
Diagnostic Methods in Forensic Pathology: Autoptic Findings and Immunohistochemical Study in Cases of Sudden Death Due to a Colloid Cyst of the Third Ventricle
 , ,
, ,
Abstract
:1. Introduction
2. Case Report
2.1. Circumstantial Data
2.2. Autopsy
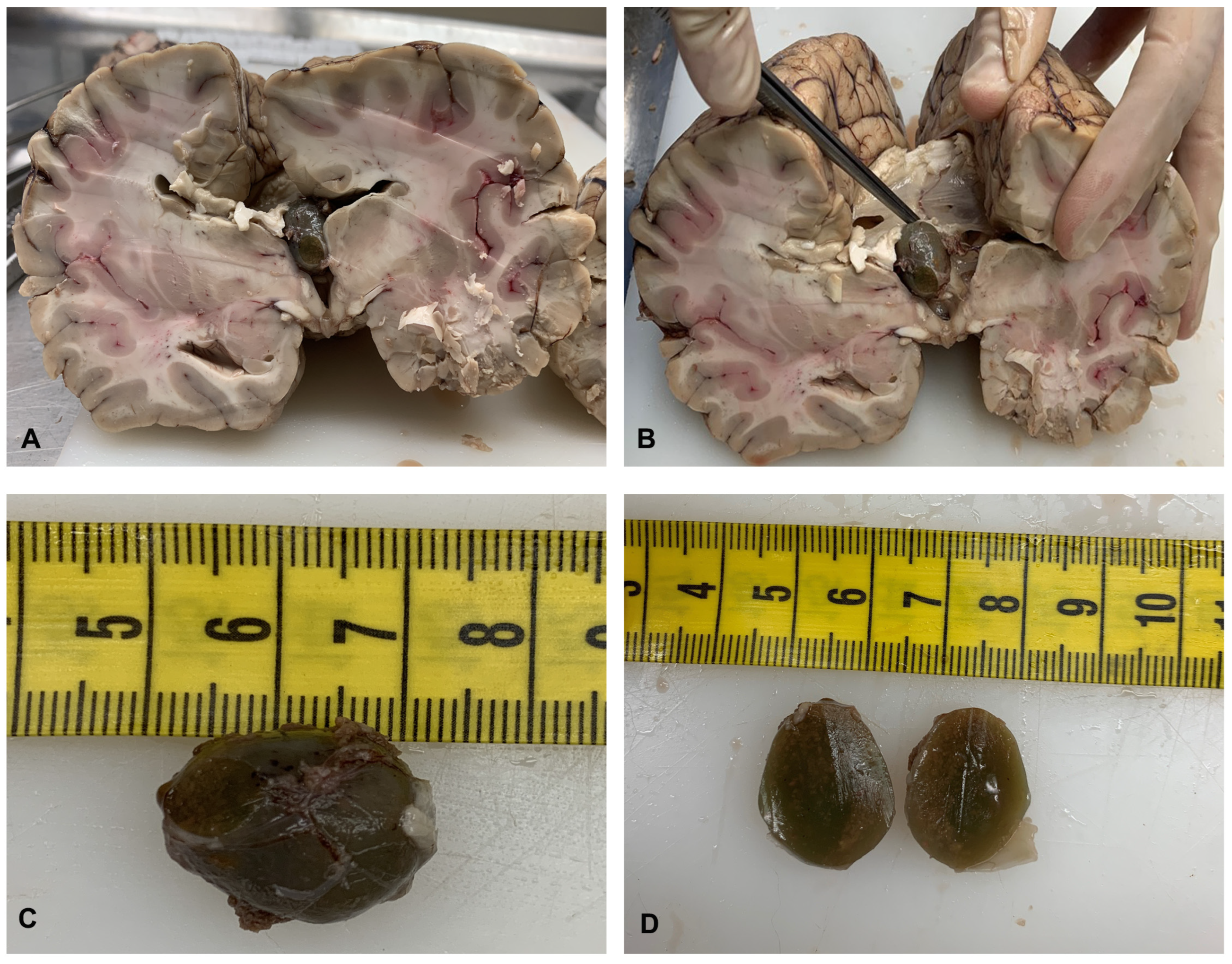
2.3. Gross Examination of the Brain after Formalin Fixation
2.4. Histological and Immunohistochemical Analysis of Colloid Cyst
2.5. Histological Analysis of Myocardial and Brain Tissue
2.6. Toxicological Analysis
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmed, S.I.; Javed, G.; Laghari, A.A.; Bareeqa, S.B.; Aziz, K.; Khan, M.; Samar, S.S.; Humera, R.A.; Khan, A.R.; Farooqui, M.O.; et al. Third Ventricular Tumors: A Comprehensive Literature Review. Cureus 2018, 10, e3417. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, G.M.; Raudino, G.; Visocchi, M.; Maione, M.; Certo, F. Out-of-third ventricle colloid cysts: Review of the literature on pathophysiology, diagnosis and treatment of an uncommon condition, with a focus on headache. J. Neurosurg. Sci. 2019, 63, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Pollock, B.E.; Schreiner, S.A.; Huston, J., 3rd. A theory on the natural history of colloid cysts of the third ventricle. Neurosurgery 2000, 46, 1077–1081; Discussion 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Di Trana, A.; Mannocchi, G.; Pirani, F.; Maida, N.L.; Gottardi, M.; Pichini, S.; Busardò, F.P. A comprehensive HPLC–MS-MS screening method for 77 new psychoactive substances, 24 classic drugs and 18 related metabolites in blood, urine and oral fluid. J. Anal. Toxicol. 2020, 44, 769–783. [Google Scholar] [CrossRef] [PubMed]
- Büttner, A.; Winkler, P.A.; Eisenmenger, W.; Weis, S. Colloid cysts of the third ventricle with fatal outcome: A report of two cases and review of the literature. Int. J. Legal Med. 1997, 110, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Tanei, T.; Fukui, K.; Kato, T.; Wakabayashi, K.; Inoue, N.; Watanabe, M. Colloid (enterogenous) cyst in the frontal lobe. Neurol. Med. Chir. 2006, 46, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Shaktawat, S.S.; Salman, W.D.; Twaij, Z.; Al-Dawoud, A. Unexpected death after headache due to a colloid cyst of the third ventricle. World J. Surg. Oncol. 2006, 4, 47. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.A.; Varma, T.R. An extraventricular colloid cyst: Case report. Br. J. Neurosurg. 1991, 5, 519–522. [Google Scholar] [CrossRef]
- Müller, A.; Büttner, A.; Weis, S. Rare occurrence of intracerebellar colloid cyst. Case report. J. Neurosurg. 1999, 91, 128–131. [Google Scholar] [CrossRef]
- Efkan, C.M.; Attar, A.; Ekinci, C.; Erdogan, A. Neuroepithelial (colloid) cyst of the parietal convexity. Acta Neurochir. 2000, 142, 1167–1168. [Google Scholar] [CrossRef]
