
Pulmonary Artery Embolization in the Management of Hemoptysis Related to Lung Tumors
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
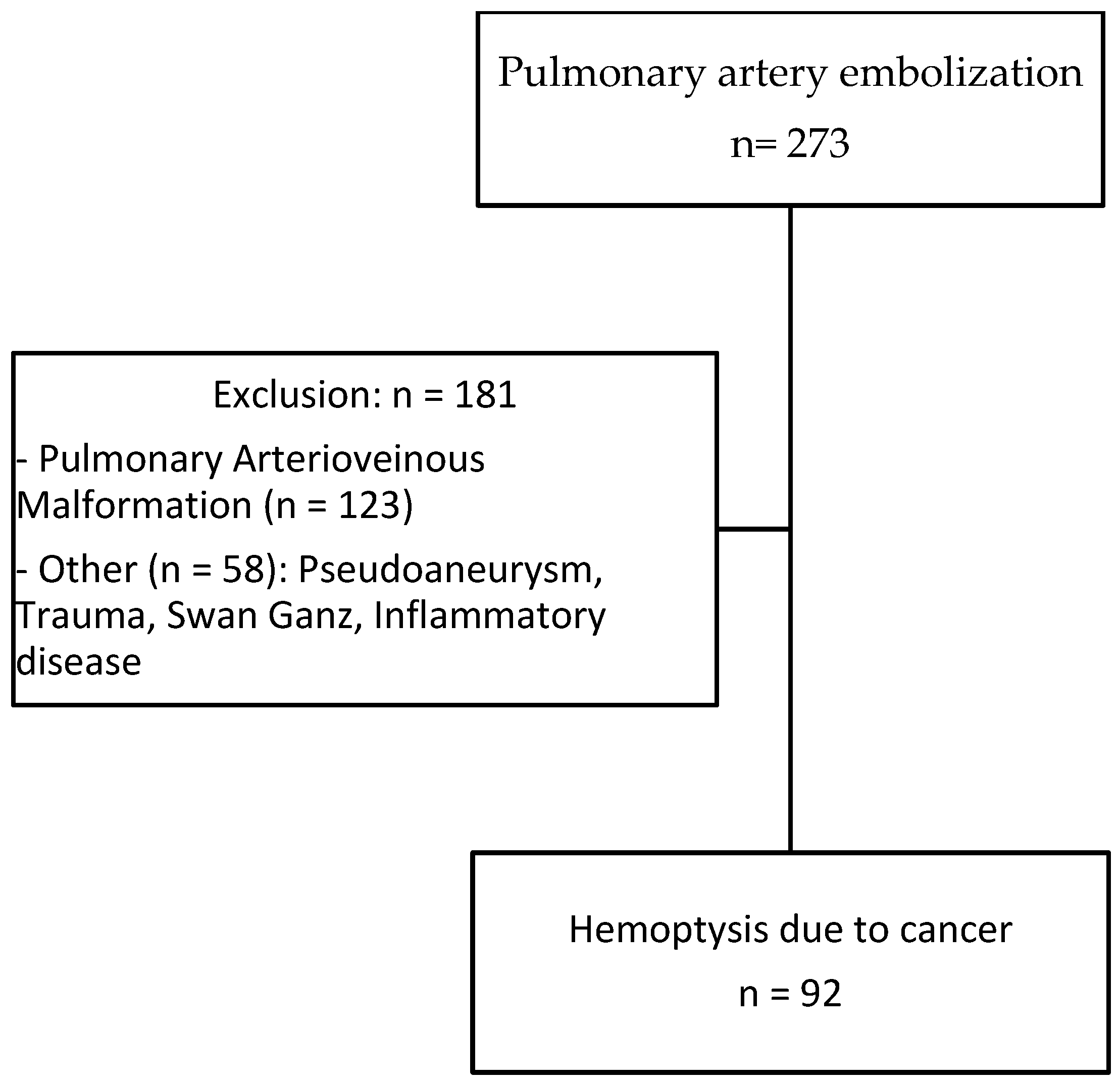
2.1. Patients
2.2. Endovascular Management
2.3. Analysis of the Outcome
3. Results
3.1. Patient Population and Analysis of Imaging
3.2. Embolization Procedure
3.3. Clinical Results and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdulmalak, C.; Cottenet, J.; Beltramo, G.; Georges, M.; Camus, P.; Bonniaud, P.; Quantin, C. Haemoptysis in Adults: A 5-Year Study Using the French Nationwide Hospital Administrative Database. Eur. Respir. J. 2015, 46, 503–511. [Google Scholar] [CrossRef]
- Chun, J.Y.; Morgan, R.; Belli, A.M. Radiological Management of Hemoptysis: A Comprehensive Review of Diagnostic Imaging and Bronchial Arterial Embolization. Cardiovasc. Interv. Radiol. 2010, 33, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Parrot, A.; Nedelcu, C.; Fartoukh, M.; Marsault, C.; Carette, M.F. Severe Hemoptysis of Pulmonary Arterial Origin: Signs and Role of Multidetector Row CT Angiography. Chest 2008, 133, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Fartoukh, M.; Khoshnood, B.; Parrot, A.; Khalil, A.; Carette, M.F.; Stoclin, A.; Mayaud, C.; Cadranel, J.; Ancel, P.Y. Early Prediction of In-Hospital Mortality of Patients with Hemoptysis: An Approach to Defining Severe Hemoptysis. Respiration 2012, 83, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Pelage, J.P.; el Hajjam, M.; Lagrange, C.; Chinet, T.; Vieillard-Baron, A.; Chagnon, S.; Lacombe, P. Pulmonary Artery Interventions: An Overview. Radiographics 2005, 25, 1653–1667. [Google Scholar] [CrossRef] [PubMed]
- Piracha, S.; Mahmood, A.; Qayyum, N.; Ganaie, M.B. Massive Haemoptysis Secondary to Mycotic Pulmonary Artery Aneurysm in Subacute Invasive Aspergillosis. BMJ Case Rep. 2018, 2018, bcr2017223088. [Google Scholar] [CrossRef] [PubMed]
- Giraldo-Montoya, Á.M.; Rodríguez-Morales, A.J.; Hernández-Hurtado, J.D.; López-Salazar, Á.; Lagos-Grisales, G.J.; Ruiz-Granada, V.H. Rasmussen Aneurysm: A Rare but Not Gone Complication of Tuberculosis. Int. J. Infect. Dis. 2018, 69, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Tsukada, J.; Hasegawa, I.; Torikai, H.; Sayama, K.; Jinzaki, M.; Narimatsu, Y. Interventional Therapeutic Strategy for Hemoptysis Originating from Infectious Pulmonary Artery Pseudoaneurysms. J. Vasc. Interv. Radiol. 2015, 26, 1046–1051.e1. [Google Scholar] [CrossRef] [PubMed]
