The Molecular Effects of Ionizing Radiations on Brain Cells: Radiation Necrosis vs. Tumor Recurrence

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Pathophysiology of Brain Radio-Induced Damage
- Depletion of vascular and glial clonogens;
- Decreased of neurogenic cells, mainly located in hippocampi;
- Altered neuronal function and loss of synaptic plasticity;
- Neuro-inflammation secondary to the production of pro-inflammatory cytokines by glial cells.
3. Diagnostic Imaging and Nuclear Medicine in Brain Tumors
4. PET Tracers in Differentiating Recurrence from Treatment Effects
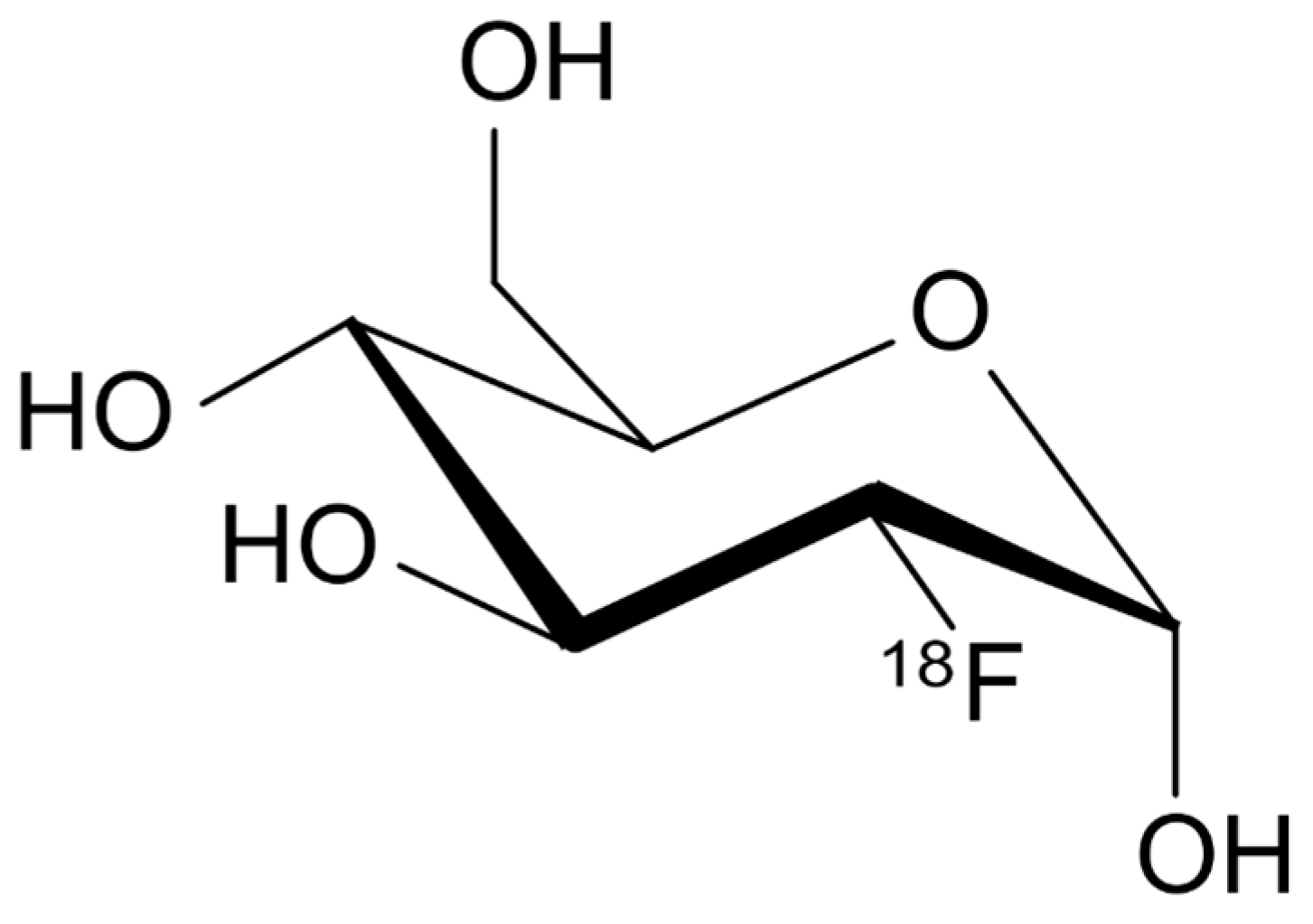
4.1. 18F-FDG
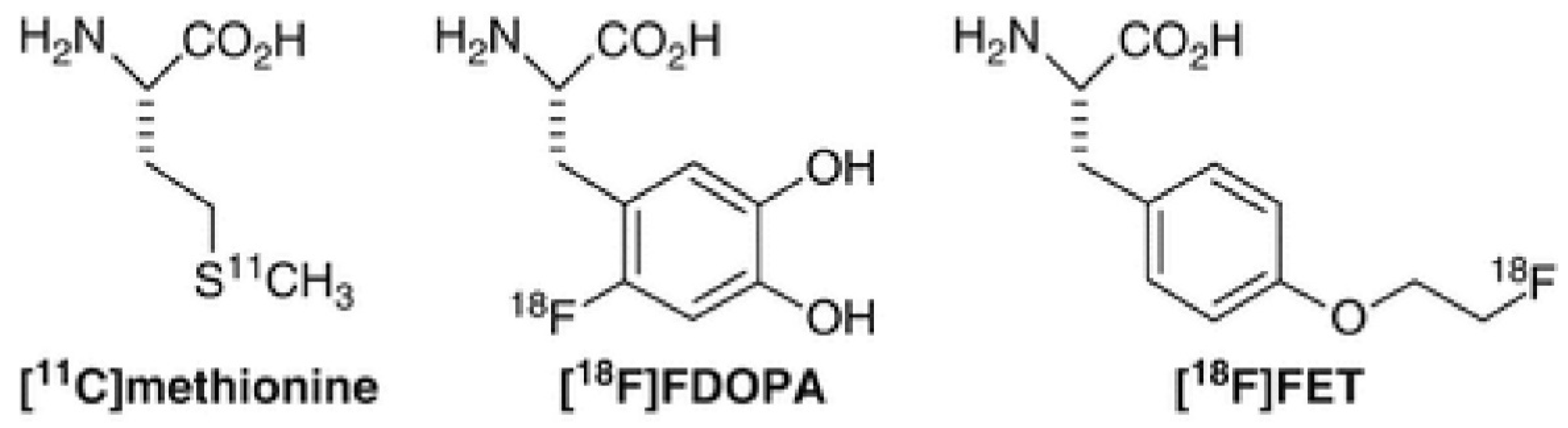
4.2. 11C-MET
4.3. 18F-FET
4.4. 18F-FDOPA
4.5. 18F-FMISO
4.6. 18F-FLT
5. Discussion
6. Future Perspectives
7. Conclusions
Funding
Conflicts of Interest
References
- Kitson, S.L.; Cuccurullo, V.; Moody, T.S.; Mansi, L. Radionuclide antibody-conjugates, a targeted therapy towards cancer. Curr. Radiopharm. 2013, 6, 57–71. [Google Scholar] [CrossRef] [PubMed]
- Dropcho, E.J. Central nervous system injury by therapeutic irradiation. Neurol. Clin. 1991, 9, 969–988. [Google Scholar] [CrossRef]
- Smart, D. Radiation Toxicity in the Central Nervous System: Mechanisms and Strategies for Injury Reduction. Semin. Radiat. Oncol. 2017, 27, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Durand, T.; Feuvret, L.; Mazeron, J.J.; Delattre, J.Y.; Hoang-Xuan, K.; Psimaras, D.; Douzane, H.; Ribeiro, M.; Capelle, L.; et al. Cognitive impairment and morphological changes after radiation therapy in brain tumors: A review. Radiother. Oncol. 2018, 128, 221–228. [Google Scholar] [CrossRef] [PubMed]
- De Felice, F.; Blanchard, P. Radiation-induced neurocognitive dysfunction in head and neck cancer patients. Tumori J. 2017, 103, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Vannorsdall, T.D. Cognitive Changes Related to Cancer Therapy. Med. Clin. North Am. 2017, 101, 1115–1134. [Google Scholar] [CrossRef] [PubMed]
- Ali, F.S.; Hussain, M.R.; Gutiérrez, C.; Demireva, P.; Ballester, L.Y.; Zhu, J.J.; Blanco, A.; Esquenazi, Y. Cognitive disability in adult patients with brain tumors. Cancer Treat Rev. 2018, 65, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Kessler, A.T.; Bhatt, A.A. Brain tumour post-treatment imaging and treatment-related complications. Insights Imaging 2018, 9, 1057–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.M.; Michel, K.A.; Bankson, J.A.; Fuller, C.D.; Klopp, A.H.; Venkatesan, A.M. Emerging Magnetic Resonance Imaging Technologies for Radiation Therapy Planning and Response Assessment. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1046–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiss, W.D. Positron emission tomography imaging in gliomas: applications in clinical diagnosis, for assessment of prognosis and of treatment effects, and for detection of recurrences. Eur. J. Neurol. 2017, 24, 1255–1270. [Google Scholar] [CrossRef] [PubMed]
