
Opportunistic CT for Prediction of Adverse Postoperative Events in Patients with Spinal Metastases
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.2. Participants and Clinical Characteristics
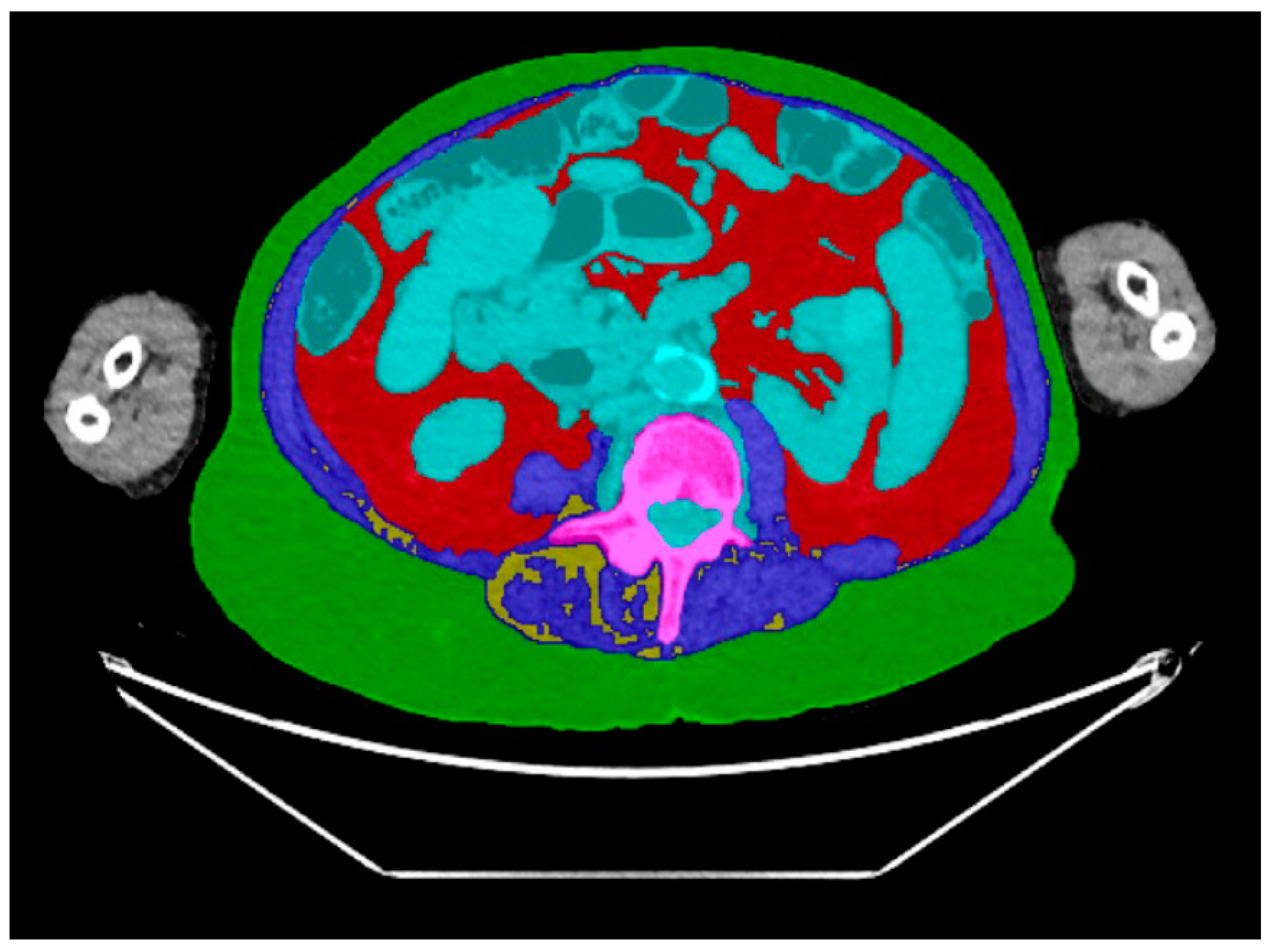
2.3. CT Body Composition Assessment
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patients and Characteristics
3.2. Length of Stay (LOS)
3.3. Postoperative Complications within 30 Days
3.4. Reoperations
4. Discussion
4.1. Future Implications
4.2. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yahanda, A.T.; Buchowski, J.M.; Wegner, A.M. Treatment, complications, and outcomes of metastatic disease of the spine: From Patchell to PROMIS. Ann. Transl. Med. 2019, 7, 216. [Google Scholar] [CrossRef] [PubMed]
- Ortiz Gómez, J.A. The incidence of vertebral body metastases. Int. Orthop. 1995, 19, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Spinal Metastases: The Obvious, the Occult, and the Impostor...: Spine. Available online: https://journals.lww.com/spinejournal/abstract/1990/01000/Spinal_Metastases__The_Obvious,_the_Occult,_and.1.aspx (accessed on 8 April 2024).
