
Diagnostic and Prognostic Roles of C-Reactive Protein, Procalcitonin, and Presepsin in Acute Kidney Injury Patients Initiating Continuous Renal Replacement Therapy
 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
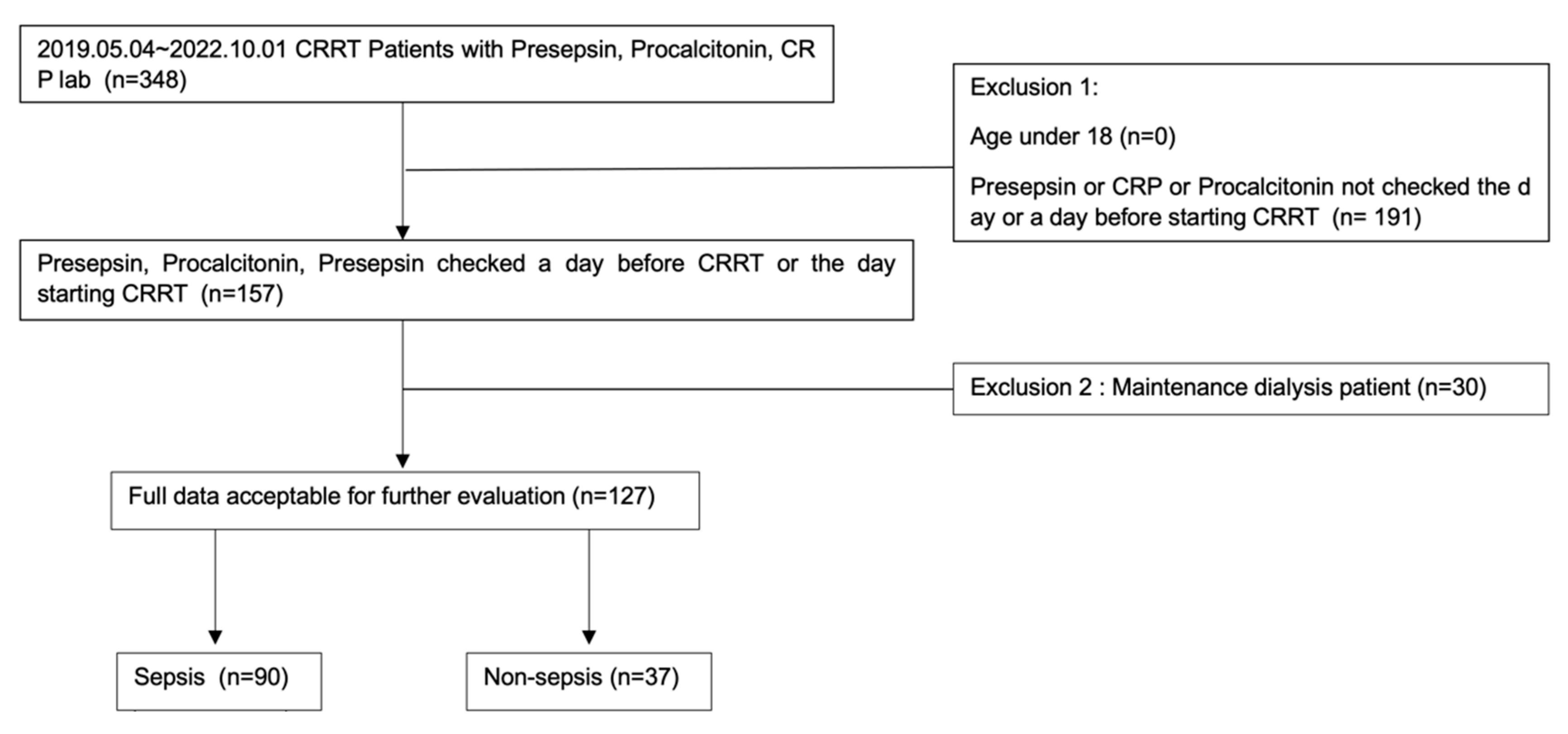
2.1. Study Design and Participants
2.2. Measurement
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Diagnostic Value of CRP, Procalcitonin, and Presepsin
3.3. Correlation between CRP, Procalcitonin, and Presepsin with Creatinine and eGFR
3.4. Prognostic Value of Procalcitonin and CRP in Sepsis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prasad, B.; Urbanski, M.; Ferguson, T.W.; Karreman, E.; Tangri, N. Early mortality on continuous renal replacement therapy (CRRT): The prairie CRRT study. Can. J. Kidney Health Dis. 2016, 3, 36. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Son, Y.J. Factors Associated with In-Hospital Mortality after Continuous Renal Replacement Therapy for Critically Ill Patients: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Heal. 2020, 17, 8781. [Google Scholar] [CrossRef]
- Druml, W. Systemic consequences of acute kidney injury. Curr. Opin. Crit. Care 2014, 20, 613–619. [Google Scholar] [CrossRef]
- Grams, M.E.; Rabb, H. The distant organ effects of acute kidney injury. Kidney Int. 2012, 81, 942–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, A.L.; Ravindran, S.; Saikant, R.; Lakshmi, S.; Kartik, R.; Manoj, G. Procalcitonin: A promising diagnostic marker for sepsis and antibiotic therapy. J. Intensiv. Care 2017, 5, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wacker, C.; Prkno, A.; Brunkhorst, F.M.; Schlattmann, P. Procalcitonin as a diagnostic marker for sepsis: A systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 426–435. [Google Scholar] [CrossRef]
- Li, S.; Rong, H.; Guo, Q.; Chen, Y.; Zhang, G.; Yang, J. Serum procalcitonin levels distinguish Gram-negative bacterial sepsis from Gram-positive bacterial and fungal sepsis. J. Res. Med. Sci. 2016, 21, 39. [Google Scholar] [CrossRef]
- Mihajlovic, D.; Brkic, S.; Uvelin, A.; Draskovic, B.; Vrsajkov, V. Use of presepsin and procalcitonin for prediction of SeptiFast results in critically ill patients. J. Crit. Care 2017, 40, 197–201. [Google Scholar] [CrossRef]
- Kan, W.C.; Huang, Y.T.; Wu, V.C.; Shiao, C.C. Predictive Ability of Procalcitonin for Acute Kidney Injury: A Narrative Review Focusing on the Interference of Infection. Int. J. Mol. Sci. 2021, 22, 6903. [Google Scholar] [CrossRef]
