
Does the Use of Intraoperative Neuromonitoring during Thyroid and Parathyroid Surgery Reduce the Incidence of Recurrent Laryngeal Nerve Injuries? A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
Inclusion/Exclusion Criteria
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author [Citation] | Year | Country | Dates of Study | Type of Study | Type of Control | NAR (Patients) | Postop Laryngoscopy | Definition of Permanent Injury | Number of Surgeons | % Female Patients | % Cancer Operations | % Total Thyroidectomy |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adamczyk [19] | 2015 | Poland | 1992–2005 | R | C | 120 (80) | Yes | 6 months | M | 100 | NS | 100 |
| Agha [49] | 2008 | Germany | 2012–2017 | R | C | (59) | Yes | NS | M | 61 | NS | 100 |
| Akici [50] | 2020 | Turkey | 2004–2012 | R | H | (273) | Yes | 6 months | S | 86 | 0 | 100 |
| Akkari [51] | 2014 | France | 2005–2012 | R | C | (90) | NS | NS | NS | 75 | NS | 44.6 |
| Alesina [52] | 2014 | Germany | 2002–2014 | PNR | C | 1708 (1114) | Yes | 6 months | M | 75 | 9 | 47 |
| Anuwong [48] | 2016 | Italy | 2003–2007 | R | H | NS | Yes | NS | S | 79 | 19 | NS |
| Atallah [53] | 2009 | France | 2006–2007 | R | C | 421 (261) | Yes | 12 months | M | 77 | 7 | 60 |
| Barczyński [54] | 2009 | Poland | 1993–2012 | PR | C | 2000 (1000) | Yes | 12 months | M | 91 | 12 | 75 |
| Barczyński [55] | 2014 | Poland | 1993–2012 | R | C | 1326 (854) | Yes | 12 months | M | 81 | 28 | 39 |
| Bonati [56] | 2022 | Italy | 2009–2015 | R | H | 1212 (638) | No | NS | M | 76 | 95 | 90 |
| Brajcich [57] | 2016 | USA | 1995–2002 | R | H | 1048 (627) | Yes | 12 months | S | 83 | 20 | 67 |
| Brauckhoff [23] | 2002 | Germany | 2007–2014 | R | H | 169 (97) | Yes | NS | M | 58 | 77 | NS |
| Calò [5] | 2017 | Italy | 2002–2005 | R | H | 4730 (2365) | Selective | 12 months | M | 80 | 31 | 100 |
| Chan [58] | 2006 | Hong Kong | 2001–2010 | R | C | 1000 (639) | Yes | 12 months | M | 79 | 22 | 61 |
| Chuang [59] | 2013 | Taiwan | 2009–2012 | R | H | 83 (71) | No | NS | S | 83 | 24 | 57 |
| DeDanschutter [24] | 2015 | Netherlands | 2014–2016 | R | H | 170 (147) | Yes | 12 months | M | 86 | 14 | 16 |
| Demiryas [60] | 2018 | Turkey | 1998–2001 | R | C | 370 (191) | Yes | 12 months | S | 9 | NS | 46 |
| Dralle [16] | 2004 | Germany | 2008–2009 | PNR | C | 23,349 | Yes | 6 months | M | 78 | 7 | 69 |
| Duclos [61] | 2011 | France | 2013–2018 | PNR | C | (686) | Yes | NS | M | 78 | 21 | 76 |
| Dudley [62] | 2021 | USA | 2008–2016 | R | C | (107) | No | 3 weeks | M | 58 | NS | NS |
| Ercetin [25] | 2019 | Turkey | NS | PR | C | 1496 (748) | Yes | 12 months | M | 89 | NS | NS |
| Frattini [63] | 2010 | Italy | 2007–2010 | R | NS | 304 (152) | Yes | NS | NS | 56 | 100 | 100 |
| Gremillion [64] | 2012 | USA | 2007–2010 | R | C | 162 (119) | NS | NS | S | NS | NS | 36 |
| Grishaeva [65] | 2022 | Germany | 2007–2011 | R | H | 2720 (1963) | Yes | 6 months | M | 77 | 0 | 38 |
| Hayward [9] | 2013 | Australia | 2012–2014 | R | C | 3736 | NS | NS | NS | NS | 18 | 53 |
| Hei [66] | 2016 | China | 1997–2016 | PR | C | 84 (70) | Yes | 6 months | S | 77 | 77 | 26 |
| Kadakia [18] | 2017 | USA | 2013–2016 | R | H | (1418) | Yes | 8 months | S | 68 | 57 | NS |
| Kai [67] | 2017 | China | 1987–2008 | R | C | 836 (552) | Yes | 6 months | M | 22 | 25 | 89 |
| Karakas [68] | 2013 | Germany | 2014–2016 | R | H | (111) | NS | NS | M | 65 | NS | NS |
| Kartal [20] | 2021 | Turkey | 2009–2019 | R | C | 839 (493) | Yes | 6 months | M | 79 | 19 | 70 |
| Kim [6] | 2020 | Korea | 2011–2014 | PNR | C | 133 (121) | Yes | 12 months | M | 72 | 100 | 100 |
| Lee [69] | 2017 | Australia | 2008–2018 | PNR | H | 1583 (990) | Yes | NS | S | 80 | 18 | 60 |
| Legre [17] | 2020 | France | 2014–2018 | R | C | 77 (47) | Selective | 6 months | M | 62 | 13 | 38 |
| Leow [70] | 2020 | Singapore | 2012–2017 | R | C | 301 (193) | Yes | 6 months | M | 74 | 25 | 15 |
| Ling [71] | 2020 | China | 2010–2016 | R | C | 1696 (1033) | Yes | 6 months | M | 73 | 46 | 76 |
