
Type 1 Diabetes Mellitus and Autoimmune Diseases: A Critical Review of the Association and the Application of Personalized Medicine

 , , and
, , and 
Abstract
:
1. Introduction
2. Materials and Methods
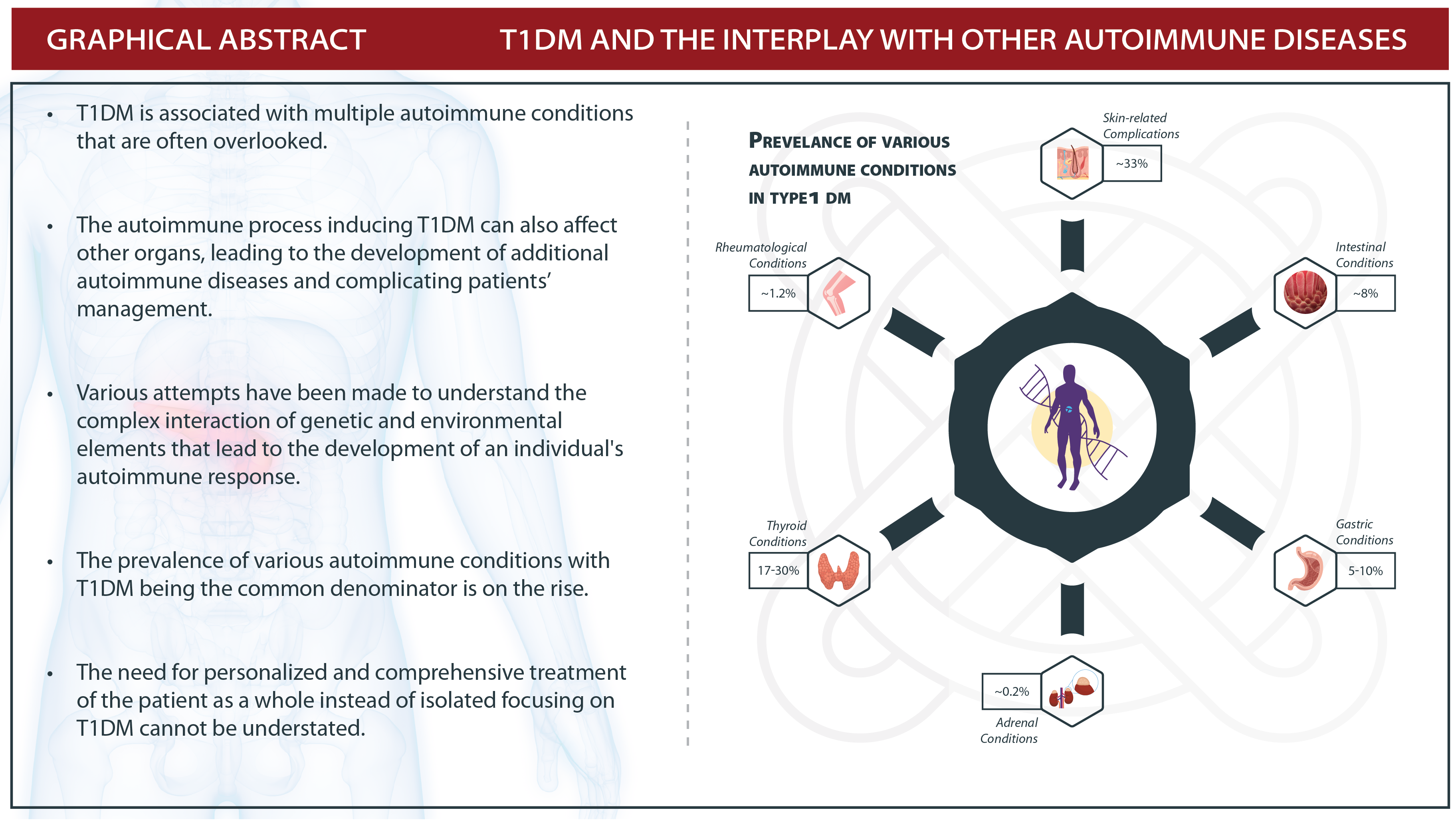
3. T1DMand Autoimmune Endocrine Pathology
3.1. Hashimoto’s Thyroiditis and Graves’ Disease
3.2. Addison’s Disease
3.3. Autoimmune Hypoparathyroidism
3.4. T1DM and Celiac Disease
3.5. Autoimmune Gastritis
3.6. T1DMand Autoimmune Skin Pathology
3.6.1. Hives
3.6.2. Alopecia
3.6.3. Psoriasis
3.7. T1DM and Rheumatological Autoimmune Pathology
3.7.1. Rheumatoid Arthritis
3.7.2. Sjogren’s Syndrome
3.7.3. Systemic Lupus Erythematosus
4. Moving towards Personalized Patient-Centered Management
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Speight, J.; Pouwer, F. Diabetes Mellitus Type 1. In Cambridge Handbook of Psychology, Health and Medicine, 3rd ed.; Cambridge University Press: Cambridge, UK, 2022; pp. 477–480. [Google Scholar] [CrossRef]
- Mobasseri, M.; Shirmohammadi, M.; Amiri, T.; Vahed, N.; Fard, H.H.; Ghojazadeh, M. Prevalence and Incidence of Type 1 Diabetes in the World: A Systematic Review and Meta-Analysis. Health Promot. Perspect. 2020, 10, 98–115. [Google Scholar] [CrossRef]
- Krzewska, A.; Ben-Skowronek, I. Effect of Associated Autoimmune Diseases on Type 1 Diabetes Mellitus Incidence and Metabolic Control in Children and Adolescents. BioMed Res. Int. 2016, 2016, 6219730. [Google Scholar] [CrossRef] [Green Version]
- Hansen, M.P. Type 1 Diabetes and Polyglandular Autoimmune Syndrome: A Review. World J. Diabetes 2015, 6, 67–79. [Google Scholar] [CrossRef]
- Biondi, B.; Kahaly, G.J.; Robertson, R.P. Thyroid Dysfunction and Diabetes Mellitus: Two Closely Associated Disorders. Endocr. Rev. 2018, 40, 789–824. [Google Scholar] [CrossRef] [Green Version]
- Nederstigt, C.; Uitbeijerse, B.S.; Janssen, L.G.M.; Corssmit, E.P.M.; de Koning, E.J.P.; Dekkers, O.M. Associated Auto-Immune Disease in Type 1 Diabetes Patients: A Systematic Review and Meta-Analysis. Eur. J. Endocrinol. 2019, 180, 135–144. [Google Scholar] [CrossRef] [Green Version]
- Volta, U.; Tovoli, F.; Caio, G. Clinical and Immunological Features of Celiac Disease in Patients with Type 1 Diabetes Mellitus. Expert Rev. Gastroenterol. Hepatol. 2011, 5, 479–487. [Google Scholar] [CrossRef]
- Cavalu, S.; Simon, V. Proteins adsorption to othopaedic biomaterials: Vibrational spectroscopy evidence. J. Optoelectron. Adv. Mater. 2007, 9, 3297–3302. [Google Scholar]
- Kota, S.K.; Meher, L.K.; Jammula, S.; Kota, S.K.; Modi, K.D. Clinical Profile of Coexisting Conditions in Type 1 Diabetes Mellitus Patients. Diabetes Metab. Syndr. 2012, 6, 70–76. [Google Scholar] [CrossRef]
- Hollowell, J.G.; Staehling, N.W.; Dana Flanders, W.; Harry Hannon, W.; Gunter, E.W.; Spencer, C.A.; Braverman, L.E. Serum TSH, T4, and Thyroid Antibodies in the United States Population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J. Clin. Endocrinol. Metab. 2002, 87, 489–499. [Google Scholar] [CrossRef]
- Franco, J.-S.; Amaya-Amaya, J.; Anaya, J.-M. Thyroid Disease and Autoimmune Diseases. In Autoimmunity: From Bench to Bedside; El Rosario University Press: Bogotá, Colombia, 2013. [Google Scholar]
- Kordonouri, O.; Hartmann, R.; Deiss, D.; Wilms, M.; Grüters-Kieslich, A. Natural Course of Autoimmune Thyroiditis in Type 1 Diabetes: Association with Gender, Age, Diabetes Duration, and Puberty. Arch. Dis. Child. 2005, 90, 411–414. [Google Scholar] [CrossRef] [Green Version]
- Kakleas, K.; Soldatou, A.; Karachaliou, F.; Karavanaki, K. Associated Autoimmune Diseases in Children and Adolescents with Type 1 Diabetes Mellitus (T1DM). Autoimmun. Rev. 2015, 14, 781–797. [Google Scholar] [CrossRef]
