
Cerebral Protection in TAVR—Can We Do Without? A Real-World All-Comer Intention-to-Treat Study—Impact on Stroke Rate, Length of Hospital Stay, and Twelve-Month Mortality

 , , , , ,
, , , , ,  ,
,  ,
,
Abstract
:1. Background
2. Methods
2.1. Study Population
2.2. Transcatheter Aortic Valve Replacement
2.3. Sentinel™ Cerebral Protection Device
2.4. Histopathology
2.5. Definition of Endpoints
2.6. Statistical Analysis
3. Results
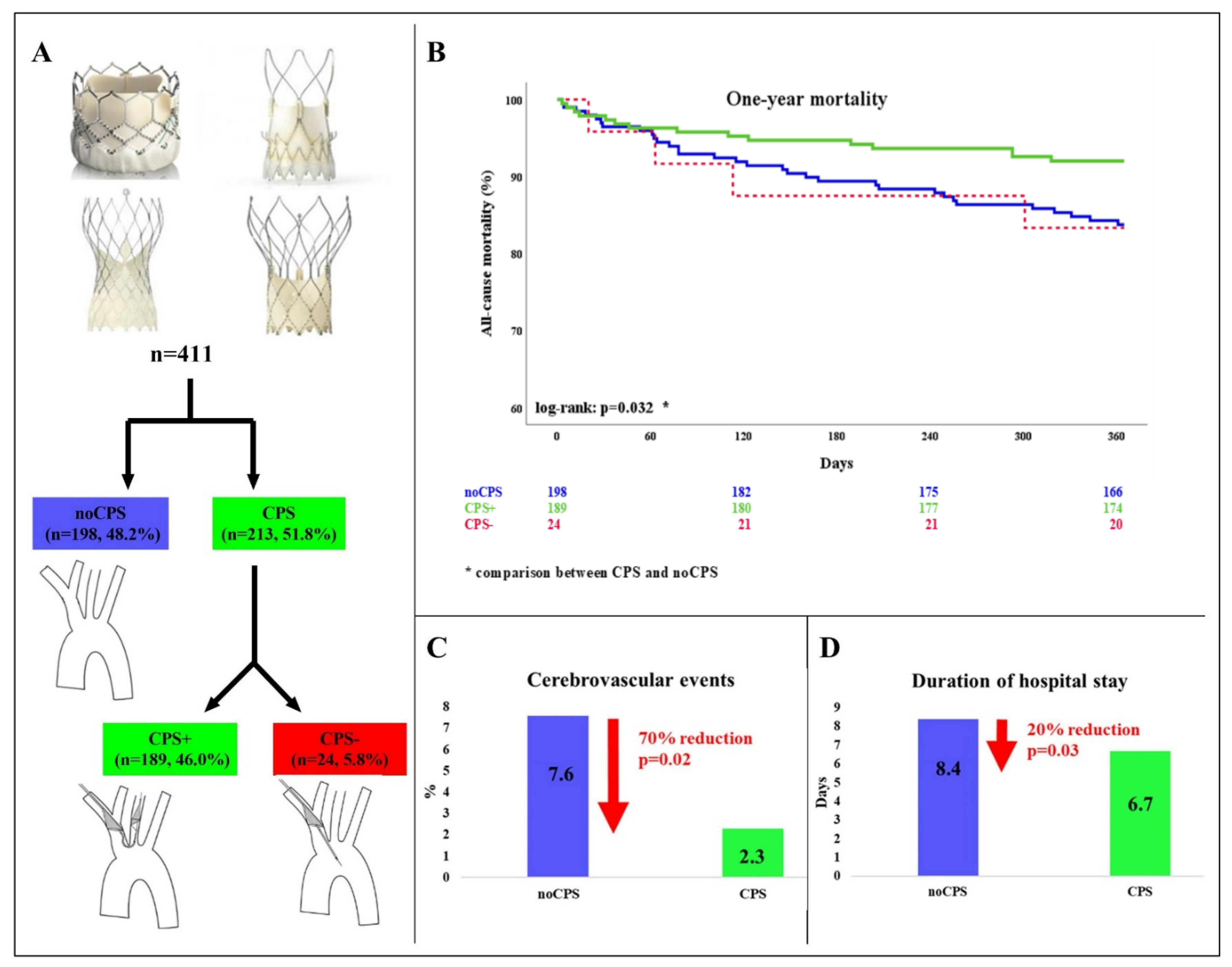
3.1. Patient Population
3.2. Cerebrovascular Events
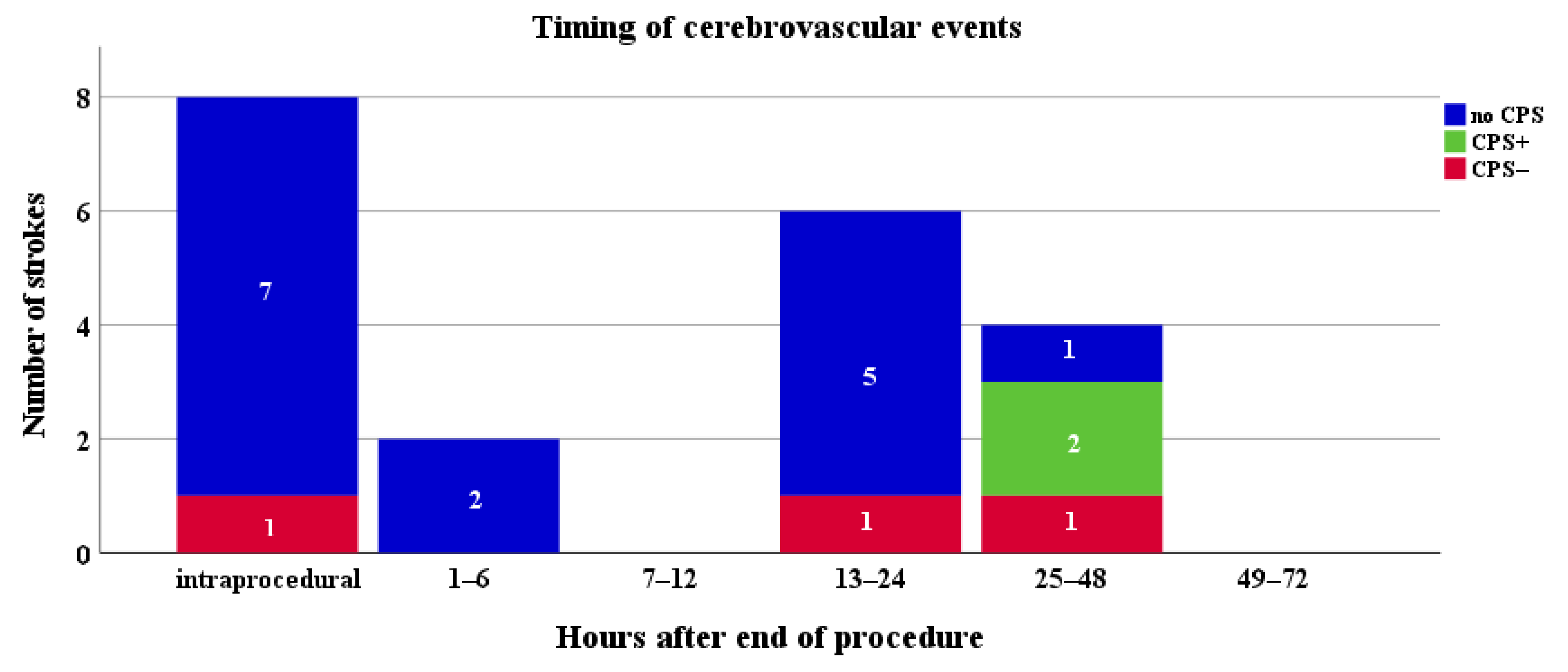
3.3. Timing of Stroke
3.4. All-Cause Mortality at 12 Months
3.5. Length of Hospital Stay
3.6. Learning Curve
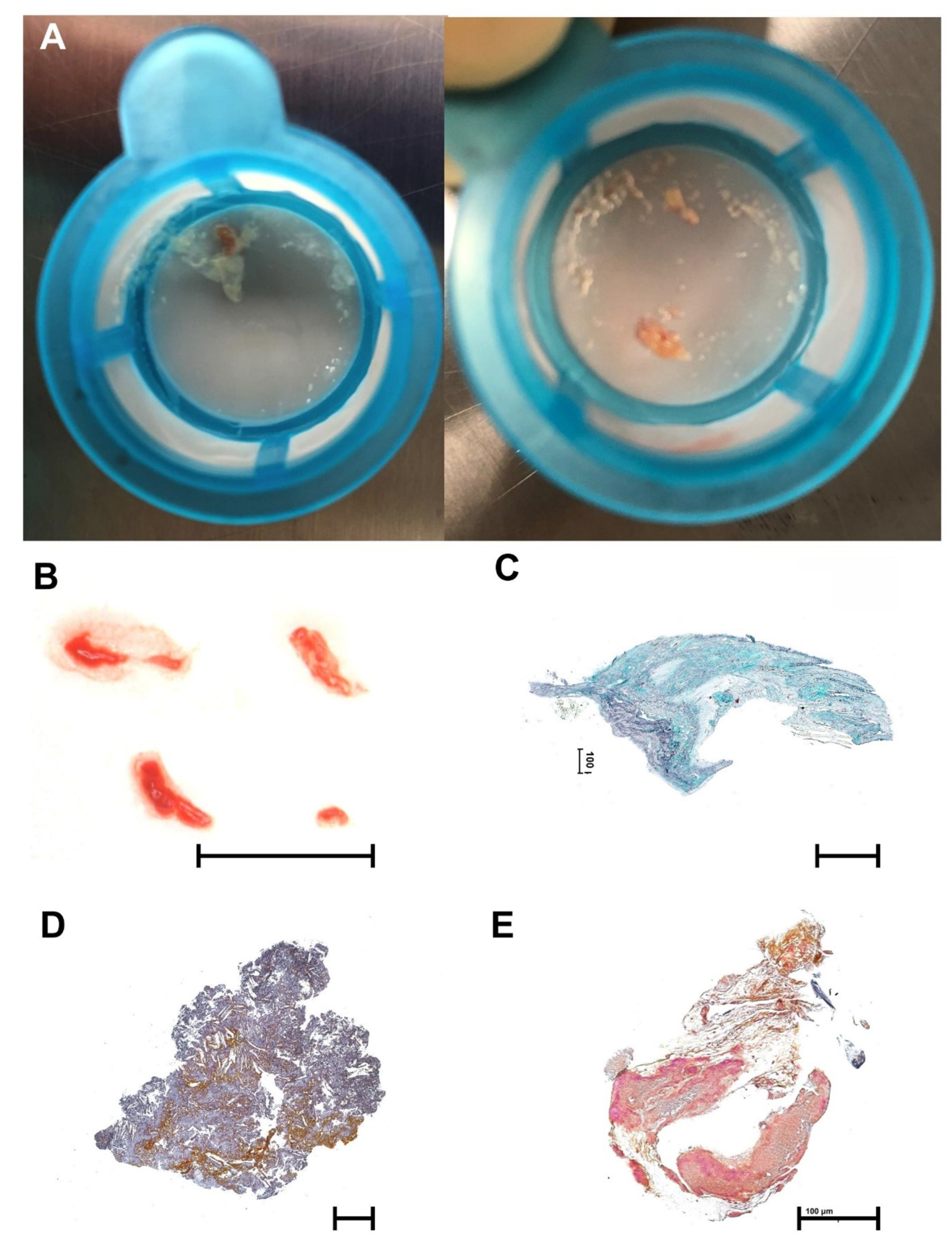
3.7. Histopathology
4. Discussion
5. Limitations
6. Conclusions
Impact on Daily Practice
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Iung, B.; Vahanian, A. Epidemiology of acquired valvular heart disease. Can. J. Cardiol. 2014, 30, 962–970. [Google Scholar] [CrossRef]
- Carroll, J.D.; Mack, M.J.; Vemulapalli, S.; Herrmann, H.C.; Gleason, T.G.; Hanzel, G.; Deeb, G.M.; Thourani, V.H.; Cohen, D.J.; Desai, N.; et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 76, 2492–2516. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 77, 450–500. [Google Scholar] [CrossRef]
- Tay, E.L.W.; Gurvitch, R.; Wijesinghe, N.; Nielispach, F.; Wood, D.; Cheung, A.; Ye, J.; Lichtenstein, S.V.; Carere, R.; Thompson, C.; et al. A high-risk period for cerebrovascular events exists after transcatheter aortic valve implantation. JACC Cardiovasc. Interv. 2011, 4, 1290–1297. [Google Scholar] [CrossRef]
- Nombela-Franco, L.; Webb, J.G.; de Jaegere, P.P.; Toggweiler, S.; Nuis, R.-J.; Dager, A.E.; Amat-Santos, I.J.; Cheung, A.; Ye, J.; Binder, R.K.; et al. Timing, predictive factors, and prognostic value of cerebrovascular events in a large cohort of patients undergoing transcatheter aortic valve implantation. Circulation 2012, 126, 3041–3053. [Google Scholar] [CrossRef]
- Mastoris, I.; Schoos, M.M.; Dangas, G.D.; Mehran, R. Stroke after transcatheter aortic valve replacement: Incidence, risk factors, prognosis, and preventive strategies. Clin. Cardiol. 2014, 37, 756–764. [Google Scholar] [CrossRef]
- Kapadia, S.; Agarwal, S.; Miller, D.C.; Webb, J.G.; MacK, M.; Ellis, S.; Herrmann, H.C.; Pichard, A.D.; Tuzcu, E.M.; Svensson, L.G.; et al. Insights into Timing, Risk Factors, and Outcomes of Stroke and Transient Ischemic Attack after Transcatheter Aortic Valve Replacement in the PARTNER Trial (Placement of Aortic Transcatheter Valves). Circ. Cardiovasc. Interv. 2016, 9, 1–10. [Google Scholar] [CrossRef]
- Auffret, V.; Regueiro, A.; Del Trigo, M.; Abdul-Jawad Altisent, O.; Campelo-Parada, F.; Chiche, O.; Puri, R.; Rodes-Cabau, J. Predictors of Early Cerebrovascular Events in Patients With Aortic Stenosis Undergoing Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 68, 673–684. [Google Scholar] [CrossRef]