- Kitson, S.L.; Cuccurullo, V.; Ciarmiello, A.; Mansi, L. Targeted Therapy Towards Cancer-A Perspective. Anticancer. Agents Med. Chem. 2017, 17, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Balentova, S.; Adamkov, M. Molecular, Cellular and Functional Effects of Radiation-Induced Brain Injury: A Review. Int. J. Mol. Sci. 2015, 16, 27796–27815. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.K. A link between vascular damage and cognitive deficits after whole-brain radiation therapy for cancer: A clue to other types of dementia? Drug Discov. Ther. 2016, 10, 79–81. [Google Scholar] [CrossRef] [Green Version]
- Furuse, M.; Nonoguchi, N.; Kawabata, S.; Miyatake, S.; Kuroiwa, T. Delayed brain radiation necrosis: pathological review and new molecular targets for treatment. Med. Mol. Morphol. 2015, 48, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, S.; Nonoguchi, N.; Furuse, M.; Yoritsune, E.; Miyata, T.; Kawabata, S.; Kuroiwa, T. Pathophysiology, diagnosis, and treatment of radiation necrosis in the brain. Neurolmedchir (Tokyo) 2015, 55, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, J.; Prust, M.; Kaiser, J. Chemotherapy, cognitive impairment and hippocampal toxicity. Neuroscience 2015, 309, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.; McBride, W.H.; Schwartz, J.L. Radiation biology in the context of changing patterns of radiotherapy. Radiat. Res. 2014, 182, 259–272. [Google Scholar] [CrossRef]
- Furdui, C.M. Ionizing radiation: mechanisms and therapeutics. Antioxid Redox Signal. 2014, 21, 218–220. [Google Scholar] [CrossRef]
- Suzuki, K. Neurotoxicity of radiation]. Brain Nerve. 2015, 67, 63–71. [Google Scholar]
- Greene-Schloesser, D.; Moore, E.; Robbins, M.E. Molecular pathways: radiation-induced cognitive impairment. Clin. Cancer Res. 2013, 19, 2294–2300. [Google Scholar] [CrossRef]
- Peiffer, A.M.; Leyrer, C.M.; Greene-Schloesser, D.M.; Shing, E.; Kearns, W.T.; Hinson, W.H.; Tatter, S.B.; Ip, E.H.; Rapp, S.R.; Robbins, M.E.; et al. Neuroanatomical target theory as a predictive model for radiation-induced cognitive decline. Neurology 2013, 80, 747–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monje, M. Cranial radiation therapy and damage to hippocampal neurogenesis. Dev. Disabil. Res. Rev. 2008, 14, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Monje, M.; Dietrich, J. Cognitive side effects of cancer therapy demonstrate a functional role for adult neurogenesis. Behav. Brain Res. 2012, 227, 376–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kam, W.W.; Banati, R.B. Effects of ionizing radiation on mitochondria. Free Radic. Biol. Med. 2013, 65, 607–619. [Google Scholar] [CrossRef] [PubMed]