- Furuya, F.; Shimura, H.; Yamashita, S.; Endo, T.; Kobayashi, T. Liganded Thyroid Hormone Receptor-α Enhances Proliferation of Pancreatic β-Cells. J. Biol. Chem. 2010, 285, 24477–24486. [Google Scholar] [CrossRef] [Green Version]
- Fukuchi, M.; Shimabukuro, M.; Shimajiri, Y.; Oshiro, Y.; Higa, M.; Akamine, H.; Komiya, I.; Takasu, N. Evidence for a Deficient Pancreatic β-Cell Response in a Rat Model of Hyperthyroidism. Life Sci. 2002, 71, 1059–1070. [Google Scholar] [CrossRef]
- Duntas, L.H.; Orgiazzi, J.; Brabant, G. The Interface between Thyroid and Diabetes Mellitus. Clin. Endocrinol. 2011, 75, 1–9. [Google Scholar] [CrossRef]
- Duntas, L.H. Thyroid Disease and Lipids. Thyroid 2002, 12, 287–293. [Google Scholar] [CrossRef]
- Kadiyala, R.; Peter, R.; Okosieme, O.E. Thyroid Dysfunction in Patients with Diabetes: Clinical Implications and Screening Strategies. Int. J. Clin. Pract. 2010, 64, 1130–1139. [Google Scholar] [CrossRef] [Green Version]
- Maratou, E.; Hadjidakis, D.J.; Peppa, M.; Alevizaki, M.; Tsegka, K.; Lambadiari, V.; Mitrou, P.; Boutati, E.; Kollias, A.; Economopoulos, T.; et al. Studies of Insulin Resistance in Patients with Clinical and Subclinical Hyperthyroidism. Eur. J. Endocrinol. 2010, 163, 625–630. [Google Scholar] [CrossRef] [Green Version]
- Solá, E.; Morillas, C.; Garzón, S.; Gómez-Balaguer, M.; Hernández-Mijares, A. Association between Diabetic Ketoacidosis and Thyrotoxicosis. Acta Diabetol. 2002, 39, 235–237. [Google Scholar] [CrossRef]
- O’mearat, N.M.; Blackman, J.D.; Sturis, J.; Polonsky, K.S. Alterations in the Kinetics of C-Peptide and Insulin Secretion in Hyperthyroidism. J. Clin. Endocrinol. Metab. 1993, 76, 79–84. [Google Scholar] [CrossRef]
- Bech, K.; Damsbo, P.; Eldrup, E.; Beck-Nielsen, H.; Røder, M.E.; Hartling, S.G.; Vølund, A.; Madsbad, S. β-Cell Function and Glucose and Lipid Oxidation in Graves’ Disease. Clin. Endocrinol. 1996, 44, 59–66. [Google Scholar] [CrossRef]
- Kalmann, R.; Mourits, M.P. Diabetes Mellitus: A Risk Factor in Patients with Graves’ Orbitopathy. Br. J. Ophthalmol. 1999, 83, 463–465. [Google Scholar] [CrossRef] [Green Version]
- Handisurya, A.; Pacini, G.; Tura, A.; Gessl, A.; Kautzky-Willer, A. Effects of T4 Replacement Therapy on Glucose Metabolism in Subjects with Subclinical (SH) and Overt Hypothyroidism (OH). Clin. Endocrinol. 2008, 69, 963–969. [Google Scholar] [CrossRef]
- Uppal, V.; Vij, C.; Bedi, G.K.; Vij, A.; Banerjee, B.D. Thyroid Disorders in Patients of Type 2 Diabetes Mellitus. Indian J. Clin. Biochem. 2013, 28, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Kahaly, G.J. Polyglandular Autoimmune Syndromes. Eur. J. Endocrinol. 2009, 161, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Weinstock, C.; Matheis, N.; Barkia, S.; Haager, M.C.; Janson, A.; Marković, A.; Bux, J.; Kahaly, G.J. Autoimmune Polyglandular Syndrome Type 2 Shows the Same HLA Class II Pattern as Type 1 Diabetes. Tissue Antigens 2011, 77, 317–324. [Google Scholar] [CrossRef]
- Papadopoulos, K.I.; Hallengren, B. Polyglandular Autoimmune Syndrome Type II in Patients with Idiopathic Addison’s Disease. Acta Endocrinol. 1990, 122, 472–478. [Google Scholar] [CrossRef]
- Chantzichristos, D.; Eliasson, B.; Johannsson, G. Management of Endocrine Disease: Disease Burden and Treatment Challenges in Patients with Both Addison’s Disease and Type 1 Diabetes Mellitus. Eur. J. Endocrinol. 2020, 183, R1–R11. [Google Scholar] [CrossRef]
- Elbelt, U.; Hahner, S.; Allolio, B. Altered Insulin Requirement in Patients with Type 1 Diabetes and Primary Adrenal Insuffciency Receiving Standard Glucocorticoid Replacement Therapy. Eur. J. Endocrinol. 2009, 160, 919–924. [Google Scholar] [CrossRef] [Green Version]
- Lankisch, T.O.; Jaeckel, E.; Strassburg, C.P. The Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy or Autoimmune Polyglandular Syndrome Type 1. Semin. Liver Dis. 2009, 29, 307–314. [Google Scholar] [CrossRef]
