
Comparison of Disease Severity Classifications of Chronic Obstructive Pulmonary Disease: GOLD vs. STAR in Clinical Practice

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
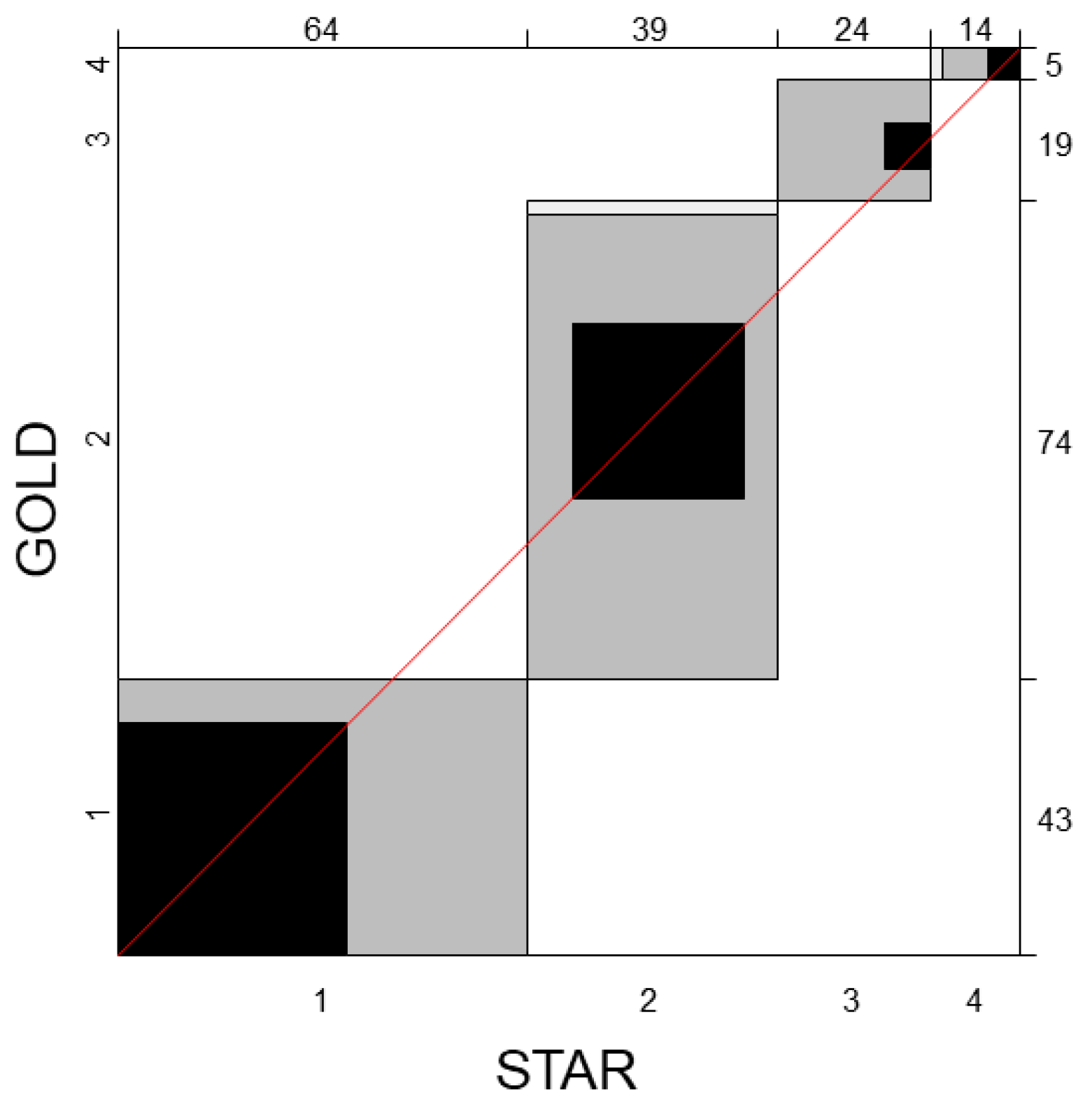
3.2. Concordance between GOLD and STAR
3.3. COPD-Specific Health Status
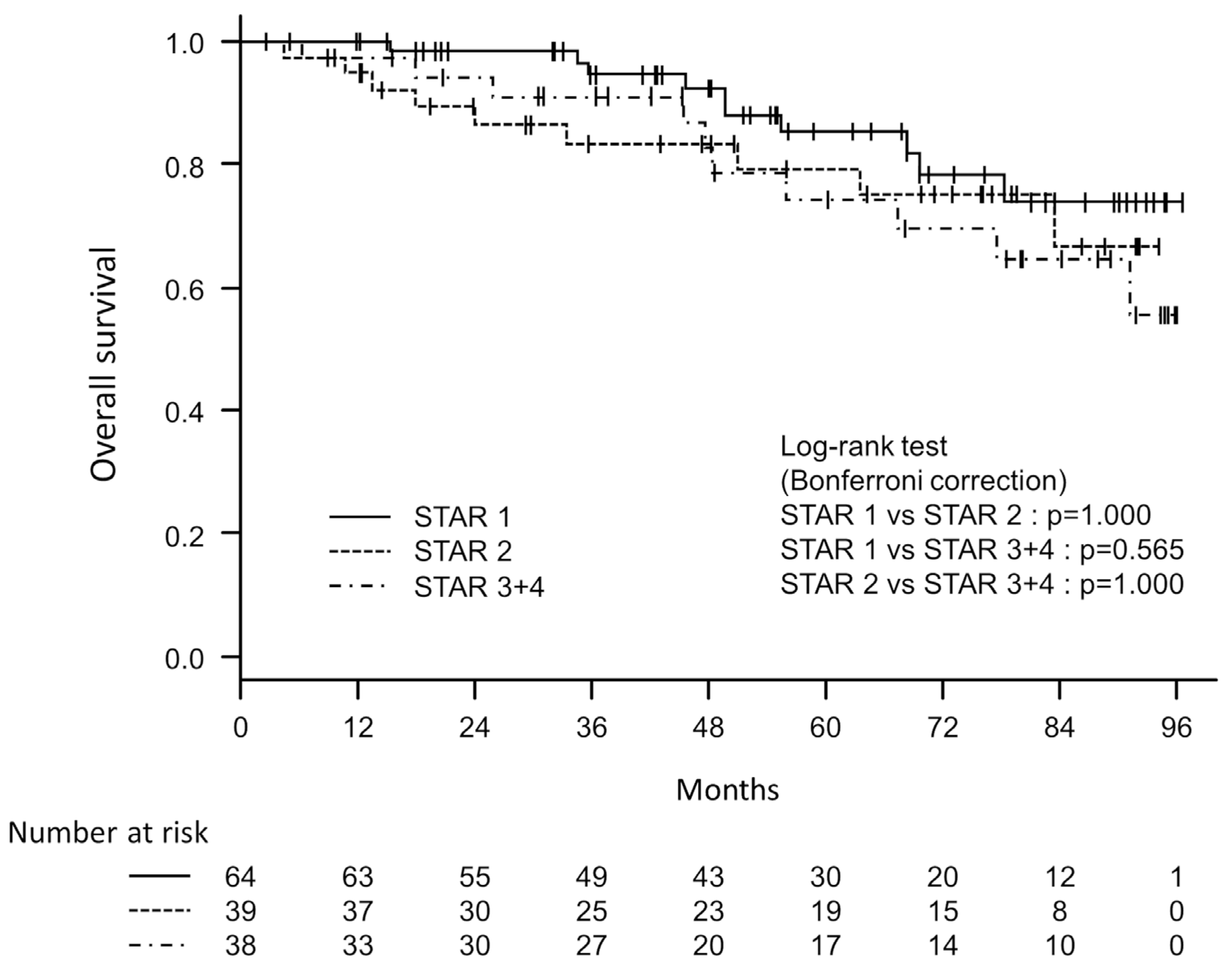
3.4. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pauwels, R.A.; Buist, A.S.; Calverley, P.M.; Jenkins, C.R.; Hurd, S.S.; Committee, G.S. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am. J. Respir. Crit. Care Med. 2001, 163, 1256–1276. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; Montes de Oca, M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2023, 207, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Izumi, T.; Tsukino, M.; Oga, T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest 2002, 121, 1434–1440. [Google Scholar] [CrossRef] [PubMed]
- Waschki, B.; Kirsten, A.; Holz, O.; Muller, K.C.; Meyer, T.; Watz, H.; Magnussen, H. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: A prospective cohort study. Chest 2011, 140, 331–342. [Google Scholar] [CrossRef]
- Casanova, C.; Cote, C.; Marin, J.M.; Pinto-Plata, V.; de Torres, J.P.; Aguirre-Jaime, A.; Vassaux, C.; Celli, B.R. Distance and oxygen desaturation during the 6-min walk test as predictors of long-term mortality in patients with COPD. Chest 2008, 134, 746–752. [Google Scholar] [CrossRef]
- O’Donnell, D.E.; Parker, C.M. COPD exacerbations · 3: Pathophysiology. Thorax 2006, 61, 354–361. [Google Scholar] [CrossRef]
- Celli, B.R.; Barnes, P.J. Exacerbations of chronic obstructive pulmonary disease. Eur. Respir. J. 2007, 29, 1224–1238. [Google Scholar] [CrossRef]
- Jones, P.; Harding, G.; Wiklund, I.; Berry, P.; Leidy, N. Improving the process and outcome of care in COPD: Development of a standardised assessment tool. Prim. Care Respir. J. 2009, 18, 208–215. [Google Scholar] [CrossRef]