- Inci, S.; Al-Rousan, N.; Söylemezoglu, F.; Gurçay, O. Intrapontomesencephalic colloid cyst: An unusual location. Case report. J. Neurosurg. 2001, 94, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Jan, M.; Ba Zeze, V.; Velut, S. Colloid cyst of the fourth ventricle: Diagnostic problems and pathogenic considerations. Neurosurgery 1989, 24, 939–942. [Google Scholar] [CrossRef] [PubMed]
- Torrey, J. Sudden death in an 11-year-old boy due to rupture of a colloid cyst of the third ventricle following ‘disco-dancing’. Med. Sci. Law 1983, 23, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Killer, H.E.; Flammer, J.; Wicki, B.; Laeng, R.H. Acute asymmetric upper nasal quandrantanopsia caused by a chiasmal colloid cyst in a patient with multiple sclerosis and bilateral retrobulbar neuritis. Am. J. Ophthalmol. 2001, 132, 286–288. [Google Scholar] [CrossRef] [PubMed]
- Jarquin-Valdivia, A.A.; Rich, A.T.; Yarbrough, J.L.; Thompson, R.C. Intraventricular colloid cyst, hydrocephalus and neurogenic stunned myocardium. Clin. Neurol. Neurosurg. 2005, 107, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Demirci, S.; Dogan, K.H.; Erkol, Z.; Gulmen, M.K. Sudden death due to a colloid cyst of the third ventricle: Report of three cases with a special sign at autopsy. Forensic Sci. Int. 2009, 189, e33–e36. [Google Scholar] [CrossRef] [PubMed]
- Turillazzi, E.; Bello, S.; Neri, M.; Riezzo, I.; Fineschi, V. Colloid cyst of the third ventricle, hypothalamus, and heart: A dangerous link for sudden death. Diagn. Pathol. 2012, 7, 144. [Google Scholar] [CrossRef]
- Al-Hashel, J.Y.; Rady, A.A.; Soliman, D.Y.; Vembu, P. Diagnostic Dilemma in a Young Woman with Acute Headache: Delayed Diagnosis of Third Ventricular Colloid Cyst with Hydrocephalus. Case Rep. Neurol. Med. 2015, 2015, 180404. [Google Scholar] [CrossRef]
- Cuoco, J.A.; Rogers, C.M.; Busch, C.M.; Benko, M.J.; Apfel, L.S.; Elias, Z. Postexercise Death Due to Hemorrhagic Colloid Cyst of Third Ventricle: Case Report and Literature Review. World Neurosurg. 2019, 123, 351–356. [Google Scholar] [CrossRef]
- Lagman, C.; Rai, K.; Chung, L.K.; Nagasawa, D.T.; Beckett, J.S.; Tucker, A.M.; Yang, I. Fatal Colloid Cysts: A Systematic Review. World Neurosurg. 2017, 107, 409–415. [Google Scholar] [CrossRef]
- Nelson, E.; Haymaker, W. Colloid cyst of the third ventricle in flyers; report of three fatal cases. J. Aviat. Med. 1957, 28, 356–363. [Google Scholar]
- De Witt Hamer, P.C.; Verstegen, M.J.; De Haan, R.J.; Vandertop, W.P.; Thomeer, R.T.; Mooij, J.J.; van Furth, W.R. High risk of acute deterioration in patients harboring symptomatic colloid cysts of the third ventricle. J. Neurosurg. 2002, 96, 1041–1045. [Google Scholar] [CrossRef] [PubMed]
- Rahmouni, K. Cardiovascular Regulation by the Arcuate Nucleus of the Hypothalamus: Neurocircuitry and Signaling Systems. Hypertension 2016, 67, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Cheung, R.T.; Hachinski, V. The insula and cerebrogenic sudden death. Arch. Neurol. 2000, 57, 1685–1688. [Google Scholar] [CrossRef] [PubMed]