| Long [72] | 2018 | China | 2012–2014 | R | C | (435) | Yes | 6 months | M | 32 | 100 | 100 |
| Mirallie [73] | 2018 | France | 1997–2016 | PNR | C | 2633 (1328) | Yes | 6 months | M | 80 | 22 | 100 |
| Mourad [74] | 2017 | USA | 1997–2016 | R | H | (213) | Yes | 7 months | S | 72 | 0 | 0 |
| Netto [75] | 2007 | Brazil | 2003–2006 | R | H | 327 (204) | Yes | 3 months | M | 93 | 58 | 63 |
| Page [76] | 2015 | France | 2001–2010 | R | H | 1534 (767) | Yes | 12 months | M | 82 | NS | 100 |
| Pei [77] | 2021 | China | 2010–2020 | R | H | 159 (109) | Yes | NS | M | 56 | 47 | NS |
| Polat [78] | 2015 | Turkey | 2010–2012 | PNR | C | 178 (94) | Yes | NS | M | 79 | 27 | 76 |
| Prokopakis [30] | 2013 | Greece | 2004–2011 | R | C | 121 (97) | No | 4 months | M | 79 | 87 | 25 |
| Ritter [26] | 2021 | Israel | 2001–2019 | R | C | 183 (113) | Yes | 12 months | M | 75 | 57 | 43 |
| Robertson [79] | 2004 | USA | 1999–2002 | R | C | 236 (165) | Yes | NS | M | 77 | 33 | NS |
| Sanguinetti [28] | 2014 | Italy | 2012 | R | C | 700 (350) | Yes | NS | M | NS | NS | 100 |
| Sari [29] | 2010 | Turkey | 2007–2009 | PR | C | 409 (237) | Yes | 12 months | M | 82 | 17 | 79 |
| Sharif [80] | 2017 | Pakistan | 2014–2017 | R | C | 400 (200) | Yes | 6 months | M | NS | NS | 100 |
| Shindo [81] | 2007 | USA | 1998–2005 | R | C | 1043 (684) | Yes | NS | S | NS | 55 | 52 |
| Sopinski [82] | 2017 | Poland | 2014–2016 | R | C | 133 (80) | NS | NS | M | 95 | 0 | 66 |
| Stevens [83] | 2012 | USA | 2004–2008 | PNR | C | 143 (91) | No | 6 months | M | 59 | 41 | 57 |
| Teksoz [27] | 2015 | Turkey | 2011–2012 | PR | C | 322 (161) | Yes | 6 months | M | 76 | 34 | 100 |
| Terris [31] | 2007 | USA | 2004–2006 | R | C | 176 (137) | Yes | 6 months | S | NS | 18 | 28 |
| Thong [84] | 2021 | Ireland | 2009–2019 | PNR | H | 1539 (1001) | Yes | 6 months | S | 81 | 23 | 55 |
| Vasileiadis [10] | 2016 | Greece | 2002–2012 | R | C | 5112 (2556) | Yes | 12 months | M | 79 | NS | 100 |
| Witt [85] | 2005 | USA | 1998–2003 | R | C | 190 | NS | 12 months | S | NS | NS | 44 |
| Wojtczak [8] | 2017 | Poland | 2011–2014 | R | C | 105 (61) | Yes | 12 months | M | 87 | 20 | 85 |
| Yarbrough [22] | 2004 | USA | 1998–2003 | R | H | 151 (111) | Selective | NS | M | 63 | 66 | 4.5 |
| Zhang [7] | 2020 | China | 2018 | R | C | 280 (200) | Yes | 6 months | M | 83 | 100 | 78 |
| Zhou [47] | 2019 | China | 2009–2014 | R | C | 418 (209) | Yes | 12 months | M | 62 | 2 | 91 |
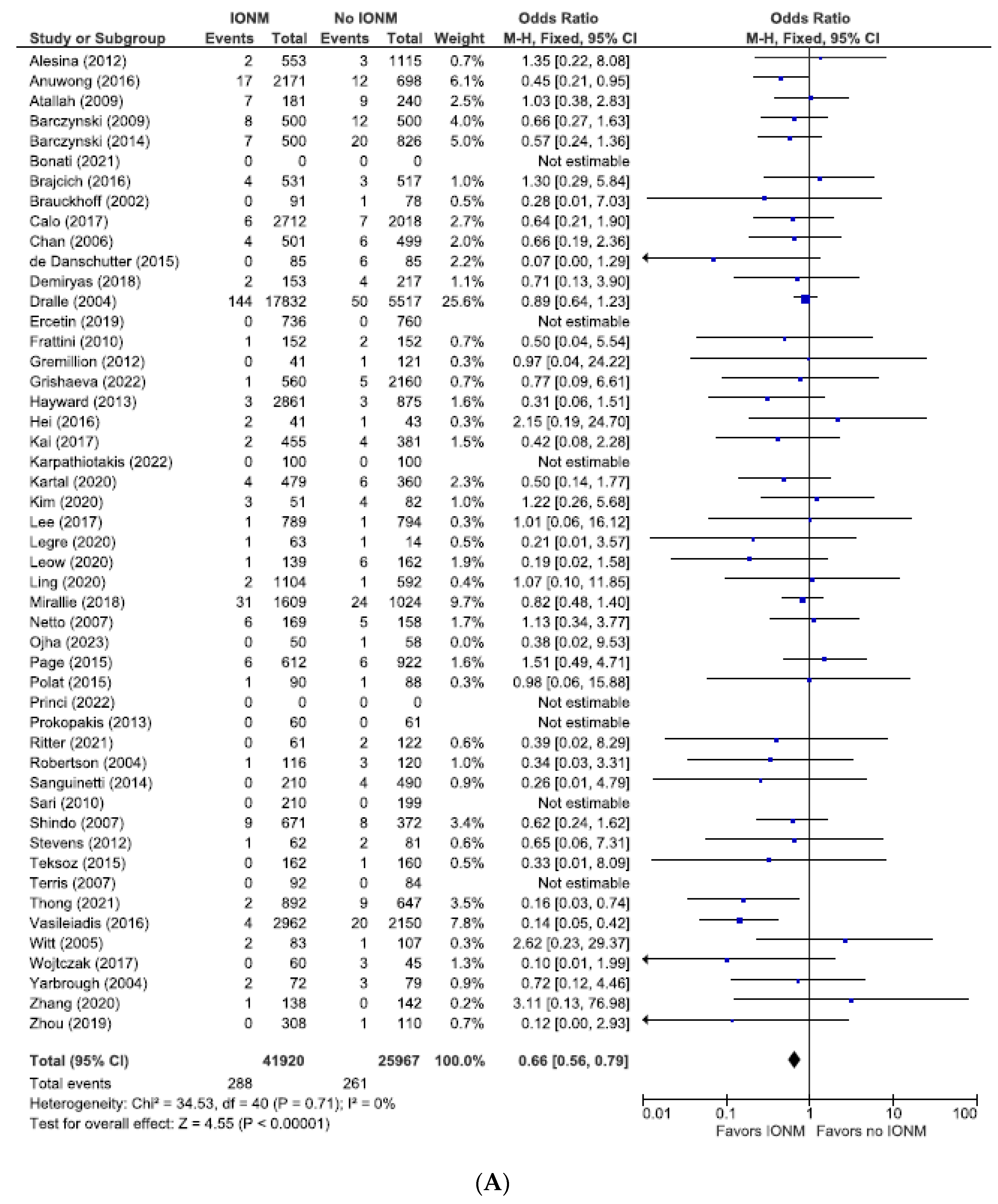
3.1. Meta-Analysis of All Studies Assessing Permanent Nerve Injury Categorized by NAR and per Patient
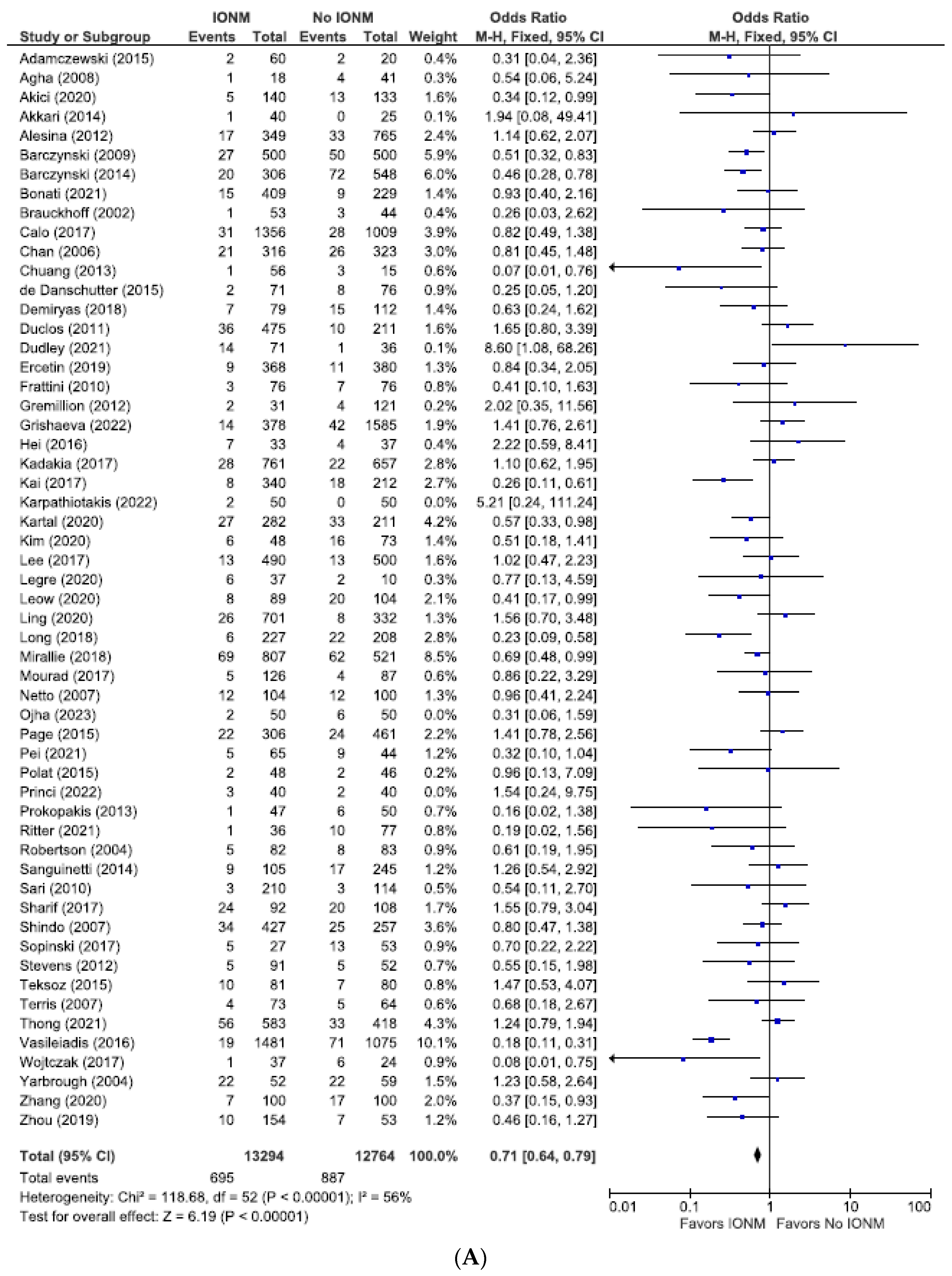
3.2. Meta-Analysis of All Studies Assessing Total Nerve Injuries Categorized by NAR and per Patient
3.3. Meta-Analysis of Randomized Controlled Trials Assessing Permanent and Total Number of Nerve Injuries Categorized by NAR
3.4. Meta-Analysis of Studies with Documented Post-Operative Laryngoscopy Assessing Permanent and Total RLN Injuries Categorized by Nerves at Risk
3.5. Meta-Analysis of All Studies with Contemporaneous Controls Assessing Permanent and Total RLN Injuries Categorized by Nerves at Risk
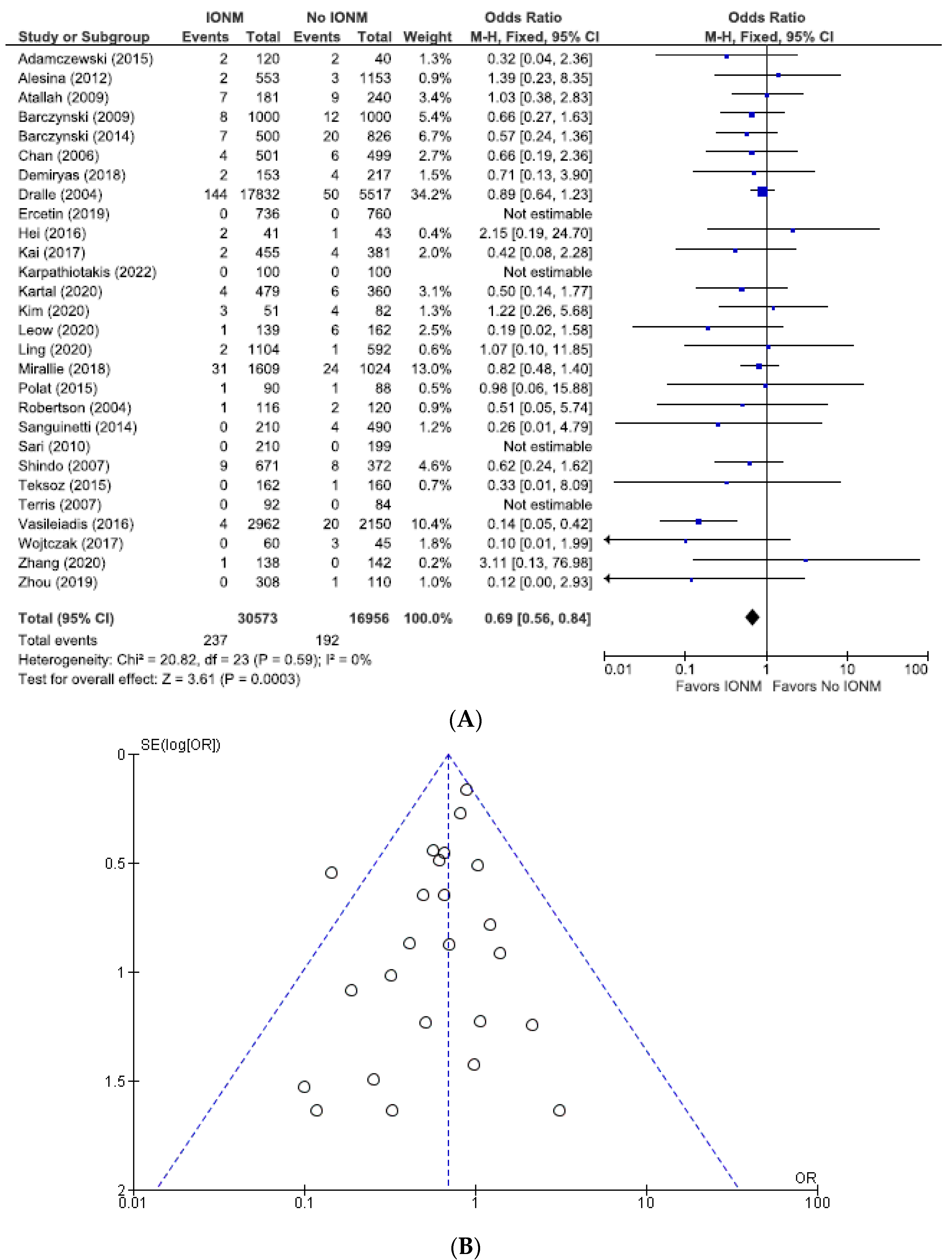
3.6. Meta-Analysis of All Studies with Contemporaneous Controls and Documented Postoperative Laryngoscopy Assessing Permanent and Total RLN Injuries Categorized by Nerves at Risk
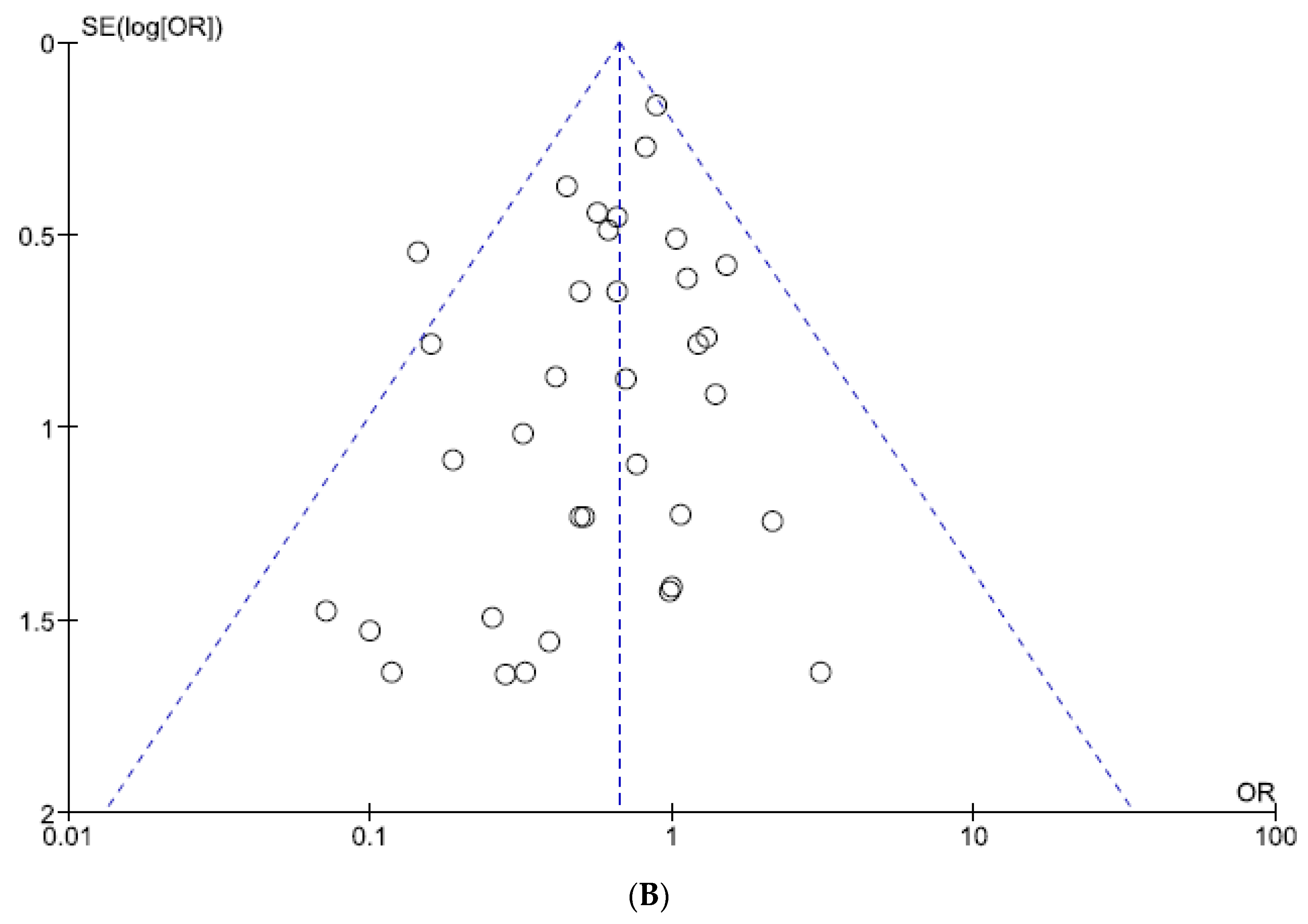
3.7. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spector, B.; Netterville, J.; Billante, C.; Clary, J.; Reinisch, L.; Smith, T. Quality-of-Life Assessment in Patients with Unilateral Vocal Cord Paralysis. Otolaryngol. Neck Surg. 2001, 125, 176–182. [Google Scholar] [CrossRef]
- Swonke, M.L.; Shakibai, N.; Chaaban, M.R. Medical Malpractice Trends in Thyroidectomies among General Surgeons and Otolaryngologists. OTO Open 2020, 4, 2473974X20921141. [Google Scholar] [CrossRef]
- Sasou, S.; Nakamura, S.-I.; Kurihara, H. Suspensory ligament of Berry: Its relationship to recurrent laryngeal nerve and anatomic examination of 24 autopsies. Head Neck 1998, 20, 695–698. [Google Scholar] [CrossRef]
