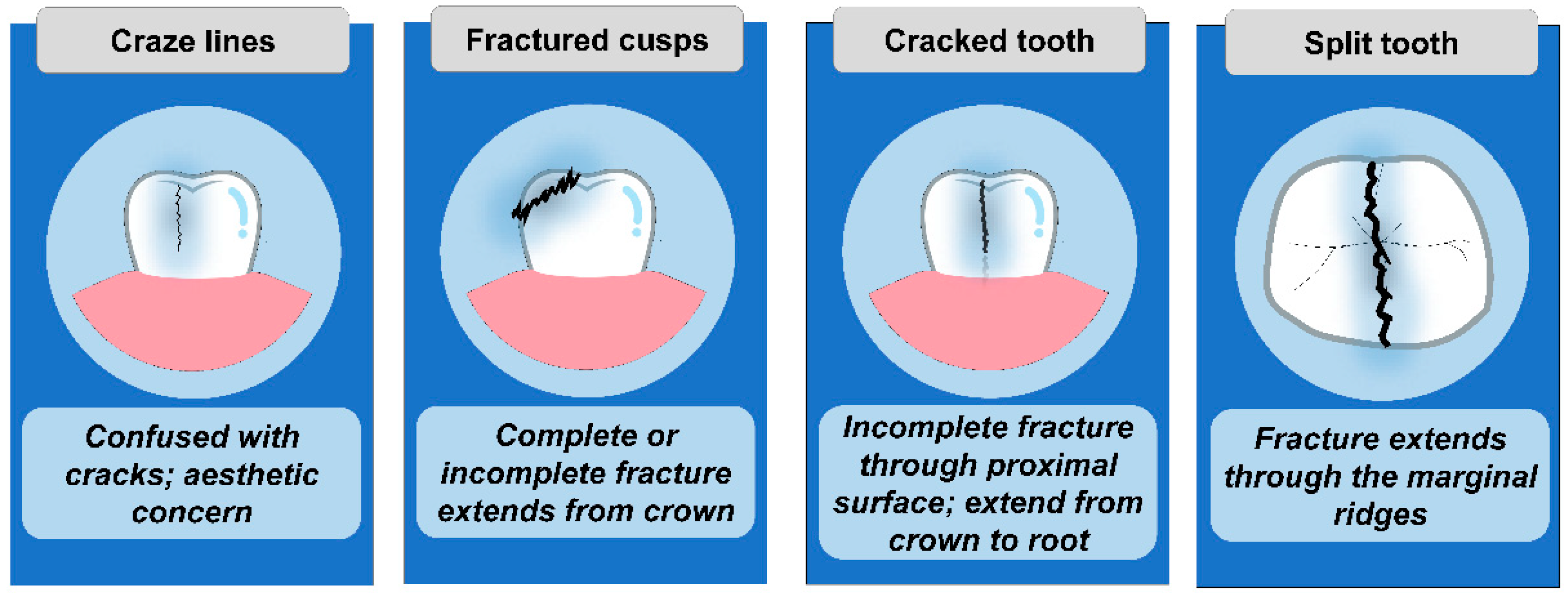
The American Association of Endodontists has divided longitudinal tooth fractures into five classes: craze line, fractured cusp, cracked tooth, split tooth, and vertical root fracture [34]. An asymptomatic crack in the tooth enamel may progress along with dentin cracks. Clinically distinguishing between the various types of cracks can be difficult (Figure 1).
Cracked tooth syndrome includes three phases:
- Craze Lines: Tiny and harmless cracks that occur in the outer enamel of the tooth.
- Cracks: It occurs when craze lines penetrate the body of the tooth (dentin).
- Fractures: A fracture occurs when cracks expand deep into the root of the tooth.
Craze lines are asymptomatic superficial lines that appear on enamel with age. They are frequently confused with cracks but can be distinguished with transillumination. Fractured cusps initiate from the coronal tooth portion, progress into the dentinal area, and end cervically. They are generally connected with large restorations that leave the cuspal enamel unsupported. A cracked tooth is defined as one that extends apically from the crown of the tooth without separating two segments, according to the AAE. A split tooth has a breakthrough both marginal ridges, totally dividing the tooth into two halves. Vertical root fractures begin from the root and are usually complete or partial. All classification methods have the difficulty of failing to relate the descriptions to clinical outcomes or treatment recommendations.
A tooth fracture was divided into two types by Silvestri and Singh (1978): complete and incompletely fractured teeth [35]. Complete fractures were then separated into vertically directed and obliquely directed complete fractures. The authors believe that the full oblique fracture occurs most frequently as a result of a thorough restoration that undermines a cusp. The undermined cusp fractures off under the stresses of physiological functions. A vertically oriented complete fracture is seen as two individual mobile tooth and root segments in relation to one another. The incomplete tooth fractures are of two types: vertical and oblique. An oblique crack originates on the occlusal surface of the tooth, involves one or few cusps, extends through the dentin in an oblique direction beneath the cusps, and ends gingivally in the cementum or enamel. Tooth segments are not completely crushed. Vertical incomplete fractures start in the enamel and extend through the dentin and the root progress. With no complete separation of segments, the crack might involve one or both the marginal ridges extending in the mesiodistal direction. Figure 2 depicts a more detailed classification scheme, and was created by Talim and Gohil (1974): [36].