- Haussig, S.; Mangner, N.; Dwyer, M.G.; Lehmkuhl, L.; Lücke, C.; Woitek, F.; Holzhey, D.M.; Mohr, F.W.; Gutberlet, M.; Zivadinov, R.; et al. Effect of a Cerebral Protection Device on Brain Lesions Following Transcatheter Aortic Valve Implantation in Patients With Severe Aortic Stenosis: The CLEAN-TAVI Randomized Clinical Trial. JAMA 2016, 316, 592–601. [Google Scholar] [CrossRef]
- Kapadia, S.R.; Kodali, S.; Makkar, R.; Mehran, R.; Lazar, R.M.; Zivadinov, R.; Dwyer, M.G.; Jilaihawi, H.; Virmani, R.; Anwaruddin, S.; et al. Protection Against Cerebral Embolism During Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2017, 69, 367–377. [Google Scholar] [CrossRef]
- Van Mieghem, N.M.; van Gils, L.; Ahmad, H.; van Kesteren, F.; van der Werf, H.W.; Brueren, G.; Storm, M.; Lenzen, M.; Daemen, J.; van den Heuvel, A.F.M.; et al. Filter-based cerebral embolic protection with transcatheter aortic valve implantation: The randomised MISTRAL-C trial. EuroIntervention 2016, 12, 499–507. [Google Scholar] [CrossRef]
- Seeger, J.; Gonska, B.; Otto, M.; Rottbauer, W.; Wohrle, J. Cerebral Embolic Protection During Transcatheter Aortic Valve Replacement Significantly Reduces Death and Stroke Compared With Unprotected Procedures. JACC. Cardiovasc. Interv. 2017, 10, 2297–2303. [Google Scholar] [CrossRef]
- Seeger, J.; Kapadia, S.R.; Kodali, S.; Linke, A.; Wohrle, J.; Haussig, S.; Makkar, R.; Mehran, R.; Rottbauer, W.; Leon, M. Rate of peri-procedural stroke observed with cerebral embolic protection during transcatheter aortic valve replacement: A patient-level propensity-matched analysis. Eur. Heart J. 2019, 40, 1334–1340. [Google Scholar] [CrossRef]
- Megaly, M.; Sorajja, P.; Cavalcante, J.L.; Pershad, A.; Gössl, M.; Abraham, B.; Omer, M.; Elbadawi, A.; Garcia, S. Ischemic Stroke With Cerebral Protection System During Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, 2149–2155. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Muñoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Genereux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.-A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. Eur. Heart J. 2012, 33, 2403–2418. [Google Scholar] [CrossRef]
- Zhao, M.; Amin-Hanjani, S.; Ruland, S.; Curcio, A.P.; Ostergren, L.; Charbel, F.T. Regional cerebral blood flow using quantitative MR angiography. AJNR Am. J. Neuroradiol. 2007, 28, 1470–1473. [Google Scholar] [CrossRef]
- Vlastra, W.; Vendrik, J.; Koch, K.T.; Baan, J.; Piek, J.J.; Delewi, R. Cerebral protection devices during transcatheter aortic valve implantation. Trends Cardiovasc. Med. 2018, 28, 412–418. [Google Scholar] [CrossRef]
- Garvey, W.; Fathi, A.; Bigelow, F.; Capenter, B.J.C. Stain technology—A combined elastic, fibrin and collagen stain. Biotech. Histochem. 1987, 2, 26. [Google Scholar] [CrossRef]
- Seeger, J.; Falk, V.; Hildick-Smith, D.; Bleiziffer, S.; Blackman, D.J.; Abdel-Wahab, M.; Allocco, D.J.; Meredith, I.T.; Wöhrle, J.; Van Mieghem, N.M. Insights on Embolic Protection, Repositioning, and Stroke: A Subanalysis of the RESPOND Study. J. Interv. Cardiol. 2020, 2020, 3070427. [Google Scholar] [CrossRef]
