
Myocardial Tissue Characterization in Patients with Hypertensive Crisis, Positive Troponin, and Unobstructed Coronary Arteries: A Cardiovascular Magnetic Resonance-Based Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
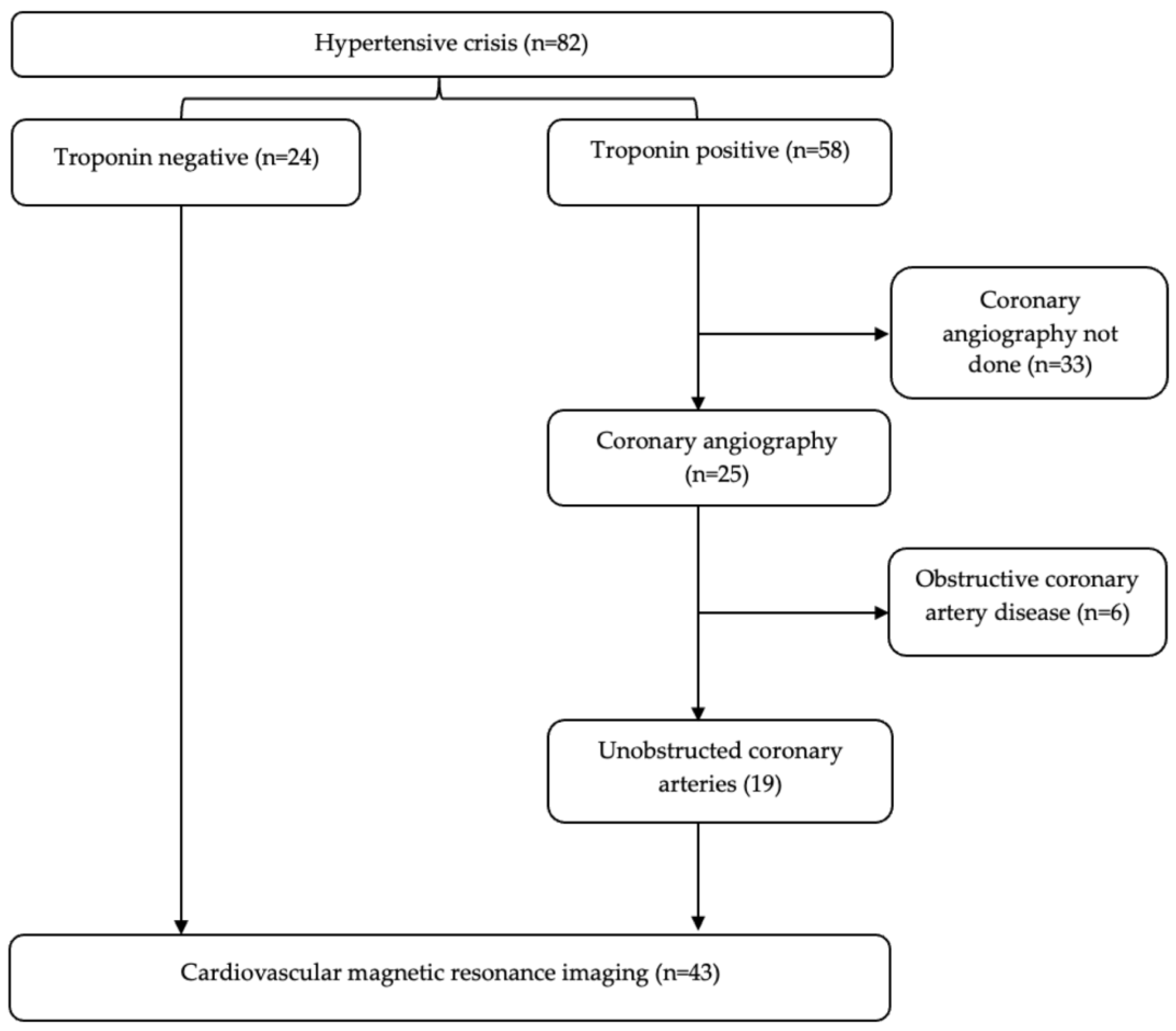
2.1. Study Population
2.2. Cardiac Magnetic Resonance Imaging
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Clinical and Demographic Characteristics
3.2. Cardiovascular Magnetic Resonance Imaging
3.2.1. Morphology and Function
3.2.2. T2-Weighted Signal Intensity Ratio and Parametric Mapping
3.2.3. Late Gadolinium Enhancement
3.3. Binary Logistic Regression of Factors Associated with Troponin-Positive Unobstructed Coronary Arteries
3.4. Receiver Operator Characteristic Curve for Predictors of Troponin-Positive Unobstructed Coronary Artery
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zampaglione, B.; Pascale, C.; Marchisio, M.; Cavallo-Perin, P. Hypertensive urgencies and emergencies. Prevalence and clinical presentation. Hypertension 1996, 27, 144–147. [Google Scholar] [CrossRef]
- Paini, A.; Tarozzi, L.; Bertacchini, F.; Aggiusti, C.; Rosei, C.A.; De Ciuceis, C.; Malerba, P.; Broggi, A.; Perani, C.; Salvetti, M.; et al. Cardiovascular prognosis in patients admitted to an emergency department with hypertensive emergencies and urgencies. J. Hypertens. 2021, 39, 2514–2520. [Google Scholar] [CrossRef]
- Talle, M.A.; Ngarande, E.; Doubell, A.F.; Herbst, P.G. Prevalence of Myocardial Injury and Myocardial Infarction in Patients with a Hypertensive Emergency: A Systematic Review. Diagnostics 2023, 13, 60. [Google Scholar] [CrossRef]
- Astarita, A.; Covella, M.; Vallelonga, F.; Cesareo, M.; Totaro, S.; Ventre, L.; Aprà, F.; Veglio, F.; Milan, A. Hypertensive emergencies and urgencies in emergency departments: A systematic review and meta-analysis. J. Hypertens. 2020, 38, 1203–1210. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; Morrow, D.A.; White, H.D. Fourth universal definition of myocardial infarction (2018). J. Am. Coll Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Lydakis, C.; Beevers, D.G. Management of patients with myocardial infarction and hypertension. Eur. Heart J. 2000, 21, 1125–1134. [Google Scholar] [CrossRef]
- Viau, D.M.; Sala-Mercado, J.A.; Spranger, M.D.; O’Leary, D.S.; Levy, P.D. The pathophysiology of hypertensive acute heart failure. Heart 2015, 101, 1861–1867. [Google Scholar] [CrossRef]
- Pattanshetty, D.J.; Bhat, P.K.; Aneja, A.; Pillai, D.P. Elevated troponin predicts long-term adverse cardiovascular outcomes in hypertensive crisis: A retrospective study. J. Hypertens. 2012, 30, 2410–2415. [Google Scholar] [CrossRef]
