
Comprehensive Deciphering the Complexity of the Deep Bite: Insight from Animal Model to Human Subjects
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Etiology
- A tongue protrusion to the side or an improper tongue position that causes the back teeth to be infraoccluding;
- Abrasive tooth wear or erosion of the occlusal surface;
- The posterior teeth’s anterior tips pointing toward the extraction sites;
- Continually sucking one’s thumb.
1.2. Deep Bite Prevalence
2. Methods
2.1. Literature Search for Research on the Genetics of Deep Bite Development
2.2. Clinical Records and Ethical Statement
2.3. Growth Considerations
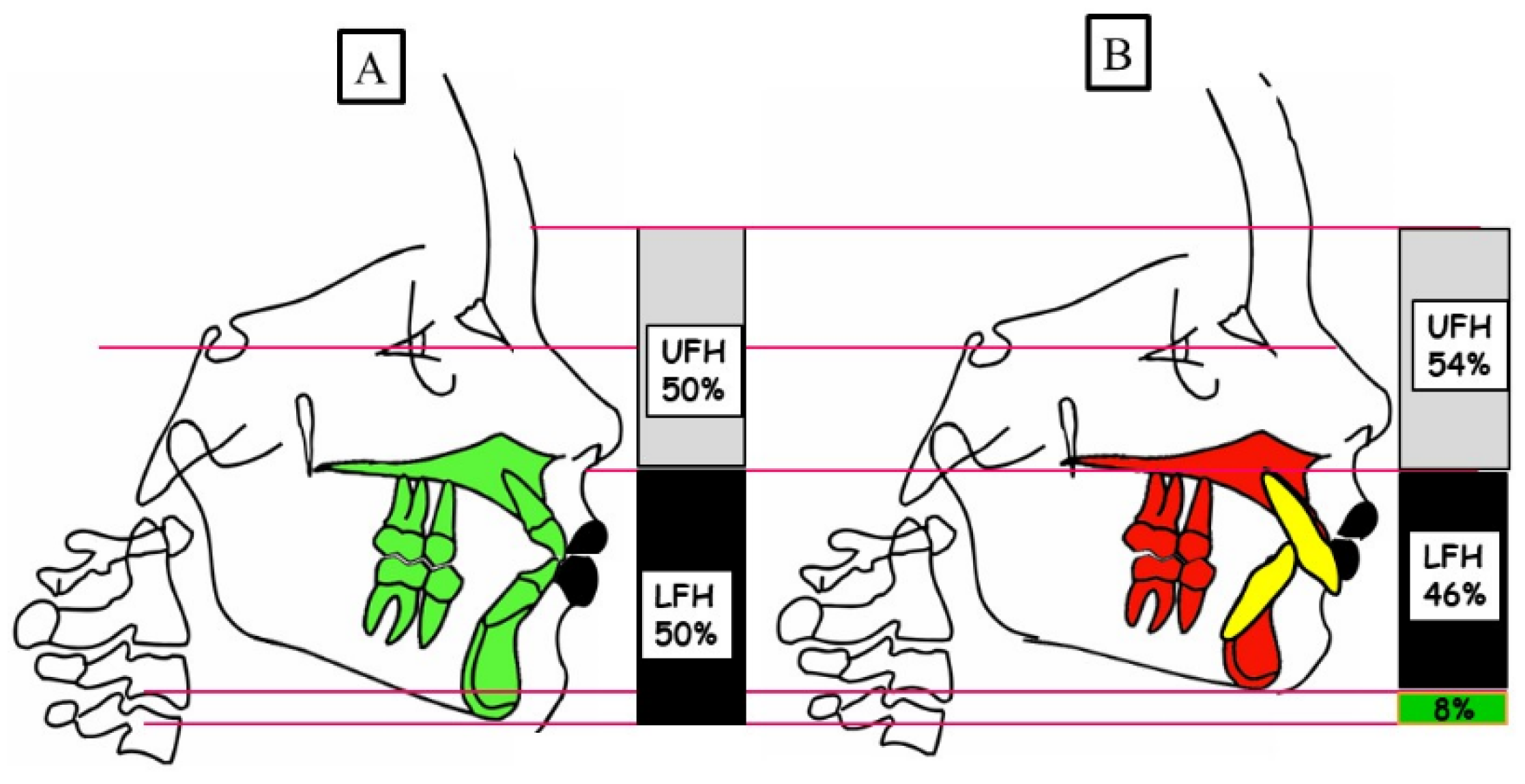
2.4. Assessment of the Vertical Dimension
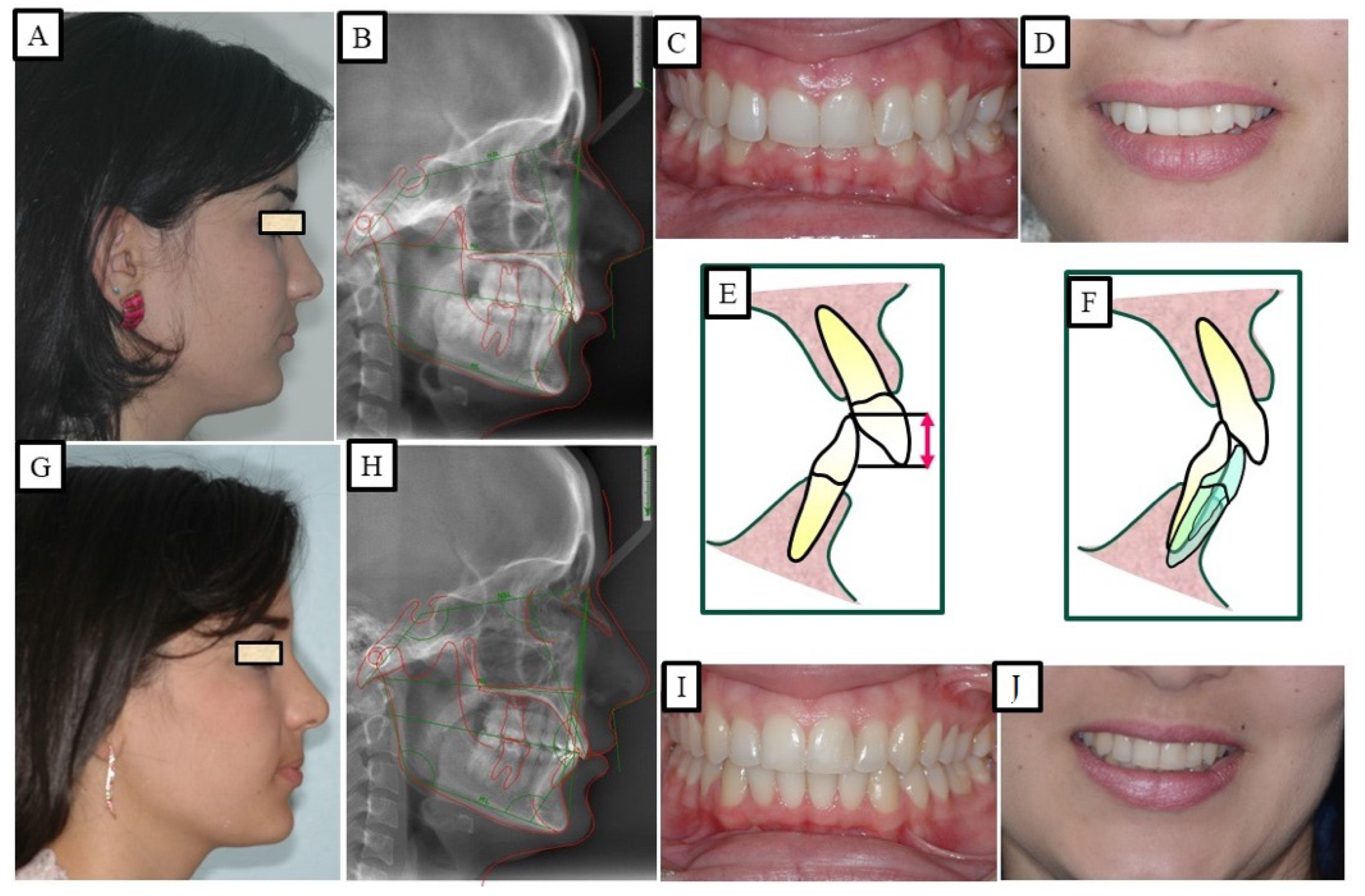
2.5. Soft Tissue Evaluation
2.6. Clinical Treatment of Deep Bite
2.7. Utilizing Mouse Models and Collaborative Cross Populations to Explore Phenotypes of Deep Bite
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Achmad, H.; Noor Armedina, R.; Timokhina, T.; Goncharov, V.V.; Sitanaya, R.; Riyanti, E. Literature Review: Problems of Dental and Oral Health Primary School Children. Indian J. Forensic Med. Toxicol. 2021, 15, 4146–4162. [Google Scholar] [CrossRef]
- Neela, P.K.; Atteeri, A.; Mamillapalli, P.K.; Sesham, V.M.; Keesara, S.; Chandra, J.; Monica, U.; Mohan, V. Genetics of Dentofacial and Orthodontic Abnormalities. Glob. Med. Genet. 2020, 7, 95. [Google Scholar] [CrossRef]
- Moreno Uribe, L.M.; Miller, S.F. Genetics of the Dentofacial Variation in Human Malocclusion. Orthod. Craniofac. Res. 2015, 18, 91. [Google Scholar] [CrossRef] [PubMed]
- Zebrick, B.; Teeramongkolgul, T.; Nicot, R.; Horton, M.J.; Raoul, G.; Ferri, J.; Vieira, A.R.; Sciote, J.J. ACTN3 R577X Genotypes Associate with Class II and Deepbite Malocclusions. Am. J. Orthod. Dentofacial. Orthop. 2014, 146, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.; Vivek, R.; Srivastava, A.; Singh, A.; Srivastava, S.; Chaturvedi, T.P. Van Der Woude Syndrome Associated with Hypodontia: A Rare Clinical Entity. Case Rep. Dent. 2012, 2012, 1–3. [Google Scholar] [CrossRef]
- Doraczynska-Kowalik, A.; Nelke, K.H.; Pawlak, W.; Sasiadek, M.M.; Gerber, H. Genetic Factors Involved in Mandibular Prognathism. J. Craniofacial Surg. 2017, 28, e422–e431. [Google Scholar] [CrossRef] [PubMed]
