Four-Dimensional Flow Magnetic Resonance Imaging for Assessment of Velocity Magnitudes and Flow Patterns in The Human Carotid Artery Bifurcation: Comparison with Computational Fluid Dynamics

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Outline of the Workflow
2.3. Magnetic Resonance (MR) Imaging Protocol
2.4. MR Imaging Data Processing
2.5. Model Boundary Condition
2.6. MRI Reconstruction and 3D Carotid Artery Model
2.7. Computational Fluid Analysis
2.8. Comparison of Velocity Magnitudes and Flow Pattern
2.9. Statistical Analysis
3. Results
3.1. Correlation of Velocity Magnitude between the 4D Flow MRI and CFD Measurements
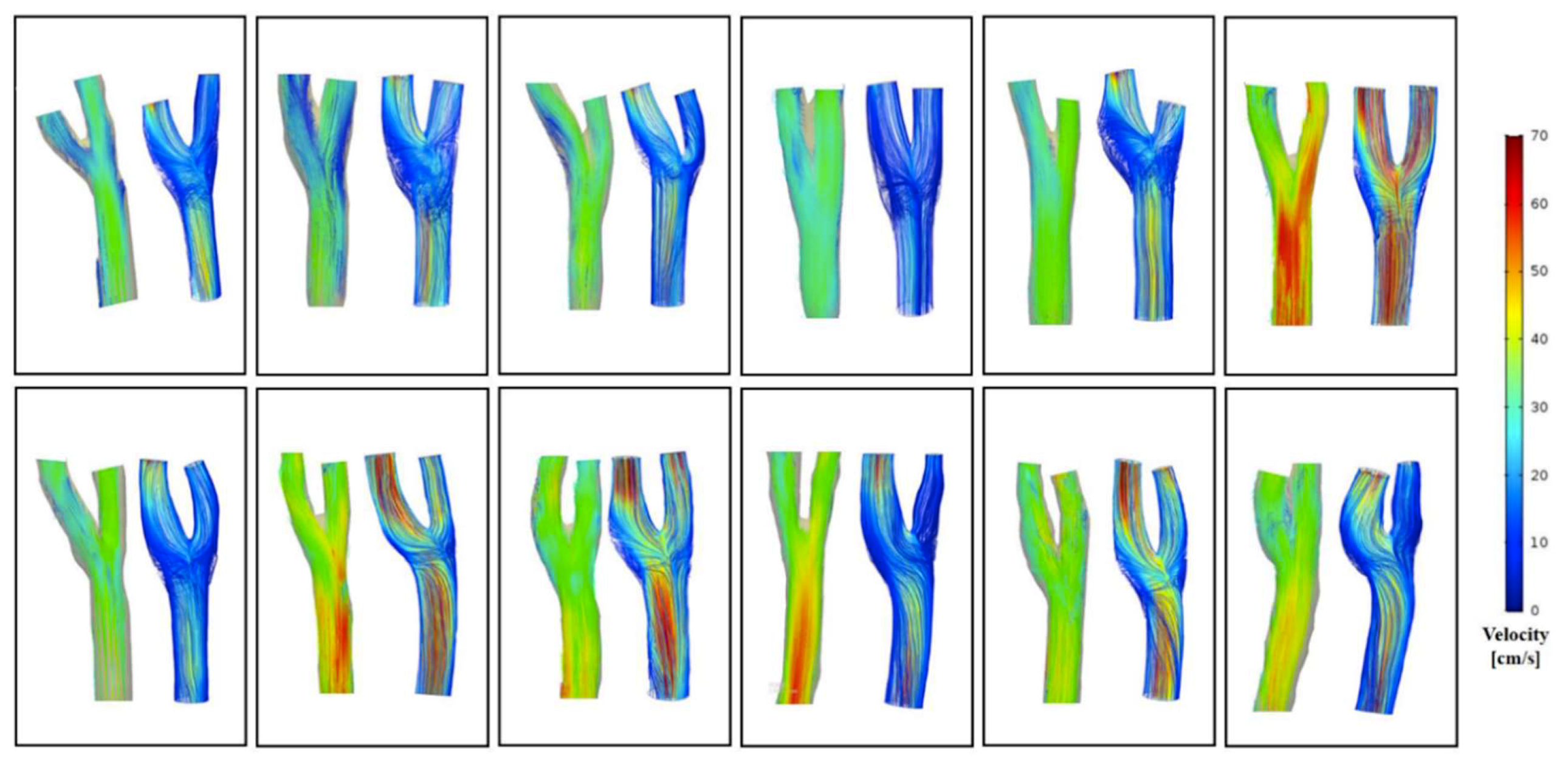
3.2. Comparison of Flow Pattern Derived by the 4D Flow MRI with CFD
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Frangos, S.G.; Gahtan, V.; Sumpio, B. Localization of Atherosclerosis: Role of Hemodynamics. Arch. Surg. 1999, 134, 1142–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeBakey, M.E.; Lawrie, G.M.; Glaeser, D.H. Patterns of atherosclerosis and their surgical significance. Ann. Surg. 1985, 201, 115–131. [Google Scholar] [CrossRef] [PubMed]
- Malek, A.M.; Alper, S.L.; Izumo, S. Hemodynamic Shear Stress and Its Role in Atherosclerosis. JAMA 1999, 282, 2035–2042. [Google Scholar] [CrossRef] [PubMed]
- Harloff, A.; Strecker, C.; Reinhard, M.; Kollum, M.; Handke, M.; Olschewski, M.; Weiller, C.; Hetzel, A. Combined Measurement of Carotid Stiffness and Intima-Media Thickness Improves Prediction of Complex Aortic Plaques in Patients With Ischemic Stroke. Stroke 2006, 37, 2708–2712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harloff, A.; Albrecht, F.; Spreer, J.; Stalder, A.F.; Bock, J.; Frydrychowicz, A.; Schöllhorn, J.; Hetzel, A.; Schumacher, M.; Hennig, J.; et al. 3D blood flow characteristics in the carotid artery bifurcation assessed by flow-sensitive 4D MRI at 3T. Magn. Reson. Med. 2009, 61, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Tempel, D.; van Haperen, R.; van der Baan, A.; Grosveld, F.; Daemen Mat, J.A.P.; Krams, R.; de Crom, R. Atherosclerotic Lesion Size and Vulnerability Are Determined by Patterns of Fluid Shear Stress. Circulation 2006, 113, 2744–2753. [Google Scholar] [CrossRef] [Green Version]
- Gelfand, B.D.; Epstein, F.H.; Blackman, B.R. Spatial and spectral heterogeneity of time-varying shear stress profiles in the carotid bifurcation by phase-contrast MRI. J. Magn. Reson. Imaging 2006, 24, 1386–1392. [Google Scholar] [CrossRef]