- Grunert, M.; Kassubek, R.; Danz, B.; Klemenz, B.; Hasslacher, S.; Stroh, S.; Schneele, L.; Langhans, J.; Ströbele, S.; Barry, S.E.; et al. Radiation and Brain Tumors: An Overview. Crit. Rev. Oncog. 2018, 23, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Freeman, C.R.; Lehnert, S. Radiotherapy dose-fractionation schedules. Hyperfractionation and accelerated treatment regimens. Neurol. Clin. 1991, 9, 351–362. [Google Scholar] [CrossRef]
- Janss, A.J.; Mazewski, C.; Patterson, B. Guidelines for Treatment and Monitoring of Adult Survivors of Pediatric Brain Tumors. Curr. Treat Options Oncol. 2019, 20, 10. [Google Scholar] [CrossRef]
- Fink, J.R.; Muzi, M.; Peck, M.; Krohn, K.A. Multimodality Brain Tumor Imaging: MR Imaging, PET, and PET/MR Imaging. J. Nucl. Med. 2015, 56, 1554–1561. [Google Scholar] [Green Version]
- Abd-Ellah, M.K.; Awad, A.I.; Khalaf, A.A.M.; Hamed, H.F.A. A review on brain tumor diagnosis from MRI images: Practical implications, key achievements, and lessons learned. Magn. Reson. Imaging 2019, 61, 300–318. [Google Scholar] [CrossRef]
- O’Neill, B.E.; Hochhalter, C.B.; Carr, C.; Strong, M.J.; Ware, M.L. Advances in Neuro-Oncology Imaging Techniques. Ochsner. J. 2018, 18, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Sanai, N.; Berger, M.S. Surgical oncology for gliomas: the state of the art. Nat. Rev. Clin. Oncol. 2018, 15, 112–125. [Google Scholar] [CrossRef]
- Branter, J.; Basu, S.; Smith, S. Tumour treating fields in a combinational therapeutic approach. Oncotarget 2018, 9, 36631–36644. [Google Scholar] [CrossRef] [PubMed]
- Zikou, A.; Sioka, C.; Alexiou, G.A.; Fotopoulos, A.; Voulgaris, S.; Argyropoulou, M.I. Radiation Necrosis, Pseudoprogression, Pseudoresponse, and Tumor Recurrence: Imaging Challenges for the Evaluation of Treated Gliomas. Contrast Media Mol. Imaging 2018, 2018, 682. [Google Scholar] [CrossRef] [PubMed]
- Domachevsky, L.; Jacene, H.A.; Sakellis, C.G.; Kim, C.K. Postradiation changes in tissues: evaluation by imaging studies with emphasis on fluorodeoxyglucose-PET/computed tomography and correlation with histopathologic findings. Pet. Clin. 2014, 9, 217–235. [Google Scholar] [CrossRef] [PubMed]
- Vellayappan, B.; Tan, C.L.; Yong, C.; Khor, L.K.; Koh, W.Y.; Yeo, T.T.; Detsky, J.; Lo, S.; Sahgal, A. Diagnosis and Management of Radiation Necrosis in Patients With Brain Metastases. Front. Oncol. 2018, 8, 395. [Google Scholar] [CrossRef] [PubMed]
- Nowosielski, M.; Wen, P.Y. Imaging Criteria in Neuro-oncology. Semin. Neurol. 2018, 38, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Van den Bent, M.J.; Wefel, J.S.; Schiff, D.; Taphoorn, M.J.; Jaeckle, K.; Junck, L.; Armstrong, T.; Choucair, A.; Waldman, A.D.; Gorlia, T.; et al. Response assessment in neuro-oncology (a report of the RANO group): assessment of outcome in trials of diffuse low-grade gliomas. Lancet Oncol. 2011, 12, 583–593. [Google Scholar] [CrossRef]
