
Hyperacute Radiation Pneumonitis after Severe irAE

1
Department of Otolaryngology-Head and Neck Surgery, Shuang Ho Hospital, Taipei Medical University, New Taipei 23561, Taiwan
2
Department of Otolaryngology-Head and Neck Surgery, Taipei Medical University Hospital, Taipei 11031, Taiwan
3
Department of Radiation Oncology, Shuang Ho Hospital, Taipei Medical University, New Taipei 23561, Taiwan
4
Department of Biomedical Imaging and Radiological Sciences, National Yang Ming Chiao Tung University, Taipei 11221, Taiwan
*
Author to whom correspondence should be addressed.
Diagnostics 2024, 14(8), 850; https://doi.org/10.3390/diagnostics14080850
Submission received: 22 March 2024
/
Revised: 11 April 2024
/
Accepted: 15 April 2024
/
Published: 19 April 2024
(This article belongs to the Section Medical Imaging and Theranostics)
{kind=link}
{kind=link}
{kind=link}
Abstract
:A 54-year-old woman presented to an outpatient clinic with a recurrence of triple-negative breast cancer and multiple bone metastases. The patient had a large mass lesion of 10 cm on the sternum. She received the immune checkpoint inhibitors pembrolizumab and taxane. Initially, the patient responded excellently to treatment, but stopped pembrolizumab for grade IV skin toxicity with multiple ulcerative wounds over the bilateral leg and trunk. The lesions abated following administration of antibiotics and oral prednisolone for two months. After that, she was referred to the radiation oncology department for further treatment. She received radiotherapy for the sternum mass but stopped radiation at 42Gy/21 fractions for severe dyspnea and fever. Blood sampling found leukocytosis with neutrophil predominance. Chest radiography showed bilateral lung infiltration. Pulmonary CT scan yielded bilateral lung patchy consolidation compatible with radiation isodose-line. Bronchial lavage showed positive Pneumocystis jiroveci PCR. Dyspnea improved after titrating methylprednisolone within two days. The patient recovered well with TMP-SMX and glucocorticoids after the initiation of therapy.
The rapid development of pneumonitis following radiation therapy in this case, especially after the use of immunotherapy, is notably significant (Figure 1 and Figure 2). Typically, radiation pneumonitis occurs within a timeframe of 6 weeks to 6 months post-treatment, aligning with our reference [1,2]. However, in this case, following a Grade 3 immune-related adverse event from immunotherapy, the patient developed radiation pneumonitis at an unusually rapid pace after receiving radiation therapy, a clinical occurrence that is quite rare.
Immunotherapy, particularly the use of immune checkpoint inhibitors, has shown revolutionary effects in the treatment of various cancers. These drugs work by activating the patient’s immune system to attack cancer cells but can also lead to the immune system attacking normal tissues of the body, causing a range of immune-related side effects, including pneumonitis [3]. Recent retrospective studies have indicated that the combined use of ICIs and radiation therapy does indeed increase the incidence of related side effects [4,5,6]. In a pooled analysis examining the association of radiation therapy (RT) with the risk of adverse events in patients receiving immune checkpoint inhibitors (ICIs), Mitchell S. Anscher et al. found that administering an ICI within 90 days following RT did not significantly increase the risk of serious adverse events, suggesting the safety of this treatment sequence [6]. However, for patients who have experienced severe immune-related adverse events (irAEs), the risk of developing severe radiation pneumonitis remains unclear.
The rapid progression of pneumonitis in this case could be attributed to the combined stimulation of the immune system by both the immune checkpoint inhibitor and radiation therapy. The serious consequences of potential opportunistic infections such as Pneumocystis jirovecii pneumonia resulting from the use of steroids should also be considered.
This occurrence also underscores the importance of close monitoring and evaluation of cancer patients undergoing immunotherapy to promptly identify and manage any potential pulmonary side effects. Furthermore, it highlights the need for personalized treatment plans for patients in cancer treatment, taking into consideration the balance between therapeutic benefits and potential side effects in treatment decisions.