- Lone, I.M.; Midlej, K.; Ben Nun, N.; Iraqi, F.A. Intestinal Cancer Development in Response to Oral Infection with High-Fat Diet-Induced Type 2 Diabetes (T2D) in Collaborative Cross Mice under Different Host Genetic Background Effects. Mamm. Genome 2023, 34, 56–75. [Google Scholar] [CrossRef] [PubMed]
- Lone, I.M.; Iraqi, F.A. Genetics of Murine Type 2 Diabetes and Comorbidities. Mamm. Genome 2022, 33, 421–436. [Google Scholar] [CrossRef] [PubMed]
- Lone, I.M.; Ben Nun, N.; Ghnaim, A.; Schaefer, A.S.; Houri-Haddad, Y.; Iraqi, F.A. High-Fat Diet and Oral Infection Induced Type 2 Diabetes and Obesity Development under Different Genetic Backgrounds. Anim. Model. Exp. Med. 2023, 6, 131–145. [Google Scholar] [CrossRef]
- Ghnaim, A.; Lone, I.M.; Ben Nun, N.; Iraqi, F.A. Unraveling the Host Genetic Background Effect on Internal Organ Weight Influenced by Obesity and Diabetes Using Collaborative Cross Mice. Int. J. Mol. Sci. 2023, 24, 8201. [Google Scholar] [CrossRef]
- Huh, A.; Horton, M.J.; Cuenco, K.T.; Raoul, G.; Rowlerson, A.M.; Ferri, J.; Sciote, J.J. Epigenetic Influence of KAT6B and HDAC4 in the Development of Skeletal Malocclusion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 568–576. [Google Scholar] [CrossRef]
- Kundakovic, M.; Jaric, I. The Epigenetic Link between Prenatal Adverse Environments and Neurodevelopmental Disorders. Genes 2017, 8, 104. [Google Scholar] [CrossRef]
- Bardideh, E.; Tamizi, G.; Shafaee, H.; Rangrazi, A.; Ghorbani, M.; Kerayechian, N. The Effects of Intrusion of Anterior Teeth by Skeletal Anchorage in Deep Bite Patients; A Systematic Review and Meta-Analysis. Biomimetics 2023, 8, 101. [Google Scholar] [CrossRef] [PubMed]
- Fattahi, H.; Pakshir, H.; Afzali Baghdadabadi, N.; Shahian Jahromi, S.; Afzali Baghdadabadi, N. Skeletal and Dentoalveolar Features in Patients with Deep Overbite Malocclusion. J. Dent. 2014, 11, 629. [Google Scholar]
- Nielsen, I.L. Vertical Malocclusions: Etiology, Development, Diagnosis and Some Aspects of Treatment. Angle Orthod. 1991, 61, 247–260. [Google Scholar] [PubMed]
- Tausche, E.; Luck, O.; Harzer, W. Prevalence of Malocclusions in the Early Mixed Dentition and Orthodontic Treatment Need. Eur. J. Orthod. 2004, 26, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Proffit, W.R.; Fields, H.W.; Larson, B.; Sarver, D.M. Contemporary Orthodontics-e-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Lux, C.J.; Dücker, B.; Pritsch, M.; Komposch, G.; Niekusch, U. Occlusal Status and Prevalence of Occlusal Malocclusion Traits among 9-Year-Old Schoolchildren. Eur. J. Orthod. 2009, 31, 294–299. [Google Scholar] [CrossRef]