- Sbano, H.; Mitchell, A.W.; Ind, P.W.; Jackson, J.E. Peripheral Pulmonary Artery Pseudoaneurysms and Massive Hemoptysis. Am. J. Roentgenol. 2005, 184, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Ference, B.A.; Shannon, T.M.; White, R.I.; Zawin, M.; Burdge, C.M. Life-Threatening Pulmonary Hemorrhage with Pulmonary Arteriovenous Malformations and Hereditary Hemorrhagic Telangiectasia. Chest 1994, 106, 1387–1390. [Google Scholar] [CrossRef] [PubMed]
- Rudziński, P.N.; Henzel, J.; Dzielińska, Z.; Lubiszewska, B.M.; Michałowska, I.; Szymański, P.; Pracoń, R.; Hryniewiecki, T.; Demkow, M. Pulmonary Artery Rupture as a Complication of Swan-Ganz Catheter Application. Diagnosis and Endovascular Treatment: A Single Centre’s Experience. Postep. W Kardiol. Interwencyjnej 2016, 12, 135–139. [Google Scholar] [CrossRef]
- Marcelin, C.; Soussan, J.; Desmots, F.; Gaubert, J.Y.; Vidal, V.; Bartoli, J.M.; Izaaryene, J. Outcomes of Pulmonary Artery Embolization and Stent Graft Placement for the Treatment of Hemoptysis Caused by Lung Tumors. J. Vasc. Interv. Radiol. 2018, 29, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Sacks, D.; McClenny, T.E.; Cardella, J.F.; Lewis, C.A. Society of Interventional Radiology Clinical Practice Guidelines. J. Vasc. Interv. Radiol. 2003, 14 Pt 2, S199–S202. [Google Scholar] [CrossRef] [PubMed]
- Bruzzi, J.F.; Rémy-Jardin, M.; Delhaye, D.; Teisseire, A.; Khalil, C.; Rémy, J. Multi-Detector Row CT of Hemoptysis. Radiographics 2006, 26, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Fedida, B.; Parrot, A.; Haddad, S.; Fartoukh, M.; Carette, M.F. Severe Hemoptysis: From Diagnosis to Embolization. Diagn. Interv. Imaging 2015, 96, 775–788. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Gilman, M.D.; Humphrey, K.L.; Salazar, G.M.; Sharma, A.; Muniappan, A.; Shepard, J.A.O.; Wu, C.C. Pulmonary Artery Pseudoaneurysms: Clinical Features and CT Findings. Am. J. Roentgenol. 2017, 208, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Kim, Y.I.; Kim, H.Y.; Zo, J.I.; Lee, J.H.; Lee, J.S. Bronchial Artery and Systemic Artery Embolization in the Management of Primary Lung Cancer Patients with Hemoptysis. Cardiovasc. Interv. Radiol. 2007, 30, 638–643. [Google Scholar] [CrossRef]