Author Contributions
Conceptualization, Supervision, Review & Editing: W.-K.C.; Methodology, Software, Resources, Data Curation, Writing—Original Draft Preparation, Visualization, Project Administration: Y.C. and W.-K.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The publication of case reports that do not contain personally identifiable information does not require the approval of our Institutional Review Board.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The original data presented in the study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen, F.; Niu, J.; Wang, M.; Zhu, H.; Guo, Z. Re-evaluating the risk factors for radiation pneumonitis in the era of immunotherapy. J. Transl. Med. 2023, 21, 368. [Google Scholar] [CrossRef] [PubMed]
- Uchida, Y.; Tsugawa, T.; Tanaka-Mizuno, S.; Noma, K.; Aoki, K.; Shigemori, W.; Nakagawa, H.; Kinose, D.; Yamaguchi, M.; Osawa, M.; et al. Exclusion of emphysematous lung from dose-volume estimates of risk improves prediction of radiation pneumonitis. Radiat. Oncol. 2017, 12, 160. [Google Scholar] [CrossRef] [PubMed]
- Verma, V.; Cushman, T.R.; Selek, U.; Tang, C.; Welsh, J.W. Safety of Combined Immunotherapy and Thoracic Radiation Therapy: Analysis of 3 Single-Institutional Phase I/II Trials. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Aiad, M.; Fresco, K.; Prenatt, Z.; Tahir, A.; Ramos-Feliciano, K.; Stoltzfus, J.; Harmouch, F.; Wilson, M.; Ramos-Feliciano, K.M. Comparison of Pneumonitis Rates and Severity in Patients with Lung Cancer Treated by Immunotherapy, Radiotherapy, and Immunoradiotherapy. Cureus 2022, 14, e25665. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Switchenko, J.M.; Buchwald, Z.S.; Patel, P.R.; Shelton, J.W.; Kahn, S.E.; Pillai, R.N.; Steuer, C.E.; Owonikoko, T.K.; Behera, M.; et al. Lung Stereotactic Body Radiation Therapy and Concurrent Immunotherapy: A Multicenter Safety and Toxicity Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 304–313. [Google Scholar] [CrossRef]