- Ali, F.S.; Arevalo, O.; Zorofchian, S.; Patrizz, A.; Riascos, R.; Tandon, N.; Blanco, A.; Ballester, L.Y.; Esquenazi, Y. Cerebral Radiation Necrosis: Incidence, Pathogenesis, Diagnostic Challenges, and Future Opportunities. Curr. Oncol. Rep. 2019, 21, 66. [Google Scholar] [CrossRef] [PubMed]
- Ellingson, B.M.; Chung, C.; Pope, W.B.; Boxerman, J.L.; Kaufmann, T.J. Pseudoprogression, radionecrosis, inflammation or true tumor progression? Challenges associated with glioblastoma response assessment in an evolving therapeutic landscape. J. Neurooncol. 2017, 134, 495–504. [Google Scholar] [CrossRef]
- Mahmood, F.; Johannesen, H.H.; Geertsen, P.; Hansen, R.H. Repeated diffusion MRI reveals earliest time point for stratification of radiotherapy response in brain metastases. Phys. Med. Biol. 2017, 62, 2990–3002. [Google Scholar] [CrossRef] [Green Version]
- Mansi, L.; Ciarmiello, A.; Cuccurullo, V. PET/MRI and the revolution of the third eye. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1519–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peyraga, G.; Robaine, N.; Khalifa, J.; Cohen-Jonathan-Moyal, E.; Payoux, P.; Laprie, A. Molecular PET imaging in adaptive radiotherapy: brain. Q. J. Nucl. Med. Mol. Imaging 2018, 62, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Cistaro, A.; Cuccurullo, V.; Quartuccio, N.; Pagani, M.; Valentini, M.C.; Mansi, L. Role of PET and SPECT in the study of amyotrophic lateral sclerosis. Biomed Res. Int. 2014, 237437, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lupi, A.; Bertagnoni, G.; Borghero, A.; Picelli, A.; Cuccurullo, V.; Zanco, P. 18FDG-PET/CT in traumatic brain injury patients: the relative hypermetabolism of vermis cerebelli as a medium and long term predictor of outcome. Curr. Radiopharm. 2014, 7, 57–62. [Google Scholar] [CrossRef]
- Segtnan, E.A.; Hess, S.; Grupe, P.; Høilund-Carlsen, P.F. 1⁸F-fluorodeoxyglucose PET/computed tomography for primary brain tumors. PET Clin. 2015, 10, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Palanichamy, K.; Chakravarti, A. Diagnostic and Prognostic Significance of Methionine Uptake and Methionine Positron Emission Tomography Imaging in Gliomas. Front. Oncol. 2017, 7, 257. [Google Scholar] [CrossRef] [PubMed]