- Garcia-Olivé, I.; Sanz-Santos, J.; Centeno, C.; Andreo, F.; Muñoz-Ferrer, A.; Serra, P.; Sampere, J.; Michavila, J.M.; Muchart, J.; Manzano, J.R. Results of Bronchial Artery Embolization for the Treatment of Hemoptysis Caused by Neoplasm. J. Vasc. Interv. Radiol. 2014, 25, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.R.; Ensor, J.E.; Gupta, S.; Hicks, M.E.; Tam, A.L. Bronchial Artery Embolization for the Management of Hemoptysis in Oncology Patients: Utility and Prognostic Factors. J. Vasc. Interv. Radiol. 2009, 20, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Shin, T.B.; Yoon, S.K.; Lee, K.N.; Choi, J.S.; Kim, Y.H.; Sung, C.G.; Kim, Y.J.; Kim, C.W. The Role of Pulmonary CT Angiography and Selective Pulmonary Angiography in Endovascular Management of Pulmonary Artery Pseudoaneurysms Associated with Infectious Lung Diseases. J. Vasc. Interv. Radiol. 2007, 18, 882–887. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 92 | |
|---|---|
| Gender, male/female n | 70/22 |
| Mean age (years) | 63.1 ± 9.9 (med 63.0, min–max 37.0–85.9) |
| Histology, n (%) (N = 86) | |
| Epidermoid | 50 (54) |
| Adenocarcinoma | 21 (22) |
| Lymphoma | 2 (2) |
| Secondary | 6 (7) |
| Undetermined | 6 (7) |
| Other | 7 (8) |
| Staging, n (%) (N = 69) | |
| I | 0 (0) |
| II | 2 (3) |
| III | 22 (32) |
| IV | 45 (65) |
| Previous treatments, n (%) (N = 92) | |
| Radiation therapy | 11 (12) |
| Chemotherapy | 51 (55) |
| Immunotherapy | 5 (5) |
| Surgical resection | 6 (6) |
| Altered coagulation n (%) (N = 92) | |
| Anticoagulation therapy | 7 (8) |
| Antiplatelet therapy | 9 (10) |
| Coagulation disorders | 2 (2) |
| Volume of hemoptysis, n (%) (N = 92) | |
| Massive | 34 (37) |
| Medium | 36 (39) |
| Minimal | 22 (24) |
| Hemodynamic status, n (%) (N = 92) | |
| Stable | 68 (74) |
| Instability | 24 (26) |
| N = 92 | |
|---|---|
| Lung tumor | |
| Longest diameter (mean SD) mm (73) | 75.2 ± 26.5 (70.0, min–max 30.0–162.0) |
| Tumor necrosis N (%) (N = 87) | 63 (72) |
| Tumor cavitation N (%) (N = 86) | 41 (47) |
| Central location N (%) (N = 91) | 73 (80) |
| Pulmonary artery appearance N (%) (N = 86) | |
| Arterial wall irregularity | 39 (45) |
| Tumoral occlusion | 24 (28) |
| Pseudoaneurysm | 18 (21) |
| Normal | 5 (6) |
| Parenchymal abnormalities N (%) (N = 37) | |
| Ground-glass attenuation | 19 (51) |
| Alveolar consolidation | 2 (5) |
| Pulmonary artery: level of embolization N (%) (N = 91) | |
| Proximal (main arteries) | 31 (34) |
| Lobar | 34 (37) |
| Segmental or more distal | 26 (29) |
| Primary embolization agent N (%) (N = 90) | |
| Coils | 35 (39) |
| Covered stent | 29 (32) |
| Acrylic glue | 13 (14) |
| Vascular plug | 12 (13) |
| Gelatin sponge | 1 (2) |
| No Recurrence (N = 43) | Recurrence (n = 37) | HR (95%IC) | p-Value | |
|---|---|---|---|---|
| Age | 62.9 ± 10 | 62.9 ± 9.7 | 1 (0.97–1.03) | 0.999 |
| Sex (%) | ||||
| Female | 13 (30.2) | 8 (21.6) | ||