- Anscher, M.S.; Arora, S.; Weinstock, C.; Amatya, A.; Bandaru, P.; Tang, C.; Girvin, A.T.; Fiero, M.H.; Tang, S.; Lubitz, R.; et al. Association of Radiation Therapy with Risk of Adverse Events in Patients Receiving Immunotherapy: A Pooled Analysis of Trials in the US Food and Drug Administration Database. JAMA Oncol. 2022, 8, 232–240. [Google Scholar] [CrossRef]
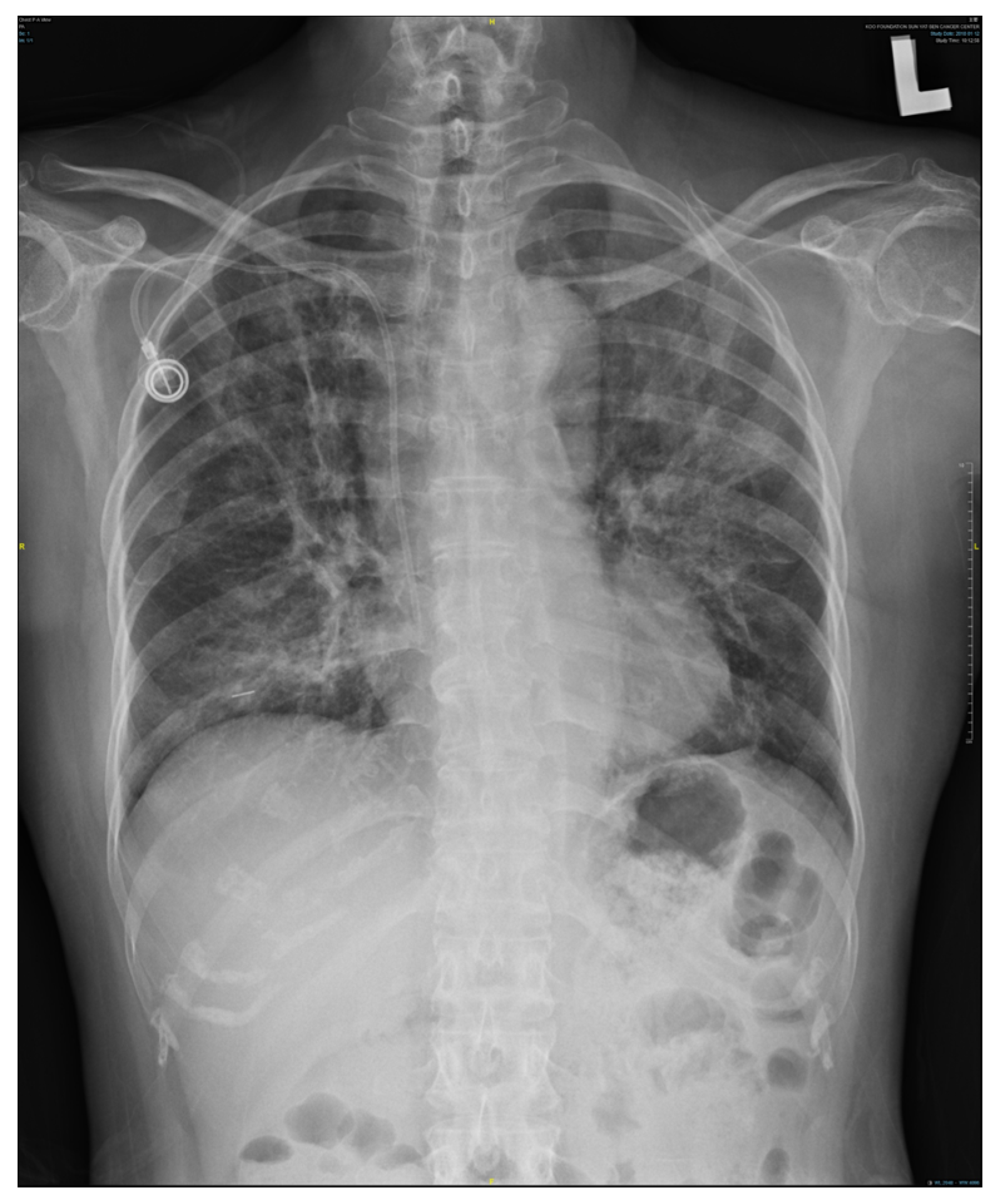
Figure 1.
Chest X-ray showing marked pneumonitis patches, demonstrating increasing bilateral lung infiltration.
Figure 1.
Chest X-ray showing marked pneumonitis patches, demonstrating increasing bilateral lung infiltration.

Figure 2.
(a,b) Axial and sagittal views of a chest CT scan illustrating severe radiation pneumonitis. The images feature a fusion of radiotherapy isodose lines with the CT scan, highlighting areas where pneumonitis patches coincide with the isodose lines. The purple line represents the 20 Gy isodose line, and the sky-blue line represents the 42 Gy isodose line, indicating the direct impact of radiation dose distribution on lung tissue.
Figure 2.
(a,b) Axial and sagittal views of a chest CT scan illustrating severe radiation pneumonitis. The images feature a fusion of radiotherapy isodose lines with the CT scan, highlighting areas where pneumonitis patches coincide with the isodose lines. The purple line represents the 20 Gy isodose line, and the sky-blue line represents the 42 Gy isodose line, indicating the direct impact of radiation dose distribution on lung tissue.


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chou, Y.; Chuang, W.-K. Hyperacute Radiation Pneumonitis after Severe irAE. Diagnostics 2024, 14, 850. https://doi.org/10.3390/diagnostics14080850
AMA Style
Chou Y, Chuang W-K. Hyperacute Radiation Pneumonitis after Severe irAE. Diagnostics. 2024; 14(8):850. https://doi.org/10.3390/diagnostics14080850
Chicago/Turabian StyleChou, Yang, and Wei-Kai Chuang. 2024. "Hyperacute Radiation Pneumonitis after Severe irAE" Diagnostics 14, no. 8: 850. https://doi.org/10.3390/diagnostics14080850
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.