- Nuis, R.-J.; Van Mieghem, N.M.; Schultz, C.J.; Moelker, A.; van der Boon, R.M.; van Geuns, R.J.; van der Lugt, A.; Serruys, P.W.; Rodes-Cabau, J.; van Domburg, R.T.; et al. Frequency and causes of stroke during or after transcatheter aortic valve implantation. Am. J. Cardiol. 2012, 109, 1637–1643. [Google Scholar] [CrossRef]
- Makkar, R.R.; Fontana, G.P.; Jilaihawi, H.; Kapadia, S.; Pichard, A.D.; Douglas, P.S.; Thourani, V.H.; Babaliaros, V.C.; Webb, J.G.; Herrmann, H.C.; et al. Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N. Engl. J. Med. 2012, 366, 1696–1704. [Google Scholar] [CrossRef]
- Dowbiggin, P.L.; Infinger, A.E.; Purick, G.T.; Swanson, D.R.; Asimos, A.; Rhoten, J.B.; VonCannon, S.; Dometrovich, M.; Studnek, J.R. Prehospital Evaluation of the FAST-ED as a Secondary Stroke Screen to Identify Large Vessel Occlusion Strokes. Prehospital Emerg. Care 2021, 1–6. [Google Scholar] [CrossRef]
- Nijenhuis, V.J.; Bennaghmouch, N.; van Kuijk, J.-P.; Capodanno, D.; ten Berg, J.M. Antithrombotic treatment in patients undergoing transcatheter aortic valve implantation (TAVI). Thromb. Haemost. 2015, 113, 674–685. [Google Scholar] [CrossRef]
- Armijo, G.; Nombela-Franco, L.; Tirado-Conte, G. Cerebrovascular Events After Transcatheter Aortic Valve Implantation. Front. Cardiovasc. Med. 2018, 5, 104. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef]
- Tam, D.Y.; Qiu, F.; Elbaz-Greener, G.; Henning, K.A.; Humphries, K.H.; Lauck, S.B.; Webb, J.; Fremes, S.E.; Wijeysundera, H.C. Predictors of Cumulative Health Care Costs Associated With Transcatheter Aortic Valve Replacement in Severe Aortic Stenosis. Can. J. Cardiol. 2020, 36, 1244–1251. [Google Scholar] [CrossRef]
- Stachon, P.; Kaier, K.; Heidt, T.; Wolf, D.; Duerschmied, D.; Staudacher, D.; Zehender, M.; Bode, C.; von Zur Mühlen, C. The Use and Outcomes of Cerebral Protection Devices for Patients Undergoing Transfemoral Transcatheter Aortic Valve Replacement in Clinical Practice. JACC. Cardiovasc. Interv. 2021, 14, 161–168. [Google Scholar] [CrossRef]
- Kaier, K.; Reinecke, H.; Naci, H.; Frankenstein, L.; Bode, M.; Vach, W.; Hehn, P.; Zirlik, A.; Zehender, M.; Reinöhl, J. The impact of post-procedural complications on reimbursement, length of stay and mechanical ventilation among patients undergoing transcatheter aortic valve implantation in Germany. Eur. J. Health Econ. 2018, 19, 223–228. [Google Scholar] [CrossRef]
- Durand, E.; Avinée, G.; Gillibert, A.; Tron, C.; Bettinger, N.; Bouhzam, N.; Gilard, M.; Verhoye, J.P.; Koning, R.; Lefevre, T.; et al. Analysis of length of stay after transfemoral transcatheter aortic valve replacement: Results from the FRANCE TAVI registry. Clin. Res. Cardiol. 2021, 110, 40–49. [Google Scholar] [CrossRef]