- Bongers, M.E.R.; Schwab, J.H. Modern Technical Concepts in Surgical Metastatic Disease. In Surgical Spinal Oncology; Springer: Cham, Switzerland, 2020; pp. 235–241. [Google Scholar] [CrossRef]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Payne, R.; Saris, S.; Kryscio, R.J.; Mohiuddin, M.; Young, B. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: A randomised trial. Lancet 2005, 366, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Nater, A.; Sahgal, A.; Fehlings, M. Management-spinal metastases. Handb. Clin. Neurol. 2018, 149, 239–255. [Google Scholar] [CrossRef] [PubMed]
- Pereira, N.R.P.; Groot, O.Q.; Verlaan, J.-J.; Bongers, M.E.; Twining, P.K.B.; Kapoor, N.D.; van Dijk, C.N.; Schwab, J.H.; Bramer, J.A. Quality of Life Changes After Surgery for Metastatic Spinal Disease. Clin. Spine Surg. A Spine Publ. 2021, 35, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Laufer, I.; Rubin, D.G.; Lis, E.; Cox, B.W.; Stubblefield, M.D.; Yamada, Y.; Bilsky, M.H. The NOMS Framework: Approach to the Treatment of Spinal Metastatic Tumors. Oncologist 2013, 18, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Ogink, P.T.; Groot, O.Q.; Karhade, A.V.; Bongers, M.E.R.; Oner, F.C.; Verlaan, J.-J.; Schwab, J.H. Wide range of applications for machine-learning prediction models in orthopedic surgical outcome: A systematic review. Acta Orthop. 2021, 92, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Karhade, A.V.; Thio, Q.C.B.S.; Ogink, P.T.; Bono, C.M.; Ferrone, M.L.; Oh, K.S.; Saylor, P.J.; Schoenfeld, A.J.; Shin, J.H.; Harris, M.B.; et al. Predicting 90-Day and 1-Year Mortality in Spinal Metastatic Disease: Development and Internal Validation. Clin. Neurosurg. 2019, 85, E671–E681. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, J.A.; Wedin, R.; Bauer, H.C.; Hansen, B.H.; Laitinen, M.; Trovik, C.S.; Keller, J.; Boland, P.J.; Healey, J.H. External validation of the Bayesian Estimated Tools for Survival (BETS) models in patients with surgically treated skeletal metastases. BMC Cancer 2012, 12, 493. [Google Scholar] [CrossRef]
- Schoenfeld, A.J.; Ferrone, M.L.; Schwab, J.H.; Blucher, J.A.; Barton, L.B.; Tobert, D.G.; Chi, J.H.; Shin, J.H.; Kang, J.D.; Harris, M.B. Prospective validation of a clinical prediction score for survival in patients with spinal metastases: The New England Spinal Metastasis Score. Spine J. 2021, 21, 28–36. [Google Scholar] [CrossRef]
- Fourney, D.R.; Frangou, E.M.; Ryken, T.C.; DiPaola, C.P.; Shaffrey, C.I.; Berven, S.H.; Bilsky, M.H.; Harrop, J.S.; Fehlings, M.G.; Boriani, S.; et al. Spinal instability neoplastic score: An analysis of reliability and validity from the spine Oncology Study Group. J. Clin. Oncol. 2011, 29, 3072–3077. [Google Scholar] [CrossRef] [PubMed]
- Groot, O.Q.B.; Ogink, P.T.; Janssen, S.J.; Pereira, N.R.P.; Lozano-Calderon, S.; Raskin, K.; Hornicek, F.; Schwab, J.H. High risk of venous thromboembolism after surgery for long bone metastases: A retrospective study of 682 patients. Clin. Orthop. Relat. Res. 2018, 476, 2052–2061. [Google Scholar] [CrossRef] [PubMed]