- Dionigi, G.; Boni, L.; Rovera, F.; Rausei, S.; Castelnuovo, P.; Dionigi, R. Postoperative laryngoscopy in thyroid surgery: Proper timing to detect recurrent laryngeal nerve injury. Langenbeck’s Arch. Surg. 2010, 395, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Calò, P.G.; Medas, F.; Conzo, G.; Podda, F.; Canu, G.L.; Gambardella, C.; Pisano, G.; Erdas, E.; Nicolosi, A. Intraoperative neuromonitoring in thyroid surgery: Is the two-staged thyroidectomy justified? Int. J. Surg. 2017, 41, S13–S20. [Google Scholar] [CrossRef]
- Kim, J.-I.; Kim, S.-J.; Xu, Z.; Kwak, J.; Ahn, J.-H.; Yu, H.W.; Chai, Y.J.; Choi, J.Y.; Lee, K.E. Efficacy of intraoperative neuromonitoring in reoperation for recurrent thyroid cancer patients. Endocrinol. Metab. 2020, 35, 918–924. [Google Scholar] [CrossRef]
- Zhang, G.-W.; Shi, M.-M.; Li, G.-L. Intraoperative Nerve Monitoring with a Thyroid Cartilage Recording Electrode: A Novel, Feasible Approach to Recurrent Laryngeal Nerve Preservation in Thyroid Carcinoma Surgery. Acta Medica Mediterr. 2020, 36, 1075. [Google Scholar] [CrossRef]
- Wojtczak, B.; Sutkowski, K.; Kaliszewski, K.; Barczyński, M.; Bolanowski, M. Thyroid reoperation using intraoperative neuromonitoring. Endocrine 2017, 58, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Hayward, N.J.; Grodski, S.; Yeung, M.; Johnson, W.R.; Serpell, J. Recurrent laryngeal nerve injury in thyroid surgery: A review. ANZ J. Surg. 2013, 83, 15–21. [Google Scholar] [CrossRef]
- Vasileiadis, I.; Karatzas, T.; Charitoudis, G.; Karakostas, E.; Tseleni-Balafouta, S.; Kouraklis, G. Association of intraoperative neuromonitoring with reduced recurrent laryngeal nerve injury in patients undergoing total thyroidectomy. JAMA Otolaryngol–Head Neck Surg. 2016, 142, 994–1001. [Google Scholar] [CrossRef]
- Lahey, F.; Hoover, W. Injuries to the Recurrent Laryngeal Nerve in Thyroid Operations: Their Management and Avoidance. Ann. Surg. 1938, 108, 545–54562. [Google Scholar]
- Edis, A.J. Prevention and management of complications associated with thyroid and parathyroid surgery. Surg. Clin. N. Am. 1979, 59, 83–92. [Google Scholar] [CrossRef]
- Karlan, M.S.; Catz, B.; Dunkelman, D.; Uyeda, R.Y.; Gleischman, S. A safe technique for thyroidectomy with complete nerve dissection and parathyroid preservation. Head Neck Surg. 1984, 6, 1014–1019. [Google Scholar] [CrossRef]
- Loré, J.M. Practical anatomical considerations in thyroid tumor surgery. Arch. Otolaryngol. Neck Surg. 1983, 109, 568–574. [Google Scholar] [CrossRef]
- Randolph, G.W.; Kobler, J.B.; Wilkins, J. Recurrent laryngeal nerve identification and assessment during thyroid surgery: Laryngeal palpation. World J. Surg. 2004, 28, 755–760. [Google Scholar] [CrossRef]
- Dralle, H.; Sekulla, C.; Haerting, J.; Timmermann, W.; Neumann, H.J.; Kruse, E.; Grond, S.; Mühlig, H.P.; Richter, C.; Voß, J.; et al. Risk factors of paralysis and functional outcome after recurrent laryngeal nerve monitoring in thyroid surgery. Surgery 2004, 136, 1310–1322. [Google Scholar] [CrossRef]
- Legré, M.; Bois, E.; Bernard, S.; Teissier, N.; Van Den Abbeele, T. Recurrent laryngeal nerve monitoring during thyroidectomy and parathyroidectomy in children. Int. J. Pediatr. Otorhinolaryngol. 2020, 131, 109846. [Google Scholar] [CrossRef] [PubMed]
- Kadakia, S.; Mourad, M.; Hu, S.; Brown, R.; Lee, T.; Ducic, Y. Utility of intraoperative nerve monitoring in thyroid surgery: 20-year experience with 1418 cases. Oral Maxillofac. Surg. 2017, 21, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Adamczewski, Z.; Chwałkiewicz, M.; Lewiński, A.; Brzeziński, J.; Dedecjus, M. Continuous intraoperative neuromonitoring (CIONM) of the recurrent laryngeal nerve is sufficient as the only neuromonitoring technique in thyroidectomy performed because of benign goitre. Ann. Agric. Environ. Med. 2015, 22, 495–498. [Google Scholar] [CrossRef]
- Kartal, K.; Aygun, N.; Celayir, M.F.; Besler, E.; Citgez, B.; Isgor, A.; Uludag, M. Intraoperative Neuromonitoring in Thyroid Surgery: An Efficient Tool to Avoid Bilateral Vocal Cord Palsy. Ear Nose Throat. J. 2021, 100 (Suppl. 5), 694S–699S. [Google Scholar] [CrossRef]