- Elbaz-Greener, G.; Rozen, G.; Kusniec, F.; Marai, I.; Carasso, S.; Ko, D.T.; Wijeysundera, H.C.; Alcalai, R.; Planer, D.; Amir, O. Comparing Trajectory of Surgical Aortic Valve Replacement in the Early vs. Late Transcatheter Aortic Valve Replacement Era. Front. Cardiovasc. Med. 2021, 8, 680123. [Google Scholar] [CrossRef]
- Seeger, J.; Virmani, R.; Romero, M.; Gonska, B.; Rottbauer, W.; Wöhrle, J. Significant Differences in Debris Captured by the Sentinel Dual-Filter Cerebral Embolic Protection During Transcatheter Aortic Valve Replacement Among Different Valve Types. JACC. Cardiovasc. Interv. 2018, 11, 1683–1693. [Google Scholar] [CrossRef]
- Vermeer, S.E.; Prins, N.D.; den Heijer, T.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M.B. Silent Brain Infarcts and the Risk of Dementia and Cognitive Decline. N. Engl. J. Med. 2003, 348, 1215–1222. [Google Scholar] [CrossRef]
- De Carlo, M.; Liga, R.; Migaleddu, G.; Scatturin, M.; Spaccarotella, C.; Fiorina, C.; Orlandi, G.; De Caro, F.; Rossi, M.L.; Chieffo, A.; et al. Evolution, Predictors, and Neurocognitive Effects of Silent Cerebral Embolism During Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, 1291–1300. [Google Scholar] [CrossRef]
- Lansky, A.J.; Schofer, J.; Tchetche, D.; Stella, P.; Pietras, C.G.; Parise, H.; Abrams, K.; Forrest, J.K.; Cleman, M.; Reinöhl, J.; et al. A prospective randomized evaluation of the TriGuardTM HDH embolic DEFLECTion device during transcatheter aortic valve implantation: Results from the DEFLECT III trial. Eur. Heart J. 2015, 36, 2070–2078. [Google Scholar] [CrossRef]
- Nazif, T.M.; Moses, J.; Sharma, R.; Dhoble, A.; Rovin, J.; Brown, D.; Horwitz, P.; Makkar, R.; Stoler, R.; Forrest, J.; et al. Randomized Evaluation of TriGuard 3 Cerebral Embolic Protection After Transcatheter Aortic Valve Replacement: REFLECT II. JACC. Cardiovasc. Interv. 2021, 14, 515–527. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All n = 411 | noCPS n = 198 (48.2%) | CPS n = 213 (51.8%) | CPS+ n = 189 (46.0%) | CPS− n = 24 (5.8%) | p-Value * | |
|---|---|---|---|---|---|---|
| Clinical and laboratory parameters | ||||||
| Age, y | 80.4 ± 6.7 | 80.4 ± 6.8 | 80.4 ± 6.7 | 80.3 ± 6.6 | 81.2 ± 7.3 | 1.000 |
| Sex, female, % | 195 (47.4) | 100 (50.5) | 95 (44.6) | 88 (46.6) | 7 (29.2) | 0.231 |
| BMI, kg/m2 | 27.2 ± 5.2 | 27.0 ± 5.3 | 27.3 ± 5.2 | 27.3 ± 5.1 | 27.5 ± 5.9 | 0.474 |
| Arterial hypertension, % | 364 (89.2) | 175 (89.3) | 189 (89.2) | 169 (89.9) | 20 (83.3) | 0.965 |
| Diabetes mellitus, % | 136 (33.4) | 65 (33.2) | 71 (33.6) | 66 (35.1) | 5 (21.7) | 0.917 |
| Peripheral artery disease, % | 46 (11.3) | 19 (9.7) | 27 (12.8) | 23 (12.2) | 4 (17.4) | 0.323 |
| Coronary artery disease, % | 260 (63.7) | 127 (64.8) | 133 (62.7) | 116 (61.7) | 17 (70.8) | 0.665 |
| Carotid artery stenosis, % | 55 (13.5) | 23 (11.7) | 32 (15.2) | 29 (15.4) | 3 (13.0) | 0.665 |
| Hyperlipidemia, % | 297 (73.2) | 136 (69.4) | 161 (76.7) | 140 (74.9) | 21 (91.3) | 0.098 |
| Prior stroke, % | 30 (7.4) | 15 (7.7) | 15 (7.1) | 11 (5.9) | 4 (17.4) | 0.834 |