- Fierabracci, A. Type 1 Diabetes in Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy Syndrome (APECED): A “Rare” Manifestation in a “Rare” Disease. Int. J. Mol. Sci. 2016, 17, 1106. [Google Scholar] [CrossRef] [Green Version]
- Alimohammadi, M.; Björklund, P.; Hallgren, Å.; Pöntynen, N.; Szinnai, G.; Shikama, N.; Keller, M.P.; Ekwall, O.; Kinkel, S.A.; Husebye, E.S.; et al. Autoimmune Polyendocrine Syndrome Type 1 and NALP5, a Parathyroid Autoantigen. N. Engl. J. Med. 2008, 358, 1018–1028. [Google Scholar] [CrossRef] [Green Version]
- Kahaly, G.J.; Frommer, L.; Schuppan, D. Celiac Disease and Glandular Autoimmunity. Nutrients 2018, 10, 814. [Google Scholar] [CrossRef] [Green Version]
- Holmes, G.K.T. Coeliac Disease and Type 1 Diabetes Mellitus—The Case for Screening. Diabet. Med. 2001, 18, 169–177. [Google Scholar] [CrossRef]
- Cerutti, F.; Bruno, G.; Chiarelli, F.; Lorini, R.; Meschi, F.; Sacchetti, C. Younger Age at Onset and Sex Predict Celiac Disease in Children and Adolescents with Type 1 Diabetes: An Italian Multicenter Study. Diabetes Care 2004, 27, 1294–1298. [Google Scholar] [CrossRef] [Green Version]
- Bratanic, N.; Smigoc Schweiger, D.; Mendez, A.; Bratina, N.; Battelino, T.; Vidan-Jeras, B. An Influence of HLA-A, B, DR, DQ, and MICA on the Occurrence of Celiac Disease in Patients with Type 1 Diabetes. Tissue Antigens 2010, 76, 208–215. [Google Scholar] [CrossRef]
- Norris, J.M.; Barriga, K.; Klingensmith, G.; Hoffman, M.; Eisenbarth, G.S.; Erlich, H.A.; Rewers, M. Timing of Initial Cereal Exposure in Infancy and Risk of Islet Autoimmunity. JAMA 2003, 290, 1713–1720. [Google Scholar] [CrossRef]
- Yeung, W.C.G.; Rawlinson, W.D.; Craig, M.E. Enterovirus Infection and Type 1 Diabetes Mellitus: Systematic Review and Meta-Analysis of Observational Molecular Studies. BMJ 2011, 342, d35. [Google Scholar] [CrossRef] [Green Version]
- Stene, L.C.; Honeyman, M.C.; Hoffenberg, E.J.; Haas, J.E.; Sokol, R.J.; Emery, L.; Taki, I.; Norris, J.M.; Erlich, H.A.; Eisenbarth, G.S.; et al. Rotavirus Infection Frequency and Risk of Celiac Disease Autoimmunity in Early Childhood: A Longitudinal Study. Am. J. Gastroenterol. 2006, 101, 2333–2340. [Google Scholar] [CrossRef]
- Kemppainen, K.M.; Ardissone, A.N.; Davis-Richardson, A.G.; Fagen, J.R.; Gano, K.A.; León-Novelo, L.G.; Vehik, K.; Casella, G.; Simell, O.; Ziegler, A.G.; et al. Early Childhood Gut Microbiomes Show Strong Geographic Differences among Subjects at High Risk for Type 1 Diabetes. Diabetes Care 2015, 38, 329–332. [Google Scholar] [CrossRef] [Green Version]
- Bhadada, S.K.; Kochhar, R.; Bhansali, A.; Dutta, U.; Kumar, P.R.; Poornachandra, K.S.; Vaiphei, K.; Nain, C.K.; Singh, K. Prevalence and Clinical Profile of Celiac Disease in Type 1 Diabetes Mellitus in North India. J. Gastroenterol. Hepatol. 2011, 26, 378–381. [Google Scholar] [CrossRef]
- Diniz-Santos, D.R.; Brandão, F.; Adan, L.; Moreira, A.; Vicente, E.J.; Silva, L.R. Bone Mineralization in Young Patients with Type 1 Diabetes Mellitus and Screening-Identified Evidence of Celiac Disease. Dig. Dis. Sci. 2008, 53, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Kaspers, S.; Kordonouri, O.; Schober, E.; Grabert, M.; Hauffa, B.P.; Holl, R.W. Anthropometry, Metabolic Control, and Thyroid Autoimmunity in Type 1 Diabetes with Celiac Disease: A Multicenter Survey. J. Pediatr. 2004, 145, 790–795. [Google Scholar] [CrossRef]
- Larsson, K.; Carlsson, A.; Cederwall, E.; Jönsson, B.; Neiderud, J.; Jonsson, B.; Lernmark, Å.; Ivarsson, S.A. Annual Screening Detects Celiac Disease in Children with Type 1 Diabetes. Pediatr. Diabetes 2008, 9, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Diamanti, A.; Capriati, T.; Basso, M.S.; Panetta, F.; Laurora, V.M.D.C.; Bellucci, F.; Cristofori, F.; Francavilla, R. Celiac Disease and Overweight in Children: An Update. Nutrients 2014, 6, 207–220. [Google Scholar] [CrossRef] [Green Version]