- Bularga, A.; Hung, J.; Daghem, M.; Stewart, S.; Taggart, C.; Wereski, R.; Singh, T.; Meah, M.N.; Fujisawa, T.; Ferry, A.V.; et al. Coronary Artery and Cardiac Disease in Patients With Type 2 Myocardial Infarction: A Prospective Cohort Study. Circulation 2022, 145, 1188–1200. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Thierry Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar]
- Pustjens, T.F.S.; Appelman, Y.; Damman, P.; ten Berg, J.M.; Jukema, J.W.; de Winter, R.J.; Agema, W.R.P.; van der Wielen, M.L.J.; Arslan, F.; Rasoul, S.; et al. Guidelines for the management of myocardial infarction/injury with non-obstructive coronary arteries (MINOCA): A position paper from the Dutch ACS working group. Neth. Heart J. 2020, 28, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Buller, P.; Rosiak, S.; Rosiak, W.; Tyczyński, M.; Gil, R.J.; Bil, J. Arterial hypertension as a risk factor for myocardial infarction with non-obstructive coronary arteries (MINOCA). Arter. Hypertens. 2021, 25, 106–111. [Google Scholar] [CrossRef]
- Bergamaschi, L.; Foà, A.; Paolisso, P.; Renzulli, M.; Angeli, F.; Fabrizio, M.; Bartoli, L.; Armillotta, M.; Sansonetti, A.; Amicone, S.; et al. Prognostic Role of Early Cardiac Magnetic Resonance in Myocardial Infarction With Nonobstructive Coronary Arteries. JACC Cardiovasc. Imaging 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Kim, B.S.; Kim, H.J.; Lee, J.H.; Shin, J.; Shin, J.H. Clinical implications of cardiac troponin-I in patients with hypertensive crisis visiting the emergency department. Ann. Med. 2022, 54, 507–515. [Google Scholar] [CrossRef] [PubMed]
- van den Born, B.J.H.; Lip, G.Y.H.; Brguljan-Hitij, J.; Cremer, A.; Segura, J.; Morales, E.; Mahfoud, F.; Amraoui, F.; Persu, A.; Kahan, T.; et al. ESC Council on hypertension position document on the management of hypertensive emergencies. Eur. Heart J. Cardiovasc. Pharmacother. 2019, 5, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef]
- Reiter, G.; Reiter, C.; Kräuter, C.; Fuchsjäger, M.; Reiter, U. Cardiac magnetic resonance T1 mapping. Part 1: Aspects of acquisition and evaluation. Eur. J. Radiol. 2018, 109, 223–234. [Google Scholar] [CrossRef]
- Kawel-Boehm, N.; Maceira, A.; Valsangiacomo-Buechel, E.R.; Vogel-Claussen, J.; Turkbey, E.B.; Williams, R.; Plein, S.; Tee, M.; Eng, J.; Bluemke, D.A. Normal values for cardiovascular magnetic resonance in adults and children. J. Cardiovasc. Magn. Reson. 2015, 17, 29. [Google Scholar] [CrossRef]
- Carbone, I.; Childs, H.; Aljizeeri, A.; Merchant, N.; Friedrich, M.G. Importance of Reference Muscle Selection in Quantitative Signal Intensity Analysis of T2-Weighted Images of Myocardial Edema Using a T2 Ratio Method. Biomed. Res. Int. 2015, 2015, 232649. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar]