- Schnell, S.; Wu, C.; Ansari, S.A. Four-dimensional MRI flow examinations in cerebral and extracerebral vessels—Ready for clinical routine? Curr. Opin. Neurol. 2016, 29, 419–428. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, S.; Itatani, K.; Furusawa, T.; Nishino, T.; Sugiyama, M.; Takehara, Y.; Yasukochi, S. Validation of numerical simulation methods in aortic arch using 4D Flow MRI. Heart Vessel. 2017, 32, 1032–1044. [Google Scholar] [CrossRef]
- Markl, M.; Chan, F.P.; Alley, M.T.; Wedding, K.L.; Draney, M.T.; Elkins, C.J.; Parker, D.W.; Wicker, R.; Taylor, C.A.; Herfkens, R.J.; et al. Time-resolved three-dimensional phase-contrast MRI. J. Magn. Reson. Imaging 2003, 17, 499–506. [Google Scholar] [CrossRef] [Green Version]
- Markl, M.; Harloff, A.; Bley, T.A.; Zaitsev, M.; Jung, B.; Weigang, E.; Langer, M.; Hennig, J.; Frydrychowicz, A. Time-resolved 3D MR velocity mapping at 3T: Improved navigator-gated assessment of vascular anatomy and blood flow. J. Magn. Reson. Imaging 2007, 25, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Sughimoto, K.; Shimamura, Y.; Tezuka, C.; Tsubota, K.i.; Liu, H.; Okumura, K.; Masuda, Y.; Haneishi, H. Effects of arterial blood flow on walls of the abdominal aorta: Distributions of wall shear stress and oscillatory shear index determined by phase-contrast magnetic resonance imaging. Heart Vessel. 2016, 31, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- Wetzel, S.; Meckel, S.; Frydrychowicz, A.; Bonati, L.; Radue, E.-W.; Scheffler, K.; Hennig, J.; Markl, M. In Vivo Assessment and Visualization of Intracranial Arterial Hemodynamics with Flow-Sensitized 4D MR Imaging at 3T. Am. J. Neuroradiol. 2007, 28, 433–438. [Google Scholar] [PubMed]
- Sarrami-Foroushani, A.; Nasr Esfahany, M.; Nasiraei Moghaddam, A.; Saligheh Rad, H.; Firouznia, K.; Shakiba, M.; Ghanaati, H.; Wilkinson, I.D.; Frangi, A.F. Velocity Measurement in Carotid Artery: Quantitative Comparison of Time-Resolved 3D Phase-Contrast MRI and Image-based Computational Fluid Dynamics. Iran. J. Radiol. Q. J. Publ. By Iran. Radiol. Soc. 2015, 12, e18286. [Google Scholar] [CrossRef] [Green Version]
- Cibis, M.; Potters, W.V.; Gijsen, F.J.H.; Marquering, H.; vanBavel, E.; van der Steen, A.F.W.; Nederveen, A.J.; Wentzel, J.J. Wall shear stress calculations based on 3D cine phase contrast MRI and computational fluid dynamics: A comparison study in healthy carotid arteries. NMR Biomed. 2014, 27, 826–834. [Google Scholar] [CrossRef]