- Bindels, B.J.J.; Thio, Q.C.B.S.; Raskin, K.A.; Ferrone, M.L.; Lozano Calderón, S.A.; Schwab, J.H. Thirty-day Postoperative Complications After Surgery For Metastatic Long Bone Disease Are Associated With Higher Mortality at 1 Year. Clin. Orthop. Relat. Res. 2020, 478, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Twining, P.K.; Groot, O.Q.; Buckless, C.G.; Kapoor, N.D.; Bongers, M.E.R.; Janssen, S.J.; Schwab, J.H.; Torriani, M.; Bredella, M.A. Body Composition Predictors of Adverse Postoperative Events in Patients Undergoing Surgery for Long Bone Metastases. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2022, 6, e22.00001. [Google Scholar] [CrossRef] [PubMed]
- Janssen, S.J.; Teunis, T.; Hornicek, F.J.; van Dijk, C.N.; Bramer, J.A.M.; Schwab, J.H. Outcome after fixation of metastatic proximal femoral fractures: A systematic review of 40 studies. J. Surg. Oncol. 2016, 114, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Pereira, N.R.P.; Ogink, P.T.; Groot, O.Q.; Ferrone, M.L.; Hornicek, F.J.; van Dijk, C.; Bramer, J.; Schwab, J.H. Complications and reoperations after surgery for 647 patients with spine metastatic disease. Spine J. 2019, 19, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Bollen, L.; van der Linden, Y.M.; Pondaag, W.; Fiocco, M.; Pattynama, B.P.M.; Marijnen, C.A.; Nelissen, R.G.H.H.; Peul, W.C.; Dijkstra, P.S. Prognostic factors associated with survival in patients with symptomatic spinal bone metastases: A retrospective cohort study of 1 043 patients. Neuro-Oncology 2014, 16, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Bongers, M.E.; Karhade, A.V.; Villavieja, J.; Groot, O.Q.; Bilsky, M.H.; Laufer, I.; Schwab, J.H. Does the SORG algorithm generalize to a contemporary cohort of patients with spinal metastases on external validation? Spine J. 2020, 20, 1646–1652. [Google Scholar] [CrossRef] [PubMed]
- Ghori, A.K.; Leonard, D.A.; Schoenfeld, A.J.; Saadat, E.; Scott, N.; Ferrone, M.L.; Pearson, A.M.; Harris, M.B. Modeling 1-year survival after surgery on the metastatic spine. Spine J. 2015, 15, 2345–2350. [Google Scholar] [CrossRef]
- Tokuhashi, Y.; Matsuzaki, H.; Oda, H.; Oshima, M.; Ryu, J. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine 2005, 30, 2186–2191. [Google Scholar] [CrossRef]
- Pereira, N.R.P.; Janssen, S.J.; van Dijk, E.; Harris, M.B.; Hornicek, F.J.; Ferrone, M.L.; Schwab, J.H. Development of a prognostic survival algorithm for patients with metastatic spine disease. J. Bone Jt. Surg. 2016, 98, 1767–1776. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, N.D.; Twining, P.K.; Groot, O.Q.; Pielkenrood, B.J.; Bongers, M.E.R.; Newman, E.T.; Verlaan, J.J.; Schwab, J.H. Adipose tissue density on CT as a prognostic factor in patients with cancer: A systematic review. Acta Oncol. 2020, 59, 1488–1495. [Google Scholar] [CrossRef] [PubMed]
- Thio, Q.C.B.S.; Karhade, A.V.; Ogink, P.T.; Bramer, J.A.M.; Ferrone, M.L.; Calderón, S.L.; Raskin, K.A.; Schwab, J.H. Development and Internal Validation of Machine Learning Algorithms for Preoperative Survival Prediction of Extremity Metastatic Disease. Clin. Orthop. Relat. Res. 2020, 478, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Groot, O.Q.; Bongers, M.E.; Buckless, C.G.; Twining, P.K.; Kapoor, N.D.; Janssen, S.J.; Schwab, J.H.; Torriani, M.; Bredella, M.A. Body composition predictors of mortality in patients undergoing surgery for long bone metastases. J. Surg. Oncol. 