- Razeghi, E.; Parkhideh, S.; Ahmadi, F.; Khashayar, P. Serum CRP levels in pre-dialysis patients. Ren. Fail. 2008, 30, 193–198. [Google Scholar] [CrossRef]
- Park, J.H.; Kim, D.H.; Jang, H.R.; Kim, M.J.; Jung, S.H.; Lee, J.E.; Huh, W.; Kim, Y.G.; Kim, D.J.; Oh, H.Y. Clinical relevance of procalcitonin and C-reactive protein as infection markers in renal impairment: A cross-sectional study. Crit. Care 2014, 18, 640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nie, X.; Wu, B.; He, Y.; Huang, X.; Dai, Z.; Miao, Q.; Song, H.; Luo, T.; Gao, B.; Wang, L.; et al. Serum procalcitonin predicts development of acute kidney injury in patients with suspected infection. Clin. Chem. Lab. Med. 2013, 51, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, G.; Shibata, S.; Fukui, Y.; Okamura, Y.; Inoue, Y. Diagnostic accuracy of procalcitonin and presepsin for infectious disease in patients with acute kidney injury. Diagn. Microbiol. Infect. Dis. 2016, 86, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Murai, A.; Mizunuma, M.; Ohta, D.; Kawano, Y.; Matsumoto, N.; Nishida, T.; Ishikura, H. Potential use of procalcitonin as biomarker for bacterial sepsis in patients with or without acute kidney injury. J. Infect. Chemother. 2015, 21, 257–263. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, Y.; Hoshino, K.; Kiyomi, F.; Kawano, Y.; Mizunuma, M.; Tanaka, J.; Nishida, T.; Ishikura, H. Comparison of accuracy of presepsin and procalcitonin concentrations in diagnosing sepsis in patients with and without acute kidney injury. Clin. Chim. Acta 2019, 490, 200–206. [Google Scholar] [CrossRef]
- Nagata, T.; Yasuda, Y.; Ando, M.; Abe, T.; Katsuno, T.; Kato, S.; Tsuboi, N.; Matsuo, S.; Maruyama, S. Clinical impact of kidney function on presepsin levels. PLoS ONE 2015, 10, e0129159. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Song, J.; Park, D.W.; Seok, H.; Ahn, S.; Kim, J.; Park, J.; Cho, H.J.; Moon, S. Diagnostic and prognostic value of presepsin and procalcitonin in non-infectious organ failure, sepsis, and septic shock: A prospective observational study according to the Sepsis-3 definitions. BMC Infect. Dis. 2022, 22, 8. [Google Scholar] [CrossRef]