- Schneider, R.; Machens, A.; Lorenz, K.; Dralle, H. Intraoperative nerve monitoring in thyroid surgery—Shifting current paradigms. Gland. Surg. 2020, 9 (Suppl. 2), S120–S128. [Google Scholar] [CrossRef] [PubMed]
- Yarbrough, D.E.; Thompson, G.B.; Kasperbauer, J.L.; Harper, C.M.; Grant, C.S. Intraoperative electromyographic monitoring of the recurrent laryngeal nerve in reoperative thyroid and parathyroid surgery. Surgery 2004, 136, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Brauckhoff, M.; Gimm, O.; Thanh, P.N.; Brauckhoff, K.; Ukkat, J.; Thomusch, O.; Dralle, H. First experiences in intraoperative neurostimulation of the recurrent laryngeal nerve during thyroid surgery of children and adolescents. J. Pediatr. Surg. 2002, 37, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- De Danschutter, S.J.R.; Schreinemakers, J.M.J.; Smit, L.H.M.; van der Laan, L.; Nuytinck, H.K.S. Thyroid surgery and the usefulness of intraoperative neuromonitoring, a single center study. J. Investig. Surg. 2015, 28, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Erçetin, C.; Şahbaz, A.; Acar, S.; Tutal, F.; Aksakal, N.; Sarı, S.; Erbil, Y. Is intraoperative nerve monitoring useful for surgical training in thyroid surgery? Turk. J. Surg. 2019, 35, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Ritter, A.; Hod, R.; Reuven, Y.; Shpitzer, T.; Mizrachi, A.; Raveh, E.; Bachar, G. Role of intraoperative recurrent laryngeal nerve monitoring for pediatric thyroid surgery: Comparative analysis. Head Neck 2021, 43, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Teksoz, S.; Bukey, Y.; Ozcan, M.; Arikan, A.E.; Ozyegin, A. Is Nerve Monitoring Required in Total Thyroidectomy? Cerrahpasa Experience. Indian J. Surg. 2015, 77, 466–471. [Google Scholar] [CrossRef]
- Sanguinetti, A.; Parmeggiani, D.; Lucchini, R.; Monacelli, M.; Triola, R.; Avenia, S.; Conti, C.; Conzo, G.; Avenia, N. Intraoperative recurrent laryngeal nerve monitoring in thyroid surgery. Ann. Ital. Chir. 2014, 85, 418–421. [Google Scholar] [PubMed]
- Sarı, S.; Erbil, Y.; Sümer, A.; Agcaoglu, O.; Bayraktar, A.; Issever, H.; Ozarmagan, S. Evaluation of recurrent laryngeal nerve monitoring in thyroid surgery. Int. J. Surg. 2010, 8, 474–478. [Google Scholar] [CrossRef]
- Prokopakis, E.; Kaprana, A.; Velegrakis, S.; Panagiotaki, I.; Chatzakis, N.; Iro, H.; Velegrakis, G. Intraoperative recurrent laryngeal nerve monitoring in revision thyroidectomy. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 2521–2524. [Google Scholar] [CrossRef]
- Terris, D.J.; Anderson, S.K.; Watts, T.L.; Chin, E. Laryngeal nerve monitoring and minimally invasive thyroid surgery: Complementary technologies. Arch. Otolaryngol. Neck Surg. 2007, 133, 1254–1257. [Google Scholar] [CrossRef] [PubMed]
- Sanabria, A.; Kowalski, L.P.; Nixon, I.; Angelos, P.; Shaha, A.; Owen, R.P.; Suarez, C.; Rinaldo, A.; Ferlito, A. Methodological quality of systematic reviews of intraoperative neuromonitoring in thyroidectomy: A systematic review. JAMA Otolaryngol. Neck Surg. 2019, 145, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Bai, B.; Chen, W. Protective Effects of Intraoperative Nerve Monitoring (IONM) for Recurrent Laryngeal Nerve Injury in Thyroidectomy: Meta-analysis. Sci. Rep. 2018, 8, 7761. [Google Scholar] [CrossRef] [PubMed]
- Cleere, E.F.; Davey, M.G.; Young, O.; Lowery, A.J.; Kerin, M.J. Intra-operative nerve monitoring and recurrent laryngeal nerve injury during thyroid surgery: A network meta-analysis of prospective studies. Langenbeck’s Arch. Surg. 2022, 407, 3209–3219. [Google Scholar] [CrossRef] [PubMed]
- Cirocchi, R.; Arezzo, A.; D’Andrea, V.; Abraha, I.; Popivanov, G.I.; Avenia, N.; Gerardi, C.; Henry, B.M.; Randolph, J.; Barczyñski, M. Intraoperative neuromonitoring versus visual nerve identification for prevention of recurrent laryngeal nerve injury in adults undergoing thyroid surgery. Cochrane Database Syst. Rev. 2019, 1, CD012483. [Google Scholar] [CrossRef] [PubMed]
