The Effects of a 4-Week, Intensified Training, and Competition Period on Salivary Hormones, Immunoglobulin A, Illness Symptoms, and Mood State in Elite Synchronised Swimmers


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Training Load
2.2.2. Saliva Collection and Analysis
2.2.3. Questionnaires
2.3. Statistical Analyses
3. Results
3.1. Training Load
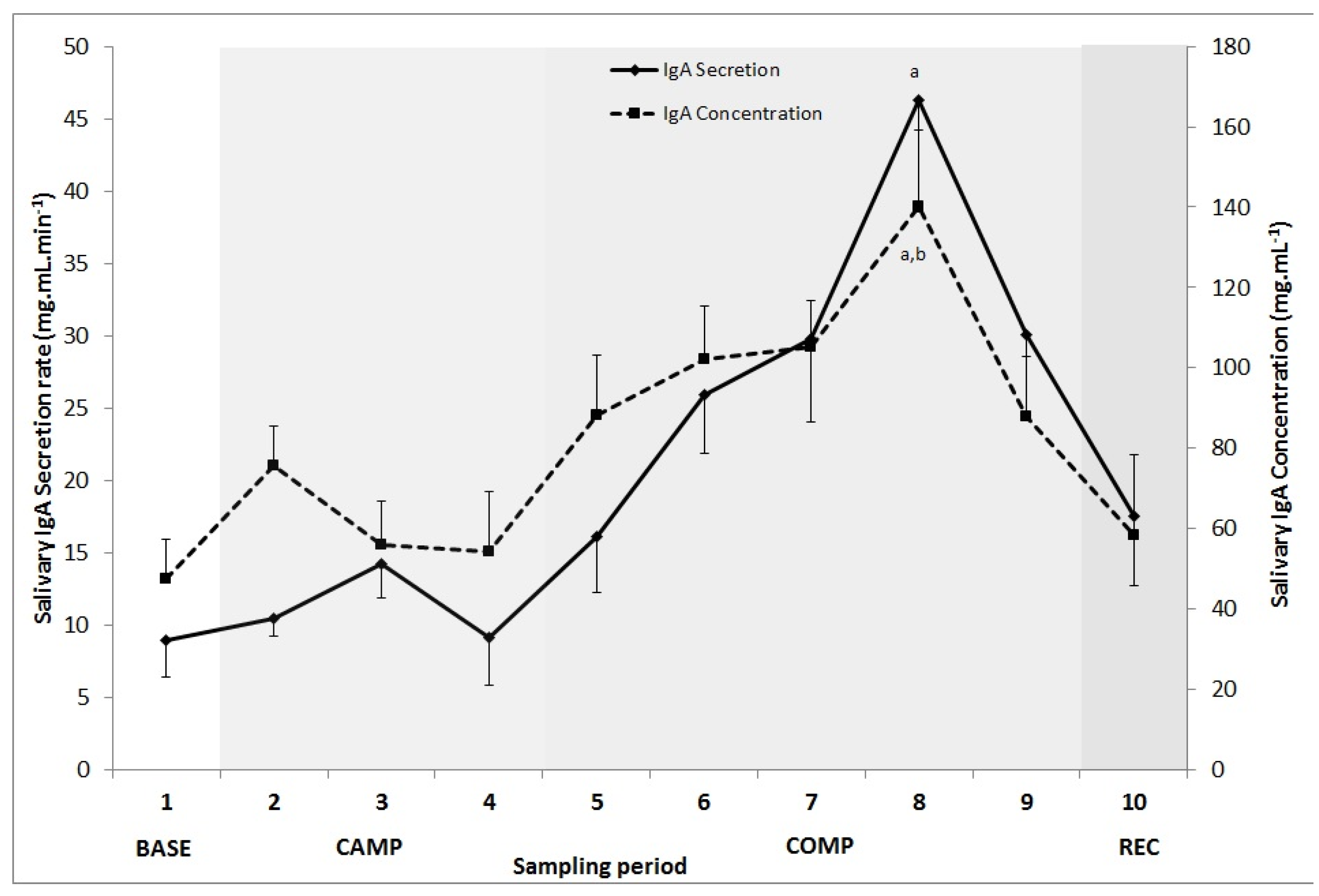
3.2. Salivary IgA and Flow Rate
3.3. Salivary C and T
3.4. DALDA
3.5. Illness Episodes
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Weinberg, S.K. Medical aspects of synchronized swimming. Clin. Sports Med. 1986, 5, 159–167. [Google Scholar] [PubMed]
- Mountjoy, M. Injuries and medical issues in synchronized olympic sports. Curr. Sports Med. Rep. 2009, 8, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Meeusen, R.; Duclos, M.; Foster, C.; Fry, A.; Gleeson, M.; Nieman, D.; Raglin, J.; Rietjens, G.; Steinacker, J.; Urhausen, A. Prevention, diagnosis, and treatment of the overtraining syndrome: Joint consensus statement of the european college of sport science and the american college of sports medicine. Med. Sci. Sports Exerc. 2013, 45, 186–205. [Google Scholar] [CrossRef] [PubMed]
- Halson, S.L. Monitoring training load to understand fatigue in athletes. Sports Med. 2014, 44, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Kellmann, M. Preventing overtraining in athletes in high-intensity sports and stress/recovery monitoring. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. 2), 95–102. [Google Scholar] [CrossRef] [PubMed]
- Urhausen, A.; Gabriel, H.; Kindermann, W. Blood hormones as markers of training stress and overtraining. Sports Med. 1995, 20, 251–276. [Google Scholar] [CrossRef] [PubMed]
- Minetto, M.A.; Lanfranco, F.; Tibaudi, A.; Baldi, M.; Termine, A.; Ghigo, E. Changes in awakening cortisol response and midnight salivary cortisol are sensitive markers of strenuous training-induced fatigue. J. Endocrinol. Investig. 2008, 31, 16–24. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J.; Morgan, W.P.; Raglin, J.S.; Barksdale, C.M.; Kalin, N.H. Mood state and salivary cortisol levels following overtraining in female swimmers. Psychoneuroendocrinology 1989, 14, 303–310. [Google Scholar] [CrossRef]
- Passelergue, P.; Lac, G. Saliva cortisol, testosterone and t/c ratio variations during a wrestling competition and during the post-competitive recovery period. Int. J. Sports Med. 1999, 20, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Duclos, M. A critical assessment of hormonal methods used in monitoring training status in athletes. Int. Sportmed. J. 2008, 9, 56–66. [Google Scholar]
- Aubets, J.; Segura, J. Salivary cortisol as a marker of competition related stress. Sci. Sports 1995, 10, 149–154. [Google Scholar] [CrossRef]
- Raglin, J.; Sawamura, S.; Alexiou, S.; Hassmen, P.; Kentta, G. Training practices and staleness in 13–18-year-old swimmers: A cross-cultural study. Pediatr. Exerc. Sci. 2000, 12, 61–70. [Google Scholar] [CrossRef]