- Arora, G.; Sharma, P.; Sharma, A.; Mishra, A.K.; Hazari, P.P.; Biswas, A.; Garg, A.; Aheer, D.; Kumar, R. 99mTc-Methionine Hybrid SPECT/CT for Detection of Recurrent Glioma: Comparison With 18F-FDG PET/CT and Contrast-Enhanced MRI. Clin. Nucl. Med. 2018, 43, e132–e138. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Z.; Zhao, X.; Wang, K.; Zhang, Y.; Fan, D.; Yu, T.; Shen, H.; Chen, Q.; Ai, L. Utility of Dynamic Susceptibility Contrast Perfusion-Weighted MR Imaging and 11C-Methionine PET/CT for Differentiation of Tumor Recurrence from Radiation Injury in Patients with High-Grade Gliomas. AJNR Am. J. Neuroradiol. 2019, 40, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Herholz, K. Brain Tumors: An Update on Clinical PET Research in Gliomas. Semin. Nucl. Med. 2017, 47, 5–17. [Google Scholar] [CrossRef]
- Floeth, F.W.; Sabel, M.; Ewelt, C.; Stummer, W.; Felsberg, J.; Reifenberger, G.; Steiger, H.J.; Stoffels, G.; Coenen, H.H.; Langen, K.J. Comparison of (18)F-FET PET and 5-ALA fluorescence in cerebral gliomas. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 731–741. [Google Scholar] [CrossRef]
- Heinzel, A.; Müller, D.; Yekta-Michael, S.S.; Ceccon, G.; Langen, K.J.; Mottaghy, F.M.; Wiesmann, M.; Kocher, M.; Hattingen, E.; Galldiks, N. O-(2-18F-fluoroethyl)-l-tyrosine PET for evaluation of brain metastasis recurrence after radiotherapy: an effectiveness and cost-effectiveness analysis. Neuro. Oncol. 2017, 19, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Humbert, O.; Bourg, V.; Mondot, L.; Gal, J.; Bondiau, P.Y.; Fontaine, D.; Saada-Bouzid, E.; Paquet, M.; Chardin, D.; Almairac, F.; et al. 18F-DOPA PET/CT in brain tumors: impact on multidisciplinary brain tumor board decisions. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Silverman, D.H.; Delaloye, S.; Czernin, J.; Kamdar, N.; Pope, W.; Satyamurthy, N.; Schiepers, C.; Cloughesy, T. 18F-FDOPA PET imaging of brain tumors: comparison study with 18F-FDG PET and evaluation of diagnostic accuracy. J. Nucl. Med. 2006, 47, 904–911. [Google Scholar] [PubMed]
- Schiepers, C.; Chen, W.; Cloughesy, T.; Dahlbom, M.; Huang, S.C. 18F-FDOPA kinetics in brain tumors. J. Nucl. Med. 2007, 48, 1651–1661. [Google Scholar] [CrossRef] [PubMed]
- Gulyás, B.; Halldin, C. New PET radiopharmaceuticals beyond FDG for brain tumor imaging. Q. J. Nucl. Med. Mol. Imaging 2012, 56, 173–190. [Google Scholar]
- Mendichovszky, I.; Jackson, A. Imaging hypoxia in gliomas. Br. J. Radiol. 2011, 84, S145–S158. [Google Scholar] [CrossRef] [Green Version]
- Nikaki, A.; Angelidis, G.; Efthimiadou, R.; Tsougos, I.; Valotassiou, V.; Fountas, K.; Prasopoulos, V.; Georgoulias, P. 18F-fluorothymidine PET imaging in gliomas: an update. Ann. Nucl. Med. 2017, 31, 495–505. [Google Scholar] [CrossRef] [Green Version]
- Nikaki, A.; Papadopoulos, V.; Valotassiou, V.; Efthymiadou, R.; Angelidis, G.; Tsougos, I.; Prassopoulos, V.; Georgoulias, P. Evaluation of the Performance of 18F-Fluorothymidine Positron Emission Tomography/Computed Tomography (18F-FLT-PET/CT) in Metastatic Brain Lesions. Diagnostics 2019, 26, 17. [Google Scholar] [CrossRef]