6. Early Methods of Diagnosing Enamel Crack
6.1. Clinical Examination
Careful clinical examination can visualize localized periodontal defects (subgingival cracks), facets on the occlusal surface of the tooth, and positive response to thermal or sweet stimuli. Once the tooth has been located, many authors recommend removing old restorations and stains to view the cracks. Rubber dam usage has the advantage of detecting the cracks more easily by keeping the tooth surface free of saliva, highlighting the crack with a clear background and preventing the interference of surrounding structures.
6.2. Visual Inspection
Visual inspection is inherently limited. Traditional visualization may not be sensitive enough to assess the presence or severity of the cracks. Although visual examination of the tooth is beneficial, cracks cannot be visualized without magnifying loupes. While it can be identified, it is not always obvious. Once the tooth has been located, many authors recommend removing old restorations and stains to aid in the visualization of the crack [37,38,39,40,41].
6.3. Exploratory Excavation
It is often difficult to find the crack beneath the removed restoration, therefore the tooth should be further excavated with the consent of the patient.
6.4. Percussion Test
The cracked tooth could be diagnosed with a positive response to apical percussion.
6.5. Periodontal Probing
The cracked tooth can be differentiated from the split tooth using periodontal probing when the line of fracture progresses beyond the gingiva. Careful probing of suspected cracks is required to reveal a periodontal pocket. Deep probing, conversely, frequently helps in the diagnosis of a split tooth, which indicates a poor prognosis.
6.6. Dye Test
Fracture lines can be highlighted with methylene blue or gentian violet stains [42]. This is due to the dye’s tendency for aggregation. However, using the dye may hide cracks or cause slight color changes in the enamel’s deeper layers [18]. In addition, the original restorative elements must be excavated before dye application, which takes 2–5 days [43]. Another problem is that a permanent aesthetic restoration is not feasible.
6.7. Transillumination
Transillumination is a useful tool for locating tooth cracks [44]. The tooth must be cleansed before transillumination, and the light source must be held above the tooth. The presence of any crack penetrating the tooth dentin will derange the transmission of light [45]. For traditional crack diagnosis, transillumination is the frequent method used (Figure 3). The use of transillumination without magnification has two disadvantages. Transillumination, for starters, causes the craze lines to give the impression of physical fractures. Additionally, the minor color shift is undetectable. The use of magnification and fiber-optic transillumination will aid in the visualization of a crack. The detected cracks, do not precisely signify the extent and form of the cracks [46].
The intensification to determine its spectrum averages from 14–18×. As per experienced clinicians, 16 times seems to be the ideal magnification [47]. The minor cracks can be properly detected using the fiber-optic transillumination equipment and the dental microscope. These are widely used as effective diagnostic tools in clinical practice.
Transillumination combined with methylene blue allows better discrimination of enamel cracks than either modality alone [40].
6.8. Bite Tests
Bite testing is performed using cotton wool rolls, orangewood sticks, rubber coarse rolls, or a 10-number round bur in a cellophane tape grip. The subject is instructed to close his mouth on an individual cusp while using wooden sticks, thereby aiding fracture cusp isolation. Cracks can be detected using cotton rolls. The subject is asked to close his mouth on the roll before suddenly releasing the pressure. The presence of pain upon sudden pressure release confirms the diagnosis. Other devices like Tooth Slooth II (Professional Results Inc., Laguna Niguel, CA, USA) and Fractfinder (Denbur, Oak Brook, IL, USA) are said to have a higher level of sensitivity when compared to wooden sticks. These along with rubber plungers of numbing ampules adjourned on a dental floss are utilized in the same way as cotton rolls. Investigation is confirmed when there is aching on sudden pressure retrieval. It aids in the correct identification of the cusp in concern. The majority of vitality tests are positive. However, due to the existing pulpitis, the affected teeth show hypersensitivity to cold stimuli. This characteristic may establish confirmation of the cracked tooth. Other researchers however believe that putting pressure on the teeth with questionable symptoms may extend the crack propagation, and hence do not recommend bite testing [13].
6.9. Radiograph
Radiographs can help to determine the overall tooth status, however, a crack is seldom seen on one [39,41,48,49]. Research has shown that conventional radiography such as bitewing imaging shows poor accuracy in crack detection [50]. Conventional periapical X-rays (PR) can be recommended when a root fracture is deviated [51], however, cone-beam computed tomography (CBCT) can identify minor periapical bone loss during vertical root fractures (VRFs) [52]. However, because CBCT has a resolution of just about 80 μm, the diagnosis of cracked teeth or detection of vertical root fractures becomes difficult [53,54].
7. Recent Advances in Diagnosing Enamel Cracks
7.1. Swept-Source Optical Coherence Tomography (SSOCT)
Optical coherence tomography is a cross-sectional diagnostic method that helps to envision optical characteristics of biological tissues. Its principle is identical to that of ultrasonic pulse-echo imaging, in which it utilizes infrared waves which reflect the internal microstructure [57,58]. Swept-source optical coherence tomography (SS-OCT) is highly sensitive [59,60,61]. It is an improvement over traditional CT for detecting cracked teeth and incipient enamel caries [62,63,64]. It allows for the construction of cross-sectional images of internal biologic structures [65]. It may also have applications in the diagnosis of restorative failures in the future [66,67]. SSOCT is a modification of the Fourier domain techniques that offer a discrete rise in sensitivity in comparison to the traditional optical coherence tomography techniques [68].