- Jahagirdar, D.; Kroll, T.; Ritchie, K.; Wyke, S. Patient-reported outcome measures for chronic obstructive pulmonary disease: The exclusion of people with low literacy skills and learning disabilities. Patient 2013, 6, 11–21. [Google Scholar] [CrossRef]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef]
- Puhan, M.A.; Garcia-Aymerich, J.; Frey, M.; ter Riet, G.; Anto, J.M.; Agusti, A.G.; Gomez, F.P.; Rodriguez-Roisin, R.; Moons, K.G.; Kessels, A.G.; et al. Expansion of the prognostic assessment of patients with chronic obstructive pulmonary disease: The updated BODE index and the ADO index. Lancet 2009, 374, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.C.; Donaldson, G.C.; Chavannes, N.H.; Kida, K.; Dickson-Spillmann, M.; Harding, S.; Wedzicha, J.A.; Price, D.; Hyland, M.E. Derivation and validation of a composite index of severity in chronic obstructive pulmonary disease: The DOSE Index. Am. J. Respir. Crit. Care Med. 2009, 180, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Stahl, E.; Lindberg, A.; Jansson, S.A.; Ronmark, E.; Svensson, K.; Andersson, F.; Lofdahl, C.G.; Lundback, B. Health-related quality of life is related to COPD disease severity. Health Qual. Life Outcomes 2005, 3, 56. [Google Scholar] [CrossRef]
- Drummond, M.B.; Hansel, N.N.; Connett, J.E.; Scanlon, P.D.; Tashkin, D.P.; Wise, R.A. Spirometric predictors of lung function decline and mortality in early chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2012, 185, 1301–1306. [Google Scholar] [CrossRef] [PubMed]
- Vaz Fragoso, C.A.; Concato, J.; McAvay, G.; Van Ness, P.H.; Rochester, C.L.; Yaggi, H.K.; Gill, T.M. The ratio of FEV1 to FVC as a basis for establishing chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2010, 181, 446–451. [Google Scholar] [CrossRef]