- Li, C.; Zhang, X.; Pang, L.; Huang, Y.; Gao, Y.; Sun, X.; Yu, J.; Meng, X. Spatial Concordance of Tumor Proliferation and Accelerated Repopulation from Pathologic Images to 3′-[18F]Fluoro-3′-Deoxythymidine PET Images: a Basic Study Guided for PET-Based Radiotherapy Dose Painting. Mol. Imaging Biol. 2018. [Google Scholar] [CrossRef]
- Enslow, M.S.; Zollinger, L.V.; Morton, K.A.; Butterfield, R.I.; Kadrmas, D.J.; Christian, P.E.; Boucher, K.M.; Heilbrun, M.E.; Jensen, R.L.; Hoffman, J.M. Comparison of 18F-fluorodeoxyglucose and 18F-fluorothymidine PET in differentiating radiation necrosis from recurrent glioma. Clin. Nucl. Med. 2012, 37, 854–861. [Google Scholar] [CrossRef]
- Straube, C.; Schmidt-Graf, F.; Wiestler, B.; Zimmer, C.; Meyer, B.; Combs, S.E. The algorithms of adjuvant therapy in gliomas and their effect on survival. J. Neurosurg. Sci. 2019, 63, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Langen, K.J.; Galldiks, N. Update on amino acid PET of brain tumours. Curr. Opin. Neurol. 2018, 31, 354–361. [Google Scholar] [CrossRef]
- Marner, L.; Henriksen, O.M.; Lundemann, M.; Larsen, V.A.; Law, I. Clinical PET/MRI in neurooncology: opportunities and challenges from a single-institution perspective. Clin. Transl. Imaging 2017, 5, 135–149. [Google Scholar] [CrossRef]
- Jung, J.H.; Ahn, B.C. Current Radiopharmaceuticals for Positron Emission Tomography of Brain Tumors. Brain Tumor Res. Treat. 2018, 6, 47–53. [Google Scholar] [CrossRef]
- Tomura, N.; Saginoya, T.; Goto, H. 11C-Methionine Positron Emission Tomography/Computed Tomography Versus 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Evaluation of Residual or Recurrent World Health Organization Grades II and III Meningioma After Treatment. J. Comput. Assist. Tomogr. 2018, 42, 517–521. [Google Scholar] [CrossRef]
- Marvaso, G.; Barone, A.; Amodio, N.; Cascini, G.L.; Scotti, V.; Bianco, C. The current status of novel PET radio-pharmaceuticals in radiotherapy treatment planning of glioma. Curr. Pharm. Biotechnol. 2014, 14, 1099–1104. [Google Scholar] [CrossRef]
- Cuccurullo, V.; Di Stasio, G.D.; Evangelista, L.; Castoria, G.; Mansi, L. Biochemical and Pathophysiological Premises to Positron Emission Tomography With Choline Radiotracers. J. Cell Physiol. 2017, 232, 270–275. [Google Scholar] [CrossRef]
- Takenaka, S.; Asano, Y.; Shinoda, J.; Nomura, Y.; Yonezawa, S.; Miwa, K.; Yano, H.; Iwama, T. Comparison of (11)C-methionine, (11)C-choline, and (18)F-fluorodeoxyglucose-PET for distinguishing glioma recurrence from radiation necrosis. Neurol. Med. Chir. 2014, 54, 280–289. [Google Scholar] [CrossRef]
- Werry, E.L.; Bright, F.M.; Piguet, O.; Ittner, L.M.; Halliday, G.M.; Hodges, J.R.; Kiernan, M.C.; Loy, C.T.; Kril, J.J.; Kassiou, M. Recent Developments in TSPO PET Imaging as A Biomarker of Neuroinflammation in Neurodegenerative Disorders. Int. J. Mol. Sci. 2019, 20. [Google Scholar] [CrossRef]