| Male | 30 (69.8) | 29 (78.4) | 1.171 (0.53–2.6) | 0.697 |
| Histology | ||||
| Primary | 36 (92.3) | 32 (91.4) | ||
| Secondary | 3 (7.7) | 3 (8.6) | 0.7423 (0.22–2.45) | 0.625 |
| Histology | ||||
| Adenocarcinoma | 8 (18.6) | 8 (21.6) | ||
| Other | 13 (30.2) | 8 (21.6) | 0.8697 (0.32–2.35) | 0.783 |
| Epidermoid | 22 (51.2) | 21(56.8) | 0.7534 (0.32–1.78) | 0.519 |
| Volume of hemoptysis | ||||
| Minimum | 9 (20.9) | 9 (21.6) | ||
| Massive | 16 (37.2) | 17 (45.9) | 0.8697 (0.32–2.35) | 0.783 |
| Medium | 18 (41.9) | 12 (32.4) | 0.7534 (0.32–1.78) | 0.519 |
| Hemodynamic condition | ||||
| Instability | 12 (27.9) | 10 (27.0) | ||
| Stability | 31 (72.1) | 27 (73.0) | 0.6006 (0.28–1.28) | 0.189 |
| Altered coagulation | ||||
| No risk factor | 32 (74.4) | 31 (83.8) | ||
| Medication or hemostatic disorders | 11 (25.6) | 6 (16.2) | 0.7475 (0.31–1.8) | 0.518 |
| Tumor cavitation | ||||
| Absence | 22 (55.0) | 15 (42.9) | ||
| Presence | 18 (45.0) | 20 (57.1) | 2.7993 (1.37–5.71) | 0.004 |
| Tumor necrosis | ||||
| Absence | 12 (29.3) | 11 (31.4) | ||
| Presence | 29 (70.7) | 24 (68.6) | 2.2617 (1.03–4.96) | 0.0416 |
| Pulmonary artery | ||||
| Normal | 4 (10) | 1 (2.9) | ||
| Irregularity | 19 (47.5) | 16 (45.7) | 2.7790 (0.35–21.20) | 0.324 |
| Occlusion | 7 (17.5) | 12 (34.3) | 2.3885 (0.30–18.70) | 0.407 |
| Pseudoaneurysm | 10 (25.0) | 6 (17.1) | 2.8484 (0.34–23.87) | 0.335 |
| Tumor size | 69.8 ± 24.8 | 82.0 ± 29.7 | 1.019584 (1.00–1.03) | 0.00351 |
| Proximal embolization | ||||
| No | 15 (55.6) | 8 (32.0) | ||
| Yes | 12 (44.4) | 17 (68.0) | 2.1525 (0.89–5.21) | 0.0891 |
| Embolization agents | ||||
| Coils | 18 (43.9) | 14 (37.8) | ||
| Glue | 10 (24.4) | 3 (8.1) | 1.32491 (0.21–2.65) | 0.6605 |
| Gelatin sponge | 0 (0.0) | 1 (2.7) | 0.08394 (1.38–102.82) | 0.0243 |
| Plug | 5 (12.2) | 5 (13.5) | 1.00006 (0.36–2.79) | 0.9999 |
| Covered stent | 8 (19.5) | 14 (37.8) | 0.80773 (0.57–2.69) | 0.5902 |
| Immediate bleeding cessation | ||||
| No | 5 (11.6) | 3 (8.1) | ||
| Yes | 38 (88.44) | 34 (91.9) | 0.7617 (0.23–2.51) | 0.655 |
| HR | HR IC: Lower 0.95 | HR IC: Upper 0.95 | p-Value | |
|---|---|---|---|---|
| Age | 1.0189 | 0.9580 | 1.084 | 0.5515 |
| Sex | ||||
| Female | ||||
| Male | 5.2860 | 0.8681 | 32.188 | 0.0708 |
| Histology | ||||
| Primary | ||||
| Secondary | 0.9551 | 0.0182 | 50.241 | 0.9819 |
| Histology | ||||
| Adenocarcinoma | ||||
| Other | 0.5557 | 0.0460 | 6.708 | 0.6439 |
| Epidermoid | 0.1385 | 0.0242 | 0.793 | 0.0264 |
| Volume of hemoptysis | ||||
| Minimal | ||||