| Atrial fibrillation, % | 169 (41.5) | 86 (43.9) | 83 (39.3) | 71 (37.8) | 12 (52.2) | 0.353 |
| COPD, % | 46 (11.3) | 20 (10.2) | 26 (12.3) | 23 (12.2) | 3 (12.5) | 0.500 |
| Prior cardiac surgery, % | 58 (14.1) | 27 (13.6) | 31 (14.6) | 24 (12.7) | 7 (29.2) | 0.789 |
| NYHA functional class | 0.187 | |||||
| I, % | 29 (7.6) | 13 (7.1) | 16 (8.0) | 16 (9.0) | 0.0 | |
| II, % | 113 (29.4) | 50 (26.9) | 63 (31.7) | 55 (31.1) | 8 (36.4) | |
| III, % | 225 (58.4) | 115 (61.8) | 110 (55.3) | 98 (55.4) | 12 (54.5) | |
| IV, % | 18 (4.7) | 8 (4.3) | 10 (5.0) | 8 (4.5) | 2 (9.1) | |
| CCS ≥ III, % | 36 (8.9) | 18 (9.1) | 18 (8.6) | 15 (8.1) | 3 (12.5) | 0.853 |
| Syncope, % | 65 (16.8) | 28 (14.9) | 37 (18.6) | 34 (19.2) | 3 (13.6) | 0.331 |
| NT-proBNP, pg/mL | 3844 ± 6517 | 4139 ± 6670 | 3584 ± 6413 | 3414 ± 6062 | 4898 ± 8721 | 0.406 |
| Creatinine, mg/dL | 1.34 ± 0.91 | 1.35 ± 0.82 | 1.34 ± 1.00 | 1.34 ± 1.03 | 1.33 ± 0.63 | 0.869 |
| Oral anticoagulation, % | 139 (34.1) | 74 (37.4) | 65 (31.0) | 55 (29.6) | 10 (41.7) | 0.171 |
| SAPT, % | 136 (33.1) | 56 (31.5) | 64 (34.9) | 56 (34.4) | 7 (38.9) | 0.504 |
| DAPT, % | 101 (28.1) | 45 (25.3) | 56 (30.8) | 52 (31.7) | 4 (22.2) | 0.247 |
| EuroSCORE II, % | 6.3 ± 5.9 | 6.4 ± 5.4 | 6.4 ± 6.4 | 6.2 ± 6.2 | 7.9 ± 7.6 | 0.997 |
| Echocardiographic parameters | ||||||
| AV mPG, mmHg | 47 ± 15 | 46 ± 14 | 49 ± 17 | 50 ± 17 | 41 ± 14 | 0.035 |
| AV pPG, mmHg | 75 ± 23 | 73 ± 21 | 78 ± 25 | 80 ± 25 | 66 ± 20 | 0.030 |
| AV Vmax, m/s | 4.3 ± 0.7 | 4.2 ± 0.6 | 4.4 ± 0.7 | 4.4 ± 0.7 | 4.0 ± 0.6 | 0.111 |
| AVA, cm2 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.126 |
| AS Stage, % | 0.906 | |||||
| High gradient | 279 (73.6) | 134 (73.2) | 145 (74.0) | 131 (75.7) | 14 (60.9) | |
| LFLG + LVEF < 50% | 47 (12.4) | 22 (12.0) | 25 (12.8) | 21 (12.1) | 4 (17.4) | |
| LFLG + LVEF ≥ 50% | 53 (14.0) | 27 (14.8) | 26 (13.3) | 21 (12.1) | 5 (21.7) | |
| AR ≥ II, % | 28 (7.1) | 16 (8.1) | 12 (6.0) | 11 (6.2) | 1 (4.3) | 0.409 |
| MR ≥ II, % | 67 (16.9) | 39 (19.9) | 28 (14.0) | 22 (12.4) | 6 (26.1) | 0.118 |
| TR ≥ II, % | 69 (17.3) | 38 (19.2) | 31 (15.5) | 26 (14.7) | 5 (21.7) | 0.331 |
| LVEF, % | 50 ± 9 | 49 ± 9 | 50 ± 9 | 50 ± 9 | 49 ± 10 | 0.315 |
| Procedural characteristics | ||||||
| Self-expanding valves, % † | 263 (64.0) | 134 (67.7) | 129 (60.6) | 116 (61.4) | 13 (54.2) | 0.133 |
| Valve size, mm | 27 ± 3 | 27 ± 3 | 26 ± 3 | 26 ± 3 | 27 ± 3 | 0.163 |
| Conscious sedation, % | 392 (95.4) | 186 (93.9) | 206 (96.7) | 182 (96.3) | 24 (100) | 0.181 |
| Procedure time, min | 59 ± 30 | 57 ± 24 | 60 ± 35 | 60 ± 36 | 61 ± 27 | 0.301 |
| Predilation, % | 198 (49.0) | 92 (47.2) | 106 (50.7) | 95 (51.4) | 11 (45.8) | 0.477 |
| Postdilation, % | 103 (25.6) | 49 (25.3) | 54 (25.8) | 48 (25.9) | 6 (25.0) | 0.894 |
| Fluoroscopy time, min | 17 ± 9 | 16 ± 8 | 19 ± 9 | 19 ± 9 | 21 ± 9 | < 0.001 |
| Contrast, mL | 144 ± 55 | 149 ± 59 | 139 ± 52 | 139 ± 51 | 138 ± 60 | 0.079 |
| Implantation > 1 valve, % | 7 (1.7) | 4 (2.0) | 3 (1.4) | 2 (1.1) | 1 (4.2) | 0.716 |