Literature suggests that a wavelength of light in the infrared region (700 to 1550 nm) shows tremendous scope for enamel imaging due to the mild absorption and scattering in this range of light [61,69]. SS-OCT uses a laser of suitable frequency to emit multiple wavelengths of light (near-infrared wavelength of 1300 nm [70]. Using SS-OCT, the enamel is highly transparent and any cracks present are revealed with good contrast [71]. With the help of a laser scanning device and a semiconductor camera, this imaging approach uses low-consistent interferometry for capturing the reflected waves of biostructures at varying pits facing weak coherent light. It creates two or three-dimensional mechanical structures [72,73]. SS-OCT has higher diagnostic accuracy than microCT, FOTI, and visual inspection [20,66].
Although SS-OCT increases resolution, it shows low specificity for sensing full-thickness cracks as the improved image of deep fractures frequently intersects the enamel plexus. Cracks extending beyond the amelodentinal junction can also be imaged using the SS-OTC, thus serving in the evaluation of the crack depth. The coronal section of the SS-OCT shows a narrowed abyss of penetration of 3 mm that can be laser irradiated. As a result, its primary applications are limited to confirmation of the initial investigation [21,66].
SS-OCT pictures reveal fracture lines and mechanical fractures. It can detect vertical fractures in extracted human teeth [74,75]. However, this detection is restricted only to the coronal area where the laser beam is irradiated. Its detection abilities are comparable to micro-CT (100%) and transillumination [20]. It can detect a whole-thickness enamel crack with the location of the crack showing light backscattering. Enamel thickness varies at different sections in a tooth. This non-uniform composition and the surface roughness have an influence on penetration depth and image contrast of SS-OCT. With the Swept-Source Optical Coherence Tomography, a longer wavelength may be used to increase the penetration dep. However, this lowers the axial resolution in the cross-section which in turn causes a struggle with crack detection [73].
7.2. Near-Infrared Imaging
Near-infrared transillumination is a recent diagnostic modality for enamel cracks [73,76,77]. Imaging with the long wavelengths of 1300–1700 nm of near-infrared illumination gives the greatest contrast between enamel and dentine [78]. Near-infrared imaging is capable of detecting of several cracks. However, it does not provide information about the precise depth of the crack nor can it differentiate between the different types of cracks [21,44]. This technique was developed to overcome the limitation of insufficient scanning range of the Swept-Source Optical Coherence Tomography [79,80]. In the Swept-Source Optical Coherence Tomography, a whole lesion scan is time-consuming and requires the patient to be immobilized during the scanning. Any movement can hamper the image quality and lead to motion-related artifacts [81,82]. Near-infrared imaging has the advantage of rapid screening of the disease region over the Swept-Source Optical Coherence Tomography
Near-infrared fluorescence (ICG-NIRF) dental imaging offers a solution for detecting cracks extending into enamel or dentine [83]. While CT scans can reveal dentin cracks, NIR images can reveal most enamel flaws that are invisible on X-ray imaging. The direction of light is a key component in the detection of a fracture: an angled exposure produced better image contrast of cracks than a parallel exposure because a shadow is produced beneath the line. The line shadow in ICG-NIRF and NIRi-II images could be used to measure the depth of the line and differentiate dentino-enamel cracks from craze lines using this shadow. ICG-NIRF images with 1-min ICG tooth immersion revealed cracks clearly, though extended ICG immersion gave images better contrast.
The quantitative light-induced fluorescence (QLF) quantifies the percentage of fluorescence change of demineralized enamel in comparison to the adjacent enamel. It is related directly to the quantity of mineral lost at the time of demineralization [84]. Jun MK examined the effectiveness of quantitative light-induced fluorescence (QLF) technology in the identification of enamel cracks on 96 human extracted teeth using blue light of wavelength 405 nm. This light is known to approach dentine beneath the enamel causing tooth fluorescence. In case of an existing lesion, some light gets shielded and portrayed as a dark area [85]. A strong correlation was seen between the histologic evaluation and the maximum fluorescence lost (F max) value, with a correlation coefficient of 0.84. It was found that for enamel inner-half cracks, QLF-D had a sensitivity of 0.87 and a specificity of 0.98, whereas cracks entering the dentino-enamel junction had a sensitivity of 0.90 and a specificity of 1.0. This suggests that QLF technology could be a valuable clinical tool in identifying enamel defects, particularly because it is nondestructive.
7.3. Cone-Beam Computed Tomography (CBCT)
Contrast-enhanced cone-beam computed tomography (CBCT) was utilized by Zhou J et al. [86] to enhance the accuracy of detection and determination of the depth of the crack. Contrast-enhanced CBCT under vacuum conditions is known to suggestively improve the diagnostic rate of cracks. However, it is not a very accurate measure of crack depths.
7.4. Other Techniques
- a.
- Ultrasonic System
Detection of CTS using ultrasonics has a promising future as it demonstrates the capability to infiltrate hard tissues, including radiopaque restorations. It is also oblivious to the hazards of ionizing radioactivity. Culijat et al. [87] used a system of integrated ultrasonics to successfully identify known cracks in simulated teeth. The first study to use laser ultrasonics utilized image analysis in combination with analysis of finite-element to precisely measure the crack depth in clinical settings was published by Sun et al. [86].
- b.
- Infrared Thermography
When other diagnostic techniques fail, infrared thermography technology can assist in the detection of small cracks (4–35.5 m). The ultrasonic power vibrates (the amplitude and detection angle should be 0.89 W within 45°, respectively) and creates local friction that generates heat [88,89]. The dentinal microcracks can then be presented under the action of the thermal imager. However, this approach has several shortcomings when it comes to detecting wide cracks [90].
- c.