- Koh, J.S.; Kim, Y.J.; Kang, D.H.; Lee, J.E.; Lee, S.I. Usefulness of presepsin in predicting the prognosis of patients with sepsis or septic shock: A retrospective cohort study. Yeungnam Univ. J. Med. 2021, 38, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Hong, D.Y.; Lee, K.R.; Paik, J.H.; Jung, H.M. Plasma presepsin level predicts acute kidney injury in patients with sepsis in the emergency department. Medicine 2022, 101, e29919. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Chen, Y.X.; Yin, Q.; Zhao, Y.Z.; Li, C.S. Diagnostic value and prognostic evaluation of Presepsin for sepsis in an emergency department. Crit. Care 2013, 17, R244. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.L.; Nie, X.; Cai, B.; Tang, J.T.; He, Y.; Miao, Q.; Song, H.L.; Luo, T.X.; Gao, B.X.; Wang, L.L.; et al. Procalcitonin levels predict acute kidney injury and prognosis in acute pancreatitis: A prospective study. PLoS ONE 2013, 8, e82250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jekarl, D.W.; Lee, S.; Kim, M.; Kim, Y.; Woo, S.H.; Lee, W.J. Procalcitonin as a prognostic marker for sepsis based on SEPSIS-3. J. Clin. Lab. Anal. 2019, 33, e22996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enguix-Armada, A.; Escobar-Conesa, R.; García-De La Torre, A.; De La Torre-Prados, M.V. Usefulness of several biomarkers in the management of septic patients: C-reactive protein, procalcitonin, presepsin and mid-regional pro-adrenomedullin. Clin. Chem. Lab. Med. 2016, 54, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Sheng, S.; Zhang, Y.H.; Ma, H.K.; Huang, Y. Albumin levels predict mortality in sepsis patients with acute kidney injury undergoing continuous renal replacement therapy: A secondary analysis based on a retrospective cohort study. BMC Nephrol 2022, 23, 52. [Google Scholar] [CrossRef]
- Järvisalo, M.J.; Hellman, T.; Uusalo, P. Mortality and associated risk factors in patients with blood culture positive sepsis and acute kidney injury requiring continuous renal replacement therapy-A retrospective study. PLoS ONE 2021, 16, e0249561. [Google Scholar] [CrossRef]
- Kee, Y.K.; Kim, D.; Kim, S.J.; Kang, D.H.; Choi, K.B.; Oh, H.J.; Ryu, D.R. Factors Associated with Early Mortality in Critically Ill Patients Following the Initiation of Continuous Renal Replacement Therapy. J. Clin. Med. 2018, 7, 334. [Google Scholar] [CrossRef] [Green Version]
- Chen, S. Retooling the creatinine clearance equation to estimate kinetic GFR when the plasma creatinine is changing acutely. J. Am. Soc. Nephrol. 2013, 24, 877–888. [Google Scholar] [CrossRef] [Green Version]
- Inker, L.A.; Titan, S. Measurement and Estimation of GFR for Use in Clinical Practice: Core Curriculum 2021. Am. J. Kidney Dis. 2021, 78, 736–749. [Google Scholar] [CrossRef]