| Valve-in-valve, % | 28 (6.9) | 13 (6.6) | 15 (7.1) | 13 (6.9) | 2 (8.3) | 0.860 |
| All n = 411 | noCPS n = 198 (48.2%) | CPS n = 213 (51.8%) | CPS+ n = 189 (46.0%) | CPS− n = 24 (5.8%) | p-Value * | |
|---|---|---|---|---|---|---|
| Cerebrovascular event at 72 h | 20 (4.9) | 15 (7.6) | 5 (2.3) | 2 (1.1) | 3 (12.5) | 0.014 |
| Disabling stroke (%) | 10 (2.4) | 7 (3.5) | 3 (1.4) | 1 (0.5) | 2 (8.3) | 0.162 |
| Non-disabling stroke (%) | 8 (1.9) | 6 (3.0) | 2 (0.9) | 1 (0.5) | 1 (4.2) | 0.162 |
| TIA (%) | 2 (0.5) | 2 (1.0) | 0 | 0 | 0 | 0.231 |
| All-cause mortality at 72 h (%) | 2 (0.5) | 1 (0.5) | 1 (0.5) | 1 (0.5) | 0 | 0.939 |
| All-cause mortality at 12 months | 51 (12.4) | 32 (16.2) | 19 (8.9) | 15 (7.9) | 4 (16.7) | 0.026 |
| Hospital stay (days) | 7.5 ± 8.0 | 8.4 ± 9.6 | 6.7 ± 6.1 | 6.4 ± 5.4 | 8.6 ± 9.9 | 0.031 |
| Univariate Regression | Multivariate Regression | |||
|---|---|---|---|---|
| Odds Ratio (95%CI) | p-Value | Odds Ratio (95%CI) | p-Value | |
| Baseline characteristics | ||||
| Sex, female | 0.727 (0.291–1.818) | 0.496 | ||
| Age | 1.007 (0.942–1.078) | 0.829 | ||
| Body mass index | 1.002 (0.916–1.096) | 0.969 | ||
| Arterial hypertension | 0.664 (0.187–2.362) | 0.527 | ||
| Diabetes mellitus | 1.365 (0.544–3.421) | 0.507 | ||
| Peripheral artery disease | 0.404 (0.053–3.087) | 0.382 | ||
| Coronary artery disease | 1.768 (0.630–4.967) | 0.279 | ||
| Carotid stenosis > 70% | 2.267 (0.789–6.508) | 0.128 | ||
| Hyperlipidemia | 1.498 (0.490–4.583) | 0.479 | ||
| Previous stroke | - | |||
| Atrial fibrillation | 0.938 (0.375–2.347) | 0.892 | ||
| COPD | 1.369 (0.386–4.854) | 0.627 | ||
| Previous cardiac surgery | 1.574 (0.507–4.886) | 0.432 | ||
| Previous syncope | 1.538 (0.486–4.875) | 0.464 | ||
| NYHA functional class | 0.938 (0.515–1.708) | 0.835 | ||
| CCS ≥ III | 1.157 (0.257–5.198) | 0.849 | ||
| NT-proBNP (log.) | 0.680 (0.297–1.560) | 0.363 | ||
| Creatinine | 0.773 (0.375–1.592) | 0.484 | ||
| Oral anticoagulation | 1.618 (0.654–4.001) | 0.296 | ||
| SAPT | 1.898 (0.750–4.805) | 0.176 | ||
| DAPT | 0.676 (0.219–2.089) | 0.497 | ||
| EuroSCORE II | 1.019 (0.955–1.088) | 0.566 | ||
| Echocardiographic parameters | ||||
| AV mPG | 0.979 (0.946–1.014) | 0.235 | ||
| AV pPG | 0.993 (0.970–1.015) | 0.519 | ||
| AVA | 2.167 (0.165–28.388) | 0.556 | ||
| AV Vmax | 0.772 (0.373–1.598) | 0.486 | ||
| LVEF | 0.987 (0.942–1.035) | 0.592 | ||
| Procedural characteristics | ||||
| Self-expanding valve | 1.390 (0.563–3.433) | 0.476 | ||
| SentinelTM | 0.293 (0.105–0.823) | 0.020 | 0.239 (0.075–0.762) | 0.016 |
| Valve size | 1.077 (0.927–1.250) | 0.331 | ||
| Predilation | 0.746 (0.294–1.896) | 0.539 | ||
| Postdilation | 1.042 (0.366–2.968) | 0.938 | ||
| Procedure time | 1.010 (1.001–1.020) | 0.032 | 1.009 (0.969–1.075) | 0.129 |
| Implantation >1 valve | 32.083 (6.620–155.493) | <0.001 | 16.710 (2.687–103.923) | 0.003 |
| Fluoroscopy time | 1.051 (1.010–1.093) | 0.014 | 1.021 (0.969–1.075) | 0.436 |