- Cavalu, S.; Popa, A.; Bratu, I.; Borodi, G.; Maghiar, A. New Evidences of Key Factors Involved in “Silent Stones” Etiopathogenesis and Trace Elements: Microscopic, Spectroscopic, and Biochemical Approach. Biol. Trace Elem. Res. 2015, 168, 311–320. [Google Scholar] [CrossRef]
- Agarwal, A.; Singh, A.; Mehtab, W.; Gupta, V.; Chauhan, A.; Rajput, M.S.; Singh, N.; Ahuja, V.; Makharia, G.K. Patients with Celiac Disease Are at High Risk of Developing Metabolic Syndrome and Fatty Liver. Intest. Res. 2021, 19, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Wang, R.; Huang, X.; Yang, F.; Yu, S. The Level of Serum Pepsinogen in Diagnosing and Evaluating the Severity of Subacute Combined Degeneration Due to Vitamin B12 Deficiency. Front. Neurol. 2021, 12, 604523. [Google Scholar] [CrossRef] [PubMed]
- Tozzoli, R.; Kodermaz, G.; Perosa, A.R.; Tampoia, M.; Zucano, A.; Antico, A.; Bizzaro, N. Autoantibodies to Parietal Cells as Predictors of Atrophic Body Gastritis: A Five-Year Prospective Study in Patients with Autoimmune Thyroid Diseases. Autoimmun. Rev. 2010, 10, 80–83. [Google Scholar] [CrossRef]
- Alonso, N.; Granada, M.L.; Soldevila, B.; Salinas, I.; Joaquin, C.; Reverter, J.L.; Juncà, J.; Cáceres, E.M.M.; Sanmartí, A. Serum Autoimmune Gastritis Markers, Pepsinogen I and Parietal Cell Antibodies, in Patients with Type 1 Diabetes Mellitus: A 5-Year Prospective Study. J. Endocrinol. Investig. 2011, 34, 340–344. [Google Scholar] [CrossRef]
- Toh, B.H. Diagnosis and Classification of Autoimmune Gastritis. Autoimmun. Rev. 2014, 13, 459–462. [Google Scholar] [CrossRef]
- De Block, C.E.M.; Van Campenhout, C.M.; De Leeuw, I.H.; Keenoy, B.M.Y.; Martin, M.; Van Hoof, V.; Van Gaal, L.E. Soluble Transferrin Receptor Level: A New Marker of Iron Deficiency Anemia, a Common Manifestation of Gastric Autoimmunity in Type 1 Diabetes. Diabetes Care 2000, 23, 1384–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modlin, I.M.; Kidd, M.; Latich, I.; Zikusoka, M.N.; Shapiro, M.D. Current Status of Gastrointestinal Carcinoids. Gastroenterology 2005, 128, 1717–1751. [Google Scholar] [CrossRef] [PubMed]
- Esteban, L.M.; Baxter, A.G. Polyspecificity of Autoimmune Responses in Type 1 (Autoimmune) Diabetes. Clin. Exp. Immunol. 2001, 126, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Kakleas, K.; Kostaki, M.; Critselis, E.; Karayianni, C.; Giannaki, M.; Anyfantakis, K.; Haramaras, I.; Fotinou, A.; Papathanasiou, A.; Karavanaki, K. Gastric Autoimmunity in Children and Adolescents with Type 1 Diabetes: A Prospective Study. Horm. Res. Paediatr. 2012, 77, 121–126. [Google Scholar] [CrossRef]
- Lima, A.L.; Illing, T.; Schliemann, S.; Elsner, P. Cutaneous Manifestations of Diabetes Mellitus: A Review. Am. J. Clin. Dermatol. 2017, 18, 541–553. [Google Scholar] [CrossRef] [PubMed]
- Passanisi, S.; Salzano, G.; Lombardo, F. Skin Involvement in Paediatric Patients with Type 1 Diabetes. Curr. Diabetes Rev. 2021, 18, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Raj, R.; Elshimy, G.; Mishra, R.; Jha, N.; Joseph, V.; Bratman, R.; Tella, S.H.; Correa, R. Dermatologic Manifestations of Endocrine Disorders. Cureus 2021, 13, e18327. [Google Scholar] [CrossRef] [PubMed]
- Pavlović, M.D.; Milenković, T.; Dinić, M.; Mišović, M.; Daković, D.; Todorović, S.; Daković, Z.; Zečevi, R.D.; Doder, R. The Prevalence of Cutaneous Manifestations in Young Patients with Type 1 Diabetes. Diabetes Care 2007, 30, 1964–1967. [Google Scholar] [CrossRef] [Green Version]
- Kolkhir, P.; Giménez-Arnau, A.M.; Kulthanan, K.; Peter, J.; Metz, M.; Maurer, M. Urticaria. Nat. Rev. Dis. Prim. 2022, 8, 61. [Google Scholar] [CrossRef]