- Davey, M.G.; Cleere, E.F.; Lowery, A.J.; Kerin, M.J. Intraoperative recurrent laryngeal nerve monitoring versus visualisation alone—A systematic review and meta-analysis of randomized controlled trials. Am. J. Surg. 2022, 224, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Higgins, T.S.; Gupta, R.; Ketcham, A.S.; Sataloff, R.T.; Wadsworth, J.T.; Sinacori, J.T. Recurrent laryngeal nerve monitoring versus identification alone on post-thyroidectomy true vocal fold palsy: A meta-analysis. Laryngoscope 2011, 121, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Graves, C.E.; Jin, C.; Duh, Q.-Y.; Gosnell, J.E.; Shen, W.T.; Suh, I.; Sosa, J.A.; Roman, S.A. Intraoperative nerve monitoring is associated with a lower risk of recurrent laryngeal nerve injury: A national analysis of 17,610 patients. Am. J. Surg. 2021, 221, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.P.; Carnassale, G.; Damiani, G.; Acampora, A.; Raffaelli, M.; De Crea, C.; Bellantone, R. “The final countdown”: Is intraoperative, intermittent neuromonitoring really useful in preventing permanent nerve palsy? Evidence from a meta-analysis. Surgery 2016, 160, 1693–1706. [Google Scholar] [CrossRef]
- Pisanu, A.; Porceddu, G.; Podda, M.; Cois, A.; Uccheddu, A. Systematic review with meta-analysis of studies comparing intraoperative neuromonitoring of recurrent laryngeal nerves versus visualization alone during thyroidectomy. J. Surg. Res. 2014, 188, 152–161. [Google Scholar] [CrossRef]
- Rulli, F.; Ambrogi, V.; Dionigi, G.; Amirhassankhani, S.; Mineo, T.; Ottaviani, F.; Buemi, A.; Di Stefano, P.; Mourad, M. Meta-analysis of recurrent laryngeal nerve injury in thyroid surgery with or without intraoperative nerve monitoring. Acta Otorhinolaryngol. Ital. 2014, 34, 223–229. [Google Scholar] [PubMed]
- Sanabria, A.; Ramirez, A.; Kowalski, L.P.; Silver, C.E.; Shaha, A.R.; Owen, R.P.; Suárez, C.; Khafif, A.; Rinaldo, A.; Ferlito, A. Neuromonitoring in thyroidectomy: A meta-analysis of effectiveness from randomized controlled trials. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 2175–2189. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Liu, J.; Zhang, H.; Zhang, P.; Wang, Z.; Dong, W.; He, L.; Zhang, T. A meta-analysis of intraoperative neuromonitoring of recurrent laryngeal nerve palsy during thyroid reoperations. Clin. Endocrinol. 2017, 87, 572–580. [Google Scholar] [CrossRef]
- Wong, K.P.; Mak, K.L.; Wong, C.K.H.; Lang, B.H.H. Systematic review and meta-analysis on intra-operative neuro-monitoring in high-risk thyroidectomy. Int. J. Surg. 2017, 38, 21–30. [Google Scholar] [CrossRef]
- Yang, S.; Zhou, L.; Lu, Z.; Ma, B.; Ji, Q.; Wang, Y. Systematic review with meta-analysis of intraoperative neuromonitoring during thyroidectomy. Int. J. Surg. 2017, 39, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Pullenayegum, E.; Marshall, J.K.; Iorio, A.; Thabane, L. Impact of including or excluding both-armed zero-event studies on using standard meta-analysis methods for rare event outcome: A simulation study. BMJ Open 2016, 6, e010983. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Dionigi, G.; Pontin, A.; Pino, A.; Caruso, E.; Wu, C.-W.; Sun, H.; Tufano, R.P.; Kim, H.Y. How does neural monitoring help during thyroid sugery for Graves’ disease? J. Clin. Transl. Endocrinol. 2019, 15, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Anuwong, A.; Lavazza, M.; Kim, H.Y.; Wu, C.-W.; Rausei, S.; Pappalardo, V.; Ferrari, C.C.; Inversini, D.; Leotta, A.; Biondi, A.; et al. Recurrent laryngeal nerve management in thyroid surgery: Consequences of routine visualization, application of intermittent, standardized and continuous nerve monitoring. Updates Surg. 2016, 68, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Agha, A.; Glockzin, G.; Ghali, N.; Iesalnieks, I.; Schlitt, H.J. Surgical treatment of substernal goiter: An analysis of 59 patients. Surg. Today 2008, 38, 505–511. [Google Scholar] [CrossRef]