- Ota, K.; Arai, K. Prevalence and Patterns of Tooth Agenesis in Angle Class II Division 2 Malocclusion in Japan. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 123–129. [Google Scholar] [CrossRef]
- Upadhyay, M.; Nagaraj, K.; Yadav, S.; Saxena, R. Mini-Implants for En Masse Intrusion of Maxillary Anterior Teeth in a Severe Class II Division 2 Malocclusion. J. Orthod. 2008, 35, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.J.; Bates, S.B.; Ehlert, A.A.; Whiting, D.P.; Chen, S.S.H.; Bollen, A.M. Stability of Deep-Bite Correction: A Systematic Review. J. World Fed. Orthod. 2012, 1, e89–e96. [Google Scholar] [CrossRef] [PubMed]
- Varlik, S.K.; Alpakan, Ö.O.; Türköz, Ç. Deepbite Correction with Incisor Intrusion in Adults: A Long-Term Cephalometric Study. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Mapare, S.; Mundada, R.; Karra, A.; Agrawal, S.; Mahajan, S.; Tadawalkar, A. Extraction or Nonextraction in Orthodontic Cases: A Review. J. Pharm. Bioallied Sci. 2021, 13, 2–5. [Google Scholar]
- Vinnakota, D.N.; Kanneganti, K.C.; Pulagam, M.; Karnati, P.K.R. Freeway Space Determination Using Lateral Profile Photographs: A Pilot Study. J. Indian Prosthodont. Soc. 2016, 16, 242–247. [Google Scholar] [CrossRef]
- Mahn, E.; Sampaio, C.S.; Pereira da Silva, B.; Stanley, K.; Valdés, A.M.; Gutierrez, J.; Coachman, C. Comparing the Use of Static versus Dynamic Images to Evaluate a Smile. J. Prosthet. Dent. 2020, 123, 739–746. [Google Scholar] [CrossRef]
- Mazurova, K.; Kopp, J.B.; Renkema, A.M.; Pandis, N.; Katsaros, C.; Fudalej, P.S. Gingival Recession in Mandibular Incisors and Symphysis Morphology-a Retrospective Cohort Study. Eur. J. Orthod. 2018, 40, 185–192. [Google Scholar] [CrossRef]
- Cakan, D.G.; Ulkur, F.; Taner, T.U. The Genetic Basis of Facial Skeletal Characteristics and Its Relation with Orthodontics. Eur. J. Dent. 2012, 6, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Bc, A. Clinical Overview of Deep Bite Management. Int. J. Contemp. Dent. 2010, 1, 30. [Google Scholar]