2022, 125, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Tsukada, K.; Miyazaki, T.; Kato, H.; Masuda, N.; Fukuchi, M.; Fukai, Y.; Nakajima, M.; Ishizaki, M.; Motegi, M.; Mogi, A.; et al. Body fat accumulation and postoperative complications after abdominal surgery. Am. Surg. 2004, 70, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Hopkins, J.; Malietzis, G.; Jenkins, J.T.; Sawyer, M.B.; Brisebois, R.; MacLean, A.; Nelson, G.; Gramlich, L.; Baracos, V.E. Assessment of Computed Tomography (CT)-Defined Muscle and Adipose Tissue Features in Relation to Short-Term Outcomes After Elective Surgery for Colorectal Cancer: A Multicenter Approach. Ann. Surg. Oncol. 2018, 25, 2669–2680. [Google Scholar] [CrossRef] [PubMed]
- Tappouni, R.; Mathew, P.; Connelly, T.M.; Luke, F.; Messaris, E. Measurement of visceral fat on preoperative computed tomography predicts complications after sigmoid colectomy for diverticular disease. Am. J. Surg. 2015, 210, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, Y.; Kaido, T.; Okumura, S.; Kobayashi, A.; Fujimoto, Y.; Ogawa, K.; Mori, A.; Hammad, A.; Hatano, E.; Uemoto, S. Muscle Steatosis is an Independent Predictor of Postoperative Complications in Patients with Hepatocellular Carcinoma. World J. Surg. 2016, 40, 1959–1968. [Google Scholar] [CrossRef]
- Veld, J.; Vossen, J.A.; De Amorim Bernstein, K.; Halpern, E.F.; Torriani, M.; Bredella, M.A. Adipose tissue and muscle attenuation as novel biomarkers predicting mortality in patients with extremity sarcomas. Eur. Radiol. 2016, 26, 4649–4655. [Google Scholar] [CrossRef]
- De Amorim Bernstein, K.; Bos, S.A.; Veld, J.; Lozano-Calderon, S.A.; Torriani, M.; Bredella, M.A. Body composition predictors of therapy response in patients with primary extremity soft tissue sarcomas. Acta Radiol. 2018, 59, 478–484. [Google Scholar] [CrossRef]
- Bongers, M.E.; Groot, O.Q.; Buckless, C.G.; Kapoor, N.D.; Twining, P.K.; Schwab, J.H.; Torriani, M.; Bredella, M.A. Body composition predictors of mortality on CT in patients with spinal metastases undergoing surgical treatment. Spine J. 2021, 22, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Nematollahi, M.A.; Jahangiri, S.; Asadollahi, A.; Salimi, M.; Dehghan, A.; Mashayekh, M.; Roshanzamir, M.; Gholamabbas, G.; Alizadehsani, R.; Bazrafshan, M.; et al. Body composition predicts hypertension using machine learning methods: A cohort study. Published online 123AD. Sci. Rep. 2023, 13, 6885. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, 1623–1627. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and validating the charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, H.; Okada, R.; Takagi, T.; Takahashi, M.; Murata, H.; Harada, H.; Nishimura, T.; Asakura, H.; Ogawa, H. New prognostic factors and scoring system for patients with skeletal metastasis. Cancer Med. 2014, 3, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Groot, O.Q.; Ogink, P.T.; Pereira, N.R.P.; Ferrone, M.L.; Harris, M.B.; Lozano-Calderon, S.A.; Schoenfeld, A.J.; Schwab, J.H. High Risk of Symptomatic Venous Thromboembolism after Surgery for Spine Metastatic Bone Lesions: A Retrospective Study. Clin. Orthop. Relat. Res. 2019, 477, 1674–1686. [Google Scholar] [CrossRef] [PubMed]