- Kentta, G.; Hassmen, P.; Raglin, J.S. Training practices and overtraining syndrome in swedish age-group athletes. Int. J. Sports Med. 2001, 22, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Halson, S.L.; Bridge, M.W.; Meeusen, R.; Busschaert, B.; Gleeson, M.; Jones, D.A.; Jeukendrup, A.E. Time course of performance changes and fatigue markers during intensified training in trained cyclists. J. Appl. Physiol. 2002, 93, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Milanez, V.F.; Ramos, S.P.; Okuno, N.M.; Boullosa, D.A.; Nakamura, F.Y. Evidence of a non-linear dose-response relationship between training load and stress markers in elite female futsal players. J. Sports Sci. Med. 2014, 13, 22–29. [Google Scholar] [PubMed]
- Gleeson, M.; McDonald, W.A.; Cripps, A.W.; Pyne, D.B.; Clancy, R.L.; Fricker, P.A. The effect on immunity of long-term intensive training in elite swimmers. Clin. Exp. Immunol. 1995, 102, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Pyne, D.B. Special feature for the olympics: Effects of exercise on the immune system: Exercise effects on mucosal immunity. Immunol. Cell Biol. 2000, 78, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, L.; Soligard, T.; Steffen, K.; Alonso, J.M.; Aubry, M.; Budgett, R.; Dvorak, J.; Jegathesan, M.; Meeuwisse, W.H.; Mountjoy, M. Sports injuries and illnesses during the london summer olympic games 2012. Br. J. Sports Med. 2013, 47, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; McDonald, W.A.; Pyne, D.B.; Cripps, A.W.; Francis, J.L.; Fricker, P.A.; Clancy, R.L. Salivary iga levels and infection risk in elite swimmers. Med. Sci. Sports Exerc. 1999, 31, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; McDonald, W.; Pyne, D.; Clancy, R.; Cripps, A.; Francis, J.; Fricker, P. Immune status and respiratory illness for elite swimmers during a 12-week training cycle. Int. J. Sports Med. 2000, 21, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Foster, C. Monitoring training in athletes with reference to overtraining syndrome. Med. Sci. Sports Exerc. 1998, 30, 1164–1168. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Daines, E.; Hector, L.; Snyder, A.C.; Welsh, R. Athletic performance in relation to training load. Wis. Med. J. 1996, 95, 370–374. [Google Scholar] [PubMed]
- Rushall, B.S. A tool for measuring stress tolerance in elite athletes. J. Appl. Sport Psychol. 1990, 2, 51–66. [Google Scholar] [CrossRef]
- Gleeson, M.; Bishop, N.; Oliveira, M.; McCauley, T.; Tauler, P.; Muhamad, A.S. Respiratory infection risk in athletes: Association with antigen-stimulated il-10 production and salivary iga secretion. Scand. J. Med. Sci. Sports 2012, 22, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.; de Moura, N.R.; Coutts, A.; Costa, E.C.; Kempton, T.; Aoki, M.S. Monitoring internal training load and mucosal immune responses in futsal athletes. J. Strength Cond. Res. 2013, 27, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.; Arsati, F.; de Oliveira Lima-Arsati, Y.B.; Simões, A.C.; de Araújo, V.C. Monitoring stress tolerance and occurrences of upper respiratory illness in basketball players by means of psychometric tools and salivary biomarkers. Stress Health 2011, 27, e166–e172. [Google Scholar] [CrossRef]