- Samuels, M.A. Neurogenic heart disease: A unifying hypothesis. Am. J. Cardiol. 1987, 60, 15J–19J. [Google Scholar] [CrossRef]
- Ryder, J.W.; Kleinschmidt-DeMasters, B.K.; Keller, T.S. Sudden deterioration and death in patients with benign tumors of the third ventricle area. J. Neurosurg. 1986, 64, 216–223. [Google Scholar] [CrossRef]
- Nguyen, H.; Zaroff, J.G. Neurogenic stunned myocardium. Curr. Neurol. Neurosci. Rep. 2009, 9, 486–491. [Google Scholar] [CrossRef]
- Wira, C.R., 3rd; Rivers, E.; Martinez-Capolino, C.; Silver, B.; Iyer, G.; Sherwin, R.; Lewandowski, C. Cardiac complications in acute ischemic stroke. West. J. Emerg. Med. 2011, 12, 414–420. [Google Scholar] [CrossRef]
- Oppenheimer, S.M.; Cechetto, D.F.; Hachinski, V.C. Cerebrogenic cardiac arrhythmias. Cerebral electrocardiographic influences and their role in sudden death. Arch. Neurol. 1990, 47, 513–519. [Google Scholar] [CrossRef]
- Nef, H.M.; Möllmann, H.; Troidl, C.; Kostin, S.; Böttger, T.; Voss, S.; Hilpert, P.; Krause, N.; Weber, M.; Rolf, A.; et al. Expression profiling of cardiac genes in Tako-Tsubo cardiomyopathy: Insight into a new cardiac entity. J. Mol. Cell. Cardiol. 2008, 44, 395–404. [Google Scholar] [CrossRef]
- De-Giorgio, F.; Arena, V. Ostial plication: A rarely reported cause of sudden death. Diagn. Pathol. 2010, 5, 15. [Google Scholar] [CrossRef]
- Neri, M.; Cerretani, D.; Fiaschi, A.I.; Laghi, P.F.; Lazzerini, P.E.; Maffione, A.B.; Micheli, L.; Bruni, G.; Nencini, C.; Giorgi, G.; et al. Correlation between cardiac oxidative stress and myocardial pathology due to acute and chronic norepinephrine administration in rats. J. Cell. Mol. Med. 2007, 11, 156–170. [Google Scholar] [CrossRef]
- Bello, S.; Neri, M.; Riezzo, I.; Othman, M.S.; Turillazzi, E.; Fineschi, V. Cardiac beriberi: Morphological findings in two fatal cases. Diagn. Pathol. 2011, 6, 8. [Google Scholar] [CrossRef]
- Koleva, M.; De Jesus, O. Hydrocephalus. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Shoyab, M. Brainstem death due to intracranial hypertension with hydrocephalus, produced by a third ventricular colloid cyst. BJR Case Rep. 2022, 8, 20220007. [Google Scholar] [CrossRef]
- Munakomi, S.; Das, J.M. Brain Herniation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Silbergeld, D.L.; Rostomily, R.C.; Alvord, E.C., Jr. The cause of death in patients with glioblastoma is multifactorial: Clinical factors and autopsy findings in 117 cases of supratentorial glioblastoma in adults. J. Neurooncol. 1991, 10, 179–185. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) Sex | Cyst Size (cm), Localization | Symptoms and Onset | Cause of Death | Histology Findings/Immunohistochemistry | Authors |
|---|---|---|---|---|---|
| 11 M | 1.5 cm in diameter; inside the third ventricle | 18-day history of severe headache after 5 min of “head-banging” | Cyst: blood clot with central hemolysis, encapsulated by fibrin and “debris” containing hemosiderin-laden macrophages/ Strongly PAS positive | Torrey (1983) [13] | |