- Akıcı, M.; Çilekar, M.; Yılmaz, S.; Arıkan, Y. Should intraoperative nerve monitoring be used routinely in primary thyroid surgeries? Pak. J. Med. Sci. 2020, 36, 276–280. [Google Scholar] [CrossRef]
- Akkari, M.; Makeieff, M.; Jeandel, C.; Raingeard, I.; Cartier, C.; Garrel, R.; Guerrier, B.; Blanchet, C.; Mondain, M. Thyroid surgery in children and adolescents: A series of 65 cases. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2014, 131, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Alesina, P.F.; Hinrichs, J.; Meier, B.; Cho, E.Y.; Bolli, M.; Walz, M.K. Intraoperative neuromonitoring for surgical training in thyroid surgery: Its routine use allows a safe operation instead of lack of experienced mentoring. World J. Surg. 2014, 38, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Atallah, I.; Dupret, A.; Carpentier, A.-S.; Weingertner, A.S.; Volkmar, P.-P.; Rodier, J.-F. Role of intraoperative neuromonitoring of the recurrent laryngeal nerve in high-risk thyroid surgery. J. Otolaryngol.—Head Neck Surg. 2009, 38, 613–618. [Google Scholar]
- Barczyński, M.; Konturek, A.; Cichoń, S. Randomized clinical trial of visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy. Br. J. Surg. 2009, 96, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Barczyński, M.; Konturek, A.; Pragacz, K.; Papier, A.; Stopa, M.; Nowak, W. Intraoperative nerve monitoring can reduce prevalence of recurrent laryngeal nerve injury in thyroid reoperations: Results of a retrospective cohort study. World J. Surg. 2014, 38, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Bonati, E.; Ivanova, S.; Loderer, T.; Cozzani, F.; Rossini, M.; Giuffrida, M.; DEL Rio, P. Intraoperative neuromonitoring in thyroidectomy for carcinoma in a high-volume academic hospital. Minerva Surg. 2022, 77, 124–129. [Google Scholar] [CrossRef]
- Brajcich, B.C.; McHenry, C.R. The utility of intraoperative nerve monitoring during thyroid surgery. J. Surg. Res. 2016, 204, 29–33. [Google Scholar] [CrossRef]
- Chan, W.-F.; Lang, B.H.-H.; Lo, C.-Y. The role of intraoperative neuromonitoring of recurrent laryngeal nerve during thyroidectomy: A comparative study on 1000 nerves at risk. Surgery 2006, 140, 866–873. [Google Scholar] [CrossRef]
- Chuang, Y.-C.; Huang, S.-M. Protective effect of intraoperative nerve monitoring against recurrent laryngeal nerve injury during re-exploration of the thyroid. World J. Surg. Oncol. 2013, 11, 2–7. [Google Scholar] [CrossRef]
- Demiryas, S.; Donmez, T.; Cekic, E. Effect of nerve monitoring on complications of thyroid surgery. North Clin. Istanb. 2017, 5, 14–19. [Google Scholar] [CrossRef]
- Duclos, A.; Lifante, J.; Ducarroz, S.; Soardo, P.; Colin, C.; Peix, J. Influence of intraoperative neuromonitoring on surgeons’ technique during thyroidectomy. World J. Surg. 2011, 35, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Dudley, S.; Nezakatgoo, N.; Rist, T.M.; Klug, T.; Shires, C.B. The utility of intraoperative nerve monitoring in secondary and tertiary Hyperparathyroid surgery. Clin. Case Rep. 2021, 9, 1634–1640. [Google Scholar] [CrossRef] [PubMed]
- Frattini, F.; Mangano, A.; Boni, L.; Rausei, S.; Biondi, A.; Dionigi, G. Intraoperative neuromonitoring for thyroid malignancy surgery: Technical notes and results from a retrospective series. Updates Surg. 2010, 62, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Gremillion, G.; Fatakia, A.; Dornelles, A.; Amedee, R.G. Intraoperative recurrent laryngeal nerve monitoring in thyroid surgery: Is it worth the cost? Ochsner J. 2012, 12, 363–366. [Google Scholar] [PubMed]
- Grishaeva, P.; Kussmann, J.; Burgstaller, T.; Klutmann, S.; Linder, K.; Fendrich, V. Recurrent laryngeal nerve paresis in benign thyroid surgery with and without intraoperative nerve monitoring. Minerva Surg. 2022, 77, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Hei, H.; Zhou, B.; Qin, J.; Song, Y. Intermittent intraoperative nerve monitoring in thyroid reoperations: Preliminary results of a randomized, single-surgeon study. Head Neck 2016, 38, E1993–E1997. [Google Scholar] [CrossRef] [PubMed]