- Mikami, Y.; Cornhill, A.; Dykstra, S.; Satriano, A.; Hansen, R.; Flewitt, J.; Seib, M.; Rivest, S.; Sandonato, R.; Lydell, C.P.; et al. Right ventricular insertion site fibrosis in a dilated cardiomyopathy referral population: Phenotypic associations and value for the prediction of heart failure admission or death. J. Cardiovasc. Magn. Reson. 2021, 23, 79. [Google Scholar] [CrossRef] [PubMed]
- Cummings, K.W.; Bhalla, S.; Javidan-Nejad, C.; Bierhals, A.J.; Gutierrez, F.R.; Woodard, P.K. A pattern-based approach to assessment of delayed enhancement in nonischemic cardiomyopathy at MR imaging. Radiographics 2009, 29, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Kwong, R.Y.; Schussheim, A.E.; Rekhraj, S.; Aletras, A.H.; Geller, N.; Davis, J.; Christian, T.F.; Balaban, R.S.; Arai, A.E. Detecting acute coronary syndrome in the emergency department with cardiac magnetic resonance imaging. Circulation 2003, 107, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Robbertse, P.P.S.; Doubell, A.F.; Lombard, C.J.; Talle, M.A.; Herbst, P.G. Evolution of myocardial oedema and fibrosis in HIV infected persons after the initiation of antiretroviral therapy: A prospective cardiovascular magnetic resonance study. J. Cardiovasc. Magn. Reson. 2022, 24, 72. [Google Scholar] [CrossRef] [PubMed]
- Robbertse, P.P.S.; Doubell, A.F.; Steyn, J.; Lombard, C.J.; Talle, M.A.; Herbst, P.G. Altered cardiac structure and function in newly diagnosed people living with HIV: A prospective cardiovascular magnetic resonance study after the initiation of antiretroviral treatment. Int. J. Cardiovasc. Imaging 2023, 39, 169–182. [Google Scholar] [CrossRef]
- Bellenger, N.G.; Davies, L.C.; Francis, J.M.; Coats, A.J.S.; Pennell, D.J. Reduction in sample size for studies of remodeling in heart failure by the use of cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2000, 2, 271–278. [Google Scholar] [CrossRef]
- Acosta, G.; Amro, A.; Aguilar, R.; Ahusnina, W.; Bhardwaj, N.; Koromia, G.A.; Studeny, M.; Irfan, A. Clinical Determinants of Myocardial Injury, Detectable and Serial Troponin Levels among Patients with Hypertensive Crisis. Cureus 2020, 12, e6786. [Google Scholar] [CrossRef]
- Rubin, S.; Cremer, A.; Boulestreau, R.; Rigothier, C.; Kuntz, S.; Gosse, P. Malignant hypertension: Diagnosis, treatment and prognosis with experience from the Bordeaux cohort. J. Hypertens. 2019, 37, 316–324. [Google Scholar] [CrossRef]
- Arcari, L.; Engel, J.; Freiwald, T.; Zhou, H.; Zainal, H.; Gawor, M.; Buettner, S.; Geiger, H.; Hauser, I.; Nagel, E.; et al. Cardiac biomarkers in chronic kidney disease are independently associated with myocardial edema and diffuse fibrosis by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2021, 23, 71. [Google Scholar] [CrossRef]