- Lone, I.M.; Zohud, O.; Nashef, A.; Kirschneck, C.; Proff, P.; Watted, N.; Iraqi, F.A. Dissecting the Complexity of Skeletal-Malocclusion-Associated Phenotypes: Mouse for the Rescue. Int. J. Mol. Sci. 2023, 24, 2570. [Google Scholar] [CrossRef] [PubMed]
- Carver, E.A.; Oram, K.F.; Gridley, T. Craniosynostosis in Twist Heterozygous Mice: A Model for Saethre-Chotzen Syndrome. Anat. Rec. 2002, 268, 90–92. [Google Scholar] [CrossRef]
- Zohud, O.; Lone, I.M.; Midlej, K.; Obaida, A.; Masarwa, S.; Schröder, A.; Küchler, E.C.; Nashef, A.; Kassem, F.; Reiser, V.; et al. Towards Genetic Dissection of Skeletal Class III Malocclusion: A Review of Genetic Variations Underlying the Phenotype in Humans and Future Directions. J. Clin. Med. 2023, 12, 3212. [Google Scholar] [CrossRef] [PubMed]
- Iraqi, F.A.; Mahajne, M.; Salaymah, Y.; Sandovski, H.; Tayem, H.; Vered, K.; Balmer, L.; Hall, M.; Manship, G.; Morahan, G.; et al. The Genome Architecture of the Collaborative Cross Mouse Genetic Reference Population. Genetics 2012, 190, 389–401. [Google Scholar] [CrossRef]
- Levy, R.; Mott, R.F.; Iraqi, F.A.; Gabet, Y. Collaborative Cross Mice in a Genetic Association Study Reveal New Candidate Genes for Bone Microarchitecture. BMC Genom. 2015, 16, 1013. [Google Scholar] [CrossRef]
- Lone, I.M.; Zohud, O.; Midlej, K.; Proff, P.; Watted, N.; Iraqi, F.A. Skeletal Class II Malocclusion: From Clinical Treatment Strategies to the Roadmap in Identifying the Genetic Bases of Development in Humans with the Support of the Collaborative Cross Mouse Population. J. Clin. Med. 2023, 12, 5148. [Google Scholar] [CrossRef] [PubMed]
- Dorman, A.; Baer, D.; Tomlinson, I.; Mott, R.; Iraqi, F.A. Genetic Analysis of Intestinal Polyp Development in Collaborative Cross Mice Carrying the Apc Min/+ Mutation. BMC Genet. 2016, 17, 1–11. [Google Scholar]
- Iraqi, F.A.; Churchill, G.; Mott, R. The Collaborative Cross, Developing a Resource for Mammalian Systems Genetics: A Status Report of the Wellcome Trust Cohort. Mamm. Genome 2008, 19, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Yehia, R.; Lone, I.M.; Yehia, I.; Iraqi, F.A. Studying the Pharmagenomic Effect of Portulaca Oleracea Extract on Anti-Diabetic Therapy Using the Collaborative Cross Mice. Phytomedicine Plus 2023, 3, 100394. [Google Scholar] [CrossRef]
- Sreedhar, C.; Baratam, S. Deep Overbite—A Review (Deep Bite, Deep Overbite, Excessive Overbite). Ann. Essences Dent. 2009, I, 8–25. [Google Scholar] [CrossRef]