| Univariate Regression | Multivariate Regression | |||
|---|---|---|---|---|
| Odds Ratio (95%CI) | p-Value | Odds Ratio (95%CI) | p-Value | |
| Baseline characteristics | ||||
| Sex, female | 1.712 (0.964–3.040) | 0.067 | ||
| Age | 0.999 (0.959–1.040) | 0.956 | ||
| Body mass index | 0.988 (0.930–1.049) | 0.684 | ||
| Arterial hypertension | 0.532 (0.259–1.093) | 0.086 | ||
| Diabetes mellitus | 1.563 (0.898–2.720) | 0.114 | ||
| Peripheral artery disease | 2.286 (1.173–4.457) | 0.015 | 0.935 (0.319–2.744) | 0.903 |
| Coronary artery disease | 1.530 (0.827–2.830) | 0.175 | ||
| Carotid stenosis > 70% | 1.653 (0.828–3.300) | 0.154 | ||
| Hyperlipidemia | 0.776 (0.429–1.401) | 0.400 | ||
| Previous stroke | 0.772 (0.240–2.479) | 0.664 | ||
| Atrial fibrillation | 2.335 (1.331–4.097) | 0.003 | 1.343 (0.662–2.724) | 0.413 |
| COPD | 1.066 (0.455–2.499) | 0.883 | ||
| Previous cardiac surgery | 1.926 (1.088–3.678) | 0.047 | 0.611 (0.185–2.016) | 0.419 |
| Previous syncope | 1.159 (0.562–2.393) | 0.689 | ||
| NYHA functional class | 1.882 (1.184–2.993) | 0.008 | 1.212 (0.727–2.021) | 0.460 |
| CCS ≥ III | 0.635 (0.198–2.040) | 0.446 | ||
| NT-proBNP (log.) | 1.369 (1.098–1.708) | 0.005 | 1.180 (0.885–1.574) | 0.259 |
| Creatinine | 1.162 (0.933–1.446) | 0.180 | ||
| Oral anticoagulation | 1.583 (0.906–2.767) | 0.107 | ||
| SAPT | 1.184 (0.638–2.197) | 0.593 | ||
| DAPT | 0.882 (0.444–1.749) | 0.719 | ||
| EuroSCORE II | 1.055 (1.025–1.085) | <0.001 | 1.034 (0.984–1.088) | 0.186 |
| Echocardiographic parameters | ||||
| AV mPG * | 0.978 (0.958–0.998) | 0.032 | 0.986 (0.963–1.011) | 0.271 |
| AV pPG * | 0.983 (0.970–0.997) | 0.018 | ||
| AVA | 1.690 (0.342–8.345) | 0.519 | ||
| AV Vmax * | 0.609 (0.397–0.936) | 0.024 | ||
| LVEF | 0.982 (0.954–1.010) | 0.199 | ||
| Procedural characteristics | ||||
| Self-expanding valve | 0.796 (0.441–1.439) | 0.451 | ||
| SentinelTM | 0.478 (0.262–0.873) | 0.016 | 0.454 (0.222–0.931) | 0.031 |
| Valve size | 1.058 (0.962–1.164) | 0.246 | ||
| Predilation | 0.888 (0.509–1.548) | 0.674 | ||
| Postdilation | 0.831 (0.425–1.622) | 0.586 | ||
| Procedure time | 1.014 (1.008–1.020) | <0.001 | 1.016 (1.005–1.027) | 0.005 |
| Implantation > 1 valve | 2.755 (0.670–11.330) | 0.160 | ||
| Fluoroscopy time | 1.026 (0.999–1.054) | 0.059 | ||
| Univariate Regression | Multivariate Regression | |||
|---|---|---|---|---|
| Regression Coefficient (95%CI) | p-Value | Regression Coefficient (95%CI) | p-Value | |
| Baseline characteristics | ||||
| Sex, female | 0.173 (−1.385, 1.731) | 0.827 | ||
| Age | 0.126 (0.911, 0.241) | 0.031 | ||
| Body mass index | −0.076 (−0.249, 0.098) | 0.390 | ||
| Arterial hypertension | −0.703 (−3.225, 1.819) | 0.584 | ||
| Diabetes mellitus | 0.558 (−1.105, 2.200) | 0.510 | ||
| Peripheral artery disease | 0.845 (−1.632, 3.322) | 0.503 | ||
| Coronary artery disease | 1.831 (0.213, 3.449) | 0.027 | 1.332 (−0.327, 2.990) | 0.115 |
| Carotid stenosis > 70% | −0.490 (−2.785, 1.804) | 0.675 | ||