- Eitel, I.; Friedrich, M.G. T2-weighted cardiovascular magnetic resonance in acute cardiac disease. J. Cardiovasc. Magn. Reson. 2011, 13, 13. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Dorado, D.; Oliveras, J. Myocardial oedema: A preventable cause of reperfusion injury? Cardiovasc. Res. 1993, 27, 1555–1563. [Google Scholar] [CrossRef]
- Dolan, R.S.; Rahsepar, A.A.; Blaisdell, J.; Suwa, K.; Ghafourian, K.; Wilcox, J.E.; Khan, S.S.; Vorovich, E.E.; Rich, J.D.; Anderson, A.S.; et al. Multiparametric Cardiac Magnetic Resonance Imaging Can Detect Acute Cardiac Allograft Rejection After Heart Transplantation. JACC Cardiovasc. Imaging 2019, 12, 1632–1641. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Cai, J.; Cui, Y.; Wang, J.; Alwalid, O.; Shen, X.; Cao, Y.; Zou, Y.; Liang, B. CMR-derived extracellular volume fraction (ECV) in asymptomatic heart transplant recipients: Correlations with clinical features and myocardial edema. Int. J. Cardiovasc. Imaging 2018, 34, 1959–1967. [Google Scholar] [CrossRef] [PubMed]
- Chaikriangkrai, K.; Abbasi, M.A.; Sarnari, R.; Dolan, R.; Lee, D.; Anderson, A.S.; Ghafourian, K.; Khan, S.S.; Vorovich, E.E.; Rich, J.D.; et al. Prognostic Value of Myocardial Extracellular Volume Fraction and T2-mapping in Heart Transplant Patients. JACC Cardiovasc. Imaging 2020, 13, 1521–1530. [Google Scholar] [CrossRef]
- Hundley, W.G.; Bluemke, D.A.; Finn, J.P.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Ho, V.B.; Jerosch-Herold, M.; Kramer, C.M.; Manning, W.J.; et al. ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J. Am. Coll Cardiol. 2010, 55, 2614–2662. [Google Scholar] [CrossRef]
- Rudolph, A.; Abdel-Aty, H.; Bohl, S.; Boyé, P.; Zagrosek, A.; Dietz, R.; Schulz-Menger, J. Noninvasive detection of fibrosis applying contrast-enhanced cardiac magnetic resonance in different forms of left ventricular hypertrophy relation to remodeling. J. Am. Coll Cardiol. 2009, 53, 284–291. [Google Scholar] [CrossRef]
- Iyer, N.R.; Le, T.T.; Kui, M.S.L.; Tang, H.C.; Chin, C.T.; Phua, S.-K.; Bryant, J.A.; Pua, C.-J.; Ang, B.; Toh, D.-F.; et al. Markers of Focal and Diffuse Nonischemic Myocardial Fibrosis Are Associated With Adverse Cardiac Remodeling and Prognosis in Patients With Hypertension: The REMODEL Study. Hypertension 2022, 79, 1804–1813. [Google Scholar] [CrossRef]
- Burchell, A.E.; Rodrigues, J.C.L.; Charalambos, M.; Ratcliffe, L.E.K.; Hart, E.C.; Paton, J.F.R.; Baumbach, A.; Manghat, N.E.; Nightingale, A.K. Comprehensive First-Line Magnetic Resonance Imaging in Hypertension: Experience From a Single-Center Tertiary Referral Clinic. J. Clin. Hypertens. 2017, 19, 13–22. [Google Scholar] [CrossRef]
- Arcari, L.; Hinojar, R.; Engel, J.; Freiwald, T.; Platschek, S.; Zainal, H.; Zhou, H.; Vasquez, M.; Keller, T.; Rolf, A.; et al. Native T1 and T2 provide distinctive signatures in hypertrophic cardiac conditions—Comparison of uremic, hypertensive and hypertrophic cardiomyopathy. Int. J. Cardiol. 2020, 306, 102–108. [Google Scholar] [CrossRef]