| 21 F | In the fourth ventricle and extended to the inferior part of the third ventricle | 3-year history of intracranial hypertension, occipital headache radiating to the cervical region, nausea, occasional vomiting | Underwent neurosurgery | Jan et al. (1989) [12] | |
| 33 F | In the right frontoparietal cerebral hemisphere | Focal epilepsy involving the left arm | Underwent neurosurgery | Cyst wall: cuboidal and ciliated columnar epithelial lining | Campbell et al. (1991) [8] |
| 40 F | 1 cm in diameter, inside the third ventricle near the foramen of Monro | Vomit and frontal headache after an intercontinental air flight | Brainstem compression caused by obstruction of the third ventricle | Cyst: lined by a single layer of flattened, non-ciliated epithelial cells, resting on a collagenous membrane/Strongly PAS-positive Brain: edema, hypoxic nerve cell changes, moderate nerve cell loss | Büttner et al. (1997) [5] |
| 33 M | 4 × 3.5 × 3.5 cm, inside the third ventricle | Recurrent headaches | Cyst: lined by a single layer of partially low cuboidal, partially flattened, non-ciliated, and ciliated epithelial cells, resting on a thin collagenous membrane/Strongly PAS positive Brain: extensive edema, hypoxic nerve cell changes | ||
| 45 F | 5 × 4 cm, extending dorsally to the surface of the cerebellum, medially to the cerebellar vermis, pressing the fourth ventricle | Signs of increased intracranial pressure, diffuse headache, gait disturbance and nausea | Underwent neurosurgery | Cyst: single layer of partly ciliated columnar epithelial cells resting on a basal lamina/Strongly PAS, collagen type IV, EMA, and S-100 protein positive | Müller et al. (1999) [9] |
| 34 M | 5 cm in diameter, in the parietal region | Seizures | Underwent neurosurgery | Cyst: stratified ciliated columnar epithelium | Efkan et al. (2000) [10] |
| 15 F | At the ventral portion of the ponto-mesencephalic junction | 3-month history of headache and diplopia | Underwent neurosurgery | Cyst: collagenous capsule lined by a single layer of non-ciliated epithelium that ranged morphologically from cuboidal to slightly columnar/Positive immunoreactivity to cytokeratin | Inci et al. (2001) [11] |
| 36 F | Optic chiasm | Sensorimotor hemi-syndrome, retrobulbar neuritis, acute asymmetric upper nasal quadrantanopsia | Underwent neurosurgery | Cyst: columnar and ciliated epithelial lining | Killer et al. (2001) [14] |
| 33 F | 1.2 cm, at the foramen of Monro in the third ventricle | 3- to 5-day history of headache, neck pain, nausea, emesis | Underwent neurosurgery | Jarquin-Valdivia et al. (2005) [15] | |
| 17 F | 1 cm, inside the third ventricle | 2-year history of intermittent headaches | Dilated ventricular system secondary to blockage of the third ventricle, intrapulmonary hemorrhage associated with congestion and edema | Shaktawat et al. (2006) [7] | |