- Hegewald, M.J.; Collingridge, D.S.; DeCato, T.W.; Jensen, R.L.; Morris, A.H. Airflow Obstruction Categorization Methods and Mortality. Ann. Am. Thorac. Soc. 2018, 15, 920–925. [Google Scholar] [CrossRef]
- Bhatt, S.P.; Balte, P.P.; Schwartz, J.E.; Cassano, P.A.; Couper, D.; Jacobs, D.R., Jr.; Kalhan, R.; O’Connor, G.T.; Yende, S.; Sanders, J.L.; et al. Discriminative Accuracy of FEV1:FVC Thresholds for COPD-Related Hospitalization and Mortality. JAMA 2019, 321, 2438–2447. [Google Scholar] [CrossRef]
- Bhatt, S.P.; Nakhmani, A.; Fortis, S.; Strand, M.J.; Silverman, E.K.; Sciurba, F.C.; Bodduluri, S. FEV(1)/FVC Severity Stages for Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2023, 208, 676–684. [Google Scholar] [CrossRef]
- Bhatt, S.P.; Nakhmani, A.; Fortis, S.; Strand, M.J.; Silverman, E.K.; Sciurba, F.C.; Bodduluri, S. Reply to Neder, to Ogata et al., and to Graham. Am. J. Respir. Crit. Care Med. 2024, 209, 343–345. [Google Scholar] [CrossRef]
- Calverley, P.M.A. A STAR Is Born: A New Approach to Assessing Chronic Obstructive Pulmonary Disease Severity. Am. J. Respir. Crit. Care Med. 2023, 208, 647–648. [Google Scholar] [CrossRef]
- Neder, J.A. Is This Really a New START in COPD? Am. J. Respir. Crit. Care Med. 2024, 209, 339–340. [Google Scholar] [CrossRef] [PubMed]
- Ogata, H.; Washio, Y.; Yoshida, M. Novel FEV(1)/FVC-based Diagnosis and Severity Classification of Chronic Obstructive Pulmonary Disease: How About FEV(1) Percent Predicted Basing? Am. J. Respir. Crit. Care Med. 2024, 209, 340–341. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.P.; Nakhmani, A.; Wilson, C.G.; Bodduluri, S. Optimal Threshold of FEV(t)/FVC Ratio for Detection of Airflow Limitation Associated with Structural Lung Disease. Am. J. Respir. Crit. Care Med. 2023, 208, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Kusunose, M.; Sanda, R.; Mori, M.; Shibayama, A.; Nakayasu, K. Comparison of Predictive Properties between Tools of Patient-Reported Outcomes: Risk Prediction for Three Future Events in Subjects with COPD. Diagnostics 2023, 13, 2269. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Kusunose, M.; Shibayama, A.; Nakayasu, K. Is Frailty a Mortality Predictor in Subjects with Chronic Obstructive Pulmonary Disease? Int. J. Chronic Obstr. Pulm. Dis. 2023, 18, 2955–2960. [Google Scholar] [CrossRef]
- Kusunose, M.; Oga, T.; Nakamura, S.; Hasegawa, Y.; Nishimura, K. Frailty and patient-reported outcomes in subjects with chronic obstructive pulmonary disease: Are they independent entities? BMJ Open Respir. Res. 2017, 4, e000196. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef]
- Sasaki, H.; Nakamura, M.; Kida, K.; Kambe, M.; Takahashi, K.; Fujimura, M. Reference values for spirogram and blood gas analysis in Japanese adults. J. Jpn. Respir. Soc. 2001, 39, S1–S17. [Google Scholar]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M.; Littlejohns, P. A self-complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. Am. Rev. Respir. Dis. 1992, 145, 1321–1327. [Google Scholar] [CrossRef]
- Hajiro, T.; Nishimura, K.; Tsukino, M.; Ikeda, A.; Koyama, H.; Izumi, T. Comparison of discriminative properties among disease-specific questionnaires for measuring health-related quality of life in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1998, 157, 785–790. [Google Scholar] [CrossRef]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef]
- Tsuda, T.; Suematsu, R.; Kamohara, K.; Kurose, M.; Arakawa, I.; Tomioka, R.; Kawayama, T.; Hoshino, T.; Aizawa, H. Development of the Japanese version of the COPD Assessment Test. Respir. Investig. 2012, 50, 34–39. [Google Scholar] [CrossRef]
- Severity of Illness. From Wikipedia, the Free Encyclopedia. Available online: https://en.wikipedia.org/wiki/Severity_of_illness (accessed on 1 January 2024).
- Disease Staging Software User Guide; Medstat Group, Inc.: Ann Arbor, MI, USA, 2001.