- Near-Infrared
A near-infrared diode laser with a wavelength of 810 nm can be employed as new technology to help control systematic CTS. When teeth in question are exposed to laser energy, the majority of patients feel a shooting ache, with a handful feeling a dull ache. This can be attributed to the energy applied to the pulp when the laser beam enters the depth of the crack generating an analogous irritation [36]. The classical investigation techniques and new advancements in clinical diagnosis should focus on problems that arise earlier during the procedure.
Zheng Y et al. examined an in vivo system that used a near-IR light source to identify enamel cracks and analyze an association between age and anterior enamel cracks [91]. Qualitative examination revealed no correlation between age and the gravity of the enamel cracks. Although not statistically significant, a tendency to increase the length of anterior enamel cracks was seen with age. An 850 nm wavelength silicon charge-coupled device (CCD) shows satisfactory results in detecting enamel cracks.
Chen Zhi et al. evaluated four distinct methods for detecting cracks in teeth, which may elicit foundations for timely crack detection [92]. Three observers independently examined crown cracks using the naked eye, microscope, methylene blue dye, and methylene blue dye with magnification on 123 freshly extracted human teeth. It was concluded that methylene blue dye used under magnification detected tooth cracks with greater accuracy. The detection of the cracks also depended on the experience and diagnostic skills of the endodontist. Table 1 lists the common methods for identifying cracked teeth.
8. Conclusions
Patients with a cracked tooth may present with a confusing array of symptoms. A cracked tooth is a distinct possibility to consider when with complaints of pain or discomfort while chewing. Enamel cracks are ominous harbingers of future pathology and need to be treated promptly. Current conventional diagnostic methods may be inconclusive. Dental professionals with a keen understanding of the classic signs combined with recent technological advances can help in early diagnosis and prevent further crack propagation and destruction.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Türp, J.C.; Gobetti, J.P. The Cracked Tooth Syndrome: An Elusive Diagnosis. J. Am. Dent. Assoc. 1996, 127, 1502–1507. [Google Scholar] [CrossRef] [PubMed]
- Rosen, H. Cracked Tooth Syndrome. J. Prosthet. Dent. 1982, 47, 36–43. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F., Jr.; Loghin, S.; Berman, L.H. The Cracked Tooth: Histopathologic and Histobacteriologic Aspects. J. Endod. 2015, 41, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Hilton, T.J.; Funkhouser, E.; Ferracane, J.L.; Gordan, V.V.; Huff, K.D.; Barna, J.; Mungia, R.; Marker, T.; Gilbert, G.H.; National Dental PBRN Collaborative Group. Associations of Types of Pain with Crack-Level, Tooth-Level and Patient-Level Characteristics in Posterior Teeth with Visible Cracks: Findings from the National Dental Practice-Based research Network. J. Dent. 2018, 70, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Ellis, S.G.S.; Macfarlane, T.V.; McCord, J.F. Influence of Patient Age on the Nature of Tooth Fracture. J. Prosthet. Dent. 1999, 82, 226–230. [Google Scholar] [CrossRef]
- Hasan, S.; Singh, K.; Salati, N. Cracked Tooth Syndrome: Overview of Literature. Int. J. Appl. Basic Med. Res. 2015, 5, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiatt, W.H. Incomplete Crown-root Fracture in Pulpal-periodontal Disease. J. Periodontol. 1973, 44, 369–379. [Google Scholar] [CrossRef]
- Yahyazadehfar, M.; Zhang, D.; Arola, D. On the Importance of Aging to the Crack Growth Resistance of Human Enamel. Acta Biomater. 2016, 32, 264–274. [Google Scholar] [CrossRef] [Green Version]
- He, B.; Huang, S.; Zhang, C.; Jing, J.; Hao, Y.; Xiao, L.; Zhou, X. Mineral Densities and Elemental Content in Different Layers of Healthy Human Enamel with Varying Teeth Age. Arch. Oral Biol. 2011, 56, 997–1004. [Google Scholar] [CrossRef]
- Attin, T.; Schmidlin, P.R.; Wegehaupt, F.; Wiegand, A. Influence of Study Design on the Impact of Bleaching Agents on Dental Enamel Microhardness: A review. Dent. Mater. 2009, 25, 143–157. [Google Scholar] [CrossRef] [Green Version]
- Lopes, G.C.; Bonissoni, L.; Baratieri, L.N.; Vieira, L.C.C.; Monteiro, S., Jr. Effect of Bleaching Agents on the Hardness and Morphology of Enamel. J. Esthet. Restor. Dent. 2002, 14, 24–30. [Google Scholar] [CrossRef]