- Bragadottir, G.; Redfors, B.; Ricksten, S.E. Assessing glomerular filtration rate (GFR) in critically ill patients with acute kidney injury--true GFR versus urinary creatinine clearance and estimating equations. Crit. Care 2013, 17, R108. [Google Scholar] [CrossRef] [Green Version]
- Endre, Z.H.; Pickering, J.W.; Walker, R.J. Clearance and beyond: The complementary roles of GFR measurement and injury biomarkers in acute kidney injury (AKI). Am. J. Physiol. Physiol. 2011, 301, F697–F707. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, A.M.; Brown, J.R.; Sidhu, M.S.; Ramanath, V.S.; Devries, J.T.; Jayne, J.E.; Hettleman, B.D.; Friedman, B.J.; Niles, N.W., 2nd; Kaplan, A.V.; et al. The evaluation of creatinine clearance, estimated glomerular filtration rate and serum creatinine in predicting contrast-induced acute kidney injury among patients undergoing percutaneous coronary intervention. Cardiovasc. Revasc. Med. 2012, 13, 3–10. [Google Scholar] [CrossRef]
- Kirwan, C.J.; Philips, B.J.; Macphee, I.A. Estimated glomerular filtration rate correlates poorly with four-hour creatinine clearance in critically ill patients with acute kidney injury. Crit. Care Res. Pr. 2013, 2013, 406075. [Google Scholar] [CrossRef] [Green Version]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Inaguma, D.; Murata, M.; Tanaka, A.; Shinjo, H. Relationship between mortality and speed of eGFR decline in the 3 months prior to dialysis initiation. Clin. Exp. Nephrol. 2017, 21, 159–168. [Google Scholar] [CrossRef]
- Medina-Liabres, K.R.P.; Jeong, J.C.; Oh, H.J.; An, J.N.; Lee, J.P.; Kim, D.K.; Ryu, D.R.; Kim, S. Mortality predictors in critically ill patients with acute kidney injury requiring continuous renal replacement therapy. Kidney Res. Clin. Pr. 2021, 40, 401–410. [Google Scholar] [CrossRef]
- Haas, L.; Eckart, A.; Haubitz, S.; Mueller, B.; Schuetz, P.; Segerer, S. Estimated glomerular filtration rate predicts 30-day mortality in medical emergency departments: Results of a prospective multi-national observational study. PLoS ONE 2020, 15, e0230998. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 127) | Sepsis (n = 90) | Non-Sepsis (n = 37) | p-Value |
|---|---|---|---|---|
| Age, y | 69 (29–97) | 70.56 (39–97) | 65 (29–89) | 0.189 |
| Male, n (%) | 88 (69.3%) | 64 (71.1%) | 24 (64.9%) | 0.679 |
| Death, n (%) | 95 (74.8%) | 69 (76.7%) | 26 (70.3%) | 0.923 |
| Site of Infection | ||||
| Respiratory | 39 (43%) | |||
| Genitourinary | 8 (9%) | |||
| Gastrointestinal | 8 (9%) | |||