- Overview of Disease Severity Measures from The Agency for Healthcare Research and Quality (AHRQ). An Official Website of the Department of Health & Human Services. Available online: https://hcup-us.ahrq.gov/db/nation/nis/severity_overview.jsp (accessed on 1 January 2024).
- Fukuchi, Y.; Nishimura, M.; Ichinose, M.; Adachi, M.; Nagai, A.; Kuriyama, T.; Takahashi, K.; Nishimura, K.; Ishioka, S.; Aizawa, H.; et al. COPD in Japan: The Nippon COPD Epidemiology study. Respirology 2004, 9, 458–465. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mean ± SD | ||
|---|---|---|
| Age | years | 75.2 ± 6.7 |
| BMI | kg/m2 | 22.8 ± 3.3 |
| Cumulative smoking | pack-years | 59.1 ± 32.0 |
| FEV1 | Liters | 1.74 ± 0.54 |
| FEV1 | %pred | 69.8 ± 20.1 |
| FEV1/FVC | % | 56.0 ± 10.7 |
| RV | %pred | 124.6 ± 52.9 |
| RV/TLC | % | 45.0 ± 11.2 |
| DLco (1) | mL/min/mmHg | 11.99 ± 5.04 |
| PaO2 (2) | mmHg | 79.2 ± 9.0 |
| SGRQ total score | (0–100) | 22.6 ± 16.4 |
| CAT score | (0–40) | 8.6 ± 7.0 |
| Sex | male/female | 130/11 |
| GOLD stage | GOLD 1/GOLD 2/GOLD 3 + 4 | 43/74/24 (30.5%/52.5%/17.0%) |
| STAR stage | STAR 1/STAR 2/STAR 3 + 4 | 64/39/38 (45.4%/27.7%/27.0%) |
| GOLD 1 N = 43 (30.5%) | GOLD 2 N = 74 (52.5%) | GOLD 3 + 4 N = 24 (17.0%) | comparison between groups (p-value) | |||||||
| n | mean ± SD | n | mean ± SD | n | mean ± SD | GOLD 1 vs. 2 | GOLD 1 vs. 3 + 4 | GOLD 2 vs. 3 + 4 | ||
| Age | years | 43 | 74.6 ± 5.9 | 74 | 75.4 ± 7.4 | 24 | 75.7 ± 5.9 | 0.735 ‡ | 0.953 ‡ | 0.989 ‡ |
| BMI | kg/m2 | 43 | 23.4 ± 2.6 | 74 | 22.9 ± 3.7 | 24 | 21.6 ± 3.0 | 0.584 ‡ | 0.046 ‡ | 0.261 ‡ |
| TLC | %pred | 43 | 107.3 ± 16.8 | 74 | 104.8 ± 29.2 | 24 | 103.9 ± 22.5 | 0.575 ‡ | 0.443 ‡ | 0.985 ‡ |
| RV | %pred | 43 | 103.9 ± 25.5 | 74 | 129.3 ± 59.0 | 24 | 147.4 ± 58.2 | 0.024 ‡ | <0.001 ‡ | 0.111 ‡ |
| RV/TLC | % | 43 | 37.3 ± 5.2 | 74 | 46.7 ± 11.8 | 24 | 53.4 ± 9.1 | <0.001 ‡ | <0.001 ‡ | 0.003 ‡ |
| DLco | mL/min/mmHg | 43 | 13.59 ± 4.00 | 74 | 11.53 ± 4.69 | 23 | 10.46 ± 6.99 | 0.016 ‡ | 0.012 ‡ | 0.290 ‡ |
| Sex | male/female | 37 (26.2%)/6 (4.3%) | 69 (48.9%)/5 (3.5%) | 24 (17.0%)/0 (0%) | 0.627 † | 0.242 † | 0.990 † | |||
| SGRQ total score | (0–100) | 43 | 13.9 ± 9.5 | 74 | 22.2 ± 15.5 | 24 | 39.4 ± 16.8 | 0.011 ‡ | <0.001 ‡ | <0.001 ‡ |
| CAT score | (0–40) | 43 | 6.0 ± 5.1 | 74 | 8.0 ± 6.4 | 24 | 15.1 ± 7.8 | 0.250 ‡ | <0.001 ‡ | <0.001 ‡ |