- Geurtsen, W. The Cracked-Tooth Syndrome: Clinical Features and Case Reports. Int. J. Periodontics Restor. Dent. 1992, 12, 395–405. [Google Scholar]
- Banerji, S.; Mehta, S.B.; Millar, B.J. Cracked Tooth Syndrome. Part 1: Aetiology and Diagnosis. Br. Dent. J. 2010, 208, 459–463. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.-E.; Jo, A.-R.; Lee, H.-J.; Kim, S.-Y. Analysis of the Characteristics of Cracked Teeth and Evaluation of Pulp Status According to Periodontal Probing Depth. BMC Oral Health 2017, 17, 135. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-H.; Eo, S.-H.; Shrestha, R.; Ihm, J.-J.; Seo, D.-G. Association between Longitudinal Tooth Fractures and Visual Detection Methods in Diagnosis. J. Dent. 2020, 101, 103466. [Google Scholar] [CrossRef]
- Gopikrishna, V.; Pradeep, G.; Venkateshbabu, N. Assessment of Pulp Vitality: A Review. Int. J. Paediatr. Dent. 2009, 19, 3–15. [Google Scholar] [CrossRef]
- Ghorbanzadeh, A.; Aminifar, S.; Shadan, L.; Ghanati, H. Evaluation of Three Methods in the Diagnosis of Dentin Cracks Caused by Apical Resection. J. Dent. 2013, 10, 175. [Google Scholar]
- Clark, D.J.; Sheets, C.G.; Paquette, J.M. Definitive Diagnosis of Early Enamel and Dentinal Cracks Based on Microscopic Evaluation. J. Esthet. Restor. Dent. 2003, 15, 391–401. [Google Scholar] [CrossRef]
- Landrigan, M.D.; Flatley, J.C.; Turnbull, T.L.; Kruzic, J.J.; Ferracane, J.L.; Hilton, T.J.; Roeder, R.K. Detection of Dentinal Cracks Using Contrast-Enhanced Micro-Computed Tomography. J. Mech. Behav. Biomed. Mater. 2010, 3, 223–227. [Google Scholar] [CrossRef]
- Lee, S.-H.; Lee, J.-J.; Chung, H.-J.; Park, J.-T.; Kim, H.-J. Dental Optical Coherence Tomography: New Potential Diagnostic System for Cracked-Tooth Syndrome. Surg. Radiol. Anat. 2016, 38, 49–54. [Google Scholar] [CrossRef]
- Kim, J.-M.; Kang, S.-R.; Yi, W.-J. Automatic Detection of Tooth Cracks in Optical Coherence Tomography Images. J. Periodontal Implant Sci. 2017, 47, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Xu, Y.; Shen, Z.; Wang, L.; Qiao, F.; Zhang, X.; Li, M.; Wu, L. The Extent of the Crack on Artificial Simulation Models with CBCT and Periapical Radiography. PLoS ONE 2017, 12, e0169150. [Google Scholar] [CrossRef] [PubMed]
- Leader, D.M. CBCT Is Valuable for Diagnosis of Tooth Fracture. Evid. Based Dent. 2015, 16, 23–24. [Google Scholar] [CrossRef] [PubMed]
- Chong, B.S. Bilateral Cracked Teeth: A Case Report. Int. Endod. J. 1989, 22, 193–196. [Google Scholar] [CrossRef]
- Ehrmann, E.H.; Tyas, M.J. Cracked Tooth Syndrome: Diagnosis, Treatment and Correlation between Symptoms and Post-Extraction Findings. Aust. Dent. J. 1990, 35, 105–112. [Google Scholar] [CrossRef]
- Brannstrom, M. Dentin and Pulp in Restorative Dentistry; Dental Therapeutic AB: Nacka, Sweden, 1981; Volume 70. [Google Scholar]
- Bergenholtz, G. Pathogenic Mechanisms in Pulpal Disease. J. Endod. 1990, 16, 98–101. [Google Scholar] [CrossRef]
- Brannstrom, M. The Hydrodynamics of the Dentine. Its Possible Relationship to Dentinal Pain. Int. Dent. J. 1972, 22, 219–227. [Google Scholar]
- Kim, S.-Y.; Kang, M.-K.; Kang, S.-M.; Kim, H.-E. Effects of Ultrasonic Instrumentation on Enamel Surfaces with Various Defects. Int. J. Dent. Hyg. 2018, 16, 219–224. [Google Scholar] [CrossRef]
- Mathew, S.; Thangavel, B.; Mathew, C.A.; Kailasam, S.; Kumaravadivel, K.; Das, A. Diagnosis of Cracked Tooth Syndrome. J. Pharm. Bioallied Sci. 2012, 4, S242. [Google Scholar] [CrossRef]
- Kahler, W. The cracked tooth conundrum: Terminology, Classification, Diagnosis, and Management. Am. J. Dent. 2008, 21, 275. [Google Scholar]
- Çelik Köycü, B.; İmirzalıoğlu, P. Heat Transfer and Thermal Stress Analysis of a Mandibular Molar Tooth Restored by Different Indirect Restorations Using a Three-Dimensional Finite Element Method. J. Prosthodont. 2017, 26, 460–473. [Google Scholar] [CrossRef]
- Fusayama, T. Indications for Self-Cured and Light-Cured Adhesive Composite Resins. J. Prosthet. Dent. 1992, 67, 46–51. [Google Scholar] [CrossRef]
- Rivera, E.M.; Walton, R.E. Cracking the Cracked Tooth Code: Detection and Treatment of Various Longitudinal Tooth Fractures. Am. Assoc. Endodontists Colleagues Excell. News Lett. 2008, 2, 1–19. [Google Scholar]
- Silvestri, A.R., Jr.; Singh, I. Treatment Rationale of Fractured Posterior Teeth. J. Am. Dent. Assoc. 1978, 97, 806–810. [Google Scholar] [CrossRef]