- Beckmann, S.H.; Kuitert, R.B.; Prahl-Andersen, B.; Segner, D.; The, R.P.; Tuinzing, D.B. Alveolar and Skeletal Dimensions Associated with Lower Face Height. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 498–506. [Google Scholar] [CrossRef]
- Baydaş, B.; Yavuz, I.; Atasaral, N.; Ceylan, I.; Dağsuyu, I.M. Investigation of the Changes in the Positions of Upper and Lower Incisors, Overjet, Overbite, and Irregularity Index in Subjects with Different Depths of Curve of Spee. Angle Orthod. 2004, 74, 349–355. [Google Scholar]
- Ceylan, I.; Eröz, Ü.B. The Effects of Overbite on the Maxillary and Mandibular Morphology. Angle Orthod. 2001, 71, 110–115. [Google Scholar]
- Al-Zubaidi, S.; Obaidi, H. The Variation of the Lower Anterior Facial Height and Its Component Parameters among the Three over Bite Relationships (Cephalometric Study). Al-Rafidain Dent. J. 2006, 6, 106–113. [Google Scholar] [CrossRef]
- El-Dawlatly, M.M.; Fayed, M.M.S.; Mostafa, Y.A. Deep Overbite Malocclusion: Analysis of the Underlying Components. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Naumann, S.A.; Behrents, R.G.; Buschang, P.H. Vertical Components of Overbite Change: A Mathematical Model. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Betzenberger, D.; Ruf, S.; Pancherz, H. The Compensatory Mechanism in High-Angle Malocclusions: A Comparison of Subjects in the Mixed and Permanent Dentition. Angle Orthod. 1999, 69, 27–32. [Google Scholar] [PubMed]
- Silness, J.; Johannessen, G.; Røynstrand, T. Longitudinal Relationship between Incisal Occlusion and Incisal Tooth Wear. Acta Odontol. Scand. 1993, 51, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Danz, J.C.; Greuter, C.; Sifakakis, L.; Fayed, M.; Pandis, N.; Katsaros, C. Stability and Relapse after Orthodontic Treatment of Deep Bite Cases—A Long-Term Follow-up Study. Eur. J. Orthod. 2014, 36, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, J.L.; Proffit, W.R. Soft Tissue Limitations in Orthodontics: Treatment Planning Guidelines. Angle Orthod. 1997, 67, 327–336. [Google Scholar]
- Al Yami, E.A.; Kuijpers-Jagtman, A.M.; Van’t Hof, M.A. Orthodontic Treatment Need Prior to Treatment and 5 Years Postretention. Community Dent. Oral Epidemiol. 1998, 26, 421–427. [Google Scholar] [CrossRef]