| STAR 1 N = 64 (45.4%) | STAR 2 N = 39 (27.7%) | STAR 3 + 4 N = 38 (27.0%) | comparison between groups (p-value) | |||||||
| n | mean ± SD | n | mean ± SD | n | mean ± SD | STAR 1 vs. 2 | STAR 1 vs. 3 + 4 | STAR 2 vs. 3 + 4 | ||
| Age | years | 64 | 76.0 ± 6.2 | 39 | 74.9 ± 7.5 | 38 | 74.1 ± 6.8 | 0.730 ‡ | 0.152 ‡ | 0.612 ‡ |
| BMI | kg/m2 | 64 | 23.4 ± 3.3 | 39 | 22.9 ± 3.4 | 38 | 21.8 ± 2.9 | 0.326 ‡ | 0.035 ‡ | 0.401 ‡ |
| TLC | %pred | 64 | 101.5 ± 24.7 | 39 | 107.6 ± 27.1 | 38 | 109.8 ± 21.8 | 0.449 ‡ | 0.052 ‡ | 0.617 ‡ |
| RV | %pred | 64 | 110.1 ± 47.6 | 39 | 134.7 ± 61.9 | 38 | 138.8 ± 45.9 | 0.020 ‡ | <0.001 ‡ | 0.222 ‡ |
| RV/TLC | % | 64 | 42.0 ± 10.0 | 39 | 47.6 ± 13.9 | 38 | 47.3 ± 9.0 | 0.046 ‡ | <0.001 ‡ | 0.565 ‡ |
| DLco | mL/min/mmHg | 64 | 13.27 ± 4.49 | 39 | 12.32 ± 5.54 | 37 | 9.42 ± 4.54 | 0.274 ‡ | <0.001 ‡ | 0.053 ‡ |
| Sex | male/female | 56 (39.7%)/8 (5.7%) | 37 (26.2%)/2 (1.4%) | 37 (26.2%)/1 (0.7%) | 0.936 † | 0.445 † | 1.000 † | |||
| SGRQ total score | (0–100) | 64 | 19.1 ± 14.8 | 39 | 19.8 ± 14.4 | 38 | 31.4 ± 18.0 | 0.945 ‡ | <0.001 ‡ | 0.004 ‡ |
| CAT score | (0–40) | 64 | 6.7 ± 5.4 | 39 | 8.3 ± 6.9 | 38 | 12.1 ± 8.2 | 0.612 ‡ | 0.002 ‡ | 0.081 ‡ |
| STAR 1 | STAR 2 | STAR 3 | STAR 4 | |
| GOLD 1 | 36 (25.3%) | 7 (5.0%) | 0 (0%) | 0 (0%) |
| GOLD 2 | 28 (19.9%) | 27 (19.1%) | 17 (12.1%) | 2 (1.4%) |
| GOLD 3 | 0 (0%) | 5 (3.5%) | 7 (5.0%) | 7 (5.0%) |
| GOLD 4 | 0 (0%) | 0 (0%) | 0 (0%) | 5 (3.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimura, K.; Kusunose, M.; Shibayama, A.; Nakayasu, K. Comparison of Disease Severity Classifications of Chronic Obstructive Pulmonary Disease: GOLD vs. STAR in Clinical Practice. Diagnostics 2024, 14, 646. https://doi.org/10.3390/diagnostics14060646
Nishimura K, Kusunose M, Shibayama A, Nakayasu K. Comparison of Disease Severity Classifications of Chronic Obstructive Pulmonary Disease: GOLD vs. STAR in Clinical Practice. Diagnostics. 2024; 14(6):646. https://doi.org/10.3390/diagnostics14060646
Chicago/Turabian StyleNishimura, Koichi, Masaaki Kusunose, Ayumi Shibayama, and Kazuhito Nakayasu. 2024. "Comparison of Disease Severity Classifications of Chronic Obstructive Pulmonary Disease: GOLD vs. STAR in Clinical Practice" Diagnostics 14, no. 6: 646. https://doi.org/10.3390/diagnostics14060646