| Massive | 2.0534 | 0.4870 | 0.1069 | 0.6333 |
| Medium | 4.5907 | 0.2178 | 0.2841 | 0.2831 |
| Hemodynamic Condition | ||||
| Instability | ||||
| Stability | 0.4662 | 0.0814 | 2.671 | 0.3915 |
| Altered Coagulation | ||||
| No risk factor | ||||
| Medication or hemostatic disorders | 0.4791 | 0.1068 | 2.150 | 0.3368 |
| Tumor Cavitation | ||||
| Absence | ||||
| Presence | 6.5971 | 1.4792 | 29.422 | 0.0134 |
| Tumor Necrosis | ||||
| Absence | ||||
| Presence | 1.1055 | 0.1844 | 6.627 | 0.9126 |
| Pulmonary Artery | ||||
| Normal | ||||
| Irregularity | 13.7288 | 0.7637 | 246.792 | 0.0756 |
| Occlusion | 17.2756 | 0.6156 | 484.781 | 0.0940 |
| Pseudoaneurysm | 85.9899 | 2.9129 | 2538.444 | 0.0099 |
| Tumor size | 1.0213 | 0.9875 | 1.056 | 0.2201 |
| Embolization Agents | ||||
| Coils | ||||
| Glue | 2.4921 | 0.3385 | 18.346 | 0.3700 |
| Gelatin sponge | 33.3437 | 1.0428 | 1066.195 | 0.0473 |
| Plug | 0.6444 | 0.0719 | 5.774 | 0.6945 |
| Covered stent | 5.7254 | 1.2774 | 25.662 | 0.0226 |
| Immediate Bleeding Cessation | ||||
| No | ||||
| Yes | 1.7720 | 0.1554 | 20.202 | 0.6450 |
| Parameters | p-Value |
|---|---|
| Epidermoid vs. adenocarcinoma | 0.33 |
| Chemotherapy vs. no chemotherapy | 0.63 |
| Heavy smoker (>40 pack years) vs. lighter smoker | 0.728 |
| Hilar tumor | 0.877 |
| Tumor > 70 mm vs. tumor < 70 mm | 0.187 |
| Tumor cavitation | 0.006 |
| Tumor necrosis | 0.011 |
| Normal vs. abnormal pulmonary artery | 0.19 |
| Pulmonary artery abnormality | 0.055 |
| Quantification of hemoptysis | 0.006 |
| Recurrence of hemoptysis | 0.31 |
| Level of embolization | 0.202 |
| Proximal vs. distal embolization | 0.249 |
| Simultaneous bronchial artery embolization | 0.04 |
| Embolization material | 0.368 |
| Coils vs. stent | 0.309 |
| Coils vs. acrylic glue | 0.17 |
| Stent vs. no stent | 0.627 |
| Alive (n = 14) | Dead (n = 78) | HR (95% IC) | p-Value | |
|---|---|---|---|---|
| Age | 67.9 (8.1) | 62.3 (10.0) | 0.991138 (0.9700972–1.012636) | 0.416 |
| Sex (%) | ||||
| Female | 5 (35.7) | 17 (21.8) | ||
| Male | 9 (64.3) | 61 (78.2) | 1.07432 (0.626638–1.841834) | 0.794 |
| Histology | ||||
| Primary | 13 (92.9) | 67 (93.1) | ||
| Secondary | 1 (7.1) | 5 (6.9) | 0.6381 (0.2564672–1.587552) | 0.334 |
| Histology | ||||
| Adenocarcinoma | 2(14.3) | 19 (24.4) | ||
| Other | 2 (14.0) | 19 (24.4) | 1.004453 (0.5257198–1.919131) | 0.989 |
| Epidermoid | 10 (71.4) | 40 (51.3) | 0.727641 (0.4135167–1.280387) | 0.2270 |
| Volume of hemoptysis | ||||
| Minimum | 6 (42.9) | 16 (20.5) | ||