- Steinman, D.A.; Thomas, J.B.; Ladak, H.M.; Milner, J.S.; Rutt, B.K.; Spence, J.D. Reconstruction of carotid bifurcation hemodynamics and wall thickness using computational fluid dynamics and MRI. Magn. Reson. Med. 2002, 47, 149–159. [Google Scholar] [CrossRef]
- Hua, Y.; Oh, J.H.; Kim, Y.B. Influence of Parent Artery Segmentation and Boundary Conditions on Hemodynamic Characteristics of Intracranial Aneurysms. Yonsei Med. J. 2015, 56, 1328–1337. [Google Scholar] [CrossRef]
- Isoda, H.; Ohkura, Y.; Kosugi, T.; Hirano, M.; Alley, M.T.; Bammer, R.; Pelc, N.J.; Namba, H.; Sakahara, H. Comparison of hemodynamics of intracranial aneurysms between MR fluid dynamics using 3D cine phase-contrast MRI and MR-based computational fluid dynamics. Neuroradiology 2010, 52, 913–920. [Google Scholar] [CrossRef] [Green Version]
- Gatehouse, P.D.; Keegan, J.; Crowe, L.A.; Masood, S.; Mohiaddin, R.H.; Kreitner, K.-F.; Firmin, D.N. Applications of phase-contrast flow and velocity imaging in cardiovascular MRI. Eur. Radiol. 2005, 15, 2172–2184. [Google Scholar] [CrossRef]
- Gharahi, H.; Zambrano, B.A.; Zhu, D.C.; DeMarco, J.K.; Baek, S. Computational fluid dynamic simulation of human carotid artery bifurcation based on anatomy and volumetric blood flow rate measured with magnetic resonance imaging. Int. J. Adv. Eng. Sci. Appl. Math. 2016, 8, 40–60. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-W.; Antiga, L.; Spence, J.D.; Steinman David, A. Geometry of the Carotid Bifurcation Predicts Its Exposure to Disturbed Flow. Stroke 2008, 39, 2341–2347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cebral, J.R.; Putman, C.M.; Alley, M.T.; Hope, T.; Bammer, R.; Calamante, F. Hemodynamics in Normal Cerebral Arteries: Qualitative Comparison of 4D Phase-Contrast Magnetic Resonance and Image-Based Computational Fluid Dynamics. J. Eng. Math. 2009, 64, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Harloff, A.; Zech, T.; Wegent, F.; Strecker, C.; Weiller, C.; Markl, M. Comparison of Blood Flow Velocity Quantification by 4D Flow MR Imaging with Ultrasound at the Carotid Bifurcation. Am. J. Neuroradiol. 2013, 34, 1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinman, D.A.; Ethier, C.R.; Rutt, B.K. Combined analysis of spatial and velocity displacement artifacts in phase contrast measurements of complex flows. J. Magn. Reson. Imaging 1997, 7, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.; Kim, G.B.; Kweon, J.; Lee, S.J.; Kim, Y.