- Piancino, M.G.; Tortarolo, A.; Di Benedetto, L.; Crincoli, V.; Falla, D. Chewing Patterns and Muscular Activation in Deep Bite Malocclusion. J. Clin. Med. 2022, 11, 1702. [Google Scholar] [CrossRef]
- Lapatki, B.G.; Klatt, A.; Schulte-Mönting, J.; Stein, S.; Jonas, I.E. A Retrospective Cephalometric Study for the Quantitative Assessment of Relapse Factors in Cover-Bite Treatment. J. Orofac. Orthop./Fortschritte Der Kieferorthopadie 2004, 65, 475–488. [Google Scholar] [CrossRef]
- Bernstein, R.L.; Preston, C.B.; Lampasso, J. Leveling the Curve of Spee with a Continuous Archwire Technique: A Long Term Cephalometric Study. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 363–371. [Google Scholar] [CrossRef]
- Canut, J.A.; Arias, S. A Long-Term Evaluation of Treated Class II Division 2 Malocclusions: A Retrospective Study Model Analysis. Eur. J. Orthod. 1999, 21, 377–386. [Google Scholar] [CrossRef]
- Zaher, A.R.; Bishara, S.E.; Jakobsen, J.R. Posttreatment Changes in Different Facial Types. Angle Orthod. 1994, 64, 425–436. [Google Scholar] [PubMed]
- Baccetti, T.; Franchi, L.; McNamara, J.A. Longitudinal Growth Changes in Subjects with Deepbite. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Sciote, J.J.; Horton, M.J.; Rowlerson, A.M.; Ferri, J.; Close, J.M.; Raoul, G. Human Masseter Muscle Fiber Type Properties, Skeletal Malocclusions, and Muscle Growth Factor Expression. J. Oral Maxillofac. Surg. 2012, 70, 440–448. [Google Scholar] [CrossRef]
- Lowe, A.A.; Santamaria, J.D.; Fleetham, J.A.; Price, C. Facial Morphology and Obstructive Sleep Apnea. Am. J. Orthod. Dentofac. Orthop. 1986, 90, 484–491. [Google Scholar] [CrossRef]
- Preston, C.B.; Maggard, M.B.; Lampasso, J.; Chalabi, O. Long-Term Effectiveness of the Continuous and the Sectional Archwire Techniques in Leveling the Curve of Spee. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 550–555. [Google Scholar] [CrossRef]
- Sonnesen, L.; Svensson, P. Temporomandibular Disorders and Psychological Status in Adult Patients with a Deep Bite. Eur. J. Orthod. 2008, 30, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, Y.; Horiuchi, M.; Soma, K. Treatment of Severe Class II Division 1 Deep Overbite Malocclusion without Extractions in an Adult. Am. J. Orthod. Dentofac. Orthop. 2008, 133, S121–S129. [Google Scholar] [CrossRef]
- Daokar, S.; Agrawal, G. Deep Bite Its Etiology, Diagnosis and Management: A Review. J. Orthod. Endod. 2016, 2, 4. [Google Scholar] [CrossRef]