- Talim, S.T.; Gohil, K.S. Management of Coronal Fractures of Permanent Posterior Teeth. J. Prosthet. Dent. 1974, 31, 172–178. [Google Scholar] [CrossRef]
- Davis, R.; Overton, J.D. Efficacy of Bonded and Nonbonded Amalgam in the Treatment: Of Teeth with Incomplete Fractures. J. Am. Dent. Assoc. 2000, 131, 469–478. [Google Scholar] [CrossRef]
- Luehke, R.G. Vertical Crown-Root Fractures in Posterior Teeth. Dent. Clin. N. Am. 1984, 28, 883–894. [Google Scholar] [CrossRef]
- Ailor, J.E., Jr. Managing Incomplete Tooth Fractures. J. Am. Dent. Assoc. 2000, 131, 1168–1174. [Google Scholar] [CrossRef]
- Wright, H.M., Jr.; Loushine, R.J.; Weller, R.N.; Kimbrough, W.F.; Waller, J.; Pashley, D.H. Identification of Resected Root-End Dentinal cracks: A Comparative Study of Transillumination and Dyes. J. Endod. 2004, 30, 712–715. [Google Scholar] [CrossRef] [Green Version]
- Cooley, R.L.; Barkmeier, W.W. Diagnosis of the Incomplete Tooth Fracture. Gen. Dent. 1979, 27, 58–60. [Google Scholar]
- Liu, H.H.; Sidhu, S.K. Cracked Teeth—Treatment Rationale and Case Management. Quintessence Int. 1995, 26, 485–492. [Google Scholar]
- Zhang, S.; Li, X.; Qi, Y.; Ma, X.; Qiao, S.; Cai, H.; Zhao, B.C.; Jiang, H.B.; Lee, E.-S. Comparison of Autogenous Tooth Materials and Other Bone Grafts. Tissue Eng. Regen. Med. 2021, 18, 327–341. [Google Scholar] [CrossRef]
- Liewehr, F.R. An Inexpensive Device for Transillumination. J. Endod. 2001, 27, 130–131. [Google Scholar] [CrossRef] [Green Version]
- Pitts, D.L.; Natkin, E. Diagnosis and Treatment of Vertical Root Fractures. J. Endod. 1983, 9, 338–346. [Google Scholar] [CrossRef]
- Mamoun, J.S.; Napoletano, D. Cracked Tooth Diagnosis and Treatment: An Alternative Paradigm. Eur. J. Dent. 2015, 9, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Madrid, C.C.; de Pauli Paglioni, M.; Line, S.R.; Vasconcelos, K.G.; Brandão, T.B.; Lopes, M.A.; Santos-Silva, A.R.; De Goes, M.F. Structural Analysis of Enamel in Teeth from Head-and-Neck Cancer Patients Who Underwent Radiotherapy. Caries Res. 2017, 51, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Abou-Rass, M. Crack Lines: The Precursors of Tooth Fractures-Their Diagnosis and Treatment. Quintessence Int. Dent. Dig. 1983, 14, 437–447. [Google Scholar]
- Griffin, J.D., Jr. Efficient, Conservative Treatment of Symptomatic Cracked Teeth. Compend. Contin. Educ. Dent. 2006, 27, 93–102. [Google Scholar]
- Al-Shami, S.A.; Mowafey, B.H.; Hamdan, H.H.; Youssef, J.M. Diagnosis of Dental Cracks by Digital Bitewing Imaging: A Laboratory Study. Mansoura J. Dent. 2022, 9, 19–21. [Google Scholar]
- Salineiro, F.C.S.; Kobayashi-Velasco, S.; Braga, M.M.; Cavalcanti, M.G.P. Radiographic diagnosis of root fractures: A systematic review, meta-analyses and sources of heterogeneity. Dentomaxillofac Radiol. 2017, 46, 8–18. [Google Scholar] [CrossRef]
- Metska, M.E.; Aartman, I.H.A.; Wesselink, P.R.; Özok, A.R. Detection of Vertical Root Fractures in Vivo in Endodontically Treated Teeth by Cone-Beam Computed Tomography Scans. J. Endod. 2012, 38, 1344–1347. [Google Scholar] [CrossRef]
- Chavda, R.; Mannocci, F.; Andiappan, M.; Patel, S. Comparing The in Vivo Diagnostic Accuracy of Digital Periapical Radiography With Cone-Beam Computed Tomography for the Detection of Vertical Root Fracture. J. Endod. 2014, 40, 1524–1529. [Google Scholar] [CrossRef]
- Brady, E.; Mannocci, F.; Brown, J.; Wilson, R.; Patel, S. A Comparison of Cone Beam Computed Tomography and Periapical Radiography for the Detection of Vertical Root Fractures in Nonendodontically Treated Teeth. Int. Endod. J. 2014, 47, 735–746. [Google Scholar] [CrossRef]
- Yuan, M.; Gao, A.T.; Wang, T.M.; Liang, J.H.; Aihemati, G.B.; Cao, Y.; Xie, X.; Miao, L.Y.; Lin, Z.T. Using Meglumine Diatrizoate to Improve the Accuracy of Diagnosis of Cracked Teeth on CONE-beam CT images. Int. Endod. J. 2020, 53, 709–714. [Google Scholar] [CrossRef]
- Roh, B.; Lee, Y. Analysis of 154 Cases of Teeth with Cracks. Dent. Traumatol. 2006, 22, 118–123. [Google Scholar] [CrossRef]
- Fujimoto, J.; Drexler, W. Introduction to Optical Coherence Tomography BT—Optical Coherence Tomography: Technology and Applications. In Biological and Medical Physics, Biomedical Engineering; Drexler, W., Fujimoto, J.G., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 1–45. ISBN 978-3-540-77550-8. [Google Scholar]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A. Optical Coherence Tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [Green Version]