- Janssen, B.; Mach, R.H. Development of brain PET imaging agents: Strategies for imaging neuroinflammation in Alzheimer’s disease. Prog. Mol. Biol. Transl. Sci. 2019, 165, 371–399. [Google Scholar]
- Ghadery, C.; Best, L.A.; Pavese, N.; Tai, Y.F.; Strafella, A.P. PET Evaluation of Microglial Activation in Non-neurodegenerative Brain Diseases. Curr. Neurol. Neurosci. Rep. 2019, 19, 38. [Google Scholar] [CrossRef] [Green Version]
- Hellberg, S.; Liljenbäck, H.; Eskola, O.; Morisson-Iveson, V.; Morrison, M.; Trigg, W.; Saukko, P.; Ylä-Herttuala, S.; Knuuti, J.; Saraste, A.; et al. Positron Emission Tomography Imaging of Macrophages in Atherosclerosis with 18F-GE-180, a Radiotracer for Translocator Protein (TSPO). Contrast Media Mol. Imaging 2018, 2018, 9186902. [Google Scholar] [CrossRef]
- Unterrainer, M.; Fleischmann, D.F.; Diekmann, C.; Vomacka, L.; Lindner, S.; Vettermann, F.; Brendel, M.; Wenter, V.; Ertl-Wagner, B.; Herms, J.; et al. Comparison of 18F-GE-180 and dynamic 18F-FET PET in high grade glioma: a double-tracer pilot study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 580–590. [Google Scholar] [CrossRef]
- Vomacka, L.; Albert, N.L.; Lindner, S.; Unterrainer, M.; Mahler, C.; Brendel, M.; Ermoschkin, L.; Gosewisch, A.; Brunegraf, A.; Buckley, C.; et al. TSPO imaging using the novel PET ligand [18F]GE-180: quantification approaches in patients with multiple sclerosis. EJNMMI Res. 2017, 7, 89. [Google Scholar] [CrossRef]
- Albert, N.L.; Unterrainer, M.; Fleischmann, D.F.; Lindner, S.; Vettermann, F.; Brunegraf, A.; Vomacka, L.; Brendel, M.; Wenter, V.; Wetzel, C.; et al. TSPO PET for glioma imaging using the novelligand 18F-GE-180: first results in patients with glioblastoma. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 2230–2238. [Google Scholar] [CrossRef]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuccurullo, V.; Di Stasio, G.D.; Cascini, G.L.; Gatta, G.; Bianco, C. The Molecular Effects of Ionizing Radiations on Brain Cells: Radiation Necrosis vs. Tumor Recurrence. Diagnostics 2019, 9, 127. https://doi.org/10.3390/diagnostics9040127
Cuccurullo V, Di Stasio GD, Cascini GL, Gatta G, Bianco C. The Molecular Effects of Ionizing Radiations on Brain Cells: Radiation Necrosis vs. Tumor Recurrence. Diagnostics. 2019; 9(4):127. https://doi.org/10.3390/diagnostics9040127
Chicago/Turabian StyleCuccurullo, Vincenzo, Giuseppe Danilo Di Stasio, Giuseppe Lucio Cascini, Gianluca Gatta, and Cataldo Bianco. 2019. "The Molecular Effects of Ionizing Radiations on Brain Cells: Radiation Necrosis vs. Tumor Recurrence" Diagnostics 9, no. 4: 127. https://doi.org/10.3390/diagnostics9040127