- Confino-Cohen, R.; Chodick, G.; Shalev, V.; Leshno, M.; Kimhi, O.; Goldberg, A. Chronic Urticaria and Autoimmunity: Associations Found in a Large Population Study. J. Allergy Clin. Immunol. 2012, 129, 1307–1313. [Google Scholar] [CrossRef]
- Kaplan, A.P.; Greaves, M. Pathogenesis of Chronic Urticaria. Clin. Exp. Allergy 2009, 39, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.Y.; Lin, C.L.; Lin, C.C.; Hsu, W.H.; Hsu, C.Y.; Kao, C.H. Risk of Urticaria in Children with Type 1 Diabetes Mellitus: A Nationwide Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyman, S.J.; Shreffler, W.G.; Rapaport, R. Type 1 Diabetes, Autoimmune Thyroid Disease, and Chronic Urticaria. Pediatr. Diabetes 2008, 9, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.Y.; Shin, C.H.; Yang, S.W. Polymorphisms of HLA Class II Predispose Children and Adolescents with Type 1 Diabetes Mellitus to Autoimmune Thyroid Disease. Autoimmunity 2003, 36, 177–181. [Google Scholar] [CrossRef]
- Villasante Fricke, A.C.; Miteva, M. Epidemiology and Burden of Alopecia Areata: A Systematic Review. Clin. Cosmet. Investig. Dermatol. 2015, 8, 397–403. [Google Scholar]
- Juárez-Rendón, K.J.; Sánchez, G.R.; Reyes-López, M.; García-Ortiz, J.E.; Bocanegra-García, V.; Guardiola-Avila, I.; Altamirano-García, M.L. Alopecia Areata. Current Situation and Perspectives. Arch. Argent. Pediatr. 2017, 115, e404–e411. [Google Scholar]
- Hunt, N.; McHale, S. The Psychological Impact of Alopecia. Br. Med. J. 2005, 331, 951–953. [Google Scholar] [CrossRef] [Green Version]
- Strazzulla, L.C.; Wang, E.H.C.; Avila, L.; Lo Sicco, K.; Brinster, N.; Christiano, A.M.; Shapiro, J. Alopecia Areata: Disease Characteristics, Clinical Evaluation, and New Perspectives on Pathogenesis. J. Am. Acad. Dermatol. 2018, 78, 1–12. [Google Scholar] [CrossRef]
- Tan, E.; Tay, Y.K.; Goh, C.L.; Giam, Y.C. The Pattern and Profile of Alopecia Areata in Singapore—A Study of 219 Asians. Int. J. Dermatol. 2002, 41, 748–753. [Google Scholar] [CrossRef]
- Betz, R.C.; Petukhova, L.; Ripke, S.; Huang, H.; Menelaou, A.; Redler, S.; Becker, T.; Heilmann, S.; Yamany, T.; Duvic, M.; et al. Genome-Wide Meta-Analysis in Alopecia Areata Resolves HLA Associations and Reveals Two New Susceptibility Loci. Nat. Commun. 2015, 6, 5966. [Google Scholar] [CrossRef] [Green Version]
- Makino, S.; Uchihashi, T.; Kataoka, Y.; Fujiwara, M. Recovery from Alopecia Areata in a Patient with Autoimmune Polyglandular Syndrome Type 3. Endocrinol. Diabetes Metab. Case Rep. 2015, 2015, 140084. [Google Scholar] [CrossRef] [Green Version]
- Arousse, A.; Boussofara, L.; Mokni, S.; Gammoudi, R.; Saidi, W.; Aounallah, A.; Belajouza, C.; Ghariani, N.; Denguezli, M.; Nouira, R. Alopecia Areata in Tunisia: Epidemio-Clinical Aspects and Comorbid Conditions. A Prospective Study of 204 Cases. Int. J. Dermatol. 2019, 58, 811–815. [Google Scholar] [CrossRef]
- Huang, K.P.; Mullangi, S.; Guo, Y.; Qureshi, A.A. Autoimmune, Atopic, and Mental Health Comorbid Conditions Associated with Alopecia Areata in the United States. JAMA Dermatol. 2013, 149, 789–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noso, S.; Park, C.; Babaya, N.; Hiromine, Y.; Harada, T.; Ito, H.; Taketomo, Y.; Kanto, K.; Oiso, N.; Kawada, A.; et al. Organ Specificity in Autoimmune Diseases: Thyroid and Islet Autoimmunity in Alopecia Areata. J. Clin. Endocrinol. Metab. 2015, 100, 1976–1983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, C.E.M.; Armstrong, A.W.; Gudjonsson, J.E.; Barker, J.N.W.N. Psoriasis. Lancet 2021, 397, 1301–1315. [Google Scholar] [CrossRef] [PubMed]