- Maynard, F.M., Jr.; Bracken, M.B.; Creasey, G.; Ditunno, J.F., Jr.; Donovan, W.H.; Ducker, T.B.; Garber, S.L.; Marino, R.J.; Stover, S.L.; Tator, C.H.; et al. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association. Spinal Cord. 1997, 35, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Bongers, M.E.; Groot, O.Q.; Buckless, C.G.; Kapoor, N.D.; Twining, P.K.; Schwab, J.H.; Torriani, M.; Bredella, M.A. Reply to the letter to editor regarding, “Body composition predictors of mortality on computed tomography in patients with spinal metastases undergoing surgical treatment”. Spine J. 2022, 22, 1583–1584. [Google Scholar] [CrossRef] [PubMed]
- Janssen, S.J. Surgical decision-making for long bone metastases. J. Orthop. Sci. 2018, 23, 394–402. [Google Scholar] [CrossRef]
- Janssen, S.J.; Kortlever, J.T.P.; Ready, J.E.; Raskin, K.A.; Ferrone, M.L.; Hornicek, F.J.; Lozano-Calderon, S.A.; Schwab, J.H. Complications after surgical management of proximal femoral metastasis: A retrospective study of 417 patients. J. Am. Acad. Orthop. Surg. 2016, 24, 483–494. [Google Scholar] [CrossRef]
- Joglekar, S.; Nau, P.N.; Mezhir, J.J. The impact of sarcopenia on survival and complications in surgical oncology: A review of the current literature. J. Surg. Oncol. 2015, 112, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Freire, P.P.; Fernandez, G.J.; Cury, S.S.; de Moraes, D.; Oliveira, J.S.; de Oliveira, G.; Dal-Pai-Silva, M.; dos Reis, P.P.; Carvalho, R.F. The pathway to cancer Cachexia: Microrna-regulated networks in muscle wasting based on integrative meta-analysis. Int. J. Mol. Sci. 2019, 20, 1962. [Google Scholar] [CrossRef] [PubMed]
- Cole, C.L.; Kleckner, I.R.; Jatoi, A.; Schwarz, E.; Dunne, R.F. The Role of Systemic Inflammation in Cancer-Associated Muscle Wasting and Rationale for Exercise as a Therapeutic Intervention. JCSM Clin. Rep. 2018, 3, 1–19. [Google Scholar] [CrossRef]
- Roubenoff, R.; Hughes, V.A. Sarcopenia: Current concepts. J. Gerontol. Ser. A 2000, 55, M716–M724. [Google Scholar] [CrossRef] [PubMed]
- Tisdale, M.J. Wasting in cancer. J. Nutr. 1999, 129, 243S–246S. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; Pluijm, S.M.F.; Deeg, D.J.H.; Harris, T.B.; Kritchevsky, S.B.; Newman, A.B.; Colbert, L.H.; Pahor, M.; Rubin, S.M.; Tylavsky, F.A.; et al. Higher inflammatory marker levels in older persons: Associations with 5-year change in muscle mass and muscle strength. J. Gerontol. Ser. A 2009, 64, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Deodato, M.; Saponaro, S.; Šimunič, B.; Martini, M.; Galmonte, A.; Murena, L.; Stella, A.B. Sex-based comparison of trunk flexors and extensors functional and contractile characteristics in young gymnasts. Sport Sci. Health 2024, 20, 147–155. [Google Scholar] [CrossRef]
- Lohr, C.; Schmidt, T.; Braumann, K.M.; Reer, R.; Medina-Porqueres, I. Sex-Based Differences in Tensiomyography as Assessed in the Lower Erector Spinae of Healthy Participants: An Observational Study. Sports Health 2020, 12, 341. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Spine (n = 196) |
|---|---|
| Median (IQR) | |
| Age (years) | 62 (53–70) |