- Chapman, A.R.; Shah, A.S.V.; Lee, K.K.; Anand, A.; Francis, O.; Adamson, P.; McAllister, D.A.; Strachan, F.E.; Newby, D.E.; Mills, N.L. Long-Term Outcomes in Patients With Type 2 Myocardial Infarction and Myocardial Injury. Circulation 2018, 137, 1236–1245. [Google Scholar] [CrossRef]
- Aquaro, G.D.; De Gori, C.; Faggioni, L.; Parisella, M.L.; Cioni, D.; Lencioni, R.; Neri, E. Diagnostic and prognostic role of late gadolinium enhancement in cardiomyopathies. Eur. Heart J. Suppl. 2023, 25 (Suppl. C), C130–C136. [Google Scholar] [CrossRef] [PubMed]
- Treibel, T.A.; Zemrak, F.; Sado, D.M.; Banypersad, S.M.; White, S.K.; Maestrini, V.; Barison, A.; Patel, V.; Herrey, A.S.; Davies, C.; et al. Extracellular volume quantification in isolated hypertension—changes at the detectable limits? J. Cardiovasc. Magn. Reson. 2015, 17, 74. [Google Scholar] [CrossRef] [PubMed]
- Doeblin, P.; Hashemi, D.; Tanacli, R.; Lapinskas, T.; Gebker, R.; Stehning, C.; Motzkus, L.A.; Blum, M.; Tahirovic, E.; Dordevic, A.; et al. CMR Tissue Characterization in Patients with HFmrEF. J. Clin. Med. 2019, 8, 1877. [Google Scholar] [CrossRef]
- Verbrugge, F.H.; Bertrand, P.B.; Willems, E.; Gielen, E.; Mullens, W.; Giri, S.; Wilson Tang, W.H.; Raman, S.V.; Verhaert, D. Global myocardial oedema in advanced decompensated heart failure. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 787–794. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Hypertensive Crisis (n = 43) | p | |
|---|---|---|---|
| Troponin-Negative Controls (n = 24) | Troponin-Positive Unobstructed Coronary Arteries (n = 19) | ||
| Age (years) | 47 ± 14 | 57 ± 11 | 0.015 |
| Females, n (%) | 16 (67) | 7 (37) | 0.052 |
| Systolic blood pressure (mmHg) | 218 ± 28 | 204 ± 28 | 0.103 |
| Diastolic blood pressure (mmHg) | 125 ± 19 | 124 ± 21 | 0.871 |
| Nonadherence, n (%) | 10/17 (59) | 5/15 (33) | ns |
| Creatinine (µmol/L) | 83 (69 to 101) | 104 (91 to 117) | 0.004 |
| Haemoglobin (g/L) | 13.8 ± 1.5 | 15.1 ± 2 | 0.002 |
| hs cTnT (ng/L) | 10 (6 to 11) | 130 (46 to 219) | <0.001 |
| NT-proBNP (ng/L) | 77 (22 to 396) | 433 (99 to 1448) | 0.025 |
| QRS duration | 88 (77 to 102) | 94 (83 to 106) | ns |
| QTc | 451 (432 to 470) | 465 (443 to 515) | 0.051 |
| LVH by SL, n (%) | 6/21 | 8/16 | 0.045 |
| LVH by CV, n (%) | 11/21 | 6/16 (38) | ns |
| ST depression, n (%) | 4/21 | 6/16 (38) | ns |
| T-wave inversion, n (%) | 8/21 (38) | 13/16 (81) | 0.009 |
| Deep T-wave inversion, n (%) | 2/21 (10) | 6/16 (38) | 0.030 |
| Pathological Q wave, n (%) | 1/21 | 0/16 | ns |
| Comorbidities: | |||
| Duration of hypertension (years) | 12 (8 to 26) | 12 (3 to 12) | ns |
| Previous MI, n (%) | 0 (0) | 1 (5) | ns |
| Chronic kidney disease, n (%) | 1 (4.2) | 5 (26) | 0.037 |