- Gomes, R.V.; Moreira, A.; Lodo, L.; Nosaka, K.; Coutts, A.J.; Aoki, M.S. Monitoring training loads, stress, immune-endocrine responses and performance in tennis players. Biol. Sport 2013, 30, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Hellhammer, D.H.; Wüst, S.; Kudielka, B.M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Salvador, A.; Suay, F.; Gonzalez-Bono, E.; Serrano, M. Anticipatory cortisol, testosterone and psychological responses to judo competition in young men. Psychoneuroendocrinology 2003, 28, 364–375. [Google Scholar] [CrossRef]
- Gleeson, M.; Allgrove, J.; Reddin, D. Salivary Cortisol, Testosterone and Immunoglobulin a Changes during 3 Consecutive Weeks of Training and International Competition in Elite Rugby Union Players. In Proceedings of the 12th Annual Congress of the European College of Sport Science, Jyväskylä, Finland, 11–14 July 2007. [Google Scholar]
- Filaire, E.; Sagnol, M.; Ferrand, C.; Maso, F.; Lac, G. Psychophysiological stress in judo athletes during competitions. J. Sports Med. Phys. Fit. 2001, 41, 263–268. [Google Scholar]
- Kushnir, M.M.; Rockwood, A.L.; Roberts, W.L.; Pattison, E.G.; Bunker, A.M.; Fitzgerald, R.L.; Meikle, A.W. Performance characteristics of a novel tandem mass spectrometry assay for serum testosterone. Clin. Chem. 2006, 52, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Adlercreutz, H.; Harkonen, M.; Kuoppasalmi, K.; Naveri, H.; Huhtaniemi, I.; Tikkanen, H.; Remes, K.; Dessypris, A.; Karvonen, J. Effect of training on plasma anabolic and catabolic steriod hormones and their response to physical exercise. Int. J. Sports Med. 1986, 7, 27–28. [Google Scholar] [CrossRef] [PubMed]
- Vuorimaa, T.; Ahotupa, M.; Hakkinen, K.; Vasankari, T. Different hormonal response to continuous and intermittent exercise in middle-distance and marathon runners. Scand. J. Med. Sci. Sports 2008, 18, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Vervoorn, C.; Quist, A.M.; Vermulst, L.J.; Erich, W.B.; de Vries, W.R.; Thijssen, J.H. The behaviour of the plasma free testosterone/cortisol ratio during a season of elite rowing training. Int. J. Sports Med. 1991, 12, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C.; Kudielka, B.M.; Gaab, J.; Schommer, N.C.; Hellhammer, D.H. Impact of gender, menstrual cycle phase, and oral contraceptives on the activity of the hypothalamus-pituitary-adrenal axis. Psychosom. Med. 1999, 61, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, H.; Dolan, N.J.; Hounsome, C.; Alajmi, N.; Bishop, N.C. Salivary siga responses to acute moderate-vigorous exercise in monophasic oral contraceptive users. Appl. Physiol. Nutr. Metab. 2015, 40, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Papacosta, E.; Nassis, G.P. Saliva as a tool for monitoring steroid, peptide and immune markers in sport and exercise science. J. Sci. Med. Sport 2011, 14, 424–434. [Google Scholar] [CrossRef] [PubMed]