| 60 M | 5 cm in diameter, in the left frontal lobe | Asymptomatic | Underwent neurosurgery | Cyst: inside the third ventricle/ Positive for cytokeratin end epithelial membrane antigen (EMA) | Tanei et al. (2006) [6] |
| 24 F | 2 cm in diameter, inside the third ventricle near the foramen of Monro | 12-month history of migraine headaches | Sudden death due to colloid cysts of the third ventricle | Cyst: a single layer of non-ciliated columnar epithelial cells with pale eosinophilic cytoplasm resting on a fibro-collagenous membrane/ Strongly positive for mucicarmine staining | Demirci et al. (2009) [16] |
| 21 F | 2 cm in diameter, in the third ventricle | 6-month history of migraine headaches | |||
| 25 M | 2.5 × 2.5 × 2 cm, inside the third ventricle | Headaches and vomiting for 3 days before the death | |||
| 10 M | 2 cm in diameter, filling the third ventricle | Severe headache, vomiting attacks | Acute cardiac arrest due to hypothalamus stimulation | Cyst: single stratum of cuboidal, semi-flattened, unciliated, and ciliated epithelial cells lying on a thin collagenous membrane/ Strongly PAS positive Brain: severe edema Heart: hypercontracted myocardial cells, short sarcomeres, very thick Z lines, myofibrils rhexis into cross-fiber | Turillazzi et al. (2012) [17] |
| 22 F | 1.22 × 1.47 × 1. 23 cm, at the foramen of Monro | 2-days of global bitemporal headache, nausea and vomiting | Brain dead 7 days after | Al-Hashel et al. (2015) [18] | |
| 21 M | 1.3 cm in diameter, in the third ventricle | Acute onset of a severe headache, nausea, vomiting, and past migraines in the last months | Brain dead after 5 days for acute obstructive hydrocephalus, cerebral edema, and uncal herniation. | Cuoco et al. (2018) [19] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montana, A.; Busardò, F.P.; Tossetta, G.; Goteri, G.; Castaldo, P.; Basile, G.; Bambagiotti, G. Diagnostic Methods in Forensic Pathology: Autoptic Findings and Immunohistochemical Study in Cases of Sudden Death Due to a Colloid Cyst of the Third Ventricle. Diagnostics 2024, 14, 100. https://doi.org/10.3390/diagnostics14010100
Montana A, Busardò FP, Tossetta G, Goteri G, Castaldo P, Basile G, Bambagiotti G. Diagnostic Methods in Forensic Pathology: Autoptic Findings and Immunohistochemical Study in Cases of Sudden Death Due to a Colloid Cyst of the Third Ventricle. Diagnostics. 2024; 14(1):100. https://doi.org/10.3390/diagnostics14010100
Chicago/Turabian StyleMontana, Angelo, Francesco Paolo Busardò, Giovanni Tossetta, Gaia Goteri, Pasqualina Castaldo, Giuseppe Basile, and Giulia Bambagiotti. 2024. "Diagnostic Methods in Forensic Pathology: Autoptic Findings and Immunohistochemical Study in Cases of Sudden Death Due to a Colloid Cyst of the Third Ventricle" Diagnostics 14, no. 1: 100. https://doi.org/10.3390/diagnostics14010100