| Diabetes mellitus, n (%) | 5 (21) | 0 (0) | 0.034 |
| Dyslipidemia, n (%) | 3 (13) | 9 (47) | 0.011 |
| Smoking, n (%) | 6 (25) | 5 (26) | ns |
| Symptoms and clinical findings: | |||
| Chest pain, n (%) | 8 (33) | 18 (95) | <0.001 |
| Cough, n (%) | 2 (8) | 9 (47) | 0.004 |
| Shortness of breath, n (%) | 4 (17) | 11 (58) | 0.005 |
| NYHA class III–IV, n (%) | 1 (4) | 9/19 (47) | <0.001 |
| Palpitations, n (%) | 7 (29) | 16 (84) | <0.001 |
| Cardiac medications: | |||
| Aldosterone antagonist, n (%) | 3 (13) | 1 (5) | ns |
| Beta-blocker, n (%) | 11 (46) | 19 (100) | <0.001 |
| Calcium channel blocker, n (%) | 21 (88) | 9 (47) | 0.004 |
| Loop diuretic, n (%) | 3 (13) | 6 (32) | ns |
| RAS inhibitor, n (%) | 19 (79) | 19 (100) | 0.034 |
| Thiazide diuretic, n (%) | 13 (54) | 1 (5) | <0.001 |
| Platelet inhibitor, n (%) | 8 (33) | 19 (100) | <0.001 |
| Statin, n (%) | 10 (42) | 19 (100) | <0.001 |
| Variable | Troponin-Negative Controls (n = 24) | Troponin-Positive, Unobstructed Coronary Arteries (n = 19) | p |
|---|---|---|---|
| Indexed LV EDV (mL/m2) | 65 (59 to 71) | 85 (68 to 100) | <0.001 |
| Indexed LV ESV (mL/m2) | 22 (16 to 32) | 36 (24 to 70) | 0.005 |
| LV ejection fraction (%) | 63 ± 12 | 52 ± 16 | 0.019 |
| Indexed LV mass (g/m2) | 80 (67 to 103) | 100 (79 to 133) | 0.017 |
| LV systolic dysfunction, n (%) | 4(17) | 10(53) | 0.012 |
| Maximum wall thickness (mm) | 14 ± 2.4 | 14.5 ± 2 | 0.483 |
| LVH, n (%) | 13 (54) | 14 (74) | 0.221 |
| Asymmetric LVH, n (%) | 4 (17) | 2 (11) | 0.678 |
| Indexed LA volume (mL/m2) | 30 (28 to 36) | 44 (32 to 56) | <0.001 |
| Global T2-w SI ratio | 1.4 ± 0.2 | 1.4 ± 0.1 | 0.551 |
| Global native T1 (ms) | 1026 ± 39 | 1042 ± 40 | 0.198 |
| Global T2 relaxation time (ms) | 47 ± 2 | 49 ± 2 | 0.004 |
| Global ECV (%) | 23 ± 3 | 25 ± 4 | 0.047 |
| LGE present, n (%) | 12/24 (50) | 14/17 (82) | 0.050 |
| Infarct pattern, n (%) | 0 (0) | 5/17 (29) | - |
| Non-ischaemic, n (%) | 12/24 (50) | 9/17 (53) | 0.445 |
| Native T1 Time, ms | T2 Relaxation Time, ms | ECV, % | |
|---|---|---|---|
| Native T1 time (ms) | - | 0.623, p = 0.004 | ns |
| T2 relaxation time (ms) | 0.623, p = 0.004 | - | 0.645, p = 0.044 |
| Indexed LV mass (g/m2) | ns | ns | ns |
| NT-proBNP (ng/L) | ns | ns | ns |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age (years) | 1.064 (1.008 to 1.122) | 0.024 | ns | ns |
| Creatinine (µmol/L) | 1.034 (1.004 to 1.064) | 0.024 | 1.041 (0.991 to 1.093) | 0.111 |
| LDH (U/L) | 1.013 (1.002 to 1.024) | 0.025 | ns | ns |
| NT-proBNP (ng/L) | 1.001 (1.000 to 1.002) | 0.117 | - | - |
| Indexed LV EDV (mL/m2) | 1.067 (1.014 to 1.123) | 0.012 | 1.089 (1.010 to 1.173) | 0.026 |
| LV ejection fraction (%) | 0.943 (0.896 to 0.992) | 0.024 | ns | ns |
| Indexed LV mass (g/m2) | 1.024 (1.001 to 1.048) | 0.024 | 0.959 (0.914 to 1.005) | 0.080 |