- Kai, H.; Xixia, L.; Miaoyun, L.; Qinchang, C.; Xinzhi, P.; Dingyuan, L.; Honghao, L. Intraoperative nerve monitoring reduces recurrent laryngeal nerve injury in geriatric patients undergoing thyroid surgery. Acta Oto-Laryngol. 2017, 137, 1275–1280. [Google Scholar] [CrossRef] [PubMed]
- Karakas, E.; Müller, H.-H.; Schlosshauer, T.; Rothmund, M.; Bartsch, D.K. Reoperations for primary hyperparathyroidism—Improvement of outcome over two decades. Langenbeck’s Arch. Surg. 2013, 398, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Fraser, S.; Glover, A.; Sidhu, S. Prospective evaluation of the utility of routine neuromonitoring for an established thyroid surgical practice. ANZ J. Surg. 2017, 87, E138–E142. [Google Scholar] [CrossRef]
- Leow, Y.G.; Lee, C.C.; Gan, J.Y.; Huang, L.M. Comparison of Outcomes of Intra-operative Neuromonitoring of Recurrent Laryngeal Nerve Versus Visualisation Alone during Thyroidectomies: A Singapore Experience. Ann. Acad. Med. Singap. 2020, 49, 870–875. [Google Scholar] [CrossRef]
- Ling, Y.; Zhao, J.; Zhao, Y.; Li, K.; Wang, Y.; Kang, H. Role of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid and parathyroid surgery. J. Int. Med. Res. 2020, 48, 300060520952646. [Google Scholar] [CrossRef] [PubMed]
- Long, M.; Diao, F.; Peng, L.; Tan, L.; Zhu, Y.; Huang, K.; Li, H. Effect of neurological monitoring in postoperative 5–15 days residual thyroidectomy after primary thyroid cancer surgery. Asia-Pacific J. Clin. Oncol. 2018, 14, e332–e335. [Google Scholar] [CrossRef] [PubMed]
- Mirallié, É.; Caillard, C.; Pattou, F.; Brunaud, L.; Hamy, A.; Dahan, M.; Prades, M.; Mathonnet, M.; Landecy, G.; Dernis, H.-P.; et al. Does intraoperative neuromonitoring of recurrent nerves have an impact on the postoperative palsy rate? Results of a prospective multicenter study. Surgery 2017, 163, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Mourad, M.; Kadakia, S.; Jategaonkar, A.; Gordin, E.; Ducic, Y. Intraoperative nerve monitoring during parathyroid surgery: The Fort Worth experience. Head Neck 2017, 39, 1662–1664. [Google Scholar] [CrossRef] [PubMed]
- Netto, I.d.P.; Vartarian, J.G.; Ferraz, P.R.R.; Salgado, P.; de Azevedo, J.B.M.; Toledo, R.N.; Testa, J.R.G.; Carrara-De-Angelis, E.; Kowalski, L.P. Vocal fold immobility after thyroidectomy with intraoperative recurrent laryngeal nerve monitoring. Sao Paulo Med. J. 2007, 125, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Page, C.; Cuvelier, P.; Biet, A.; Strunski, V. Value of intra-operative neuromonitoring of the recurrent laryngeal nerve in total thyroidectomy for benign goitre. J. Laryngol. Otol. 2015, 129, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Pei, M.; Zhu, S.; Zhang, C.; Wang, G.; Hu, M. The value of intraoperative nerve monitoring against recurrent laryngeal nerve injury in thyroid reoperations. Medicine 2021, 100, e28233. [Google Scholar] [CrossRef]
- Polat, A.K.; Lap, G.; Ozbalci, S.; Karabulut, K.; Gungor, B.; Polat, C.; Erzurumlu, K. Intraoperative nerve monitoring in thyroid surgery. Ann. Ital. Chir. 2015, 86, 207–211. [Google Scholar]
- Robertson, M.L.; Steward, D.L.; Gluckman, J.L.; Welge, J. continuous laryngeal nerve integrity monitoring during thyroidectomy: Does it reduce risk of injury? Otolaryngol. Neck Surg. 2004, 131, 596–600. [Google Scholar] [CrossRef]
- Sharif, I.; Mehboob, L. Comparison of use of manual nerve monitor verses continuous nerve monitoring in total thyroidectomy in Pakistan. Int. J. Adv. Biotechnol. Res. 2017, 8, 1954–1956. [Google Scholar]
- Shindo, M.; Chheda, N.N. Incidence of vocal cord paralysis with and without recurrent laryngeal nerve monitoring during thyroidectomy. Arch Otolaryngol—Head Neck Surg. 2007, 133, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Sopiński, J.; Kuzdak, K.; Hedayati, M.; Kołomecki, K. Role of intraoperative neuromonitoring of the recurrent laryngeal nerves during thyroid reoperations of recurrent goiter. Ann. Surg. 2017, 89, 11–15. [Google Scholar] [CrossRef]