| Soft tissue | 6 (6%) | |||
| Fungal | 7 (7%) | |||
| Others | 22 (24%) | |||
| Positive blood culture | 29 | |||
| 30-day mortality | 81 (63.8%) | 62 (68.9%) | 19 (51.4%) | 0.565 |
| Hb (g/dL) | 9.75 (3.8–18.80) | 9.49 (3.8–15.10) | 10.72 (4.90–18.80) | 0.123 |
| Albumin (g/dL) | 2.74 (1.7–4.8) | 2.63 (1.7–4.10) | 3.03 (1.80–4.80) | 0.002 |
| Cr (mg/dL) | 2.76 (0.43–22) | 2.77 (0.43–22) | 2.57 (0.83–6.93) | 0.682 |
| eGFR (mL/min/1.73 m2) | 33.14 (2.0–145) | 31.99 (2–93) | 33.15 (7.0–74) | 0.891 |
| Phosphate (mg/dL) | 5.12 (1.4–16) | 5.20 (1.4–16) | 4.91 (1.50–9.50) | 0.613 |
| Potassium (mEq/L) | 4.47 (2.20–9.0) | 4.48 (2.2–9) | 4.26 (2.90–6.26) | 0.560 |
| Total Ca (mg/dL) | 7.42 (5.50–9.70) | 7.32 (5.50–9.40) | 7.72 (5.90–9.70) | 0.158 |
| WBC (×109/L) | 12,910 (10–55,770) | 12,614 (10–55,770) | 13,002 (1020–29,400) | 0.864 |
| Platelet (×103/µL) | 120 (5–471) | 110 (5–471) | 147 (41–289) | 0.186 |
| CRP (mg/dL) | 15.06 (0.1–40) | 19.48 (0.8–40) | 5 (0.50–23.20) | <0.001 |
| Presepsin (pg/mL) | 2802 (172–20,000) | 3204 (386–20,000) | 1578.95 (172–5822) | 0.003 |
| Procalcitonin (ng/mL) | 38.97 (0.05–200) | 51.04 (0.57–200) | 5.78 (0.05–48) | <0.001 |
| SOFA score | 11.66 (4.0–19.0) | 12.1 (4.0–19.0) | 1578 (172–5822) | 0.212 |
| Lactate (mmol/L) | 5.52 (0.70–20) | 5.56 (0.70–20) | 6.31 (1–17) | 0.509 |
| Organs | Main Principal Diagnoses | n |
|---|---|---|
| Cardiovascular (n = 13) | Heart failure | 3 |
| MI | 3 | |
| PTE | 2 | |
| Pulmonary hypertension | 1 | |
| Aortic dissection | 1 | |
| Others | 3 | |
| Respiratory (n = 1) | ILD | 1 |
| Hepatobiliary (n = 9) | Liver cirrhosis aggravation | 3 |
| Hepatitis | 5 | |
| Others | 1 | |
| Renal (n = 6) | CKD aggravation | 3 |
| AKI | 2 | |
| Others | 1 | |
| Bleeding (n = 3) | GI bleeding | 1 |
| Spleen rupture | 1 | |
| Hematoma | 1 | |
| Others (n = 5) | HLH | 1 |
| Hanging | 2 | |
| Catecholamine crisis | 1 | |
| Vasculitis | 1 |
| Marker | AUC (95%CI) | p Value | Cut-Off Value | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|
| Presepsin | 0.706 (0.604–0.808) | <0.001 | 1390 (pg/mL) | 66.7 | 67.5 |
| Procalcitonin | 0.845 (0.765–0.958) | <0.001 | 2.86 (ng/mL) | 81.1 | 81.0 |
| CRP | 0.901 (0.844–0.958) | <0.001 | 9.05 (mg/L) | 77.8 | 86.4 |
| Pearson Coefficient (r) | Significance (p-Value) | |
|---|---|---|
| eGFR | −0.137 | 0.124 |
| Presepsin | 0.098 | 0.271 |
| CRP | 0.471 | <0.001 |
| Cr | −0.14 | 0.873 |
| Age | −0.012 | 0.896 |
| WBC | −0.044 | 0.621 |