-H.; Lee, D.H.; Yang, D.H.; Kim, N. Hemodynamic Measurement Using Four-Dimensional Phase-Contrast MRI: Quantification of Hemodynamic Parameters and Clinical Applications. Korean J. Radiol 2016, 17, 445–462. [Google Scholar] [CrossRef] [Green Version]
- Ha, H.; Kim, G.B.; Kweon, J.; Kim, Y.-H.; Kim, N.; Yang, D.H.; Lee, S.J. Multi-VENC acquisition of four-dimensional phase-contrast MRI to improve precision of velocity field measurement. Magn. Reson. Med. 2016, 75, 1909–1919. [Google Scholar] [CrossRef]
- Ku, D.N. BLOOD FLOW IN ARTERIES. Annu. Rev. Fluid Mech. 1997, 29, 399–434. [Google Scholar] [CrossRef]
- Dyvorne, H.; Knight-Greenfield, A.; Jajamovich, G.; Besa, C.; Cui, Y.; Stalder, A.; Markl, M.; Taouli, B. Abdominal 4D Flow MR Imaging in a Breath Hold: Combination of Spiral Sampling and Dynamic Compressed Sensing for Highly Accelerated Acquisition. Radiology 2015, 275, 245–254. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Velocity at the Carotid Bifurcation (n = 12) | 4D Flow MRI | CFD | Difference | p |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Maximum velocity (cm/s) | 50.29 ± 11.66 | 47.21 ± 11.02 | 6.12% | 0.05 |
| Minimum velocity (cm/s) | 23.06 ± 11.84 | 17.19 ± 3.85 | 25.46% | 0.11 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngo, M.T.; Kim, C.I.; Jung, J.; Chung, G.H.; Lee, D.H.; Kwak, H.S. Four-Dimensional Flow Magnetic Resonance Imaging for Assessment of Velocity Magnitudes and Flow Patterns in The Human Carotid Artery Bifurcation: Comparison with Computational Fluid Dynamics. Diagnostics 2019, 9, 223. https://doi.org/10.3390/diagnostics9040223
Ngo MT, Kim CI, Jung J, Chung GH, Lee DH, Kwak HS. Four-Dimensional Flow Magnetic Resonance Imaging for Assessment of Velocity Magnitudes and Flow Patterns in The Human Carotid Artery Bifurcation: Comparison with Computational Fluid Dynamics. Diagnostics. 2019; 9(4):223. https://doi.org/10.3390/diagnostics9040223
Chicago/Turabian StyleNgo, Minh Tri, Chul In Kim, Jinmu Jung, Gyung Ho Chung, Dong Hwan Lee, and Hyo Sung Kwak. 2019. "Four-Dimensional Flow Magnetic Resonance Imaging for Assessment of Velocity Magnitudes and Flow Patterns in The Human Carotid Artery Bifurcation: Comparison with Computational Fluid Dynamics" Diagnostics 9, no. 4: 223. https://doi.org/10.3390/diagnostics9040223