- Stevens, K.; Stojadinovic, A.; Helou, L.B.; Solomon, N.P.; Howard, R.S.; Shriver, C.D.; Buckenmaier, C.C.; Henry, L.R. The impact of recurrent laryngeal neuromonitoring on multi-dimensional voice outcomes following thyroid surgery. J. Surg. Oncol. 2012, 105, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Thong, G.; Brophy, C.; Sheahan, P. Use of intraoperative neural monitoring for prognostication of recovery of vocal mobility and reduction of permanent vocal paralysis after thyroidectomy. Head Neck 2021, 43, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Witt, R.L. Recurrent laryngeal nerve electrophysiologic monitoring in thyroid surgery: The standard of care? J. Voice 2005, 19, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Sanabria, A.; Silver, C.E.; Suárez, C.; Shaha, A.; Khafif, A.; Owen, R.P.; Rinaldo, A.; Ferlito, A. Neuromonitoring of the laryngeal nerves in thyroid surgery: A critical appraisal of the literature. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 2383–2395. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 Cochrane; John Wiley & Sons: Chichester, UK, 2022. [Google Scholar]
- Zheng, S.; Xu, Z.; Wei, Y.; Zeng, M.; He, J. Effect of intraoperative neuromonitoring on recurrent laryngeal nerve palsy rates after thyroid surgery—A meta-analysis. J. Formos. Med. Assoc. 2013, 112, 463–472. [Google Scholar] [CrossRef]



















| Author | Year | Favors IONM in Reducing Permanent RLN Injuries | Favors IONM in Reducing Transient RLN Injuries | Favors IONM in Reducing Total RLN Injuries |
|---|---|---|---|---|
| Bai [32] | 2018 | Yes | Yes | Yes |
| Cleere [33] | 2022 | No | No | NS |
| Cirocchi [34] | 2019 | No | No | No |
| Davey [35] | 2022 | No | No | No |
| Higgins [36] | 2011 | No | No | No |
| Kim [37] | 2021 | Yes | Yes | Yes |
| Lombardi [38] | 2016 | No | NS | NS |
| Pisanu [39] | 2014 | No | No | No |
| Rulli [40] | 2014 | No | Yes | NS |
| Sanabria [41] | 2013 | No | No | NS |
| Sun (reoperations) [42] | 2017 | Yes | No | Yes |
| Wong (high-risk patients) (Random effects analysis) [43] | 2017 | No | No | Yes |
| Wong (high-risk patients) (Fixed effects analysis) [43] | 2017 | No | Yes | Yes |
| Yang [44] | 2017 | No | No | No |
| Zheng [45] | 2013 | No | Yes | Yes |
| Category | Type of Injury | Assessment | % Injury IONM | % Injury No IONM | OR (95% CI) IONM vs. No IONM |
|---|---|---|---|---|---|
| All studies | Permanent | NAR | 0.69 | 1.0 | 0.66 (0.56–0.79) |
| Patient | 1.2 | 1.8 | 0.61 (0.49–0.76) | ||
| All studies | Total injuries | NAR | 3.0 | 4.2 | 0.72 (0.65–0.79) |
| Patient | 5.2 | 6.9 | 0.71 (0.64–0.79) | ||
| Randomized | Permanent | NAR | 0.47 | 0.65 | 0.73 (0.33–1.61) |
| Total | NAR | 2.6 | 3.4 | 0.74 (0.52–1.06) | |
| Postoperative laryngoscopy | Permanent | NAR | 0.75 | 1.0 | 0.67 (0.55–0.80) |
| Total | NAR | 3.4 | 4.6 | 0.68 (0.61–0.76) | |
| Contemporaneous controls | Permanent | NAR | 0.72 | 1.1 | 0.67 (0.55–0.82) |
| Total | NAR | 2.9 | 4.9 | 0.65 (0.57–0.74) | |
| Contemporaneous controls AND laryngoscopy | Permanent | NAR | 0.78 | 1.1 | 0.69 (0.56–0.84) |
| Total | NAR | 3.1 | 5.0 | 0.63 (0.55–0.72) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saxe, A.; Idris, M.; Gemechu, J. Does the Use of Intraoperative Neuromonitoring during Thyroid and Parathyroid Surgery Reduce the Incidence of Recurrent Laryngeal Nerve Injuries? A Systematic Review and Meta-Analysis. Diagnostics 2024, 14, 860. https://doi.org/10.3390/diagnostics14090860
Saxe A, Idris M, Gemechu J. Does the Use of Intraoperative Neuromonitoring during Thyroid and Parathyroid Surgery Reduce the Incidence of Recurrent Laryngeal Nerve Injuries? A Systematic Review and Meta-Analysis. Diagnostics. 2024; 14(9):860. https://doi.org/10.3390/diagnostics14090860
Chicago/Turabian StyleSaxe, Andrew, Mohamed Idris, and Jickssa Gemechu. 2024. "Does the Use of Intraoperative Neuromonitoring during Thyroid and Parathyroid Surgery Reduce the Incidence of Recurrent Laryngeal Nerve Injuries? A Systematic Review and Meta-Analysis" Diagnostics 14, no. 9: 860. https://doi.org/10.3390/diagnostics14090860