- Otis, L.L.; Everett, M.J.; Sathyam, U.S.; Colston, B.W., Jr. Optical Coherence Tomography: A New Imaging: Technology for Dentistry. J. Am. Dent. Assoc. 2000, 131, 511–514. [Google Scholar] [CrossRef]
- Colston, B.W.; Sathyam, U.S.; DaSilva, L.B.; Everett, M.J.; Stroeve, P.; Otis, L.L. Dental OCT. Opt. Express 1998, 3, 230–238. [Google Scholar] [CrossRef]
- Wang, X.-J.; Milner, T.E.; De Boer, J.F.; Zhang, Y.; Pashley, D.H.; Nelson, J.S. Characterization of Dentin and Enamel by Use of Optical Coherence Tomography. Appl. Opt. 1999, 38, 2092–2096. [Google Scholar] [CrossRef]
- Shimada, Y.; Sadr, A.; Burrow, M.F.; Tagami, J.; Ozawa, N.; Sumi, Y. Validation of Swept-Source Optical Coherence Tomography (SS-OCT) for the Diagnosis of Occlusal caries. J. Dent. 2010, 38, 655–665. [Google Scholar] [CrossRef]
- Nakagawa, H.; Sadr, A.; Shimada, Y.; Tagami, J.; Sumi, Y. Validation of Swept Source Optical Coherence Tomography (SS-OCT) for the Diagnosis of Smooth Surface Caries in Vitro. J. Dent. 2013, 41, 80–89. [Google Scholar] [CrossRef]
- Natsume, Y.; Nakashima, S.; Sadr, A.; Shimada, Y.; Tagami, J.; Sumi, Y. Estimation of Lesion Progress in Artificial Root Caries by Swept Source Optical Coherence Tomography in Comparison to Transverse Microradiography. J. Biomed. Opt. 2011, 16, 071408. [Google Scholar] [CrossRef]
- Tabata, T.; Shimada, Y.; Sadr, A.; Tagami, J.; Sumi, Y. Assessment of Enamel Cracks at Adhesive Cavosurface Margin Using Three-Dimensional Swept-Source Optical Coherence Tomography. J. Dent. 2017, 61, 28–32. [Google Scholar] [CrossRef]
- Imai, K.; Shimada, Y.; Sadr, A.; Sumi, Y.; Tagami, J. Noninvasive Cross-Sectional Visualization of Enamel Cracks by Optical Coherence Tomography in Vitro. J. Endod. 2012, 38, 1269–1274. [Google Scholar] [CrossRef]
- Sadr, A.; Shimada, Y.; Mayoral, J.R.; Hariri, I.; Bakhsh, T.A.; Sumi, Y.; Tagami, J. Swept Source Optical Coherence tomography for Quantitative and Qualitative Assessment of Dental Composite Restorations. In Proceedings of the Lasers in Dentistry XVII; SPIE, San Francisco, CA, USA, 22–27 January 2011; Volume 7884, pp. 63–72. [Google Scholar]
- Leitgeb, R.; Hitzenberger, C.K.; Fercher, A.F. Performance of Fourier Domain vs. Time Domain Optical Coherence Tomography. Opt. Express 2003, 11, 889–894. [Google Scholar] [CrossRef]
- Feldchtein, F.I.; Gelikonov, G.V.; Gelikonov, V.M.; Iksanov, R.R.; Kuranov, R.V.; Sergeev, A.M.; Gladkova, N.D.; Ourutina, M.N.; Warren, J.A.; Reitze, D.H. In Vivo OCT Imaging of Hard and Soft Tissue of the Oral Cavity. Opt. Express 1998, 3, 239–250. [Google Scholar] [CrossRef]
- Chinn, S.R.; Swanson, E.A.; Fujimoto, J.G. Optical Coherence Tomography Using a Frequency-Tunable Optical Source. Opt. Lett. 1997, 22, 340–342. [Google Scholar] [CrossRef]
- Shimada, Y.; Sadr, A.; Sumi, Y.; Tagami, J. Application of Optical Coherence Tomography (OCT) for Diagnosis of Caries, Cracks, and Defects of Restorations. Curr. Oral Health Rep. 2015, 2, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fercher, A.F.; Drexler, W.; Hitzenberger, C.K.; Lasser, T. Optical Coherence Tomography-Principles and Applications. Rep. Prog. Phys. 2003, 66, 239. [Google Scholar] [CrossRef]
- Segarra, M.S.; Shimada, Y.; Sadr, A.; Sumi, Y.; Tagami, J. Three-Dimensional Analysis of Enamel Crack Behavior Using Optical Coherence Tomography. J. Dent. Res. 2017, 96, 308–314. [Google Scholar] [CrossRef]
- Yoshioka, T.; Sakaue, H.; Ishimura, H.; Ebihara, A.; Suda, H.; Sumi, Y. Detection of Root Surface Fractures with Swept-Source Optical Coherence Tomography (SS-OCT). Photomed. Laser Surg. 2013, 31, 23–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shemesh, H.; van Soest, G.; Wu, M.-K.; Wesselink, P.R. Diagnosis of Vertical Root Fractures with Optical Coherence Tomography. J. Endod. 2008, 34, 739–742. [Google Scholar] [CrossRef] [PubMed]
- Fried, W.A.; Simon, J.C.; Lucas, S.; Chan, K.H.; Darling, C.L.; Staninec, M.; Fried, D. Near-IR Imaging of Cracks in Teeth. Proc. SPIE Int. Soc. Opt. Eng. 2014, 8929, 89290Q. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.; Lee, D.; Darling, C.L.; Fried, D. Nondestructive Assessment of the Severity of Occlusal Caries Lesions with Near-Infrared Imaging at 1310 Nm. J. Biomed. Opt. 2010, 15, 47011. [Google Scholar] [CrossRef] [Green Version]