| LVH, n (%) | 2.369 (0.646 to 8.685) | 0.193 | - | - |
| LGE, n (%) | 4.667 (1.061 to 20.533) | 0.042 | 2.739 (0.291 to 25.748) | 0.378 |
| Native T1 (ms) | 1.011 (0.994 to 1.027) | 0.198 | - | - |
| T2 relaxation time (ms) | 1.925 (1.160 to 3.193) | 0.011 | 2.097 (1.022 to 4.302) | 0.043 |
| T2-w SI ratio | 3.334 (0.020 to 158.2) | 0.541 | - | - |
| ECV (%) | 1.271 (0.988 to 1.634) | 0.062 | - | - |
| AUC (95% CI) | Sensitivity | Specificity | +LR | −LR | Criteria | p | |
|---|---|---|---|---|---|---|---|
| Age (years) | 0.71 (0.549 to 0.836) | 95 | 42 | 1.62 | 0.13 | >43 | 0.0090 |
| Creatinine (µmol/L) | 0.74 (0.578 to 0.857) | 90 | 63 | 2.39 | 0.17 | >85 | 0.0035 |
| NT-proBNP (ng/L) | 0.71 (0.544 to 0.838) | 50 | 87 | 3.83 | 0.58 | >477 | 0.0128 |
| Indexed LV EDV (mL/m2) | 0.80 (0.653 to 0.908) | 95 | 54 | 2.07 | 0.10 | >64.9 | <0.0001 |
| Lactate dehydrogenase (U/L) | 0.72 (0.550 to 0.852) | 93 | 44 | 1.65 | 0.15 | >207 | 0.0091 |
| Indexed LAV (mL/m2) | 0.82 (0.671 to 0.919) | 95 | 50 | 1.89 | 0.11 | >29.7 | <0.0001 |
| Indexed LV mass (g/m2) | 0.71 (0.555 to 0.840) | 68 | 70 | 2.35 | 0.45 | >92.1 | 0.0073 |
| LV ejection fraction (%) | 0.70 (0.538 to 0.828) | 53 | 75 | 2.11 | 0.63 | 55 | 0.0183 |
| Global native T1 time (ms) | 0.61 (0.449 to 0.755) | 52 | 83 | 3.16 | 0.57 | >1048 | 0.2269 |
| Global T2 relaxation time (ms) | 0.71 (0.552 to 0.838) | 84 | 58 | 2.02 | 0.27 | >47.2 | 0.0086 |
| Mid-ventricular T2 relaxation time (ms) | 0.73 (0576 to 0856) | 84 | 46 | 1.55 | 0.34 | >47.7 | 0.0031 |
| Global ECV fraction * (%) | 0.71 (0.518 to 0.852) | 70 | 73 | 2.57 | 0.41 | >23 | 0.0602 |
| Mid-ventricular ECV (%) | 0.77 (0.586 to 0.898) | 70 | 77 | 3.08 | 0.39 | >23 | 0.0061 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talle, M.A.; Doubell, A.F.; Robbertse, P.-P.S.; Lahri, S.; Herbst, P.G. Myocardial Tissue Characterization in Patients with Hypertensive Crisis, Positive Troponin, and Unobstructed Coronary Arteries: A Cardiovascular Magnetic Resonance-Based Study. Diagnostics 2023, 13, 2943. https://doi.org/10.3390/diagnostics13182943
Talle MA, Doubell AF, Robbertse P-PS, Lahri S, Herbst PG. Myocardial Tissue Characterization in Patients with Hypertensive Crisis, Positive Troponin, and Unobstructed Coronary Arteries: A Cardiovascular Magnetic Resonance-Based Study. Diagnostics. 2023; 13(18):2943. https://doi.org/10.3390/diagnostics13182943
Chicago/Turabian StyleTalle, Mohammed A., Anton F. Doubell, Pieter-Paul S. Robbertse, Sa’ad Lahri, and Philip G. Herbst. 2023. "Myocardial Tissue Characterization in Patients with Hypertensive Crisis, Positive Troponin, and Unobstructed Coronary Arteries: A Cardiovascular Magnetic Resonance-Based Study" Diagnostics 13, no. 18: 2943. https://doi.org/10.3390/diagnostics13182943