| Platelet | −0.220 | 0.013 |
| Lactate | 0.097 | 0.279 |
| Albumin | −0.185 | 0.038 |
| Hb | 0.127 | 0.155 |
| Na | −0.152 | 0.088 |
| p | 0.082 | 0.362 |
| TCa | −0.231 | 0.009 |
| K | −0.009 | 0.918 |
| SOFA score | 0.175 | 0.049 |
| Univariate HR (95% CI) | p-Value | Multivariate HR (95% CI) | p-Value | |
|---|---|---|---|---|
| Age | 1.010 (0.990–1.031) | 0.343 | 1.029 (1.006–1.052) | 0.012 |
| Sex | 1.328 (0.773–2.280) | 0.304 | ||
| Platelet | 0.997 (0.994–1.000) | 0.021 | 0.997 (0.995–1.000) | 0.040 |
| Lactate | 1.136 (1.076–1.199) | <0.001 | 1.081 (1.015–1.151) | 0.015 |
| Albumin | 0.443 (0.252–0.777) | 0.005 | 0.487 (0.258–0.919) | 0.026 |
| Hb | 0.922 (0.805–1.055) | 0.239 | ||
| eGFR | 1.015 (1.003–1.026) | 0.010 | 1.014 (1.002–1.026) | 0.019 |
| Cr | 0.941 (0.832–1.063) | 0.326 | ||
| SOFA score | 1.135 (1.061–1.213) | <0.001 | ||
| PCT ≥ 3.00 ng/mL | 2.061 (1.103–3.850) | 0.023 | ||
| CRP ≥ 31 mg/L | 2.079 (1.124–3.845) | 0.020 | 2.007 (1.036–3.887) | 0.039 |
| Presepsin ≥ 693 pg/mL | 1.921 (0.771–4.782) | 0.161 | ||
| K | 1.062 (0.886–1.272) | 0.517 | ||
| TCa | 0.807 (0.610–1.067) | 0.132 | ||
| p | 1.105 (1.009–1.210) | 0.032 | 1.165 (1.045–1.300) | 0.039 |
| Na | 1.012 (0.979–1.046) | 0.490 | ||
| CRP | 1.010 (0.988–1.032) | 0.395 | ||
| Presepsin | 1.00 (1.00–1.00) | 0.471 | ||
| PCT | 1.002 (0.998–1.005) | 0.306 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, S.; Kim, M.-J.; Ko, H.-J.; Lee, E.-J.; Kim, H.-R.; Jeon, J.-W.; Ham, Y.-R.; Na, K.-R.; Lee, K.-W.; Lee, S.-I.; et al. Diagnostic and Prognostic Roles of C-Reactive Protein, Procalcitonin, and Presepsin in Acute Kidney Injury Patients Initiating Continuous Renal Replacement Therapy. Diagnostics 2023, 13, 777. https://doi.org/10.3390/diagnostics13040777
Han S, Kim M-J, Ko H-J, Lee E-J, Kim H-R, Jeon J-W, Ham Y-R, Na K-R, Lee K-W, Lee S-I, et al. Diagnostic and Prognostic Roles of C-Reactive Protein, Procalcitonin, and Presepsin in Acute Kidney Injury Patients Initiating Continuous Renal Replacement Therapy. Diagnostics. 2023; 13(4):777. https://doi.org/10.3390/diagnostics13040777
Chicago/Turabian StyleHan, Suyeon, Moo-Jun Kim, Ho-Joon Ko, Eu-Jin Lee, Hae-Ri Kim, Jae-Wan Jeon, Young-Rok Ham, Ki-Ryang Na, Kang-Wook Lee, Song-I. Lee, and et al. 2023. "Diagnostic and Prognostic Roles of C-Reactive Protein, Procalcitonin, and Presepsin in Acute Kidney Injury Patients Initiating Continuous Renal Replacement Therapy" Diagnostics 13, no. 4: 777. https://doi.org/10.3390/diagnostics13040777