| Body mass index (in kg/m2) a | 26 (23–30) |
| Duration primary diagnosis untill metastatic operation (days) | 397 (26–1464) |
| Albumin (g/dL) | 3.8 (3.4–4.2) |
| % (n) | |
| Male | 63 (123) |
| Additional Modified Charlson comorbidity b | 65 (127) |
| Primary tumor growth c | |
| Slow | 25 (48) |
| Moderate | 34 (67) |
| Rapid | 41 (81) |
| Additional metastases d | 70 (138) |
| Spinal pain | 88 (172) |
| ASIA impairment scale (preoperative) a | |
| Neurological deficit (A, B, C, or D) | 45 (88) |
| No neurological deficit (E) | 55 (108) |
| Metastases region | |
| Thoracic | 54 (105) |
| Lumbar | 28 (54) |
| Cervical | 14 (28) |
| Combined | 4.6 (9) |
| Previous local radiotherapy | 33 (64) |
| Previous systemic therapy | 55 (107) |
| Pathological fracture | 54 (106) |
| Number of spine levels undergoing operation | |
| 1 | 47 (93) |
| 2 | 16 (32) |
| 3 or more | 36 (71) |
| Type of surgery | |
| Vertebrectomy or corpectomy with stabilization | 40 (78) |
| Decompression and stabilization | 39 (76) |
| Decompression | 14 (28) |
| Stabilization | 7.1 (14) |
| Surgical approach | |
| Posterior | 86 (169) |
| Anterior | 11 (22) |
| Combined | 2.6 (5) |
| Two-staged procedure | 1.0 (2) |
| Body composition measures a | Median (IQR) or % (n) |
| Subcutanous adipose tissue | |
| Area (cm2) | 249 (180–320) |
| Visceral adipose tissue | |
| Area (cm2) | 124 (75–211) |
| Muscle | |
| Area (cm2) | 140 (116–165) |
| Outcomes | |
| Length of stay in days | 9 (6–13) |
| Postoperative complications within 30 days | 31% (61) |
| Reoperations | 16% (31) |
| Variables | Odds Ratio (95% CI) | Standard-Error | p-Value |
|---|---|---|---|
| Albumin | 0.42 (0.21; 0.82) | 0.143 | 0.01 |
| ASIA impairment scale (preoperative) | |||
| Neurological deficit (A, B, C, or D) | Reference value | ||
| No neurological deficit (E) | 0.65 (0.30; 1.41) | 0.258 | 0.28 |
| Metastases region | |||
| Thoracic | Reference value | ||
| Lumbar | 0.88 (0.39; 1.98) | 0.363 | 0.76 |
| Cervical | 0.12 (0.02; 0.55) | 0.093 | 0.01 |
| Combined | 0.11 (0.01; 1.17) | 0.133 | 0.07 |
| Previous systemic therapy | 1.27 (0.58; 2.78) | 0.508 | 0.55 |
| Muscle area (cm2) | 0.99 (0.98; 0.99) | 0.006 | 0.047 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapoor, N.D.; Groot, O.Q.; Buckless, C.G.; Twining, P.K.; Bongers, M.E.R.; Janssen, S.J.; Schwab, J.H.; Torriani, M.; Bredella, M.A. Opportunistic CT for Prediction of Adverse Postoperative Events in Patients with Spinal Metastases. Diagnostics 2024, 14, 844. https://doi.org/10.3390/diagnostics14080844
Kapoor ND, Groot OQ, Buckless CG, Twining PK, Bongers MER, Janssen SJ, Schwab JH, Torriani M, Bredella MA. Opportunistic CT for Prediction of Adverse Postoperative Events in Patients with Spinal Metastases. Diagnostics. 2024; 14(8):844. https://doi.org/10.3390/diagnostics14080844
Chicago/Turabian StyleKapoor, Neal D., Olivier Q. Groot, Colleen G. Buckless, Peter K. Twining, Michiel E. R. Bongers, Stein J. Janssen, Joseph H. Schwab, Martin Torriani, and Miriam A. Bredella. 2024. "Opportunistic CT for Prediction of Adverse Postoperative Events in Patients with Spinal Metastases" Diagnostics 14, no. 8: 844. https://doi.org/10.3390/diagnostics14080844