- Chicharro, J.L.; Lucia, A.; Perez, M.; Vaquero, A.F.; Urena, R. Saliva composition and exercise. Sports Med. 1998, 26, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Ring, C.; Carroll, D.; Hoving, J.; Ormerod, J.; Harrison, L.K.; Drayson, M. Effects of competition, exercise, and mental stress on secretory immunity. J. Sport Sci. 2005, 23, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, L.; Sharp, N.C.C.; Doherty, M. Circadian effects on the acute responses of salivary cortisol and iga in well trained swimmers. Br. J. Sports Med. 2002, 36, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Farzanaki, P.; Azarbayjani, M.; Rasaee, M.; Jourkesh, M.; Ostojic, S.; Stannard, S.; Shabestar Branch, I.; Jourkesh, M. Salivary immunoglobulin a and cortisol response to training in young elite female gymnasts. Braz. J. Microbiol. 2008, 2, 252–258. [Google Scholar]
- Herman, L.; Foster, C.; Maher, M.; Mikat, R.; Porcari, J. Validity and reliability of the session rpe method for monitoring exercise training intensity. S. Afr. J. Sports Med. 2006, 18, 14–17. [Google Scholar] [CrossRef]
- Borresen, J.; Lambert, M.I. The quantification of training load, the training response and the effect on performance. Sports Med. 2009, 39, 779–795. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Time Point (Mean ± SD) | BASE | CAMP | COMP | REC |
|---|---|---|---|---|
| IgA concentration (mg·mL−1) | 47.6 ± 31.0 a | 62.0 ± 32.6 a | 107.4 ± 39.4 | 58.4 ± 62.8 |
| IgA secretion rate (mg·mL·min−1) | 9.0 ± 8.2 a | 11.3 ± 4.5 a | 30.9 ± 13.9 | 17.6 ±15.2 |
| Saliva flow rate (mL·min−1) | 0.19 ± 0.10 | 0.21 ± 0.07 | 0.30 ± 0.11 | 0.35 ± 0.14 |
| Salivary C (µg·mL−1) | 0.63 ± 0.27 a | 0.62 ± 0.19 a | 1.21 ± 0.32 | 0.64 ± 0.32 a |
| Salivary T (pg·mL−1) | 78.9 ± 37.7 | 68.7 ± 31.4 | 70.0 ± 36.4 | 63.5 ±39.7 |
| Illness symptom score | 7 ± 9 | 1 ± 1 | 4 ± 7 | 1 ± 2 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanner, A.; Day, S. The Effects of a 4-Week, Intensified Training, and Competition Period on Salivary Hormones, Immunoglobulin A, Illness Symptoms, and Mood State in Elite Synchronised Swimmers. Sports 2017, 5, 64. https://doi.org/10.3390/sports5030064
Tanner A, Day S. The Effects of a 4-Week, Intensified Training, and Competition Period on Salivary Hormones, Immunoglobulin A, Illness Symptoms, and Mood State in Elite Synchronised Swimmers. Sports. 2017; 5(3):64. https://doi.org/10.3390/sports5030064
Chicago/Turabian StyleTanner, Amy, and Shannon Day. 2017. "The Effects of a 4-Week, Intensified Training, and Competition Period on Salivary Hormones, Immunoglobulin A, Illness Symptoms, and Mood State in Elite Synchronised Swimmers" Sports 5, no. 3: 64. https://doi.org/10.3390/sports5030064
APA StyleTanner, A., & Day, S. (2017). The Effects of a 4-Week, Intensified Training, and Competition Period on Salivary Hormones, Immunoglobulin A, Illness Symptoms, and Mood State in Elite Synchronised Swimmers. Sports, 5(3), 64. https://doi.org/10.3390/sports5030064