| Massive | 5 (35.7) | 29 (37.2) | 2.1008 (1.134935–3.888751) | 0.0181 |
| Medium | 3 (21.4) | 33 (42.3) | 2.0151 (1.105948–3.671448) | 0.0221 |
| Hemodynamic condition | ||||
| Instability | 2 (14.3) | 22 (28.2) | ||
| Stability | 12 (85.7) | 56 (71.8) | 0.5984 (0.360253–0.9938743) | 0.0473 |
| Altered coagulation | ||||
| No risk factor | 8 (57.1) | 65 (83.3) | ||
| Medication or hemostatic disorders | 6 (42.9) | 13 (16.7) | 0.8487 (0.4668211–1.542828) | 0.591 |
| Tumor cavitation | ||||
| Absence | 9 (64.3) | 36 (50.0) | ||
| Presence | 5 (35.7) | 36 (50.0) | 2.0597 (1.277593–3.320675) | 0.00302 |
| Tumor necrosis | ||||
| Absence | 6 (42.8) | 18 (24.7) | ||
| Presence | 8 (57.2) | 55 (75.3) | 1.9091 (1.113582–3.272895) | 0.0187 |
| Pulmonary artery | ||||
| Normal | 1 (7.2) | 4 (5.6) | ||
| Irregularity | 4 (28.6) | 35 (48.6) | 1.3260 (0.4692674–3.746619) | 0.594 |
| Occlusion | 3 (21.4) | 21 (29.2) | 0.8468 (0.2862588–2.504777) | 0.764 |
| Pseudoaneurysm | 6 (42.8) | 12 (16.7) | 1.3277 (0.4243536–4.154165) | 0.626 |
| Tumor size | 71.08 (13.32) | 75.97 (28.44) | 1.01113 (1.0–1.02) | 0.023 |
| Proximal embolization | ||||
| No | 6 (60.0) | 20 (40.0) | ||
| Yes | 4 (40.0) | 30 (60.0) | 1.1918 (0.6748679–2.104721) | 0.545 |
| Embolization agents | ||||
| Coils | 9 (64.3) | 26 (34.2) | ||
| Glue | 2 (14.3) | 11 (14.5) | 1.7710 (0.8662912–3.620735) | 0.1172 |
| Gelatin sponge | 0 (0.0) | 1 (1.3) | 7.1076 (0.9108879–55.459520) | 0.0614 |
| Plug | 0 (0.0) | 12 (15.8) | 1.1839 (0.5957885–2.352425) | 0.6300 |
| Covered stent | 3 (21.4) | 26 (34.2) | 1.3588 (0.7881746–2.342384) | 0.2699 |
| Recurrence of hemoptysis | ||||
| No | 8 (57.1) | 36 (51.4) | ||
| Yes | 4 (42.9) | 34 (48.6) | 0.7623 (0.4703713–1.235272) | 0.27 |
| Immediate bleeding cessation | ||||
| No | 0 (0.0) | 8 (10.3) | ||
| Yes | 14 (100.0) | 70 (89.7) | 0.5703 (0.2731161–1.190974) | 0.135 |
| HR | HR IC: Lower 0.95 | HR IC: Upper 0.95 | p-Value | |
|---|---|---|---|---|
| Age | 1.01594 | 0.97192 | 1.0620 | 0.48405 |
| Sex | ||||
| Female | 1 (Ref) | |||
| Male | 1.60732 | 0.53484 | 4.8303 | 0.39794 |
| Histology | ||||
| Primary | 1 (Ref) | |||
| Secondary | 1.32056 | 0.16292 | 10.7037 | 0.79452 |
| Histology | ||||
| Adenocarcinoma | 1 (Ref) | |||
| Other | 0.65678 | 0.15641 | 2.7580 | 0.56581 |
| Epidermoid | 0.33961 | 0.11544 | 0.9992 | 0.04982 |
| Volume Of Hemoptysis | ||||
| Minimal | 1 (Ref) | |||
| Massive | 4.49076 | 0.22268 | 0.80803 | 0.08609 |
| Medium | 5.44441 | 0.18367 | 1.20513 | 0.02763 |
| Hemodynamic Condition | ||||
| Instability | 1 (Ref) | |||