- Mew, J.R.C. The Postural Basis of Malocclusion: A Philosophical Overview. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 729–738. [Google Scholar] [CrossRef]
- Masella, R.S.; Meister, M. Current Concepts in the Biology of Orthodontic Tooth Movement. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Cheong, Y.W.; Lo, L.J. Facial Asymmetry: Etiology, Evaluation, and Management. Chang. Gung Med. J. 2011, 34, 341–351. [Google Scholar] [PubMed]
- Pollard, D.; Akyalcin, S.; Wiltshire, W.A.; Rody, W.J. Relapse of Orthodontically Corrected Deepbites in Accordance with Growth Pattern. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Kilic, N.; Oktay, H.; Ersoz, M. Effects of Force Magnitude on Relapse: An Experimental Study in Rabbits. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Hans, M.G.; Kishiyama, C.; Parker, S.H.; Wolf, G.R.; Noachtar, R. Cephalometric Evaluation of Two Treatment Strategies for Deep Overbite Correction. Angle Orthod. 1994, 64, 265. [Google Scholar] [PubMed]
- Ng, J.; Major, P.W.; Heo, G.; Flores-Mir, C. True Incisor Intrusion Attained during Orthodontic Treatment: A Systematic Review and Meta-Analysis. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 212–219. [Google Scholar] [CrossRef]
- Millett, D.T.; Cunningham, S.J.; O’Brien, K.D.; Benson, P.E.; de Oliveira, C.M. Orthodontic Treatment for Deep Bite and Retroclined Upper Front Teeth in Children. Cochrane Database Syst. Rev. 2018, 2018, CD005972. [Google Scholar] [CrossRef]















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watted, N.; Lone, I.M.; Zohud, O.; Midlej, K.; Proff, P.; Iraqi, F.A. Comprehensive Deciphering the Complexity of the Deep Bite: Insight from Animal Model to Human Subjects. J. Pers. Med. 2023, 13, 1472. https://doi.org/10.3390/jpm13101472
Watted N, Lone IM, Zohud O, Midlej K, Proff P, Iraqi FA. Comprehensive Deciphering the Complexity of the Deep Bite: Insight from Animal Model to Human Subjects. Journal of Personalized Medicine. 2023; 13(10):1472. https://doi.org/10.3390/jpm13101472
Chicago/Turabian StyleWatted, Nezar, Iqbal M. Lone, Osayd Zohud, Kareem Midlej, Peter Proff, and Fuad A. Iraqi. 2023. "Comprehensive Deciphering the Complexity of the Deep Bite: Insight from Animal Model to Human Subjects" Journal of Personalized Medicine 13, no. 10: 1472. https://doi.org/10.3390/jpm13101472