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dand, N.; Mahil, S.K.; Capon, F.; Smith, C.H.; Simpson, M.A.; Barker, J.N. Psoriasis and Genetics. Acta Derm. Venereol. 2020, 100, adv00030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and Comorbid Diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef] [Green Version]
- Wielosz, E.; Majdan, M.; Żychowska, I.; Jeleniewicz, R. Coexistence of Five Autoimmune Diseases: Diagnostic and Therapeutic Difficulties. Rheumatol. Int. 2008, 28, 919–923. [Google Scholar] [CrossRef]
- Christophers, E. Psoriasis: Heterogeneity, Innate Immunity and Comorbidities. Expert Rev. Dermatol. 2012, 7, 195–202. [Google Scholar] [CrossRef]
- Caroppo, F.; Galderisi, A.; Moretti, C.; Ventura, L.; Belloni Fortina, A. Prevalence of Psoriasis in a Cohort of Children and Adolescents with Type 1 Diabetes. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e589–e591. [Google Scholar] [CrossRef] [PubMed]
- Di Costanzo, L.; Fattorusso, V.; Mozzillo, E.; Patrì, A.; Di Caprio, R.; De Nitto, E.; Balato, N.; Franzese, A. Psoriasis in Children with Type 1 Diabetes: A New Comorbidity to Be Considered? Acta Diabetol. 2017, 54, 803–804. [Google Scholar] [CrossRef] [PubMed]
- Vashist, S.; Mahajan, V.; Mehta, K.; Chauhan, P.; Yadav, R.; Sharma, S.; Sharma, V.; Sharma, A.; Chowdhary, B.; Kumar, P. Association of Psoriasis with Autoimmune Disorders: Results of a Pilot Study. Indian Dermatol. Online J. 2020, 11, 753. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.L.; Burnet, S.P.; McNeil, J.D. Musculoskeletal Manifestations of Diabetes Mellitus. Br. J. Sport. Med. 2003, 37, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Burner, T.W.; Rosenthal, A.K. Diabetes and Rheumatic Diseases. Curr. Opin. Rheumatol. 2009, 21, 50–54. [Google Scholar] [CrossRef]
- Gibofsky, A. Epidemiology, Pathophysiology, and Diagnosis of Rheumatoid Arthritis: A Synopsis. Am. J. Manag. Care 2014, 20, S128–S135. [Google Scholar]
- Karlson, E.W.; Chang, S.C.; Cui, J.; Chibnik, L.B.; Fraser, P.A.; De Vivo, I.; Costenbader, K.H. Gene-Environment Interaction between HLA-DRB1 Shared Epitope and Heavy Cigarette Smoking in Predicting Incident Rheumatoid Arthritis. Ann. Rheum. Dis. 2010, 69, 54–60. [Google Scholar] [CrossRef]
- Heliovaara, M.; Aho, K.; Knekt, P.; Impivaara, O.; Reunanen, A.; Aromaa, A. Coffee Consumption, Rheumatoid Factor, and the Risk of Rheumatoid Arthritis. Ann. Rheum. Dis. 2000, 59, 631–635. [Google Scholar] [CrossRef] [Green Version]
- Cush, J.J. Rheumatoid Arthritis: Early Diagnosis and Treatment. Med. Clin. N. Am. 2021, 105, 355–365. [Google Scholar] [CrossRef]
- Wasserman, A.M. Diagnosis and Management of Rheumatoid Arthritis. Am. Fam. Physician 2011, 84, 1245–1252. [Google Scholar] [CrossRef]
- Liao, K.P.; Gunnarsson, M.; Källberg, H.; Ding, B.; Plenge, R.M.; Padyukov, L.; Karlson, E.W.; Klareskog, L.; Askling, J.; Alfredsson, L. Specific Association of Type 1 Diabetes Mellitus with Anti-Cyclic Citrullinated Peptide-Positive Rheumatoid Arthritis. Arthritis Rheum. 2009, 60, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.K.; Salam, M.; Parks, D.; McGill, J.B.; Hughes, J. High Prevalence of Systemic Rheumatic Diseases in Women with Type 1 Diabetes. J. Diabetes Complicat. 2018, 32, 737–739. [Google Scholar] [CrossRef] [PubMed]
- Vivino, F.B. Sjogren’s Syndrome: Clinical Aspects. Clin. Immunol. 2017, 182, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, R.; Brokstad, K.A.; Jonsson, M.V.; Delaleu, N.; Skarstein, K. Current Concepts on Sjögren’s Syndrome—Classification Criteria and Biomarkers. Eur. J. Oral Sci. 2018, 126, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Emmi, G.; Greco, M.; Borro, M.; Sardanelli, F.; Murdaca, G.; Indiveri, F.; Puppo, F. Sjögren’s Syndrome: A Systemic Autoimmune Disease. Clin. Exp. Med. 2022, 22, 9–25. [Google Scholar] [CrossRef]