| Stability | 0.89437 | 0.32958 | 2.4271 | 0.82652 |
| Altered Coagulation | ||||
| No risk factor | 1 (Ref) | |||
| Medication or hemostatic disorders | 0.64646 | 0.23181 | 1.8029 | 0.40447 |
| Tumor Cavitation | ||||
| Absence | 1 (Ref) | |||
| Presence | 4.95697 | 1.84528 | 13.3159 | 0.00150 |
| Tumor Necrosis | ||||
| Absence | 1 (Ref) | |||
| Presence | 0.93443 | 0.30310 | 2.8808 | 0.90602 |
| Pulmonary Artery | ||||
| Normal | 1 (Ref) | |||
| Irregularity | 5.31143 | 0.98012 | 28.7834 | 0.05278 |
| Occlusion | 5.15053 | 0.69212 | 38.3285 | 0.10946 |
| Pseudoaneurysm | 13.91491 | 2.03048 | 95.3590 | 0.00734 |
| Tumor size | 1.02046 | 0.99964 | 1.0417 | 0.05412 |
| Embolization Agents | ||||
| Coils | 1 (Ref) | |||
| Glue | 2.33382 | 0.72102 | 7.5541 | 0.15731 |
| Gelatin sponge | 21.24199 | 1.28991 | 349.8082 | 0.03251 |
| Plug | 0.91880 | 0.28363 | 2.9764 | 0.88770 |
| Covered stent | 6.20609 | 2.10414 | 18.3046 | 0.00094 |
| Immediate Bleeding Cessation | ||||
| No | 1 (Ref) | |||
| Yes | 0.81238 | 0.22729 | 2.9036 | 0.74918 |
| Recurrence of hemoptysis | ||||
| No | 1 (Ref) | |||
| Yes | 0.26032 | 0.09907 | 0.6840 | 0.00633 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Claudinot, A.; Douane, F.; Morla, O.; Perret, C.; Neveu, M.; Thouveny, F.; Bouvier, A.; Hureaux, J.; Le Guen, A.; Jouan, J.; et al. Pulmonary Artery Embolization in the Management of Hemoptysis Related to Lung Tumors. J. Pers. Med. 2023, 13, 1597. https://doi.org/10.3390/jpm13111597
Claudinot A, Douane F, Morla O, Perret C, Neveu M, Thouveny F, Bouvier A, Hureaux J, Le Guen A, Jouan J, et al. Pulmonary Artery Embolization in the Management of Hemoptysis Related to Lung Tumors. Journal of Personalized Medicine. 2023; 13(11):1597. https://doi.org/10.3390/jpm13111597
Chicago/Turabian StyleClaudinot, Amandine, Frédéric Douane, Olivier Morla, Christophe Perret, Marine Neveu, Francine Thouveny, Antoine Bouvier, José Hureaux, Arnaud Le Guen, Jérémy Jouan, and et al. 2023. "Pulmonary Artery Embolization in the Management of Hemoptysis Related to Lung Tumors" Journal of Personalized Medicine 13, no. 11: 1597. https://doi.org/10.3390/jpm13111597
APA StyleClaudinot, A., Douane, F., Morla, O., Perret, C., Neveu, M., Thouveny, F., Bouvier, A., Hureaux, J., Le Guen, A., Jouan, J., Heautot, J.-F., Larralde, A., Cerasuolo, D., Bergot, E., Fohlen, A., & Pelage, J.-P. (2023). Pulmonary Artery Embolization in the Management of Hemoptysis Related to Lung Tumors. Journal of Personalized Medicine, 13(11), 1597. https://doi.org/10.3390/jpm13111597