| Hyperlipidemia | −0.493 (−2.267, 1.282) | 0.585 | ||
| Previous stroke | 0.000 (−3.003, 3.003) | 1.000 | ||
| Atrial fibrillation | 0.515 (−1.076, 2.106) | 0.525 | ||
| COPD | −0.488 (−2.955, 1.979) | 0.697 | ||
| Previous cardiac surgery | −0.239 (−2.474, 1.995) | 0.833 | ||
| Previous syncope | 2.227 (0.126, 4.328) | 0.038 | 1.834 (−0.309, 3.976) | 0.093 |
| NYHA functional class | 0.737 (−0.265, 1.739) | 0.149 | ||
| CCS ≥ III | −0.324 (−3.087, 2.440) | 0.818 | ||
| NT-proBNP (log.) | 2.263 (0.976, 3.550) | <0.001 | 0.426 (−0.293, 1.144) | 0.244 |
| Creatinine | 0.650 (−0.205, 1.505) | 0.136 | ||
| Oral anticoagulation | 0.057 (−1.584, 1.699) | 0.945 | ||
| SAPT | 0.585 (−1.161, 2.332) | 0.510 | ||
| DAPT | −0.072 (−1.899, 1.755) | 0.938 | ||
| EuroSCORE II | 0.117 (−0.013, 0.247) | 0.078 | ||
| Echocardiographic parameters | ||||
| AV mPG | −0.030 (−0.084, 0.024) | 0.273 | ||
| AV pPG | −0.003 (−0.040, 0.034) | 0.871 | ||
| AVA | −5.240 (−9.953, −0.527) | 0.029 | −4.355 (−8.985, 0.275) | 0.065 |
| AV Vmax | 0.077 (−1.194, 1.348) | 0.906 | ||
| LVEF | −0.101 (−0.192, −0.011) | 0.029 | −0.072 (−0.166, 0.023) | 0.136 |
| Procedural characteristics | ||||
| Self-expanding valve | 1.480 (−0.134, 3.094) | 0.072 | ||
| SentinelTM | −1.972 (−3.520, −0.423) | 0.013 | −2.474 (−4.075, −0.874) | 0.003 |
| Valve size | −0.015 (−0.301, 0.270) | 0.915 | ||
| Predilation | −0.864 (−2.441, 0.713) | 0.282 | ||
| Postdilation | −1.064 (−2.875, 0.748) | 0.249 | ||
| Procedure time | 0.023 (−0.003, 0.048) | 0.088 | ||
| Implantation > 1 valve | 3.386 (−2.634, 9.405) | 0.269 | ||
| Fluoroscopy time | 0.127 (0.036, 0.219) | 0.006 | 0.196 (0.097, 0.294) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donà, C.; Koschutnik, M.; Nitsche, C.; Winter, M.-P.; Seidl, V.; Siller-Matula, J.; Mach, M.; Andreas, M.; Bartko, P.; Kammerlander, A.A.; et al. Cerebral Protection in TAVR—Can We Do Without? A Real-World All-Comer Intention-to-Treat Study—Impact on Stroke Rate, Length of Hospital Stay, and Twelve-Month Mortality. J. Pers. Med. 2022, 12, 320. https://doi.org/10.3390/jpm12020320
Donà C, Koschutnik M, Nitsche C, Winter M-P, Seidl V, Siller-Matula J, Mach M, Andreas M, Bartko P, Kammerlander AA, et al. Cerebral Protection in TAVR—Can We Do Without? A Real-World All-Comer Intention-to-Treat Study—Impact on Stroke Rate, Length of Hospital Stay, and Twelve-Month Mortality. Journal of Personalized Medicine. 2022; 12(2):320. https://doi.org/10.3390/jpm12020320
Chicago/Turabian StyleDonà, Carolina, Matthias Koschutnik, Christian Nitsche, Max-Paul Winter, Veronika Seidl, Jolanta Siller-Matula, Markus Mach, Martin Andreas, Philipp Bartko, Andreas Anselm Kammerlander, and et al. 2022. "Cerebral Protection in TAVR—Can We Do Without? A Real-World All-Comer Intention-to-Treat Study—Impact on Stroke Rate, Length of Hospital Stay, and Twelve-Month Mortality" Journal of Personalized Medicine 12, no. 2: 320. https://doi.org/10.3390/jpm12020320