- Shimomura, H.; Nakase, Y.; Furuta, H.; Nishi, M.; Nakao, T.; Hanabusa, T.; Sasaki, H.; Okamoto, K.; Furukawa, F.; Nanjo, K. A Rare Case of Autoimmune Polyglandular Syndrome Type 3. Diabetes Res. Clin. Pract. 2003, 61, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Frazzei, G.; van Vollenhoven, R.F.; de Jong, B.A.; Siegelaar, S.E.; van Schaardenburg, D. Preclinical Autoimmune Disease: A Comparison of Rheumatoid Arthritis, Systemic Lupus Erythematosus, Multiple Sclerosis and Type 1 Diabetes. Front. Immunol. 2022, 13, 3207. [Google Scholar] [CrossRef] [PubMed]
- Narváez, J. Systemic Lupus Erythematosus 2020. Med. Clin. 2020, 155, 494–501. [Google Scholar] [CrossRef]
- Nashi, R.A.; Shmerling, R.H. Antinuclear Antibody Testing for the Diagnosis of Systemic Lupus Erythematosus. Med. Clin. N. Am. 2021, 105, 387–396. [Google Scholar] [CrossRef]
- Connelly, K.; Morand, E.F. Systemic Lupus Erythematosus: A Clinical Update. Intern. Med. J. 2021, 51, 1219–1228. [Google Scholar] [CrossRef]
- Bao, Y.K.; Weide, L.G.; Ganesan, V.C.; Jakhar, I.; McGill, J.B.; Sahil, S.; Cheng, A.L.; Gaddis, M.; Drees, B.M. High Prevalence of Comorbid Autoimmune Diseases in Adults with Type 1 Diabetes from the HealthFacts Database. J. Diabetes 2019, 11, 273–279. [Google Scholar] [CrossRef]
- Orozco, G.; Sánchez, E.; González-Gay, M.A.; López-Nevot, M.A.; Torres, B.; Cáliz, R.; Ortego-Centeno, N.; Jiménez-Alonso, J.; Pascual-Salcedo, D.; Balsa, A.; et al. Association of a Functional Single-Nucleotide Polymorphism of PTPN22, Encoding Lymphoid Protein Phosphatase, with Rheumatoid Arthritis and Systemic Lupus Erythematosus. Arthritis Rheum. 2005, 52, 219–224. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, M.; Ahmed, S.; Anderson, M.S.; Atkinson, M.A.; Becker, D.; Bingley, P.J.; Bosi, E.; Brusko, T.M.; DiMeglio, L.A.; Evans-Molina, C.; et al. Introducing the Endotype Concept to Address the Challenge of Disease Heterogeneity in Type 1 Diabetes. Diabetes Care 2019, 43, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Klonoff, D.C. Personalized Medicine for Diabetes. J. Diabetes Sci. Technol. 2008, 2, 335–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genuth, S. Insights from The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study on The Use of Intensive Glycemic Treatment to Reduce The Risk of Complications of Type 1 Diabetes. Endocr. Pract. 2006, 12, 34–41. [Google Scholar] [CrossRef]
- Bresson, D.; von Herrath, M. Moving towards efficient therapies in type 1 diabetes: To combine or not to combine? Autoimmun. Rev. 2007, 6, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Zaia, J.A. The status of gene vectors for the treatment of diabetes. Cell Biochem. Biophys. 2007, 48, 183–190. [Google Scholar] [CrossRef]
- Onengut-Gumuscu, S.; Chen, W.-M.; Burren, O.; Cooper, N.J.; Quinlan, A.; Mychaleckyj, J.C.; Farber, E.; Bonnie, J.K.; Szpak, M.; Schofield, E.; et al. Fine mapping of type 1 diabetes susceptibility loci and evidence for colocalization of causal variants with lymphoid gene enhancers. Nat. Genet. 2015, 47, 381–386. [Google Scholar] [CrossRef]
- Onengut-Gumuscu, S.; Chen, W.-M.; Robertson, C.C.; Bonnie, J.K.; Farber, E.; Zhu, Z.; Oksenberg, J.R.; Brant, S.R.; Bridges, S.L.; Edberg, J.C.; et al. Type 1 Diabetes Risk in African-Ancestry Participants and Utility of an Ancestry-Specific Genetic Risk Score. Diabetes Care 2019, 42, 406–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz-Peña, R. Personalized Medicine in Autoimmune Diseases. J. Pers. Med. 2021, 11, 1181. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Autoimmune Pathology | Antibodies | Reference |
|---|---|---|
| Hashimoto’s thyroiditis | Antithyroid peroxidase antibodies Antithyroglobulin antibodies | [4,8] |
| Basedow-Graves-disease | Antithyrotropin receptor antibodies (TRAb) | [11,12] |