- Bühler, C.; Ngaotheppitak, P.; Fried, D. Imaging of Occlusal Dental Caries (Decay) with near-IR Light at 1310-Nm. Opt. Express 2005, 13, 573–582. [Google Scholar] [CrossRef]
- Stanga, P.E.; Tsamis, E.; Papayannis, A.; Stringa, F.; Cole, T.; Jalil, A. Swept-Source Optical Coherence Tomography AngioTM (Topcon Corp, Japan): Technology Review. OCT Angiogr. Retin. Macular Dis. 2016, 56, 13–17. [Google Scholar]
- Hsieh, Y.-S.; Ho, Y.-C.; Lee, S.-Y.; Chuang, C.-C.; Tsai, J.; Lin, K.-F.; Sun, C.-W. Dental Optical Coherence Tomography. Sensors 2013, 13, 8928–8949. [Google Scholar] [CrossRef] [Green Version]
- Machoy, M.; Seeliger, J.; Szyszka-Sommerfeld, L.; Koprowski, R.; Gedrange, T.; Woźniak, K. The Use of Optical Coherence Tomography in Dental Diagnostics: A State-of-the-Art Review. J. Healthc. Eng. 2017, 2017, 7560645. [Google Scholar] [CrossRef] [Green Version]
- Zavareh, A.T.; Barajas, O.; Hoyos, S. An Efficient Estimation Algorithm for the Calibration of Low-Cost SS-OCT Systems. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 1169–1172. [Google Scholar]
- Li, Z.; Holamoge, Y.V.; Li, Z.; Zaid, W.; Osborn, M.L.; Ramos, A.; Miller, J.T.; Li, Y.; Yao, S.; Xu, J. Detection and Analysis of Enamel Cracks by ICG-NIR Fluorescence Dental Imaging. Ann. N. Y. Acad. Sci. 2020, 1475, 52–63. [Google Scholar] [CrossRef]
- Amaechi, B.T.; Higham, S.M. Quantitative Light-Induced Fluorescence: A Potential Tool for General Dental Assessment. J. Biomed. Opt. 2002, 7, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Angmar-Månsson, B.; Ten Bosch, J.J. Quantitative Light-Induced Fluorescence (QLF): A Method for Assessment of Incipient Caries Lesions. Dentomaxillofacial Radiol. 2001, 30, 298–307. [Google Scholar] [CrossRef]
- Sun, K.; Yuan, L.; Shen, Z.; Xu, Z.; Zhu, Q.; Ni, X.; Lu, J. Scanning Laser-Line Source Technique for Nondestructive Evaluation of Cracks in Human Teeth. Appl. Opt. 2014, 53, 2366–2374. [Google Scholar] [CrossRef]
- Culjat, M.O.; Singh, R.S.; Brown, E.R.; Neurgaonkar, R.R.; Yoon, D.C.; White, S.N. Ultrasound Crack Detection in a Simulated Human Tooth. Dentomaxillofacial Radiol. 2005, 34, 80–85. [Google Scholar] [CrossRef]
- Bernardes, R.A.; de Moraes, I.G.; Duarte, M.A.H.; Azevedo, B.C.; de Azevedo, J.R.; Bramante, C.M. Use of Cone-Beam Volumetric Tomography in the Diagnosis of Root Fractures. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 270–277. [Google Scholar] [CrossRef]
- Strassler, H.E.; Pitel, M.L. Using Fiber-Optic Transillumination as a Diagnostic Aid in Dental Practice. Compendium 2014, 35, 80–88. [Google Scholar]
- Hassan, B.; Metska, M.E.; Ozok, A.R.; van der Stelt, P.; Wesselink, P.R. Comparison of Five Cone Beam Computed Tomography Systems for the Detection of Vertical Root Fractures. J. Endod. 2010, 36, 126–129. [Google Scholar] [CrossRef]
- Zheng, Y.; Oh, M.H.; Song, W.S.; Kim, K.H.; Shin, I.H.; Kim, M.S.; Cho, J.H. Infrared Clinical Enamel Crack Detector Based on Silicon Ccd and Its Application: A High-Quality and Low-Cost Option. J. Imaging 2021, 7, 259. [Google Scholar] [CrossRef]
- Chen, Z. Evaluate Four Different Ways in Diagnosing Tooth Cracks. Res. Sq. 2020, 1–15. [Google Scholar] [CrossRef]
Figure 1.
Type of tooth fractures.

Figure 2.
Classification of tooth fractures [36].
Figure 2.
Classification of tooth fractures [36].

Figure 3.
(A) Enamel crack. (B) Transillumination used to confirm presence of crack.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Four common methods for identifying cracked teeth [13].
Table 1.
Four common methods for identifying cracked teeth [13].
| Features | Transillumination | Intraoral X-ray | CBCT | SS-OCT |
|---|---|---|---|---|
| Distinguish the type of crack | × [70] | × [90] | × [18] | ✓ [86] |
| Show root fractures | × [70] | ✓ [1] | ✓ [81] | × [86] |
| Determine the crack depth | × [18] | × [10] | ✓ [86] | ✓ [17] |
| Produce radiation | × [92] | ✓ [50] | ✓ [56] | × [18] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zidane, B. Recent Advances in the Diagnosis of Enamel Cracks: A Narrative Review. Diagnostics 2022, 12, 2027. https://doi.org/10.3390/diagnostics12082027
AMA Style
Zidane B. Recent Advances in the Diagnosis of Enamel Cracks: A Narrative Review. Diagnostics. 2022; 12(8):2027. https://doi.org/10.3390/diagnostics12082027
Chicago/Turabian StyleZidane, Bassam. 2022. "Recent Advances in the Diagnosis of Enamel Cracks: A Narrative Review" Diagnostics 12, no. 8: 2027. https://doi.org/10.3390/diagnostics12082027
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.