| Addison’s disease | Antibodies against 21-hydroxylase | [27,32] |
| Hypoparathyroidism | Antibodies against CaSR(Calcium-Sensing Receptor) Anti NALP5-antibodies | [49] |
| Celiac disease | Antibodies tissue transglutaminase Anti-endomysium antibodies Antigliadin antibodies | [50] |
| Autoimmune gastritis | Antibodies against parietal cells Antibodies against intrinsec factor | [52] |
| Rheumatoid arthritis | Rheumatoid factor FR AAN antinuclear antibodies | [56,76,82] |
| Sjogrens disease | Antinuclear antibodies AAN Anti SS-A/anti-Ro antibodies Anti SS-B/anti-La-antibodies | [92,99] |
| Antinuclear-AAN-antiboies Anti SS-A/anti-Ro antibodies- Anti SS-B/anti-La antibodies Anti-Sm (Smith)-antibodies Antibodies against double-stranded DNA (anti-dc-DNAantibody) | [102] |
| Personalized Medicine | Application in T1DM | References |
|---|---|---|
| Personalized Diagnosis | ||
| 1. HbA1c in Diagnosis and Monitoring | HbA1c is affected by glucose levels, hemoglobin, and red cell stability. Unexpected HbA1c variations can be discovered by blood investigations and genetic testing, hence allowing an individualized approach. | [105] |
| 2. Subcategories in T1DM | Etiological types of T1DM can be established on basis of age of onset of diabetes and type of islet cell antibody present (GAD, ICA512/IA-2, insulin, zinc transporter 8 [ZnT8]) | [106] |
| 3. Early diagnosis of diabetic neuropathy—tight control of DM | Insulin and C-peptide deficiencies cause acute metabolic irregularities, persistent gene regulatory perturbations, poor neurotrophism, protein–protein interactions, and particular degenerative diseases in type 1 DPN (Diabetic Peripheral neuropathy). Hence, complications can be prevented by an individualized approach. | [107] |
| Personalized Therapy | ||
| 1. Intensive insulin therapy | Individually tailored insulin therapy based on HbA1c has proven to be more beneficial. | [108] |
| 2. Immune therapy | Auto-aggressive T cell repertoire varies between patients and the number of residual beta-cells will directly affect insulin production post-treatment. Thus, a combination therapy can be more useful. | [109] |
| 3. Gene therapy | Restoration of insulin responsiveness, suppression of autoimmunity, functional replacement of pancreatic islets, and correction of vascular and nerve damage associated with prolonged hyperglycemia can all be done with gene therapy, and the future holds great promise for the same. | [110] |
| Personalized Prevention and Risk Stratification | ||
| 1. Primary prevention of T1DM in pre-stage 1 | Individual genotyping of the genes on which more than 30% of the T1DM genetic risk is attributed to human leukocyte antigen (HLA) complex genes and more than 50 non-HLA loci. | [111] |
| 2. T1D genetic risk scores (T1D-GRS) | High T1D-GRS has low PPV in populations with low prevalence. | [111,112] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popoviciu, M.S.; Kaka, N.; Sethi, Y.; Patel, N.; Chopra, H.; Cavalu, S. Type 1 Diabetes Mellitus and Autoimmune Diseases: A Critical Review of the Association and the Application of Personalized Medicine. J. Pers. Med. 2023, 13, 422. https://doi.org/10.3390/jpm13030422
Popoviciu MS, Kaka N, Sethi Y, Patel N, Chopra H, Cavalu S. Type 1 Diabetes Mellitus and Autoimmune Diseases: A Critical Review of the Association and the Application of Personalized Medicine. Journal of Personalized Medicine. 2023; 13(3):422. https://doi.org/10.3390/jpm13030422
Chicago/Turabian StylePopoviciu, Mihaela Simona, Nirja Kaka, Yashendra Sethi, Neil Patel, Hitesh Chopra, and Simona Cavalu. 2023. "Type 1 Diabetes Mellitus and Autoimmune Diseases: A Critical Review of the Association and the Application of Personalized Medicine" Journal of Personalized Medicine 13, no. 3: 422. https://doi.org/10.3390/jpm13030422